
Abstract
Purpose
Survival time after bisphosphonate use has been increasingly recognized to be associated with the incidence of medication-related osteonecrosis of the jaw (MRONJ); however, this has not been elucidated sufficiently in the literature. This study aimed to clarify the incidence of MRONJ and the corresponding survival rate of patients treated with zoledronic acid (ZA) for each type of cancer and obtain useful information for the oral/dental supportive care of cancer patients.
Methods
We evaluated 988 patients who were administered ZA at our hospital; among them, 862 patients with metastatic bone tumors or myeloma were included.
Results
The median survival time (MST) after ZA initiation was 35, 34, 8, 41, 12, and 6 months for patients with breast, prostrate, lung, myeloma, renal, and other cancers, respectively. Patients with cancers that had a short survival time (lung and other cancers [MST = 8 and 6 months, respectively] and cancers with MST < 10 months) did not develop MRONJ; this could be attributed to the shorter duration of ZA administration. The cumulative incidence of MRONJ in breast cancer, prostate cancer, and multiple myeloma was related to the frequency of anti-resorptive drug use and the increased risk over time. In renal cancer, the cumulative incidence of MRONJ increased early, although the MST was 12 months.
Conclusion
For the dentists in charge of dental management, it is essential to be aware of prognosis-related factors, predict MRONJ risk for each cancer treatment, and use risk prediction in dental management planning, particularly for cancers with non-poor prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Bisphosphonate (BP) or denosumab (Dmab) has been used to prevent and treat skeletal-related adverse events caused by cancer bone metastases and multiple myeloma. Many patients benefit from such bone-modifying agents (BMAs). However, medication-related osteonecrosis of the jaw (MRONJ), a serious adverse event, sometimes severely reduces the patient’s quality of life [1]. MRONJ is a disease common to both the medical and dental fields, with no established treatment strategy; therefore, more emphasis should be placed on its prevention. The risk of developing MRONJ can be reduced significantly through dental evaluation and patient management by a team of healthcare providers before and during drug therapy and in the long term [2,3,4]. Non-restorable teeth and those with a poor prognosis should be extracted before initiating BMA administration [5]. Various recommendations, including the need for BP withdrawal, have been proposed for tooth extraction after BP use in non-cancer patients [5, 6]. However, there has been little discussion of the criteria for extracting teeth with poor prognosis before BP treatment in patients with and without cancer. The frequency of adverse events is between 0.2 and 6.7% in cancer patients exposed to BMA, whereas the risk of developing MRONJ in patients affected by osteometabolic diseases, including osteoporosis, is very low, with a prevalence between 0 and 0.4% [5]. Although patients with cancer are at a higher risk of developing MRONJ than those with bone metabolic diseases, the criteria for extraction of teeth with poor prognosis prior to BMA use should be considered more carefully from the perspective of the relationship between life expectancy and cancer type. Recent advances in cancer drug therapy have contributed to improving the prognosis of cancer patients with bone metastases, but prolonging survival leads to an increase in the cumulative dose of BP preparations and long-term BP treatment. These are the most important risk factors for the development of BP-related osteonecrosis of the jaw [7]. The survival time after initiating BP administration has been recently recognized to be associated with MRONJ incidence. However, to our knowledge, no studies have comprehensively demonstrated the relationship between the survival time of patients with each cancer type after bone metastasis and the survival time of patients with myeloma and MRONJ incidence, with the time of BP initiation as the baseline. Patients with a survival time of < 1 year after bone metastasis unsurprisingly have a low chance of MRONJ; in contrast, some cancer types appear to have a high MRONJ incidence, although the survival time is relatively short. Hence, we hypothesized that survival after bone metastasis was not simply related to MRONJ incidence; there are other factors at play. This study aimed to clarify the survival rate and MRONJ incidence in patients treated with zoledronic acid (ZA) at our hospital for each type of cancer and obtain useful information for oral/dental supportive care of cancer patients.
Methods
Patient selection and study design
This retrospective, observational, single-center study included consecutive cancer patients with bone metastasis or multiple myeloma who were diagnosed in our hospital and administered ZA from July 2008 to December 2014.
The inclusion criteria were as follows: ZA initiated at our institution for bone metastases or multiple myeloma and an assessment for MRONJ at the time of evaluation. The exclusion criteria were as follows: starting ZA for reasons other than bone metastases and multiple myeloma and having a history of taking other BP preparations before initiating ZA therapy. The evaluation point was February 2018, and the observation period was from ZA initiation to the evaluation point. The occurrence of MRONJ and survival after ZA treatment initiation were confirmed at the evaluation point.
Bone metastasis was detected by whole-body scintigraphy or positron emission tomography/computed tomography (CT) and other imaging modalities (e.g., standard X-rays, CT, or magnetic resonance imaging of the skeleton). The data related to each patient covered the whole course of the disease and all cancer treatments. Assessed variables included sex, age, sites of bone metastases, survival after bone metastasis diagnosis, survival after MRONJ diagnosis, times of BP therapy, and occurrence of MRONJ. For patients whose survival was difficult to confirm in the medical records of our hospital, confirmation was made through inquiries to the transferring facility or resident registration inquiries with the cooperation of our hospital cancer registry. Finally, the patients’ cancer types were classified into breast, prostate, lung, multiple myeloma, renal, and other cancers, and the 3- and 5-year survival rates for each type and the 8-year cumulative incidence rate of MRONJ were investigated. Breast and prostate cancers were divided into two groups: exclusively bone metastasis (BM) and visceral metastasis (VM; including metastasis to the lung, liver, brain, skin, muscle, pleura, and peritoneum). Thereafter, subgroup analysis was performed. In cases where patients were switched to Dmab after initiating ZA, data on the frequency of ZA and Dmab use were compiled. The total frequency of BMA use was compared among cancer types.
Statistical analysis
Statistical analysis was performed using JMP 14 (SAS Institute, Cary, NC). The 3- and 5-year survival rates and the 8-year cumulative incidence of MRONJ were calculated using the Kaplan–Meier method. Any significant inter-group differences were evaluated using the log-rank test. The Wilcoxon rank-sum test was used to compare the duration to MRONJ occurrence in each group and box plots were used to display the frequency of BMA use. Statistical significance was established at p < 0.05.
Results
Patient details
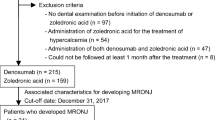
As shown in the flow chart (Fig. 1), 126 of the 988 enrolled patients were ineligible. These included patients with hypercalcemia (n = 112), osteosarcoma (n = 12), bone invasion of solid tumors (n = 1), and non-metastatic pelvic fracture (n = 1). Among 862 included patients, the median age (interquartile range [IQR]) was 65 (57–73) years. The proportions of males (46%) and females (54%) were similar. The cancers were classified into six groups: breast cancer (n = 287, 33%), prostate cancer (n = 163, 19%), lung cancer (n = 134, 16%), multiple myeloma (n = 86, 10%), renal cancer (n = 40, 5%), and other cancers (n = 152, 18%).

Flow chart of study selection. We enrolled 988 patients who started receiving zoledronic acid (ZA) at our hospital between July 2008 and December 2014. Of the 988 patients, the following 126 who were administered ZA for reasons other than bone metastases and multiple myeloma were ineligible: hypercalcemia (n = 112), osteosarcoma (n = 12), bone infiltration of solid tumors (n = 1), and non-metastatic pelvic fractures (n = 1). Thus, 862 people were surveyed, the evaluation points were set in February 2018, and the observation period extended between the initiation of ZA therapy and the evaluation points
Among 862 patients, 757 (88%) received ZA alone, while the remaining 106 (12%) switched to Dmab after ZA administration. Almost all patients received a base dose of 4 mg of ZA intravenously every 4 weeks, but some patients received a reduced dose in the range of 3.0–3.5 mg considering renal function. Dmab was administered at 120 mg/4 weeks. Among patients with breast and renal cancers, 73 (25%) and 7 (17%), respectively, switched to Dmab, mainly because of decreased renal function; in other cancer types, > 90% of patients received ZA alone (Table 1).
Cumulative survival rate after ZA initiation, cumulative MRONJ incidence rate, and time to MRONJ onset
Overall and sex differences
The overall median survival time (MST) after ZA administration was 21 months. Sixty-five patients (7.5%) developed MRONJ, and the 8-year cumulative incidence of MRONJ was 32.1%. The MST was 14 and 26 months for males and females, respectively, with a significant inter-group difference observed with log-rank test (p = 0.002). Although 30 males and 35 females developed MRONJ, the 8-year cumulative MRONJ incidence was 34.2% and 30.4% for males and females, respectively, with the log-rank test showing no statistically significant difference (p = 0.18; Table 2).
Overall, the cumulative incidence of MRONJ increased steadily after initiating ZA therapy: 4.7%, 18.1%, and 32.1% at 2, 5, and 8 years, respectively (Fig. 2a).

Survival curve after zoledronic acid use and cumulative incidence of osteonecrosis of the jaw. a Overall, the cumulative incidence of medication-related osteonecrosis of the jaw (MRONJ) increased yearly since initiating zoledronic acid (ZA) administration. The 2-, 5-, and 8-year cumulative incidences were 4.7%, 18.1%, and 32.1%, respectively. b The median survival time (MST) of patients with each cancer type after initiating ZA administration was as follows: breast cancer, 35 months; prostate cancer, 34 months; lung cancer, 8 months; myeloma, 41 months; renal cancer, 12 months, and other cancers, 6 months. The three cancer types with the longest MST (breast cancer, prostate cancer, myeloma) had a long and good prognosis. Contrastingly, lung cancer and other cancers had a poor prognosis. Renal cancer showed a survival curve between that of the above two groups. c The cumulative incidence of MRONJ was highest in prostate cancer, which had a good prognosis, followed by renal and breast cancer. Unlike other cancers, renal cancer was characterized by MRONJ development at an early stage. No bone necrosis occurred in patients with bone metastases from lung cancer or other cancers with poor prognosis. The log-rank test showed a significant difference in cumulative incidence between renal and breast cancer (p = 0.0035) and between renal cancer and myeloma (p = 0.0148)
Comparison between types of cancer
The MST of each cancer type after initiating ZA administration is shown in Table 2. Breast cancer, prostate cancer, and myeloma had a long MST (> 30 months). However, lung cancer and other cancers had an MST < 10 months. Renal cancer showed an intermediate survival curve between these with an MST of 12 months (Fig. 2b).
The incidence of MRONJ and cumulative incidence for 8 years for each cancer type are shown in Table 2. The 8-year cumulative incidence rate for MRONJ was the highest for prostate cancer, the group with the best prognosis, followed by renal and breast cancer. Unlike other cancers, renal cancer was characterized by the early occurrence of MRONJ. The log-rank test showed a significant difference in the cumulative incidence between renal and breast cancer (p = 0.0035) and between renal cancer and myeloma (p = 0.0148; Fig. 2c). Subgroup analysis was performed on breast and prostate cancer, which are solid cancers with a good prognosis. The 5-year survival rates for the BM and VM groups were 63.1% and 22.2%, respectively, for breast cancer (p < 0.0001) and 38.1% and 27.8%, respectively, for prostate cancer (p = 0.067). In breast cancer, the prognosis was significantly better in the BM group than in the VM group. The 8-year cumulative incidences of MRONJ in the BM and VM groups were 47.2% and 26.5%, respectively, for breast cancer (p = 0.25) and 42.5% and 7.7%, respectively, for prostate cancer (p = 0.66). There was a tendency for the BM group to show a high cumulative incidence, but no significant difference was observed (Table 2).
Frequency of BMA use and time to MRONJ occurrence
The median number of times BMA was used for each cancer type was 26, 18, 10, 7, 3.5, and 3 for breast cancer, prostate cancer, myeloma, renal cancer, lung cancer, and other cancers, respectively. The frequency of BMA use was significantly different between most cancer types (Fig. 3a). When comparing the time to MRONJ onset exclusively in patients with MRONJ (n = 65), the median time to onset of MRONJ was 44, 27, 32, and 17 months for breast cancer, prostate cancer, multiple myeloma, and renal cancer, respectively. Breast cancer had a significantly longer time to MRONJ development than prostate (p = 0.0187) or kidney cancer (p = 0.0062; Fig. 3b).

Comparison of bone-modifying agent (BMA) usage frequency for each cancer type, period until medication-related osteonecrosis of the jaw (MRONJ) occurrence, and BMA usage frequency in MRONJ group and non-MRONJ group. a The median frequency of BMA was use for cancer types with MRONJ was as follows: breast cancer, 26 times; prostate cancer, 18.5 times; myeloma, 10 times; and renal cancer, 7 times. In lung cancer and other cancers, wherein MRONJ did not occur, the median BMA usage was 4 and 3 times, respectively. b The box plot displays the duration from BMA therapy initiation to onset of MRONJ for four cancer types. Breast cancer had a significantly longer duration to MRONJ development than prostate or renal cancer (p = 0.019, p = 0.006, respectively). c BMA therapy was used significantly more frequently in the MRONJ group than in the non-MRONJ group in each cancer type. In the MRONJ group, the median BMA usage was 45 times for breast cancer, which was significantly higher than that for prostate (27 times, p = 0.002) or renal cancer (19 times; p = 0.003)
The four cancer types in which MRONJ occurred (n = 576) were divided into two groups, an MRONJ group (n = 65) and a non-MRONJ group (n = 511), and the median number of times of BMA use was compared. Median BMA usage in the MRONJ and non-MRONJ groups was 45 and 24 times, respectively, for breast cancer (p < 0.0001); 27 and 17 times, respectively, for prostate cancer (p < 0.0087); 28 and 10 times, respectively, for myeloma (p < 0.0065); and 19 and 5 times, respectively, for renal cancer (p < 0.0302). That is, the frequency of BMA use was significantly higher in the MRONJ group than in the non-MRONJ group in each cancer type. In the MRONJ development group (n = 65), the median frequency of BMA use until the onset of MRONJ was 45 times for breast cancer, which was significantly higher than 27 times for prostate cancer (p = 0.0023) and 19 times for renal cancer (p = 0.0031; Fig. 3c).
Myeloma showed different MRONJ risks for two solid cancers, breast and prostate cancer. The 5-year cumulative incidence of MRONJ was 19.2%, 22.1%, and 13.2% for breast cancer, prostate cancer, and myeloma, respectively. The cumulative incidence over the subsequent 8 years was 34.8%, 39.4%, and 19.4% for breast cancer, prostate cancer, and myeloma, respectively. That is, a high increase of 15% or more was observed in bone metastases of solid tumors over 3 years, whereas a low increase of about 6% was observed in myeloma (Fig. 3b). The median frequency of BMA use was significantly lower for myeloma (n = 10) than for breast cancer (n = 26) and prostate cancer (18.5; p < 0.0001 and p = 0.0071, respectively; Fig. 3a).
Discussion
We conducted a retrospective survey of the survival time after ZA administration and cumulative incidence of MRONJ in patients taking ZA, based on the hypothesis that MRONJ risk differs depending on the cancer type and that it may be related to prognosis—or the number of times BMA is administered. Overall, the 8-year cumulative incidence of MRONJ after ZA use was 32.1% and the 3-year cumulative incidence was 9.1% in this study. Soutome et al. reported a 3-year cumulative incidence of 29.2% [8]; therefore, our hospital had a lower cumulative incidence of MRONJ. The significant difference in survival time between males and females was considered to reflect the effects of renal and lung cancers, as MSTs for prostate and breast cancer were almost consistent. However, there was no significant difference between the sexes in the cumulative incidence of MRONJ. Although prostate cancer had a higher cumulative incidence than breast cancer, the absence of osteonecrosis in lung cancer, which occurred more often in males than in females, led to a lower cumulative incidence among males. Therefore, we presumed that there was no sex difference in the cumulative incidence of MRONJ. The cumulative incidence of MRONJ increased over time (4.7%, 18.1%, and 32.1% at 2, 5, and 8 years, respectively) (Fig. 2a); however, further analysis of each cancer type revealed that this was not a simple increase over time.
Breast cancer, prostate cancer, and multiple myeloma
In multiple myeloma, the Mayo Clinic consensus statement on the use of BMAs recommends discontinuing BP after 2 years of treatment for patients who achieve a complete response and/or plateau phase and suggests that patients with active disease, no response, or impending bone disease for > 2 years can have treatment frequency reduced to every 3 months [9]. Corso et al. also reported that the group receiving ZA monthly for 1 year and every 3 months thereafter had a similar incidence of skeletal-related events but had a one-eighth reduction in risk of osteonecrosis than the group that continued to receive ZA monthly [10]. We believe that the low number of BP doses for myeloma in the three carcinomas with good prognosis at our institution is the reason why the cumulative incidence of MRONJ remained low. However, for bone metastases of solid tumors, there is no indication for BP discontinuation or reduction, and after initiation, MRONJ risk tends to increase as the frequency of BMA administration continues to increase according to survival. Among breast cancer patients with distant metastasis, patients with BM and VM showed poor prognosis in the internal VM group [11,12,13]. Similarly, in the prostate cancer group, those with VM generally had a worse prognosis than those with BM [14, 15]. In our study, breast and prostate cancers showed a better prognosis in the BM group, and in breast cancer, the difference was significant. The cumulative incidence of MRONJ also tended to be higher in the BM group. Katagiri et al. found that six items, including primary tumor and presence of visceral metastases, were important prognostic factors in patients with bone metastases and scored these items to show their correlation with prognosis [16]. PathFX has been developed to depict survival trajectories based on machine learning, which is useful for predicting survival in cancer patients with bone metastases [17,18,19,20]. This tool can help orthopedic surgeons avoid invasive reconstructive procedures for patients with bone metastases and a short survival prognosis. In addition, it may also improve dental management.
Renal cancer
Although renal cancer has an MST of 12 months after ZA administration, approximately 24 months shorter from average than the abovementioned three carcinomas with good prognosis, it has a high MRONJ incidence, with an 8-year cumulative incidence rate of 37.9%, second only to that of prostate cancer. It is characteristic that the MRONJ incidence rate reaches 25.5% as early as 20 months. Only renal cancer developed MRONJ in the early stage, causing us to investigate further. van Cann et al. reported that the MRONJ incidence rate was 11% in patients treated with both BMA and vascular endothelial growth factor receptor-tyrosine kinase inhibitor, and the risk of developing MRONJ was 5–10 times higher than that in patients treated with BMA alone [21]. In Vallina et al.’s review of MRONJ patients treated with sunitinib alone or with BP, 49 of 58 patients (84%) were treated with BP [22]. Sunitinib may also cause MRONJ when used alone, although this is very rare [23,24,25,26,27]. Sunitinib-induced suppression of angiogenesis impairs host defense against infection and may increase the risk of osteonecrosis [26]. Bone exposure was sometimes preceded by oral mucositis [28], leading to oral mucosal damage, gingival inflammation and mucositis, delayed wound healing, and infection [24, 26]. In this study, 10 of 40 patients (25.0%) with renal cancer received only palliative irradiation or best supportive care and no intense therapy, whereas 26 of 30 patients (86.7%) who received cancer drug therapy received molecular targeted drugs, three patients (10.0%) received interferon, and one patient (3.3%) received cytotoxic agents. Nineteen patients (63.3%) were treated with sunitinib; 5 of 6 (83%) patients with MRONJ were treated with sunitinib. The time to MRONJ development was 17 months, which was clearly shorter than that of other cancers. Dentists need to make concentrated efforts to prevent MRONJ while considering these factors.
Lung cancer and other cancers
In lung cancer and other cancers with poor prognosis after BM, MRONJ did not occur. The MSTs were as short as 7 and 5 months, respectively, and the median BMA usage was only 4 and 3 times, respectively. We concluded that the low frequency of BMA use was the reason MRONJ did not develop.
There are a few reports on the prognosis of patients with bone metastases from lung cancer. Sugiura et al. reported an MST of 7.2 months [29], which is in close agreement with our findings. Few papers mention MRONJ incidence in patients with bone metastases from lung cancer. Scagliotti et al. found no difference in the cumulative incidence of MRONJ between patients administered ZA or Dmab (0.8% vs. 0.7%, respectively). Moreover, MST was higher in the Dmab group than in the ZA group (8.6 vs. 6.4 months; hazard ratio, 0.68; p = 0.035) [30]. In this study, lung cancer was classified as a group with poor prognosis after BM. However, targeted therapy and immunotherapy have rapidly improved the prognosis of lung cancer in recent years; therefore, dentists should consider the associated increased risk of MRONJ.
Dental management after bone metastasis
In this study, the average MST of breast cancer, prostate cancer, and myeloma was 34 months. Currently, it is predicted that the prognosis for each cancer type after BMA initiation will improve with advance in cancer treatment. In order to avoid the occurrence of MRONJ, it is necessary to prevent odontogenic infections through dental management after the initiation of BMA from a more long-term perspective. On the other hand, before BMA initiation, applying the same tooth extraction criteria used for patients with a good prognosis to patients with a poor prognosis who have an extremely low or no risk of MRONJ may lead to unnecessarily invasive overtreatment. From that point of view, our results showing that MRONJ did not occur in cancers such as lung, bladder, urinary duct, or gastrointestinal cancer is useful information. Many studies have established that preventive oral care methods combined with effective oral health practices are associated with a lower rate of MRONJ [31,32,33,34,35,36,37,38,39,40,41,42,43,44]. Ongoing collaboration among dentists, dental specialists, and oncologists is essential to optimal patient care [45]. In addition to the concept of preventing odontogenic infections, the dentists in charge of dental management before the initiation of BMA need to obtain information on prognosis based on the histological type of cancer, the presence or absence of gene mutation or VM, and the content of cancer treatment from the oncologist or cancer therapist.
Limitations of this study
This was a retrospective cohort study conducted at a single facility. Additionally, the dental management status and MRONJ staging difference after initiating BMA need to be further investigated as secondary endpoints. Since Dmab was launched in Japan in 2012, there have been fewer cases treated with it than ZA and the observation period may have been shorter than the target period of this study. Therefore, patients who started BMA with Dmab were excluded from our study. In a study by Hallmer et al., the incidence of MRONJ was higher among breast cancer patients treated with Dmab than among those treated with ZA (13.6% vs. 4.1%) and the MRONJ risk was higher among the former (p = 0.0011) [46]. Future studies are necessary to investigate patients who mainly used Dmab, including the content of their cancer drug therapy.
Conclusion
We found that MRONJ did not occur in lung cancer or other cancers with poor prognosis after BM administration. This was partially consistent with our hypothesis. For cancers without a poor prognosis, survival time was not the sole determinant of MRONJ risk. The comparisons between patients’ prognoses after initiating BMA therapy and occurrence of MRONJ on the same time axis for each cancer type could be pivotal for oncologists and dentists.
Data availability
The datasets used and/or analyzed during the current study are not openly and universally available due to human data and are available from the corresponding author on reasonable request.
Code availability
Not applicable
References
Capocci M, Romeo U, Guerra F, Mannocci A, Tenore G, Annibali S, Ottolenghi L (2017) Medication-related osteonecrosis of the jaws (MRONJ) and quality of life evaluation: a pilot study. Clin Ter 168:e253–e257
Napenas JJ, Kujan O, Arduino PG, Sukumar S, Galvin S, Baricevic M, Costella J, Czerninski R, Peterson DE, Lockhart PB (2015) World Workshop on Oral Medicine VI: controversies regarding dental management of medically complex patients: assessment of current recommendations Oral Surg Oral Med Oral Pathol. Oral Radiol 120:207–226
Wan JT, Sheeley DM, Somerman MJ, Lee JS (2020) Mitigating osteonecrosis of the jaw (ONJ) through preventive dental care and understanding of risk factors. Bone Res 8:14
Di Fede O, Panzarella V, Mauceri R, Fusco V, Bedogni A, Lo Muzio L, Sipmo Onj B, Campisi G (2018) The dental management of patients at risk of medication-related osteonecrosis of the jaw: new paradigm of primary prevention. Biomed Res Int 2018:2684924
Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo T, Mehrotra B, O’Ryan F, American Association of Oral and Maxillofacial Surgeons (2014) American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw–2014 update. J Oral Maxillofac Surg 72:1938–1956
Mozzati M, Arata V, Gallesio G (2013) Tooth extraction in osteoporotic patients taking oral bisphosphonates. Osteoporos Int 24:1707–1712
Thumbigere-Math V, Tu L, Huckabay S, Dudek AZ, Lunos S, Basi DL, Hughes PJ, Leach JW, Swenson KK, Gopalakrishnan R (2012) A retrospective study evaluating frequency and risk factors of osteonecrosis of the jaw in 576 cancer patients receiving intravenous bisphosphonates. Am J Clin Oncol 35:386–392
Soutome S, Hayashida S, Funahara M, Sakamoto Y, Kojima Y, Yanamoto S, Umeda M (2018) Factors affecting development of medication-related osteonecrosis of the jaw in cancer patients receiving high-dose bisphosphonate or denosumab therapy: is tooth extraction a risk factor? PLoS One 13:e0201343
Lacy MQ, Dispenzieri A, Gertz MA, Greipp PR, Gollbach KL, Hayman SR, Kumar S, Lust JA, Rajkumar SV, Russell SJ, Witzig TE, Zeldenrust SR, Dingli D, Bergsagel PL, Fonseca R, Reeder CB, Stewart AK, Roy V, Dalton RJ, Carr AB, Kademani D, Keller EE, Viozzi CF, Kyle RA (2006) Mayo clinic consensus statement for the use of bisphosphonates in multiple myeloma. Mayo Clin Proc 81:1047–1053
Corso A, Varettoni M, Zappasodi P, Klersy C, Mangiacavalli S, Pica G, Lazzarino M (2007) A different schedule of zoledronic acid can reduce the risk of the osteonecrosis of the jaw in patients with multiple myeloma. Leukemia 21:1545–1548
Harries M, Taylor A, Holmberg L, Agbaje O, Garmo H, Kabilan S, Purushotham A (2014) Incidence of bone metastases and survival after a diagnosis of bone metastases in breast cancer patients. Cancer Epidemiol 38:427–434
James JJ, Evans AJ, Pinder SE, Gutteridge E, Cheung KL, Chan S, Robertson JF (2003) Bone metastases from breast carcinoma: histopathological - radiological correlations and prognostic features. Br J Cancer 89:660–665
Jacobson AF, Shapiro CL, Van den Abbeele AD, Kaplan WD (2001) Prognostic significance of the number of bone scan abnormalities at the time of initial bone metastatic recurrence in breast carcinoma. Cancer 91:17–24
Pond GR, Sonpavde G, de Wit R, Eisenberger MA, Tannock IF, Armstrong AJ (2014) The prognostic importance of metastatic site in men with metastatic castration-resistant prostate cancer. Eur Urol 65:3–6
Gandaglia G, Karakiewicz PI, Briganti A, Passoni NM, Schiffmann J, Trudeau V, Graefen M, Montorsi F, Sun M (2015) Impact of the site of metastases on survival in patients with metastatic prostate cancer. Eur Urol 68:325–334
Katagiri H, Okada R, Takagi T, Takahashi M, Murata H, Harada H, Nishimura T, Asakura H, Ogawa H (2014) New prognostic factors and scoring system for patients with skeletal metastasis. Cancer Med 3:1359–1367
Piccioli A, Spinelli MS, Forsberg JA, Wedin R, Healey JH, Ippolito V, Daolio PA, Ruggieri P, Maccauro G, Gasbarrini A, Biagini R, Piana R, Fazioli F, Luzzati A, Di Martino A, Nicolosi F, Camnasio F, Rosa MA, Campanacci DA, Denaro V, Capanna R (2015) How do we estimate survival? External validation of a tool for survival estimation in patients with metastatic bone disease-decision analysis and comparison of three international patient populations. BMC Cancer 15:424
Forsberg JA, Wedin R, Boland PJ, Healey JH (2017) Can we estimate short- and intermediate-term survival in patients undergoing surgery for metastatic bone disease? Clin Orthop Relat Res 475:1252–1261
Ogura K, Gokita T, Shinoda Y, Kawano H, Takagi T, Ae K, Kawai A, Wedin R, Forsberg JA (2017) Can a multivariate model for survival estimation in skeletal metastases (PATHFx) be externally validated using Japanese patients? Clin Orthop Relat Res 475:2263–2270
Anderson AB, Wedin R, Fabbri N, Boland P, Healey J, Forsberg JA (2020) External validation of PATHFx version 3.0 in patients treated surgically and nonsurgically for symptomatic skeletal metastases. Clin Orthop Relat Res 478:808–818
van Cann T, Loyson T, Verbiest A, Clement PM, Bechter O, Willems L, Spriet I, Coropciuc R, Politis C, Vandeweyer RO, Schoenaers J, Debruyne PR, Dumez H, Berteloot P, Neven P, Nackaerts K, Woei AJF, Punie K, Wildiers H, Beuselinck B (2018) Incidence of medication-related osteonecrosis of the jaw in patients treated with both bone resorption inhibitors and vascular endothelial growth factor receptor tyrosine kinase inhibitors. Support Care Cancer 26:869–878
Vallina C, Ramirez L, Torres J, Casanas E, Hernandez G, Lopez-Pintor RM (2019) Osteonecrosis of the jaws produced by sunitinib: a systematic review. Med Oral Patol Oral Cir Bucal 24:e326–e338
Abel Mahedi Mohamed H, Nielsen CEN, Schiodt M (2018) Medication related osteonecrosis of the jaws associated with targeted therapy as monotherapy and in combination with antiresorptives. A report of 7 cases from the Copenhagen Cohort. Oral Surg Oral Med Oral Pathol Oral Radiol 125:157–163
Ashrafi F, Derakhshandeh A, Movahedian B, Moghaddas A (2017) Osteonecrosis of the jaws in patient received bisphosphonates and sunitinib separately: a case report. J Res Pharm Pract 6:182–185
Fleissig Y, Regev E, Lehman H (2012) Sunitinib related osteonecrosis of jaw: a case report Oral Surg Oral Med Oral Pathol. Oral Radiol 113:e1-3
Nicolatou-Galitis O, Migkou M, Psyrri A, Bamias A, Pectasides D, Economopoulos T, Raber-Durlacher JE, Dimitriadis G, Dimopoulos MA (2012) Gingival bleeding and jaw bone necrosis in patients with metastatic renal cell carcinoma receiving sunitinib: report of 2 cases with clinical implications. Oral Surg Oral Med Oral Pathol Oral Radiol 113:234–238
Koch FP, Walter C, Hansen T, Jager E, Wagner W (2011) Osteonecrosis of the jaw related to sunitinib. Oral Maxillofac Surg 15:63–66
Hoefert S, Eufinger H (2010) Sunitinib may raise the risk of bisphosphonate-related osteonecrosis of the jaw: presentation of three cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 110:463–469
Sugiura H, Yamada K, Sugiura T, Hida T, Mitsudomi T (2008) Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop Relat Res 466:729–736
Scagliotti GV, Hirsh V, Siena S, Henry DH, Woll PJ, Manegold C, Solal-Celigny P, Rodriguez G, Krzakowski M, Mehta ND, Lipton L, Garcia-Saenz JA, Pereira JR, Prabhash K, Ciuleanu TE, Kanarev V, Wang H, Balakumaran A, Jacobs I (2012) Overall survival improvement in patients with lung cancer and bone metastases treated with denosumab versus zoledronic acid: subgroup analysis from a randomized phase 3 study. J Thorac Oncol 7:1823–1829
Gabbert TI, Hoffmeister B, Felsenberg D (2015) Risk factors influencing the duration of treatment with bisphosphonates until occurrence of an osteonecrosis of the jaw in 963 cancer patients. J Cancer Res Clin Oncol 141:749–758
Guarneri V, Miles D, Robert N, Dieras V, Glaspy J, Smith I, Thomssen C, Biganzoli L, Taran T, Conte P (2010) Bevacizumab and osteonecrosis of the jaw: incidence and association with bisphosphonate therapy in three large prospective trials in advanced breast cancer. Breast Cancer Res Treat 122:181–188
Haidar A, Jonler M, Folkmar TB, Lund L (2009) Bisphosphonate (zoledronic acid)-induced osteonecrosis of the jaw. Scand J Urol Nephrol 43:442–444
Kajizono M, Sada H, Sugiura Y, Soga Y, Kitamura Y, Matsuoka J, Sendo T (2015) Incidence and risk factors of osteonecrosis of the jaw in advanced cancer patients after treatment with zoledronic acid or denosumab: a retrospective cohort study. Biol Pharm Bull 38:1850–1855
Mavrokokki T, Cheng A, Stein B, Goss A (2007) Nature and frequency of bisphosphonate-associated osteonecrosis of the jaws in Australia. J Oral Maxillofac Surg 65:415–423
Merigo E, Manfredi M, Meleti M, Guidotti R, Ripasarti A, Zanzucchi E, D’Aleo P, Corradi D, Corcione L, Sesenna E, Ferrari S, Poli T, Bonaninil M, Vescovi P (2006) Bone necrosis of the jaws associated with bisphosphonate treatment: a report of twenty-nine cases. Acta Biomed 77:109–117
Palaska PK, Cartsos V, Zavras AI (2009) Bisphosphonates and time to osteonecrosis development. Oncologist 14:1154–1166
Patel CG, Yee AJ, Scullen TA, Nemani N, Santo L, Richardson PG, Laubach JP, Ghobrial IM, Schlossman RL, Munshi NC, Anderson KC, Raje NS (2014) Biomarkers of bone remodeling in multiple myeloma patients to tailor bisphosphonate therapy. Clin Cancer Res 20:3955–3961
Pires FR, Miranda A, Cardoso ES, Cardoso AS, Fregnani ER, Pereira CM, Correa ME, Almeida JP, Alves Fde A, Lopes MA, de Almeida OP (2005) Oral avascular bone necrosis associated with chemotherapy and bisphosphonate therapy. Oral Dis 11:365–369
Rabelo GD, Assuncao JN Jr, Chavassieux P, Soares HA, Alves FA, Lemos CA Jr (2015) Bisphosphonate-related osteonecrosis of the jaws and its array of manifestations. J Maxillofac Oral Surg 14:699–705
Saad F, Shore N, Van Poppel H, Rathkopf DE, Smith MR, de Bono JS, Logothetis CJ, de Souza P, Fizazi K, Mulders PF, Mainwaring P, Hainsworth JD, Beer TM, North S, Fradet Y, Griffin TA, De Porre P, Londhe A, Kheoh T, Small EJ, Scher HI, Molina A, Ryan CJ (2015) Impact of bone-targeted therapies in chemotherapy-naive metastatic castration-resistant prostate cancer patients treated with abiraterone acetate: post hoc analysis of study COU-AA-302. Eur Urol 68:570–577
Sim Ie W, Sanders KM, Borromeo GL, Seymour JF, Ebeling PR (2015) Declining incidence of medication-related osteonecrosis of the jaw in patients with cancer. J Clin Endocrinol Metab 100:3887–3893
Vidal-Real C, Perez-Sayans M, Suarez-Penaranda JM, Gandara-Rey JM, Garcia-Garcia A (2015) Osteonecrosis of the jaws in 194 patients who have undergone intravenous bisphosphonate therapy in Spain. Med Oral Patol Oral Cir Bucal 20:e267-272
Walter C, Grotz KA, Kunkel M, Al-Nawas B (2007) Prevalence of bisphosphonate associated osteonecrosis of the jaw within the field of osteonecrosis. Support Care Cancer 15:197–202
Yarom N, Shapiro CL, Peterson DE, Van Poznak CH, Bohlke K, Ruggiero SL, Migliorati CA, Khan A, Morrison A, Anderson H, Murphy BA, Alston-Johnson D, Mendes RA, Beadle BM, Jensen SB, Saunders DP (2019) Medication-related osteonecrosis of the jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J Clin Oncol 37:2270–2290
Hallmer F, Bjarnadottir O, Gotrick B, Malmstrom P, Andersson G (2020) Incidence of and risk factors for medication-related osteonecrosis of the jaw in women with breast cancer with bone metastasis: a population-based study. Oral Surg Oral Med Oral Pathol Oral Radiol 130:252–257
Acknowledgements
We greatly appreciate Takashi Yoshida, Shota Natsuyama, and Kenta Uchida, students of the School of Dental Medicine of Hokkaido University, for their cooperation in entering the data during the study. We also would like to thank Mami Saito from the hospital-based cancer registry for cooperating with the life prognosis survey. We thank Editage (www.editage.jp) for editing and reviewing this manuscript for English language.
Author information
Authors and Affiliations
Contributions
Hironobu Hata, Kenji Imamachi, and Michihiro Ueda conceptualized and designed the study. Hironobu Hata and Kenji Imamachi collected and assembled the data. Masashi Matsuzaka and Hiroaki Hiraga performed the statistical analysis of the data. Hiroaki Hiraga, Toshihisa Osanai, Toru Harabayashi, Katsuya Fujimoto, Satoshi Oizumi, and Masato Takahashi analyzed and interpreted the data. Hironobu Hata drafted the manuscript. Kazuhito Yoshikawa, Jun Sato, Yutaka Yamazaki, and Yoshimasa Kitagawa proofread the manuscript and provided insights to improve it. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed on human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This single-center, retrospective, observational study protocol and patient information were approved by the Hokkaido Cancer Center Hospital Ethics Review Board (clinical study number 02–10), and informed consent was waived by this board because of the retrospective design of the study. Permission to access raw data from hospital cancer registries for life prognosis survey was also granted by the ethics review board.
Consent for publication
Not applicable
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hata, H., Imamachi, K., Ueda, M. et al. Prognosis by cancer type and incidence of zoledronic acid–related osteonecrosis of the jaw: a single-center retrospective study. Support Care Cancer 30, 4505–4514 (2022). https://doi.org/10.1007/s00520-022-06839-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-022-06839-4