
Abstract
Background
This study examined which patient- and physician-related factors influence guideline violations in adjuvant chemotherapy.
Patients and methods
In a prospective multi-center cohort study, patients with primary breast cancer were sampled consecutively over a period of four years (2009–2012). Patients completed a questionnaire prior to surgery and prior to adjuvant therapy. This questionnaire assessed health-related quality of life (QoL) using the European Organization for Research and Treatment of Cancer (EORTC) QLQ-C30, psychiatric co-morbidity with the Patient Health Questionnaire (PHQ), demographic characteristics (age, education), and the intensity of fear for chemotherapy.
After surgery, a multi-professional team discussed recommendation for adjuvant chemotherapy, and this decision was documented in a database together with the indication for chemotherapy according to the German S3 guideline. This multi-professional team was blinded to that algorithm-based decision. Six months later, it was documented whether the patient had received adjuvant chemotherapy or not.
Results
Altogether, 857 patients were included in the study. In 391 of these patients, the tumor board (TB) decided to recommend chemotherapy. The most important reasons for not recommending chemotherapy were somatic co-morbidity not allowing adjuvant chemotherapy and age >75 years.
Of these 391 patients, 73 (19 %) patients eventually did not receive chemotherapy. Deviations from the initial therapy decision were more frequent in older patients (≥75 years) with poor QoL. If the QoL was good, higher age was not related to deviation. There was some evidence that patients with higher education less frequently received chemotherapy (CT). Furthermore, if patients were very afraid of chemotherapy, deviations from the initial therapy decision were more likely. Co-morbidity and fear of CT were not related to the likelihood of deviating from the initial therapy decision.
Conclusion
Nineteen percent of patients eventually did not receive chemotherapy, despite guideline and TB recommendations. In these patients, this mainly occurred in association with poor QoL in elderly patients >75 years old. In the group with a chemotherapy recommendation, patients’ fear of chemotherapy is another factor preventing patients from undergoing adjuvant chemotherapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With approximately 75,000 newly diagnosed cases in Germany [1], breast cancer is the most common malignancy in women, and this is true throughout industrialized countries. The prognosis of breast cancer has improved dramatically over the last decades through implementation of multimodal therapy approaches and an improved understanding of tumor biology itself [2–4]. These improvements in breast cancer therapy have been driven by randomized breast cancer studies and the effort for quality assurance in breast cancer care, i.e., by implementing certified breast cancer centers [5]. Despite these tremendous efforts, only about 70 % of breast cancer patients undergo guideline-adherent therapy, resulting in unfavorable outcome parameters for patients with guideline violations [6–11]. Due to patient-related factors preventing guideline-adherent adjuvant therapy, there is no doubt that 100 % guideline adherence in a daily routine of collective breast cancer patients is impossible. Co-morbidities are deemed to be the most important factors, but there are several others, i.e., the patients’ preferences. Because of the high percentage of non-guideline-conforming treatments, there is an urgent need for an investigation into the reasons for deviating from therapy decisions in adjuvant breast cancer therapy. Understanding the factors influencing guideline adherence in breast cancer care is the basis for potential interventions which could improve therapy compliance in defined subgroups and thereby the patients’ outcomes [12]. There is convincing evidence that the oncological outcomes of breast cancer patients are substantially influenced by compliance with therapy decisions based on internationally developed guidelines.
The aim of the prospective BRENDA II study is therefore an assessment of patient- and physician-related factors that influence therapy decisions that prevent patients from undergoing guideline-adherent adjuvant treatment in primary breast cancer care. Another goal of the study is to define subgroups with potentially preventable guideline violations that could profit from targeted interventions to possibly improve guideline adherence and outcomes.
Patients and methods
In a prospective multi-center cohort study, patients with primary breast cancer were sampled consecutively over a period of four years (2009–2012) in four German breast cancer centers, all certified by the German Cancer Society. After a pilot phase (pre-planed) which started at the University Medical Center in Ulm, the three partner clinics started the BRENDA II study. Those patients who agreed to participate were sampled consecutively.
Patients were approached three times by interviewers (through a physician or a certified breast care nurse): before surgery (t1), before initiation of adjuvant treatment (t2), and after completion of adjuvant radio- and/or chemotherapy (t3).
Patients were eligible for this study if they had been diagnosed with primary breast cancer (histologically confirmed). Exclusion criteria were as follows: metastatic disease, recurrent disease, bilateral breast cancer, primary occult disease and phylloides tumor, inability to complete an interview, and no written informed consent.
After the patient’s consultation with her doctor, she was informed about the study by the doctor and asked to participate. If she agreed, the doctor handed over the first series of questionnaires and interviewed the patient. Follow-up interviews were performed by trained breast care nurses. We collected data at the University Medical Center in Ulm, Kempten Hospital, Memmingen Hospital, and Esslingen Hospital, all of which are breast cancer centers certified by the German Cancer Society. Ethical approval was obtained from the Ethics Committee of Ulm University.
After surgery, a multi-professional team discussed recommendation for adjuvant chemotherapy, and this decision was documented in a database together with the indication for chemotherapy according to the German S3 guideline. The multi-professional team was blinded to this algorithm-based decision. Six months later, it was documented whether the patient had received adjuvant chemotherapy or not.
Patients were included in the analysis when chemotherapy was indicated (high risk) or possible (intermediate risk) according to the guidelines and when the multi-professional team had decided to recommend chemotherapy.
Instruments
Clinical data were obtained from the medical records by trained data managers. Demographic data such as age and education were provided by the patient.
Co-morbid somatic diseases were documented and subsequently coded according to the Charlson co-morbidity index [13]. This index assigns weights to diseases depending on the risk of dying from the disease. A sum score ≥3 was considered to be a “severe somatic co-morbidity.”
We elicited psychiatric co-morbidity using the German version [14] of the Patient Health Questionnaire (PHQ) (13), a self-administered instrument assessing mental disorders according to the criteria of the ICD-10. It has been validated using the structured clinical interview [15] as the gold standard [14].
Quality of life (QoL) was ascertained using the European Organization for Research and Treatment of Cancer Core Instrument (EORTC QLQ-C30) [16]. This is a self-administered questionnaire assessing different dimensions of QoL. Patients were grouped as “poor QoL” (versus “good QoL”) if their global QoL score at t1 exceeded the 75th percentile of the general German population’s age- and sex-specific norms [17].
Fear of CT was measured by asking the patient: “How much are you afraid of chemotherapy?” (“not at all” to “very much” on a 4-point Likert scale). Doctor support was measured using the patient involvement in care scales (PICS) [18], adapted for Germany [19].
Adherence to the initial treatment decision was established by comparing the treatment decision, taken by the tumor board (TB) and documented by physicians, with the subsequently received CT.
We used the German national S3 guideline for diagnosis, treatment, and follow-up care in breast cancer (2008 version) [20] to classify CT indication. It has been previously demonstrated by Wolters et al. [21] that adjuvant CT recommendations do not differ in internationally validated evidence-based guidelines (see Table 1 online only). Risk group classification was based on the St. Gallen criteria [22].
Statistical analysis
Absolute and relative frequencies of treatment decisions regarding CT and subsequent application of CT were calculated.
Potential predictors of the tumor board decision and of deviations from this initial treatment decision were tested separately for the high- and intermediate-risk patients using multivariate logistic regressions. Effect modification was tested using likelihood ratio tests. If effect modification was present, stratum-specific odds ratios (OR) were calculated.
We considered the following variables as potentially relevant predictors: age at study entry (≥75 vs. <75 years), education (≥10 vs. <10 years of schooling), somatic co-morbidity (severe vs. no severe), psychiatric co-morbidity (yes vs. no), global QoL at t2 (poor vs. good QoL), and fear of CT at t1 (high vs. low). Variables were entered simultaneously into the model.
To address potential cluster effects of the different hospitals, we repeated the analyses with mixed effects modeling while including the hospital as a random effect.
As this is an explorative study, we have chosen not to employ the term “statistically significant” or to use a threshold p value, but rather to discuss differences that cannot be explained by random variation only based on the 95 % confidence intervals. Statistical analyses were performed using STATA 12.1 (StataCorp. 2011, College Station, TX: StataCorp LP).
Results
Sample
Eight hundred fifty-seven primary breast cancer patients were treated at the clinics during the study period and screened for inclusion criteria; 849 met the criteria and were contacted to participate in the study. Of these, 90 patients declined participation or could not be included due to dementia or language problems, and 759 patients completed the questionnaires. Non-participants were on average older (64 vs. 58 years), but the distribution of risk was equal in both the groups.
The majority of the participating patients had ductal invasive (n = 589) or lobular invasive carcinoma (n = 123). Tumor size (pT) was stage 1 in 378, stage 2 in 309, stage 3 in 43, stage 4 in 17, and unknown in 12 cases. Lymph nodes were infiltrated in 248 patients. In seven patients, both breasts were affected by cancer simultaneously. One hundred patients were HER2/neu-positive, and further 104 patients were estrogen receptor-negative.
Guideline recommendation
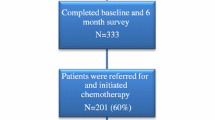
Based on the St. Gallen (2007) criteria and guideline recommendations, we identified 241 high-risk patients with a clear indication for adjuvant chemotherapy and 537 intermediate-risk patients, for whom it was possible but not mandatory to indicate adjuvant chemotherapy according to the guideline (see Figure 1). In 15 cases, a classification was not possible due to missing data.

Tumor board decisions according to guideline-based indication for chemotherapy (including all the risk groups)
Tumor board decision
In 395 cases, the tumor board decided to apply CT; in 430 cases, they did not see an indication for CT; and in 32 cases, no information about the tumor board decision was available (Fig. 1, Table 2).
In the high-risk patients, the tumor board decided to apply CT less frequently in patients aged ≥75 years (odds ratio (OR) 0.2; 95 % CI 0.0–0.7) and more frequently in patients with a high fear of CT (OR 2.8; 95 % CI 1.0–8.0).
In the patients with intermediate risk, the tumor board’s decision to apply CT was less often in patients aged ≥75 (OR 0.4; 95 % CI 0.2–0.8) and in patients with severe somatic co-morbidity (OR 0.3; 95 % CI 0.1–0.8).
There was no evidence that patient-related factors like psychiatric co-morbidities, quality of life (QoL), or education were related with the tumor board decision (see Table 2).
Only the high- and intermediate-risk patients (n = 778) were carried on to further analysis. In 391 of these patients, the interdisciplinary tumor board had decided to apply adjuvant chemotherapy. In 363 cases, they decided against CT, and in 24 cases, no data about the tumor board decision were available.
Application of adjuvant chemotherapy
Of those with an indication for adjuvant chemotherapy according to the guideline and the tumor board (n = 391), 19 % (n = 73) did not eventually receive adjuvant chemotherapy. Ten percent of the high-risk and 28 % of the intermediate-risk group did not receive adjuvant chemotherapy (see Table 3 and Fig. 1). In the different centers, the percentage of patients not receiving chemotherapy was 6, 8, 14, and 21 % respectively.
In the high-risk patients with a TB decision to apply CT (n = 205), deviations from the initial treatment decision were more likely if patients were old (≥75 years) and simultaneously reported poor QoL (OR 0.003; 95 % CI 0.0001–0.1). If patients were old but had good QoL, no such effect was observed (OR 0.1; 95 % CI 0.0–2.4). Patients with higher educational status more often declined adjuvant chemotherapy (OR 0.3; 95 % CI 0.1–1.1). Co-morbidity and fear of chemotherapy were not related to the application of chemotherapy in the high-risk patients (see Table 4)
In the intermediate-risk patients with a TB decision to apply CT (n = 186), we did not find any effect modification of age by QoL on chemotherapy application. Here, neither age (OR 0.6; 95 % CI 0.1–2.8) nor QoL (OR 1.5; 95 % CI 0.6–3.5) was related to the eventual treatment given. Similarly, education and co-morbidity were not related to treatment application. However, if the patients were very afraid of chemotherapy, they received it less frequently (OR 0.4; 95 % CI 0.2–0.9) (see Table 4).
To address potential cluster effects of the different hospitals, we repeated these analyses with mixed effects modeling, including the hospital as a random effect. This did not change the effect estimates.
Discussion
Our goal is to improve guideline adherence and, subsequently, the prognosis of our breast cancer patients by investigating and understanding predictors of deviations from guideline recommendations and to define patient subgroups that could profit from a targeted intervention to improve guideline adherence.
The prospective BRENDA II study observed that tumor board decisions on chemotherapy are influenced by the somatic co-morbidities and the age of the breast cancer patients. About 19 % of the patients with an indication for adjuvant chemotherapy who have been deemed suitable by the tumor board decline adjuvant chemotherapy. The main patient-related factors driving this decision are age, poor QoL, and patients’ fear of chemotherapy.
Our data show that one out of five breast cancer patients does not follow guideline recommendation and tumor board decision concerning adjuvant chemotherapy, which subsequently is associated with an unfavorable prognosis, as demonstrated in several observational studies investigating guideline adherence in breast cancer care [6–11]. Translating clinical research in our daily routine for breast cancer patients is a major challenge for clinical oncologists with the goal to improve prognosis for our patients. The BRENDA II study demonstrates that further research investigating physician- and patient-related factors preventing patients from guideline-adherent adjuvant treatment is needed in order to potentially define subgroups that could profit from interventions improving their guideline adherence: these interventions could be further detailed information or additional time for shared decision-making with their treating physicians [12]. However, there is also no doubt that 100 % guideline adherence is not achievable in a routine cohort of patients with somatic and psychiatric co-morbidities. Of course, several other factors like household income, access to cancer care, etc. may influence treatment decisions in addition to the ones measured in our study, and we were not able to assess all potential predictors.
There are only few studies that investigated non-initiation of adjuvant chemotherapy in early breast cancer [23]. Neugut et al. [23] investigated reasons for non-initiation of adjuvant chemotherapy focusing on physician-related factors and tumor board decisions. In addition to these studies, the focus of BRENDA II is on patients’ decisions concerning adjuvant chemotherapy following the tumor board decision. There are several other studies investigating the frequency of non-compliance in adjuvant endocrine therapy [12, 24–26] but neither of them investigated potential predictors of this decision making in adjuvant therapy. The BRENDA I study demonstrated that guideline adherence is significantly associated with improved survival parameters in several breast cancer subtypes [6–10]. We therefore assume that these factors (somatic co-morbidity, age, QoL, etc.) influence therapy decisions and, respectively, negatively influence outcome parameters.
A major strength of our study is that trained physicians/breast care nurses interviewed participants, which substantially improved documentation quality [27] of the data. In addition, using a prospective design reduced the likelihood of information bias (in patients and physicians alike). Physicians were also blinded to the guideline-based algorithm regarding chemotherapy. This made their decision independent of this information. The multi-center design used to enroll patients, and the consecutive order of patient inclusion increased the representativeness and external validity of our findings.
We used internationally validated standardized instruments to measure predictors of treatment decision and treatment application, which again reduced information bias and increased comparability of results.
However, there are also some limitations we would like to mention. First of all, there are several other factors potentially influencing patients’ therapy decisions (i.e., rural/urban areas, negative experiences with medical services, etc.) that we were not able to assess in our study because we had to limit the questions asked to patients. Therefore, this weakness should be taken into account when interpreting the results.
Currently, because of the short follow-up, we cannot demonstrate outcome results, and we therefore only have retrospective evidence from the BRENDA I study demonstrating that guideline adherence is associated with favorable outcome parameters [6–10]. Nevertheless, currently, we cannot prospectively demonstrate that guideline adherence is associated with improved survival parameters.
This is the first prospective study investigating the frequency and reasons for deviations from therapy decisions concerning adjuvant chemotherapy in primary breast cancer. We put all our effort into improving our patients’ outcomes, but a daily routine cohort of patients differs significantly from a selected cohort in a randomized trial. Of course, not 100 % of patients will be able to follow guideline-adherent adjuvant treatment due to non influenceable factors like somatic co-morbidities. However, there is an urgent need for a deeper understanding of preventable or influenceable factors that prevent patients from adhering to guidelines, for example the fear of chemotherapy. This could be targeted by educating patients and the public about modern methods of chemotherapy and about supportive care, for example. We cannot emphasize enough that improving patients’ compliance in our daily routine cancer services would improve outcome parameters.
References
Robert-Koch-Institute, Breast cancer incidence in Germany 2014, http://www.rki.de/Krebs/DE/Content/Krebsarten/Brustkrebs/brustkrebs_node.html. Accessed 1 Jul 2015.
Van Ewijk R, Schwentner L, Wöckel A, König J, Kreienberg R, Blettner M (2013) Trends in patient characteristics, treatment and survival in breast cancer in a non-selected retrospective clinical cohort study of 2,600 patients. Arch Gynecol Obstet 287(1):103–10
Van Luijt PA, Fracheboud J, Heijnsdijk EA, den Heeten GJ, de Koning HJ, National evaluation team for breast cancer screening in Netherlands study groups (NETB) (2013) Nation-wide data on screening performance during the transition to digital mammography: observations in 6 million screens. Eur J Cancer 49(16):3517–25
Wo JY, Chen K, Neville BA, Lin NU, Punglia RS (2011) Effect of very small tumor size on cancer-specific mortality in node-positive breast cancer. J Clin Oncol 29(19):2619–27
Kowalski C, Ferencz J, Brucker SY, Kreienberg R, Wesselmann S. Quality of care in breast cancer centers: results of benchmarking by the German Cancer Society and German Society for Breast Disease. Breast 2014; doi: 10.1016/j.breast.2014.11.014
Hancke K, Denkinger MD, König J, Kurzeder C, Wöckel A, Herr D et al (2010) Standard treatment of female patients with breast cancer decreases substantially for women aged 70 years and older: a German clinical cohort study. Ann Oncol 21(4):748–53
Schwentner L, Wolters R, Wischnewsky MB, Kreienberg R, Wöckel A (2010) Survival of patients with bilateral versus unilateral breast cancer and impact of guideline adherent adjuvant treatment: a multi-centre cohort study of 5292 patients. Breast 21(2):171–7
Schwentner L, Wolters R, Koretz K, Wischnewsky MB, Kreienberg R, Rottscholl R et al (2012) Triple-negative breast cancer: the impact of guideline-adherent adjuvant treatment on survival—a retrospective multi-centre cohort study. Breast Cancer Res Treat 132(3):1073–80
Wolters R, Wöckel A, Janni W, Novopashenny I, Ebner F, Kreienberg R et al (2013) Comparing the outcome between multicentric and multifocal breast cancer: what is the impact on survival and is there a role for guideline-adherent adjuvant therapy? A retrospective multi-center cohort study of 8,935 patients. Breast Cancer Res Treat 142(3):579–90
Wöckel A, Wolters R, Wiegel T, Novopashenny I, Janni W, Kreienberg R et al (2014) The impact of adjuvant radiotherapy on the survival of primary breast cancer patients: a retrospective multicenter cohort study of 8935 subjects. Ann Oncol 25(3):628–32
Hebert-Croteau N, Brisson J, Latreille J, Rivard M, Abdelaziz N, Martin G (2004) Compliance with consensus recommendations for systemic therapy is associated with improved survival of women with nodal negative breast cancer. J Clin Oncol 22:3685–93
Ziller V, Kyvernitakis I, Knöll D, Storch A, Hars O, Hadji P (2013) Influence of a patient information program on adherence and persistence with an aromatase inhibitor in breast cancer treatment—the COMPAS study. BMC Cancer 13:407
D‘Hoore W, Sicotte C, Tiquin C (1993) Risk adjustment in outcome assessment: the Charlson comorbidity index. Methods Inf Med 32:382–7
Löwe B, Spitzer RL, Zipfel S, Herzog W (2002) PHQ-D Gesundheitsfragebogen für Patienten. Pfizer, Manual. Karlsruhe
Spitzer RL, Williams J, Kroenke K (1999) Prime MD today. Evaluation of metal disorders. Pfizer, New York
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ et al (1993) The European Organization For Research And Treatment Of Cancer QLQ-C30—a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–76
Schwarz R, Hinz A (2001) Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. EurJ Cancer 37:1345–51
Lerman CE, Brody DS, Caputo GC, Smith DG, Lazaro CG, Wolfson HG (1990) Patients’ perceived involvement in care scale: relationship to attitudes about illness and medical care. J Gen Intern Med 5:29–33
Scheibler F, Freise D, Pfaff H (2004) Die Einbeziehung von Patienten in die Behandlung—Validierung der deutschen PICS-Skalen. J Publ Health 12:199–209
Kreienberg R, Kopp I, Albert U, Bartsch H, Beckmann MW, Berg D, et al. Interdisciplinary S3 guideline for diagnosis and therapy of breast cancer in women. German cancer society 2008
Wolters R, Regierer AC, Schwentner L, Geyer V, Possinger K, Kreienberg R et al (2012) A comparison of international breast cancer guidelines—do the national guidelines differ in treatment recommendations? Eur J Cancer 48(1):1–11
Goldhirsch A, Wood WC, Gelber RD, Coates AS, Thürlimann B, Senn HJ (2007) Progress and promise: highlights of the international expert consensus on the primary therapy of early breast cancer 2007. Ann Oncol 18(7):1133–44
Neugut AI, Hillyer GC, Kushi LH, Lamerato L, Leoce N, Nathanson SD et al (2012) Noninitiation of adjuvant chemotherapy in women with localized breast cancer: the breast cancer quality of care study. J Clin Oncol 30(31):3800–9
Barron TI, Cahir C, Sharp L, Bennett K (2013) A nested case-control study of adjuvant hormonal therapy persistence and compliance, and early breast cancer recurrence in women with stage I–III breast cancer. Br J Cancer 109:1513–21
Harbeck N, Blettner M, Hadji P, Jakisch C, Lück HJ, Windermuth-Kieselbach C et al (2013) Patient’s Anastrozole Compliance to Therapy (PACT) program: baseline data and patient characteristics from a population-based, randomized study evaluating compliance to aromatase inhibitor therapy in postmenopausal women with hormone-sensitive early breast cancer. Breast Care (Basel) 8(2):110–20
Banning M (2012) Adherence to adjuvant therapy in post-menopausal breast cancer patients: a review. Eur J Cancer Care 21(1):10–9
Schouten LJ, Jager JJ, van den Brandt PA (1993) Quality of cancer registry data: a comparison of data provided by clinicians with those of registrations personnel. Br J Cancer 68(5):974–7
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study and the BRENDA project have been approved by the ethics committee of the University of Ulm.
Conflict of interest
The authors declare that they have no competing interests.
Funding source
This work was supported by the German Federal Ministry of Education and Research (BMBF-Grant-01ZP0505).
Rights and permissions
About this article

Cite this article
Schwentner, L., Van Ewijk, R., Kühn, T. et al. Exploring patient- and physician-related factors preventing breast cancer patients from guideline-adherent adjuvant chemotherapy—results from the prospective multi-center study BRENDA II. Support Care Cancer 24, 2759–2766 (2016). https://doi.org/10.1007/s00520-016-3088-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-016-3088-3