
Abstract
Purpose
A systematic review and a meta-analysis were performed to assess the associations between change over time in physical activity and weight and quality of life and mortality in colorectal cancer patients.
Methods
The PubMed, Embase, and Cochrane Central Register of Controlled Trials databases were searched for English language articles published between January 1, 1990 and October 7, 2013. These articles reported results for changes in physical activity and body weight, assessed at pre- to post-diagnosis or at post-diagnosis only. A random effects model was used to analyze pooled quality of life and mortality estimates.
Results
Seven eligible studies were identified and analyzed. Increased physical activity was associated with higher overall quality of life scores (N = 3 studies; standardized mean difference (SMD) = 0.74, 95 % confidence interval (CI) = 0.66–0.82), reduced disease-specific mortality risk (hazard ratio (HRpooled) = 0.70, 95 % CI = 0.55–0.85), and reduced overall mortality (HRpooled = 0.75, CI = 0.62–0.87) (N = 2 studies). Weight gain was not associated with disease-specific (HRpooled = 1.02, CI = 0.84–1.20) or overall (HRpooled = 1.03, CI = 0.86–1.19) mortality (N = 3 studies).
Conclusions
Increased physical activity was associated with improved quality of life, a reduced risk of colorectal cancer, and overall mortality rate. Given the paucity of the literature published on this topic, this finding should be interpreted with caution.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Worldwide, colorectal cancer is ranked among the leading types of cancer that affect both women and men. In 2012, approximately 1.4 million new cases, or 10 % of all cancer sites, were of colorectal origin [1]. Advances in early detection, and in surgical and medical treatment, have led to improved survival of patients. In the USA, the relative 5-year survival rate is 65 % for all stages combined and is as high as 90 % for localized tumors [2]. In the USA, 1.1 million people were previously estimated to be living with a previous diagnosis of colorectal cancer [2]. In the UK, colorectal cancer survivors accounted for 26 % of all cancer survivors in 2008 [3]. The number of survivors is expected to increase further as a consequence of the implementation of screening programs.
Cancer survivors are usually encouraged to engage in healthier lifestyles that have positive effects on prognosis and survival [4–6]. A growing body of supporting evidence describes the beneficial effects of physical activity on health outcomes among cancer survivors [7–11]. For colorectal cancer survivors, suggestive evidence for the association between higher physical activity and lower mortality rates has emerged from studies that evaluated pre-diagnosis or post-diagnosis health behaviors of survivors [12, 13]. A higher amount of recreational physical activity before and after diagnosis is associated with lower mortality [14], and longer leisure time spent sitting is associated with a higher risk of death [15]. Some studies suggest an association between body weight of colorectal cancer survivors and survival probability [7]. Pre-diagnosis obesity is associated with poor overall and colorectal cancer-specific survival [16, 17]. A body mass index ≥35 kg m−2 at diagnosis is associated with an increased risk of recurrence of colorectal cancer and death [18].
Improvements in quality of life in colorectal cancer survivors are also positively associated with physical activity [19–22]. Healthy lifestyle, particularly physical activity, is also increasingly promoted to cancer survivors in an attempt to manage the psychosocial and physical consequences of the cancer and its treatment, which can negatively affect quality of life [8, 23–25]
There is growing evidence showing that physical inactivity and high body weight are associated with higher mortality and lower quality of life among colorectal cancer survivors. Yet, most studies have focused on assessing the amount or categories of physical activity and weight at one point of time with cancer outcome rather than the impact of actual changes of physical activity or body weight over time. While it is recommended that cancer survivors increase physical activity or made healthy changes in their body weight, we actually do not know if these changes will necessarily improve cancer-related survival and quality of life. The evidence regarding a possible association of actual change over time in these behaviors with mortality and quality of life has not been summarized. Blanchard et al. [26] attempted to quantify the change in the amount of physical activity associated with quality of life, but this study included survivors of different cancer types, predominantly breast cancer survivors.
The purpose of this study was to systematically review the literature reporting on longitudinal changes in physical activity and weight on quality of life and mortality in colorectal cancer survivors.
Methods
Search strategy and study selection
We performed a literature search to identify empirical studies on the association of changes in physical activity and weight, overweight, and/or obesity with quality of life (i.e., physical, social, emotional, and functional well-being of the survivors) and mortality (i.e., disease-specific and overall mortality) among survivors. Searches of eligible English language articles were performed using the Medline (PubMed), Embase, and Cochrane Central Register of Controlled Trials databases. The search included all peer-reviewed articles that were published by October 7, 2013. Electronic search strategies were developed using the terms “(colorectal neoplasms AND survivors) OR colorectal cancer surviv* OR colorectal tumor surviv* OR colorectal tumour surviv* OR colorectal neoplasm surviv* OR colonic cancer surviv* OR colonic tumor surviv* OR colonic tumour surviv* OR colonic neoplasm surviv* and one of the following terms: lifestyle, change* OR modif*, life change events OR life change event*, exerci* OR physical activity OR motor activity, body weight OR body weight* OR body mass*, or quetelet OR body mass index OR body mass index.”
Survivors were defined as individuals diagnosed with cancer from the time of initial diagnosis and followed through their lifetime, using the definition of the National Coalition of Cancer Survivorship adopted by the Office of Cancer Survivorship Research of the National Cancer Institute [27].
We considered retrospective and prospective cohort studies, case control studies, and randomized controlled trials (RCTs) in which ancillary data were reported as observational studies. Physical activity and body weight were required to be assessed at least twice, before and after diagnosis, or during two follow-up periods after diagnosis. We included studies in which quality of life, measured by standardized instruments, and overall mortality, disease-specific mortality, disease-free or recurrence-free survival were the outcome measures. Studies retained eligibility if they also reported on adult men and women, aged ≥18 years, and diagnosed with a primary colorectal cancer (malignant neoplasm of the colon, rectum, or both). We excluded studies that included patients with familial adenomatous polyposis, hereditary non-polyposis colorectal cancer, or cancers that were not of colorectal cell origin (e.g., melanoma, Hodgkin’s disease).
All authors participated in screening of the retrieved titles and review of the article abstracts. Disagreements were discussed by the group and resolved by consensus. SJO and IS selected the full papers for inclusion in the review. Any final discrepancies were resolved by consensus between these two coauthors or after consultation with the entire group of coauthors.
Data extraction
Study characteristics included in the analysis were extracted independently by SJO and IS. The extracted data included the title, the first author’s name, publication year, type of design, study population origin, period of diagnosis, sample size, response rate, and age at diagnosis. Data on definitions and measures of changes in physical activity and body weight, comparison groups, quality of life scales, and unit outcomes (quality of life scores, mean differences, or mortality hazard ratios (HRs), 95 % confidence intervals (CI), and standard deviation or standard error of the mean values) were also extracted.
Quality assessment
The methodological quality of each selected study was assessed using a 10-item checklist adapted from Mols et al. [28] (Table 1). Zero points were assigned to an item if it did not meet a criterion or was not sufficiently described. If the criteria were all met, the study was assigned the maximum value of 14 points. Studies that scored ≥75 % of the maximum score (≥11 points) were considered to be of “high quality.” Studies that scored 50–75 % of the maximum score (7–10 points) were rated as “adequate quality.” Studies that scored <50 % (≤6 points) were considered to be of “low quality.”
Statistical analysis
If ≥2 studies were available, the quality of life scores or adjusted HRs with the corresponding standard deviation or CI values that were measured after the changes in physical activity or body weight were pooled. Change was defined as the difference in the individual’s physical activity level or weight between the baseline and the last reported measurement for the time period used in the study (i.e., pre-diagnosis to post-diagnosis or only post-diagnosis). Changes in physical activity level were conceptualized as an increase, decrease, or no change in the amount of physical activity between the two time points (Table 2), or an increase from a low to a higher category of physical activity level, a decrease from a high to a lower category or no change in category between the two time points (Table 2). In the meta-analysis, we compared increased with decreased (or unchanged) physical activity level (reference) and weight gain with stable weight (reference). For the meta-analysis, we considered only weight gain over time, as weight loss in cancer survivors can be unintentional and unrelated to changes in lifestyle, e.g., due to taste alterations [29], anorexia, and wasting syndrome [30].
For studies that reported quality of life data, we calculated the standardized mean difference (SMD) and compared patients that increased physical activity level (or maintained at active level) with patients that decreased physical activity level during follow-up or were unchanged (this was for one study in the group of inactive/insufficiently active at baseline, [31]) (Table 2).
For the studies that reported mortality data, the reported adjusted HRs with corresponding CIs were pooled, and physical activity or weight gain were compared with the reference group (no change or decrease).
Pooled effect estimates were calculated using a random effects model that accounted for within-study and between-study variation [32]. Heterogeneity of effects across studies was tested using the I 2 statistic, which represented the percent of total variation across studies that was attributable to heterogeneity rather than to chance. The Chi-square statistic was also used to test heterogeneity. An I 2 statistic index >50 % and a Chi-square p value <0.10 indicated the presence of substantial heterogeneity in the data.
Small study effects (e.g., publication bias) were assessed using the Egger’s regression asymmetry test [33] and funnel plot analysis. These effects were assumed to be present for p values <0.10. When they were present, the HR values were naturally logarithm-transformed, and standard errors calculated using the Greenland formula [34].
All statistical analyses were performed using STATA 12.0 software (StataCorp, College Station, TX, USA).
Results
Selection of studies
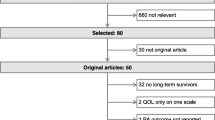
The search of the three databases yielded 2,053 article titles (excluding 1,406 duplicates) (Fig. 1). A total of 1,891 articles were excluded after screening the titles, and 110 were excluded after abstract reviews. Forty-five of the remaining 52 articles were excluded after reading the full text publications. Seven articles were included in the current review. Three (43 %) were ranked as high quality [31, 35, 36], and four (57 %) were ranked as adequate quality [37–40].

Flow chart, selection of articles
Characteristics of the studies
Descriptions of the characteristics of the studies described in the included articles are presented in Table 2. Except for one article [37], all were published after 2003. One article included results of an ancillary analysis of an RCT using data combined from two study arms [38]. Two articles reported studies of the same research group, using data from the same study cohort, but each examined a different endpoint (quality of life [31], mortality [35]). Quality of life was the endpoint in three reported studies [31, 37, 38], using the Functional Assessment of Cancer Therapy-Colorectal (FACT-C), which measures colorectal cancer-specific quality of life. Mortality was the endpoint in four reported studies [35, 36, 39, 40].
In five articles, the association of changes over time in physical activity level with quality of life or mortality was reported. Three articles focused on changes in weight and mortality over time. No articles examined associations between weight change and quality of life.
Both weight and physical activity were self-reported. In one study, physical activity was measured retrospectively [37]. The instruments for the assessment of physical activity varied among the studies. The Leisure Score Index (LSI) of Godin Leisure-Time Exercise Questionnaire was used in the studies reported by Courneya et al. [37, 38], while the Active Australia Survey was used in the study of Lynch et al. [31]. Meyerhardt et al. [39] used the self-reported data on time spent for walking and vigorous activities of the Nurses’ Health Study. Physical activity measures were quantified as the number of metabolic equivalents (MET) per week, the number of minutes of physical activity per week, and meeting or not meeting a guideline for moderate to strenuous intensity exercise per week. A substantial proportion of survivors had a decline in physical activity during treatment and merely returned to pretreatment levels in the long term. Courneya et al. [37] found that there was a decrease in the proportion of physically active (≥16 MET week−1) survivors. At pre-diagnosis, 61.5 % were physically active. This proportion declined to 36.9 % during treatment and to 53.1 % post-treatment. A decrease in the proportion of survivors that were sufficiently active (≥150 min week−1) was observed in the Lynch et al. [31] cohort study. This proportion declined from 53 % at pre-diagnosis to 32 % at 6-month post-diagnosis, then increased to 37 % at 12 months and 39 % at 24-month post-diagnosis. Pooled HR estimates were not calculated for the association between decreased physical activity and mortality because these data were published in only one article [39]. A considerable proportion of survivors (64 % in the Meyerhardt et al. [40] and 27.8 % in the Baade et al. [35] studies) gained ≥5 kg after completion of treatment.
Change in physical activity and quality of life
Patients that increased their physical activity level or remained active throughout the diagnosis and treatment phases had significantly higher quality of life scores than patients with reduced physical activity levels after treatment. In the individual studies, there was a clear association between change in physical activity level and quality of life when patients who increased, decreased, or did not change their activity levels were compared (Table 2). In their 1997 study, Courneya et al. [37] found that patients who maintained their pre-diagnosis activity levels had higher FACT-C scores compared with patients who decreased their activity levels. In the ancillary study performed within the RCT, Courneya et al. [38] found that FACT-C scores were lower in individuals that were less fit at the end of follow-up. FACT-C scores increased 4.3 points in individuals that increased their cardiovascular fitness, while a decrease of 2.2 points was observed in those who remained unchanged or showed a decrease in cardiovascular fitness. Fitness was assessed by the treadmill test. Lynch et al. [31] measured the intra-individual change in physical activity and found an increase of approximately 8 FACT-C points, from 109.9 (standard deviations (SD) = 10.5) to 117.9 (SD = 10.9) points in individuals who were inactive or insufficiently active at baseline but became more active during follow-up.
Figure 2 presents the results for the forest plot for the association between changes in physical activity level and quality of life. The meta-analysis revealed that compared with decreased physical activity post-diagnosis and/or post-treatment, increased physical activity was associated with significantly higher quality of life scores (SMD = 0.74 (CI = 0.66–0.82) with no heterogeneity between the studies (I 2 = 16.5 %, p value = 0.302)). The analysis of publication bias indicated that no bias was present (Egger’s test; p value = 0.701).

Forest plot of the association between change in physical activity and quality of life among colorectal cancer survivors. The squares indicate the study-specific point estimates. The width of the horizontal lines indicates the 95 % confidence intervals (CIs). The diamonds represent the pooled estimates. Maintainers indicate those active throughout study period and permanent relapsers those active pre-diagnosis, but inactive both during treatment and post-treatment (Courneya, 1997); unchanged physical activity indicates those inactive/insufficiently active at baseline (Lynch 2008)
Change in physical activity and survival
There was a significant association between increases in physical activity in the post-diagnosis period and reduced colorectal cancer death, but increases from pre-diagnosis to 5-month post-diagnosis were not significant (Table 2, Fig. 3). However, the overall pooled HR estimate of 0.70 (CI = 0.55–0.85) indicated that the change was significant. The tests for heterogeneity among the studies for the effect of increased physical activity on disease-specific mortality were not significant (I 2 = 48.5 %, p value = 0.101). A similar pattern was observed for overall mortality (pooled HR = 0.75, CI = 0.62–0.87; I 2 = 56.7 %, p value = 0.055; Fig. 3).

Forest plot of the association between increase in physical activity and disease-specific and overall mortality among colorectal cancer survivors. The squares indicate the study-specific point estimates. The width of the horizontal lines indicates the 95 % confidence intervals (CIs). The diamonds represent the pooled estimates. Reference group in Meyerhardt et al. (2006): unchanged activity category (MET h/week); reference group in Baade et al. (2011): unchanged or decreased in physical activity level
The results of the Egger’s test indicated that no publication bias (p value = 0.885) was present in the studies that examined the effect of physical activity on disease-specific mortality.
Weight gain and survival
The Meyerhardt et al. [40] study was the only study that assessed the impact of change in body weight on disease-free and recurrence-free survival (Table 2). Recurrence was defined as tumor recurrence, occurrence of a new primary colon tumor, or death from any cause. These survival endpoints were not included in the comparisons of the three studies that reported data on weight and mortality changes. In the studies included, there was a tendency for a U-shape for the association between change in weight and either disease-specific or overall mortality (Table 2). As aforementioned, we considered only weight gain over time for the meta-analysis, as weight loss in cancer survivors can be unintentional and unrelated to health behaviors. Despite a tendency toward an association between weight gain from pre- to post-diagnosis and mortality, weight gain did not significantly affect disease-specific mortality (pooled HR = 1.02, CI = 0.84–1.20; I 2 = 15.6 %, p value = 0.315) or overall mortality (pooled HR = 1.03, CI = 0.86–1.19; I 2 = 0.0 %, p value = 0.886) (Fig. 4).

Forest plot of the association between weight gain and disease-specific and overall mortality among colorectal cancer survivors. The squares indicate the study-specific point estimates, and the width of the horizontal lines indicates the 95 % confidence intervals (CIs). The diamonds represent the pooled estimates. Reference group in Meyerhardt et al. (2008) and Baade et al. (2011): ±2 kg; reference group in Campbell (2012): weight stable
The results for the Egger’s test indicated that no publication bias was present (p values = 0.249).
Discussion
We systematically reviewed the literature for studies examining the association between longitudinal change in physical activity level and weight and quality of life and mortality among colorectal cancer patients. Despite the general focus on adoption of healthier lifestyles and its effect on quality of life for cancer survivors, we retrieved only seven studies that examined this issue. Increase in physical activity level was associated with an improved quality of life and improved prognosis. There was no association between weight gain and mortality among survivors.
Two recent systematic reviews and meta-analyses of RCTs also concluded that physical activity interventions during active treatment and post-treatment may improve quality of life of cancer survivors [10, 11], but this finding was mostly based on RCTs conducted among breast cancer survivors. Two recently published RCTs evaluating an intervention aimed at increasing physical activity in colorectal cancer survivors failed to find an intervention effect on quality of life despite significant improvements in physical activity level in the intervention group compared with the control group [41, 42]. Hawkes et al. [42] found that participation in the CanChange intervention program (Cancer Council Queensland, Brisbane, Australia) yielded significant between-group difference in physical activity at 12-month post-diagnosis, which did not translate into differences in quality of life characteristics between the intervention and control groups. Similarly, Pinto et al. [41] found no significant between-group differences in quality of life characteristics despite increases in physical activity and fitness in the intervention group, which also received telephone counseling to support physical activity. Assessment of individual change would probably have been more likely to capture the effects of change in physical activity level on quality of life in these RCTs. Based on the results of three observational studies, in this current meta-analysis, we did find a positive association between an increase in physical activity level and quality of life. These contrasting findings from the observational studies might have been a consequence of selection bias as the RCTs probably included colorectal cancer survivors who experienced fewer disease-related symptoms or physical side effects of treatment or survivors who were more able and willing to engage into physical activity post-treatment. Pre-diagnosis exercise and exercise intention were found to be significant determinants of post-treatment physical activity, which was predominantly mediated by the individual’s attitude [43]. However, as recently stated by Inoue-Choi et al. [44], it is also possible that individuals with higher quality of life post-treatment were more capable of physical activity.
A limited number of studies evaluated change in physical activity over time and prognosis [35, 39].The results of our current meta-analysis suggested that an increase in physical activity, particularly during the post-diagnosis period, is associated with a decrease in colorectal cancer-specific and overall mortality. The observed findings for change in physical activity measured from pre- to post-diagnosis were seemingly dependent on the length of the interval. Meyerhardt et al. [39] found that at approximately 22-month post-diagnosis, there was a significant decrease in disease-specific mortality among women who had increased their pre-diagnosis physical activity category compared with women who remained in the same category or shifted to a lower category. However, in a population with a comparable age and stage distribution, Baade et al. [35] found that at 5-month post-diagnosis, there was no association between an increase in physical activity level and disease-specific mortality.
There are also few studies of weight change over time and potential effects on quality of life and survival in colorectal cancer patients. Only three studies have addressed the association between weight change and colorectal cancer-specific and overall mortality. The results of this current meta-analysis suggested that there were no beneficial or detrimental effects of weight gain on mortality. In studies with breast cancer survivors, women who gain weight after diagnosis were significantly more likely to experience cancer recurrence and mortality [45], which has been attributed to a simultaneous increase in fat mass and a decrease in lean body mass [46]. A possible explanation for this contradictory observation in colorectal cancer survivors might be, as suggested by Lynch et al. [31], that their weight gain is not related to health behavior, but instead is a reflection of the recovery of experienced weight loss related to the cancer, treatment, or both, which could have led to changes in body composition.
Our review has several limitations resulting from the availability and the methodology of the published data, and these limitations should be considered when interpreting our results. First, the number of studies on the effects of change over time in physical activity and body weight on quality of life and mortality was very limited. Except for one study in which physical activity was based on changes in physical fitness as measured in treadmill test over the course of the study [38], data on both body weight and physical activity in most studies were self-reported instead of objective assessments. Having been diagnosed with colorectal cancer, and probably subsequently having acquired the knowledge on physical inactivity and weight being risk factors for colorectal cancer, might have influence on their reporting. Asking participants to recall their pre-diagnosis physical activity levels and weight is also subjected to bias. Second, there were large variations in the lengths of the interval used for measuring change over time in physical activity and weight as well as variations in baseline time points of measurements, either pre-diagnosis, post-diagnosis, or post-treatment (surgery or adjuvant therapy). These variations make recommendations for a specific timing to engage into healthy behaviors (soon after diagnosis or short after treatment) and specific duration for colorectal cancer survivors difficult. Third, the follow-up periods after diagnosis and subsequent timing of endpoint variations in physical activity categories differed between studies. The length of follow-up after diagnosis for quality of life measurement was often limited to 2 years (median of 7 to 24 months), while the greatest impact on quality of life among colorectal cancer survivors seems to occur in the first 2–3 years after diagnosis and stabilizes beyond 3-year post-diagnosis [47]. Hence, both physical activity and quality of life could have been affected by clinical, medical, and psychological factors experienced by survivors [20, 48, 49].However, despite these short follow-up periods after diagnosis, the three studies included in current meta-analysis indicated a beneficial effect of physical activity on quality of life. The median length of follow-up for the endpoint mortality varied between 5 and 10 years. Although the study design were prospective observational and adjustments were made in the analyses, it is possible that changes in health behaviors other than physical activity or weight have influenced the observed association. Outcome from recent studies suggest that the effect of combination of healthy behaviors rather than the effect of a single healthy behavior should be examined [50]. Effect of combination of healthy behaviors, including maintaining normal body weight, staying physically active, and eating healthy diet, is associated with low risk of mortality [51] and high quality of life [21, 23, 44, 50].However, results from prospective studies should provide evidence on whether change over time into healthier behavior combination among cancer survivors is also associated with positive effects on survival and quality of life.
In conclusion, based on an analysis of seven studies, we found that an increase in physical activity levels was associated with improved quality of life and reduced risk of disease-specific mortality in colorectal cancer survivors. Our study showed neither positive nor negative effects of weight gain on mortality. Given the paucity of the literature published on this topic, our findings should be interpreted with caution. More prospective studies with large sample sizes are needed, which apply objective assessments to quantify the change in physical activity level and weight post-diagnosis, and which account for the individual’s initial activity and weight status from the moment of cancer diagnosis, to understand what level of physical activity provides prognostic effects. Such studies may support the development of appropriate health education and (personalized) intervention strategies to improve the health and quality of life for colorectal cancer survivors.
References
Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F (2013) GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer, http://globocan.iarc.fr, accessed on 18/02/2014.
SEER Stat Fact Sheets: colon and rectum (2010). vol 2011. National Cancer Institute, Bethesda
Maddams J, Brewster D, Gavin A, Steward J, Elliott J, Utley M, Moller H (2009) Cancer prevalence in the United Kingdom: estimates for 2008. Br J Cancer 101(3):541–547
Demark-Wahnefried W, Pinto BM, Gritz ER (2006) Promoting health and physical function among cancer survivors: potential for prevention and questions that remain. J Clin Oncol 24(32):5125–5131
Doyle C, Kushi LH, Byers T, Courneya KS, Demark-Wahnefried W, Grant B, McTiernan A, Rock CL, Thompson C, Gansler T, Andrews KS (2006) Nutrition and physical activity during and after cancer treatment: an American Cancer Society guide for informed choices. CA Cancer J Clin 56(6):323–353
Demark-Wahnefried W, Jones LW (2008) Promoting a healthy lifestyle among cancer survivors. Hematol Oncol Clin N Am 22(2):319–342, viii
Vrieling A, Kampman E (2010) The role of body mass index, physical activity, and diet in colorectal cancer recurrence and survival: a review of the literature. Am J Clin Nutr 92(3):471–490
Davies NJ, Batehup L, Thomas R (2011) The role of diet and physical activity in breast, colorectal, and prostate cancer survivorship: a review of the literature. Br J Cancer 105(Suppl 1):S52–S73. doi:10.1038/bjc.2011.423
Ballard-Barbash R, Friedenreich CM, Courneya KS, Siddiqi SM, McTiernan A, Alfano CM (2012) Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J Natl Cancer Inst 104(11):815–840
Mishra SI, Scherer RW, Geigle PM, Berlanstein DR, Topaloglu O, Gotay CC, Snyder C (2012) Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Syst Rev 8, CD007566
Mishra SI, Scherer RW, Snyder C, Geigle PM, Berlanstein DR, Topaloglu O (2012) Exercise interventions on health-related quality of life for people with cancer during active treatment. Cochrane Database Syst Rev 8, CD008465. doi:10.1002/14651858.CD008465.pub2
Meyerhardt JA, Heseltine D, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, Thomas J, Nelson H, Whittom R, Hantel A, Schilsky RL, Fuchs CS (2006) Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. J Clin Oncol 24(22):3535–3541
Meyerhardt JA, Giovannucci EL, Ogino S, Kirkner GJ, Chan AT, Willett W, Fuchs CS (2009) Physical activity and male colorectal cancer survival. Arch Intern Med 169(22):2102–2108
Kuiper JG, Phipps AI, Neuhouser ML, Chlebowski RT, Thomson CA, Irwin ML, Lane DS, Wactawski-Wende J, Hou L, Jackson RD, Kampman E, Newcomb PA (2012) Recreational physical activity, body mass index, and survival in women with colorectal cancer. Cancer Causes Control 23(12):1939–1948. doi:10.1007/s10552-012-0071-2
Campbell PT, Patel AV, Newton CC, Jacobs EJ, Gapstur SM (2013) Associations of recreational physical activity and leisure time spent sitting with colorectal cancer survival. J Clin Oncol 31(7):876–885
Haydon AM, Macinnis RJ, English DR, Giles GG (2006) Effect of physical activity and body size on survival after diagnosis with colorectal cancer. Gut 55(1):62–67
Doria-Rose VP, Newcomb PA, Morimoto LM, Hampton JM, Trentham-Dietz A (2006) Body mass index and the risk of death following the diagnosis of colorectal cancer in postmenopausal women (United States). Cancer Causes Control 17(1):63–70
Dignam JJ, Polite BN, Yothers G, Raich P, Colangelo L, O’Connell MJ, Wolmark N (2006) Body mass index and outcomes in patients who receive adjuvant chemotherapy for colon cancer. J Natl Cancer Inst 98(22):1647–1654
Mosher CE, Sloane R, Morey MC, Snyder DC, Cohen HJ, Miller PE, Demark-Wahnefried W (2009) Associations between lifestyle factors and quality of life among older long-term breast, prostate, and colorectal cancer survivors. Cancer 115(17):4001–4009
Buffart LM, Thong MS, Schep G, Chinapaw MJ, Brug J, van de Poll-Franse LV (2012) Self-reported physical activity: its correlates and relationship with health-related quality of life in a large cohort of colorectal cancer survivors. PLoS One 7(5):e36164. doi:10.1371/journal.pone.0036164
Grimmett C, Bridgewater J, Steptoe A, Wardle J (2011) Lifestyle and quality of life in colorectal cancer survivors. Qual Life Res 20(8):1237–1245
Peddle CJ, Au HJ, Courneya KS (2008) Associations between exercise, quality of life, and fatigue in colorectal cancer survivors. Dis Colon Rectum 51(8):1242–1248
Blanchard CM, Courneya KS, Stein K (2008) Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: results from the American Cancer Society’s SCS-II. J Clin Oncol 26(13):2198–2204
Hawkes AL, Gollschewski S, Lynch BM, Chambers S (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors ‘CanChange’: a pilot study. Psycho-Oncology 18(4):449–455. doi:10.1002/pon.1527
Pekmezi DW, Demark-Wahnefried W (2011) Updated evidence in support of diet and exercise interventions in cancer survivors. Acta Oncol 50(2):167–178. doi:10.3109/0284186X.2010.529822
Blanchard CM, Baker F, Denniston MM, Courneya KS, Hann DM, Gesme DH, Reding D, Flynn T, Kennedy JS (2003) Is absolute amount or change in exercise more associated with quality of life in adult cancer survivors? Prev Med 37(5):389–395
Cancer Survivorship Research (NCI) http://cancercontrol.cancer.gov/ocs/definitions.html; accessed 07 October 2013.
Mols F, Vingerhoets AJ, Coebergh JW, van de Poll-Franse LV (2005) Quality of life among long-term breast cancer survivors: a systematic review. Eur J Cancer 41(17):2613–2619
DeWys WD, Walters K (1975) Abnormalities of taste sensation in cancer patients. Cancer 36(5):1888–1896
Tisdale MJ (2010) Cancer cachexia. Curr Opin Gastroenterol 26(2):146–151. doi:10.1097/MOG.0b013e3283347e77
Lynch BM, Cerin E, Owen N, Hawkes AL, Aitken JF (2008) Prospective relationships of physical activity with quality of life among colorectal cancer survivors. J Clin Oncol 26(27):4480–4487
DerSimonian R, Kacker R (2007) Random-effects model for meta-analysis of clinical trials: an update. Contemp Clin Trials 28(2):105–114
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315(7109):629–634
Greenland S (1987) Quantitative methods in the review of epidemiologic literature. Epidemiol Rev 9:1–30
Baade PD, Meng X, Youl PH, Aitken JF, Dunn J, Chambers SK (2011) The impact of body mass index and physical activity on mortality among patients with colorectal cancer in Queensland, Australia. Cancer Epidemiol Biomarkers Prev 20(7):1410–1420
Campbell PT, Newton CC, Dehal AN, Jacobs EJ, Patel AV, Gapstur SM (2012) Impact of body mass index on survival after colorectal cancer diagnosis: the Cancer Prevention Study-II Nutrition Cohort. J Clin Oncol 30(1):42–52
Courneya KS, Friedenreich CM (1997) Relationship between exercise pattern across the cancer experience and current quality of life in colorectal cancer survivors. J Altern Complement Med 3(3):215–226
Courneya KS, Friedenreich CM, Quinney HA, Fields AL, Jones LW, Fairey AS (2003) A randomized trial of exercise and quality of life in colorectal cancer survivors. Eur J Cancer Care (Engl) 12(4):347–357
Meyerhardt JA, Giovannucci EL, Holmes MD, Chan AT, Chan JA, Colditz GA, Fuchs CS (2006) Physical activity and survival after colorectal cancer diagnosis. J Clin Oncol 24(22):3527–3534
Meyerhardt JA, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, Nelson H, Whittom R, Hantel A, Thomas J, Fuchs CS (2008) Impact of body mass index and weight change after treatment on cancer recurrence and survival in patients with stage III colon cancer: findings from Cancer and Leukemia Group B 89803. J Clin Oncol 26(25):4109–4115
Pinto BM, Papandonatos GD, Goldstein MG, Marcus BH, Farrell N (2011) Home-based physical activity intervention for colorectal cancer survivors. Psycho-Oncology 22(1):54–64. doi:10.1002/pon.2047
Hawkes AL, Chambers SK, Pakenham KI, Patrao TA, Baade PD, Lynch BM, Aitken JF, Meng X, Courneya KS (2013) Effects of a telephone-delivered multiple health behavior change intervention (CanChange) on health and behavioral outcomes in survivors of colorectal cancer: a randomized controlled trial. J Clin Oncol 31(18):2313–2321
Courneya KS, Friedenreich CM, Arthur K, Bobick TM (1999) Understanding exercise motivation in colorectal cancer patients: a prospective study using the theory of planned behavior. Rehabil Psychol 44(1):68–84
Inoue-Choi M, Lazovich D, Prizment AE, Robien K (2013) Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention is associated with better health-related quality of life among elderly female cancer survivors. J Clin Oncol 31(14):1758–1766. doi:10.1200/JCO.2012.45.4462
Kroenke CH, Chen WY, Rosner B, Holmes MD (2005) Weight, weight gain, and survival after breast cancer diagnosis. J Clin Oncol 23(7):1370–1378
Demark-Wahnefried W, Peterson BL, Winer EP, Marks L, Aziz N, Marcom PK, Blackwell K, Rimer BK (2001) Changes in weight, body composition, and factors influencing energy balance among premenopausal breast cancer patients receiving adjuvant chemotherapy. J Clin Oncol 19(9):2381–2389
Ramsey SD, Andersen MR, Etzioni R, Moinpour C, Peacock S, Potosky A, Urban N (2000) Quality of life in survivors of colorectal carcinoma. Cancer 88(6):1294–1303
Chambers SK, Lynch BM, Aitken J, Baade P (2009) Relationship over time between psychological distress and physical activity in colorectal cancer survivors. J Clin Oncol 27(10):1600–1606. doi:10.1200/JCO.2008.18.5157
Chambers SK, Meng X, Youl P, Aitken J, Dunn J, Baade P (2012) A five-year prospective study of quality of life after colorectal cancer. Qual Life Res 21(9):1551–1564. doi:10.1007/s11136-011-0067-5
Schlesinger S, Walter J, Hampe J, von Schonfels W, Hinz S, Kuchler T, Jacobs G, Schafmayer C, Nothlings U (2014) Lifestyle factors and health-related quality of life in colorectal cancer survivors. Cancer Causes Control 25(1):99–110. doi:10.1007/s10552-013-0313-y
Inoue-Choi M, Robien K, Lazovich D (2013) Adherence to the WCRF/AICR guidelines for cancer prevention is associated with lower mortality among older female cancer survivors. Cancer Epidemiol Biomarkers Prev 22(5):792–802. doi:10.1158/1055-9965.EPI-13-0054
Acknowledgments
This work was supported by internal funding from the department of Public Health of the Erasmus MC, University Medical Center Rotterdam. We acknowledge the support of the librarian, Louis Volkers.
Funding
This work was supported by internal funding from the department of Public Health of the Erasmus MC, University Medical Center Rotterdam. The funder did not participate in the study design, data collection, data analysis and interpretation, writing the manuscript, or in the decision to submit the paper for publication.
Conflict of interest
The authors have no conflicts of interest to report.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Otto, S.J., Korfage, I.J., Polinder, S. et al. Association of change in physical activity and body weight with quality of life and mortality in colorectal cancer: a systematic review and meta-analysis. Support Care Cancer 23, 1237–1250 (2015). https://doi.org/10.1007/s00520-014-2480-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-014-2480-0