
Abstract
Purpose
Early recognition of neoplastic pericarditis (npe) is crucial for the planning of subsequent therapy. The aim of the present study was to construct the scoring system assessing the probability of npe, in the patients requiring pericardial fluid (pf) drainage due to large pericardial effusion.
Methods
One hundred forty-six patients, 74 males and 72 females, entered the study. Npe based on positive pf cytology and/or pericardial biopsy specimen was recognised in 66 patients, non-npe in 80. Original scoring system was constructed based on parameters with the highest diagnostic value: mediastinal lymphadenopathy on chest CT scan, increased concentration of tumour markers (cytokeratin 19 fragments—Cyfra 21-1 and carcinoembryonic antigen—CEA) in pf, bloody character of pf, signs of imminent cardiac tamponade on echocardiography and tachycardia exceeding 90 beats/min on ECG. Each parameter was scored with positive or negative points depending on the positive and negative predictive values (PPV, NPV).
Results
The area under curve (AUC) for the scoring system was 0.926 (95%CI 0.852–0.963) and it was higher than AUC for Cyfra 21-1 0.789 (95%CI 0.684–0.893) or CEA 0.758 (95%CI 0.652–0.864). The score optimally discriminating between npe and non-npe was 0 points (sensitivity 0.84, specificity 0.91, PPV 0.9, NPV 0.85).
Conclusion
Despite chest CT and tumour marker evaluation in pericardial fluid were good discriminators between npe and non-npe, the applied scoring system further improved the predicting of neoplastic disease in the studied population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Large pericardial effusion is defined, according to recent ESC guidelines, as at least 2 cm of echo-free space on echocardiography [1]. In 20–50% of patients, it is caused by neoplastic pericardial involvement [2–4], and in 10–25%, it is the first sign of neoplastic disease [1]. The most frequent primary sites of malignancy are the lung, breast and lymphoma/leukaemia [1, 3]. Adenocarcinoma is predominating histology in case of solid tumours presenting with pericardial metastases [5].
Malignant pericardial involvement is combined with poor prognosis, due to frequent development of cardiac tamponade and frequent relapse after pericardiocentesis [1, 3, 5–7]. Nevertheless, the recent advances of intrapericardial treatment followed by appropriate systemic chemotherapy prolonged the life expectancy of the patients with neoplastic pericardial disease [8–12].
Thus, the early recognition of neoplastic pericarditis (npe) is crucial for the planning of subsequent therapy. Our group published previously the paper concerning the diagnostic value of various clinical, radiological and biochemical parameters in the assessment of the probability of npe [13].
The aim of the present study was to construct the scoring system that could be used for the assessment of npe probability in the patients with large pericardial effusion, requiring pericardial fluid drainage.
Methods
The retrospective analysis concerned 430 patients with pericardial effusion, diagnosed and treated in the Department of Chest Medicine of the National Tuberculosis and Lung Diseases Research Institute in Warsaw, in the period of 1982–2008. One hundred ninety-one of them required pericardial fluid drainage. Forty-five of those were excluded due to lack of definite diagnosis of the cause of pericardial effusion. Thus, the study population consisted of 146 patients: 74 males and 72 females, median age 57 (21–88) years. Pericardiocentesis was performed in 57 patients, subxiphoid pericardiotomy in 38, pericardioscopy in 51.
The criteria of the recognition of npe used in this study were as follows:
-
1.
Neoplastic cells found in pericardial fluid cytological examination and/or
-
2.
Neoplastic infiltration present in the pericardial biopsy specimen
The criteria of the recognition of non-neoplastic pericarditis (non-npe) were as follows:
-
1.
Negative pericardial fluid cytology
-
2.
Negative pericardial fluid biopsy specimen
-
3.
No neoplastic disease present at the time of hospitalisation and during 1 year of subsequent follow-up.
Npe was recognised in 66 patients, non-npe in 80. The specific causes of pericardial effusion were listed in Table 1.
The applied diagnostic procedures consisted of clinical examination, 12-lead ECG, transthoracic echocardiographic examination (Siemens Accusuin Sequoia), chest X-ray and chest computed tomography (Somaton Sensation 16). Pericardial fluid (pf) assays consisted of morphology, biochemical parameters, microbiological cultures and tumour marker concentration (carcinoembryonic antigen—CEA and cytokeratin 19 fragments—Cyfra 21-1, by immunoenzymatic assay, Elecsys Roche).
Statistical analysis was performed in several steps:
-
1.
The assessment of diagnostic accuracy of various parameters in predicting npe. For continuous parameters, the receiver operator characteristic (ROC) curves were applied to find the optimal cut off values.
-
2.
For each parameter:
-
A table 2 × 2 was constructed to assess the sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV) and likelihood ratios (LR) at the cut off level. Only parameters with either sensitivity or specificity exceeding 0.60 were taken into account.
-
R-Spearman’s coefficient was computed to assess the correlation with neoplastic pericarditis.
-
3.
The construction of the scoring system based on individual parameters, with ranks depending on the importance of measured parameter determined with Spearman’s correlation test, and the predictive values of the analysed parameter.
-
4.
The calculation of total score for every individual patient in the study (by summing up the ranks for individual parameters). In case of lack of information concerning any procedure, the score of 0 points was introduced.
-
5.
The comparison of the diagnostic utility of the applied scoring system with the utility of single parameters (ROC curves and areas under curve—AUC).
Results
The diagnostic values of chosen parameters and their ranking of importance were presented in Table 2. The highest diagnostic sensitivity was combined with the presence of enlarged mediastinal lymph nodes, exceeding 10 mm in short diameter, in chest CT (sensitivity 0.93, specificity 0.7). The determinants with high diagnostic specificity but lower sensitivity were pf Cyfra 21-1 concentration with a cut off value of 95 ng/ml (specificity 0.95, sensitivity 0.64) and pf CEA concentration with a cut off value 5 ng/ml (specificity 0.94, sensitivity 0.65). Most sensitive determinants were HR on ECG exceeding 90/min and bloody pericardial effusion (sensitivity 0.82 and 0.86, respectively).
The scoring system based on importance of selected parameters and their PPV and NPV values was presented in Table 3. The Cyfra 21-1 pf values were divided into three ranges: >95, 35.5–95 and <35.5 ng/ml. Pf Cyfra 21-1>95 ng/ml and pf CEA >5 ng/ml were scored three points due to their highest PPV. Lack of enlarged mediastinal lymph nodes on chest CT was scored minus three points as it was combined with the highest NPV.
The individual scores, obtained in every patient included in the present study, were presented in Fig. 1. The optimal discriminating cut off value between npe and non-npe was calculated at 0 points: sensitivity 0.84, specificity 0.91, PPV 0.90, NPV 0.85. ROC curve revealed the high diagnostic utility of the applied scoring system, AUC 0.919 (95%CI 0.869–0.971) (Fig. 2). The AUC values for Cyfra 21-1 and CEA were lower than for scoring system: 0.789 (95%CI 0.684–0.893) and 0.758 (95%CI 0.652–0.864), respectively (Fig. 2).

Individual scores obtained in the participants of the study, depending on the aetiology of pericardial effusion

ROC curves of applied scoring system, comparing to pericardial fluid CEA and Cyfra 21-1 concentration
Discussion
Despite the progress concerning the recognition of neoplastic pericardial involvement, the indications for invasive diagnostics in pericardial disease are still under debate. The recent ESC recommendations state that pericardiocentesis is indicated for patients with clinical suspicion of malignancy in case of moderate to large pericardial effusion [1]. In such an occasion, the pf drainage should be the subsequent procedure of choice [1, 14]. In the remaining population of patients, the pericardiocentesis should be preserved for those with signs and symptoms of cardiac tamponade or with the suspicion of bacterial infection [1]. Moreover, pericardiocentesis is the recommended procedure of first choice, pericardioscopy with biopsy is adviced only in the reference centres [1]. Thus, according to experts opinion, the clinical management depends largely on the cause of pericardial involvement. This is justified by the fact that some types of pathology, like pericarditis in the course of thyroid disorders and immune or autoreactive pericarditis, are rarely progressing to cardiac tamponade, even in case of large amount of fluid [15]. In others, like neoplastic or infective pericarditis, the development of cardiac tamponade is very probable [15]. Thus, it is important in the patient with large pericardial effusion to assess the probability of npe.
Trying to address this issue, we aimed to construct the scoring system that would assess the probability of neoplastic disease in the patients with large pf, requiring drainage.
The system was based on six parameters: one measured on ECG (HR > 90/min), one echocardiographic (large effusion with the diastolic collapse of right ventricular or right atrial free wall), one radiological (the increased size of mediastinal lymph nodes in chest CT) and three parameters related to the characteristics of pf—its bloody character and increased tumour marker concentration (Cyfra 21-1 and CEA).
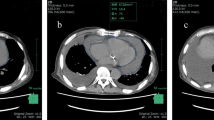
One of the best discriminators between npe and non-npe was lymphadenopathy on chest CT. The presence of enlarged mediastinal lymph nodes was 0.93 specific and 0.7 sensitive for npe. This observation may be due to the fact that most pericardial metastases develop via the mediastinal lymph nodes. The high diagnostic value of lymphadenopathy in chest CT for the recognition of npe was described also by Sun et al. [16]. Recently, Maggiolini et al. found that the workup including chest CT provided a significantly higher diagnostic yield than the workup based on chest X-ray [17]. Thus, in our opinion, chest CT should be listed as the procedure of first choice in the patient with large pe, independently on chest X-ray result, due to the fact that it demonstrates the structures not well visualised on chest X-ray, such as enlarged mediastinal lymph nodes, the foci of ground glass attenuation suspicious of neoplasia and also signs of aortic dissection. According to the recent ESC guidelines, chest CT is advised as the procedure of second choice, in case of suspected sequestration of pf, pericardial thickening or chest X-ray radiological changes (IIa C) [1].
The other change in clinical practice, proposed by our group, was the evaluation of tumour markers, pf Cyfra 21-1 and CEA, in every patient requiring pf drainage. ESC guidelines state that tumour markers evaluation in pf may be considered (IIa B), if npe is suspected. The choice of Cyfra 21-1 was based on its value in lung and breast cancer, which are the most frequent types of primary tumours in the patients with npe, and also in mesothelioma, which is a rare but difficult to diagnose pericardial malignancy [18]. CEA is the marker of choice for many adenocarcinomas [19]. The clinical value of tumour marker assessment in pf was reported by our group before [19], as well as by other investigators [20, 21].
The ongoing discussion in literature concerns the optimal cut off values: for CEA, the reported pericardial or pleural fluid cut offs were 5–8.5 ng/ml [19, 21, 22], for Cyfra 21-1 50–60 ng/ml [22, 23]. We proposed the three ranges of Cyfra 21-1 concentrations in pf, based on ROC curve analysis: >95 ng/ml—high probability of npe, 35.5–95 ng/ml—medium probability, <35.5 ng/ml—low probability of npe.
The AUC of CEA in the present study was 0.76, very similar to that reported by Karatolios et al. [21]. The AUC for Cyfra 21-1 in our study was 0.79.
Conclusion
Despite chest CT and tumour marker evaluation in pericardial fluid were good discriminators between npe and non-npe, the applied scoring system further improved the prediction of neoplastic disease in the studied population. The algorithm was better than any single parameter used in the diagnostic process. The prospective value of the applied scoring system is presently under evaluation.
References
Adler Y, Charron P, Imazio M et al (2015) 2015 ESC guidelines for the diagnosis and management of pericardial diseases. Eur Heart J 36:2921–2964
Maisch B, Ristic A, Pankuweit S (2010) Evaluation and management of pericardial effusion in patients with neoplastic disease. Prog Cardiovasc Dis 53:157–163
Orbach A, Schliamser JE, Flugelman MY, Zafrir B (2016) Contemporary evaluation of the causes of cardiac tamponade: acute and long-term outcomes. Cardiol J 23:57–63
Sanchez-Enrique C, Nunez-Gil IJ, Viana-Tejedor A et al (2016) Cause and long-term outcome of cardiac tamponade. Am J Cardiol 117:664–669
Kim SH, Kwak MH, Park S et al (2010) Clinical characteristics of malignant pericardial effusion associated with recurrence and survival. Cancer Res Treat 42:210–216
Rafique AM, Patel N, Biner S et al (2011) Frequency of recurrence of pericardial tamponade in patients with extended versus non-extended pericardial catheter drainage. Am J Cardiol 108:1820–1825
Numico G, Cristofano A, Occelli M et al (2016) Prolonged drainage and intrapericardial bleomycin administration for cardiac tamponade secondary to cancer-related pericardial effusion. Medicine(Baltimore) 95:e3273
Lestuzzi C, Bearz A, Lafaras C et al (2011) Neoplastic pericardial disease in lung cancer: impact on outcomes of different treatment strategies. A multicenter study. Lung Cancer 72:340–347
Tomkowski W, Wiśniewska J, Szturmowicz M et al (2004) Evaluation of intrapericardial cisplatin administration in cases with recurrent malignant pericardial effusion and cardiac tamponade. Supp Care Cancer 12:53–57
Maisch B, Ristic AD, Pankuweit S et al (2002) Neoplastic pericardial effusion: efficacy and safety of intrapericardial treatment with cisplatin. Eur Heart J 23:1625–1631
Burazor I, Imazio M, Markel G, Adler Y (2013) Malignant pericardial effusion. Cardiology 124:224–232
Li BT, Pearson A, Pavlakis N et al (2014) Malignant cardiac tamponade from non-small cell lung cancer: case series from the era of molecular targeted therapy. J Clin Med 4:75–84
Pawlak-Cieślik A, Szturmowicz M, Fijałkowska A et al (2012) Diagnosis of malignant pericarditis: a single centre experience. Kardiol Pol 70:1147–1153
El Haddad D, Iliescu C, Yusuf SW et al (2015) Outcomes of cancer patients undergoing percutaneous pericardiocentesis for pericardial effusion. JACC 66:1119–1128
Ristic AD, Imazio M, Adler Y et al (2014) Triage strategy for urgent management of cardiac tamponade: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 35:2279–2284
Sun JS, Park KL, Kang DK (2010) CT findings in patients with pericardial effusion: differentiation of malignant and benign disease. AJR 194:489–494
Maggiolini S, De Carlini CC, Ferri LA et al (2016) The role of early contrast-enhanced chest computed tomography in the aetiological diagnosis of patients presenting with cardiac tamponade or large pericardial effusion. Eur Heart J Cardiovasc Imaging 17:421–428
Paganuzzi M, Onetto M, Marroni P et al (2001) Diagnostic value of Cyfra 21-1 tumour marker and CEA in pleural effusion due to mesothelioma. Chest 119:1138–1142
Szturmowicz M, Tomkowski W, Fijałkowska A et al (2005) Diagnostic utility of Cyfra 21-1 and CEA assays in pericardial fluid for the recognition of neoplastic pericarditis. Int J Biol Markers 20:43–49
Koh KK, Kim EJ, Cho CH et al (1994) Adenosine deaminase and carcinoembryonic antigen in pericardial effusion diagnosis, especially in suspected tuberculous pericarditis. Circulation 89:2728–2735
Karatolios K, Pankuweit S, Maish B (2013) Diagnostic value of biochemical markers in malignant and non-malignant pericardial effusion. Heart Fail Rev 18:337–344
Antonangelo L, Sales RK, Cora AP et al (2015) Pleural fluid tumour markers in malignant pleural effusion with inconclusive cytologic results. Current Oncol 22:e336
Hsieh TC, Huang WW, Lai CL et al (2013) Diagnostic value of tumor markers in lung adenocarcinoma-associated cytologically negative pleural effusions. Cancer Cytopathol 121:483–488
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in the study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments. The written consent of agreement for all diagnostic procedures was obtained from every patient.
Source of funding
This study was supported by the National Tuberculosis and Lung Diseases Research Institute, project no 3.10.
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
ESM 1
(DOCX 13 kb)
Rights and permissions
About this article

Cite this article
Szturmowicz, M., Pawlak-Cieślik, A., Fijałkowska, A. et al. The value of the new scoring system for predicting neoplastic pericarditis in the patients with large pericardial effusion. Support Care Cancer 25, 2399–2403 (2017). https://doi.org/10.1007/s00520-017-3645-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-017-3645-4