
Abstract
The most common situation encountered in the operating room scheduling is the uncertainty of operation times. This situation may cause the operations to be delayed or canceled. In this study, stochastic operating room scheduling is discussed under the uncertainty of operation times. In real life, variability may vary depending on many factors from operation to operation/patient to patient. These factors are the surgeon's experience, the difficulty of the operation, the patient's weight, age, disease history, etc. In this study, separate coefficients of variability were determined for each operation, taking into account the variability factors. Operations are scheduled, taking into account the operation-specific coefficients of variation. To evaluate the variability factors, analytical network process method was used considering the interaction between them. The level of uncertainty/coefficient of variation of each operation was determined with the PROMETHEE method. Finally, the logical modeling power of constraint programming is used to solve the operating room scheduling problem. In the proposed constraint programming model, the flexibility of the goal programming method was utilized. For the modeling of uncertainties, a chance-constrained approach was used. The case study demonstrates that the proposed approach is a novel and outstanding technique, and the proposed CP model is efficient in solving the problem. As a result of the study, the uncertainty in the operation time of each patient was calculated as the variability according to the factor weights, and the tables were reconstructed according to this situation. The performance and effectiveness of the new schedules obtained under variability are shown.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Operating rooms are the most important source of income and expense of hospitals (Monteiro et al. 2015; Hamid et al. 2019). The scheduling of the operations to be performed in these units in the right order to optimize a certain purpose plays an important role on the efficiency and income of the operating rooms (Van Oostrum et al. 2010; Gür et al. 2019). Planning of operation is a problem of assigning operations to operating rooms, taking into account the available resources in hospitals (Eren and Gür 2018). In most current applications, real-life situations encountered in scheduling processes that complicate the problem structure are not taken into account. This shows that in modeling processes, researchers manage the process under assumptions. But in real life this is not the case. There are many uncertainties to consider in the scheduling process (Jebali and Diabat 2015). Considering the types of uncertainty considered in the literature (Table 1), random arrival of patients, insufficiency of equipment/material (resource uncertainty), availability of bed, post-operative stay and operation times come to the fore (Vali-Siar et al. 2018). Researchers, on the other hand, mostly consider the uncertainty of operation times. Considering the uncertain nature of operation times in the planning of the operating room, it can ensure effective use of the units and prevent cancelation or postponement of operations (Molina-Pariente et al. 2018).
In this study, a new solution approach for the operating room scheduling problem involving the uncertainty of operation times is presented. In the planning structure, during a limited planning horizon of a few days, elective patients to be operated in each day are assigned to the operating rooms. Uncertainty of operation times greatly affects the effective use of operating rooms (Najjarbashi and Lim 2020). For this reason, taking into account the uncertainty of operation times, it is aimed to improve the utilization rate and to prevent costs arising indirectly from over or under utilization. At the same time, with the right planning, the operations of the patients on the waiting list can be carried out on time and the patient satisfaction rate can be increased. For this reason, the uncertain nature of the operations for elective patients was taken into account in the operating room scheduling. In the literature, the uncertainty of operation times is considered under the assumption of a constant coefficient of variation. However, in real life, operation times may vary on the basis of each patient. In hospitals, the patient's health history, in addition to other reasons such as the late arrival of patients, may cause the average estimated operation time to be prolonged. It is stated that when this situation is encountered in real life, the plans made are disrupted, and there are disruptions. Each patient should be examined specifically in medical terms. Contrary to this situation, when the patients are not evaluated specifically, that is, when the variability is taken as constant, the accuracy and effectiveness of the planning are negatively affected. When the literature is examined, it has been seen that many factors are effective on operation times. Based on these factors, in the study, first, the factors that cause the uncertainty of the operation times were investigated. One of the problems addressed in the study is to determine the uncertainty factors and calculate how effective they are. For this, a literature review was conducted. The factors were determined as the surgeon's experience, the difficulty of the surgery, the patient's age, weight, smoking and alcohol use, disease history, availability of equipment and materials, and weekly working hours. Considering these factors based on each patient, it is seen that they directly affect the operation process. For this reason, in this study, the factors that cause the uncertainty of operation times were investigated, and their variability was analyzed on a per-patient basis. Modeling was carried out considering the number of patients on the waiting list. To quantitatively evaluate these factors, which are expressed qualitatively in the study, multi-criteria decision-making methods, frequently used in the literature, were used. Analytical network process (ANP) method, one of the multi-criteria decision-making methods, was used for evaluation. This method was used because it gives effective results in qualitative evaluations and takes into account the interactions/feedbacks among factors that are not at the same level. After the factors were evaluated in line with the opinions of the doctors working in the hospital, the variations of the operations were determined using the PROMETHEE method, one of the multi-criteria decision-making methods. This method was preferred because it is easy to use and enables the evaluation of each operation on the basis of each criterion. After the variability of each operation was determined, scheduling was made across a planning horizon. For the stochastic operating room scheduling problem, a chance-constraint programming model has been proposed where the coefficients of variation differ from patient to patient. The logical modeling power of constraint programming is used to solve the problem. Constraint programming and goal programming methods were used to optimize the several objectives related to operating room scheduling problem. The study's main purpose is to provide an idea that allows the preparation of more usable schedules suitable for real life.
This study consists of seven parts. In the second part studies dealing with the problem of scheduling surgical operations in the literature are given. In the third part, the definition of the problem is discussed and the proposed approach is explained by mentioning the structure of the problem. In the fourth part, the suggested models are given. In the fifth part, a case study is given. In the sixth and seventh part, the results of the study are discussed from the managerial point of view.
2 Literature review
Timely treatment and increased efficiency in operating rooms require an appropriate management policy (Lin and Li 2021; Kayvanfar et al. 2021). In the literature, attention is drawn to effective management and planning for operating room scheduling. The operating room scheduling problem is an optimization problem that involves balancing the operation start time of the patients who will come to the hospital and the resources assigned during a surgery period (Nazif 2018; Silva and Souza 2020). Complexity is increasing as operating rooms have many resources (surgical team and equipment) (Hamid et al. 2019; Breuer et al. 2020; Park et al. 2021). This situation causes difficulties in scheduling processes. The biggest challenge in making correct planning is the uncertainty in the nature of the scheduling processes. In deterministic studies, these uncertainties are ignored under assumptions. In stochastic studies, these uncertainties are included in the process. The most discussed uncertainties in the literature are the uncertainty of operation times and the arrival of the cases (Cardoen et al. 2010). Table 1 is listed according to the types of uncertainty considered in the studies in the literature. Researchers often use stochastic programming approaches to manage these uncertainties.
In Table 1, it is seen that among the types of uncertainty, researchers mostly focus on the uncertainty experienced during the operation times. Studies (Saadouli et al. 2015; Noorizadegan and Seifi 2018; Kumar et al. 2018; Pang et al. 2018; Liu et al. 2018; Wang et al. 2018; Zhang et al. 2019 Rahimi et al. (2023); Schouten et al. (2023)), which generally address uncertainties experienced during the operation period, categorized patients as elective or non-elective when planning the operating rooms (Gür and Eren 2018a, b). Uncertainty in operation times can be considered separately for the emergency patient group and elective patients. The elective group of patients does not need immediate treatment and can be carried out at a pre-determined time frame. On the other hand, the non-elective patient group needs urgent treatment although their arrival is unknown. M’Hallah and Visintin (2019) considered the uncertainty of surgical times for the elective patient group. It also considered the uncertainty of intensive care unit times and post-operative hospitalization times. Dai et al. (2023) pointed out the uncertainties in elective patient planning and operation times and also mentioned that it is necessary to deal with the uncertainties in the intensive care unit and patients' bed demands. For this purpose, they modeled an operating room planning problem involving uncertainty using fuzzy numbers and sets.
Uncertainty in operation times is an important constraint for operating rooms. This uncertainty causes patient cancelations or postponements. Especially since the elective patient group is the main source of income for hospitals (Wang et al. 2023), plans are being made to prevent any mishaps that may occur in these operations. Uncertainty is one of the most important factors causing delays in elective patients. It is seen in the literature that there is a particular focus on the uncertainty of operation times and the arrival of emergency patients. At the same time, when looking at the studies, many methods are used to deal with these uncertainties. Stochastic approaches are one of the most widely used methods.
In the literature, it is adopted as a common assumption for non-elective patient groups that emergency patients are treated in private facilities (Brans and Smet 2016; Cardoen et al. 2010; Guerriero and Guido 2011; Gür and Eren 2018a, b). Adopting a different policy on the arrival of emergency patients, Kamran et al. (2019) accepted that the operation times were randomly distributed. In the study, they determined the capacity in the planning of the operating room for the arrival of the emergency patients and presented the possibility of a separate slack in the program. So, a part of the capacity of operating rooms is reserved for emergency patients. In this context, they aimed to minimize the total patient waiting time (Molina-Pariente et al. 2018; Belkhamsa et al. 2018; Otten et al. 2019). In the studies examined, the researchers used different solution approaches to increase the effectiveness of the solution process.
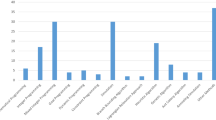
Figure 1 shows the solution techniques used in recent studies in the literature. Figure 1 focuses only on stochastic studies. As can be seen in this figure, researchers try different techniques and use the advantages of the methods to improve the solution process. According to Fig. 1, more studies using optimization techniques are needed for managing uncertainty. At this point, chance-constrained programming comes into prominence as an effective approach that allows the constraints including problem parameters to be distorted according to the probability levels of certain distributions (Atalay and Apaydin 2011). Chance-chance programming in the literature guarantees a balanced utilization rate in operating rooms (Wang et al. 2019). In Noorizadegan and Seifi (2018) study, operating rooms were characterized by uncertain operation times. By working on the elective patient group, they aimed to minimize the cost of opening the operating rooms and the penalties related to the turnover times. Wang et al. (2019) aimed to minimize the number of open operating rooms by chance-constraint programming. With this programming, which permits partial distortion of the constraints, researchers provide approximate reliability in finishing an operating room without overtime.

In addition, recently, in the literature, researchers have been reviewing the limitations of their studies to ensure their suitability to real life and developing new solution approaches despite the increasing complexity of the problem. Wang et al. (2022), Miao and Wang (2023), Rahimi et al. (2023), and Zhu et al. (2023) discuss distributed surgical planning applications in their study. With this newly implemented system, an alliance is established between hospitals to prevent patient cancelations and patient postponements. According to this alliance, in cases where there are too many emergency cases, and there are not enough resources, referrals are made to other hospitals.
The aim of this study is to increase the efficiency of the operating room and increase the reliability of the operation by expressing the uncertainty of operation times in real life with chance constraints. In addition, it is aimed to evaluate the situations that affect operation times in real life and the factors that will be the main source of uncertainty in operation times. In the literature, there is no study in which the factors causing uncertainty are evaluated, taking into account the variability of operation times specific to the patient. In the literature, variability is generally taken as constant. This suggests that the real-life situation of the patients is not fully reflected in the planning. When we look at the studies in recent years, we see that they focus especially on the uncertainties in operation times. This supports that our study touches upon an important point. At the same time, studies in the literature indicate that rather than addressing the factors that cause uncertainty in operation times mentioned in this study, the postponements or cancelations that this situation will cause should be prevented. For this reason, first of all, identifying the factors that cause uncertainty and analyzing their variability in operation times allows planning to be more effective and to obtain results closer to real life. The reasons for uncertainty in operation times are situations encountered in real life, and their inclusion in modeling is important for the realism of the plans. In this way, it is possible to obtain more accurate estimates of operation times in planning and prevent disruptions such as patient postponements. In addition, by planning the use of resources correctly, significant inequality between the actual demand in the hospital on a given day and the current capacity will be prevented, and patient satisfaction will increase, and increases in operating costs resulting from situations such as overtime will be prevented.
The contribution of this study to the literature is as follows: (i) Data from the Gür et al., (2019)’s study, including different types of surgical operations, were considered. It was applied considering the distribution of surgical times. The main difference from Gür et al. (2019)'s study is the investigation of the underlying causes of the uncertainty of operation times. At the same time, they are evaluated quantitatively, and a separate state of variability is calculated for each patient. (ii) Stochastic chance-constraint constraint programming model was applied by considering time uncertainty. (iii) Real-life constraints such as the different requirements of surgeons are considered. (iv) The factors causing uncertainty in the operation times were evaluated. (v) Evaluation of these factors has not been found among previous studies in the literature. (vi) With the ANP method, factors were evaluated by considering the interaction between them. (vii) With the PROMETHEE method, each operation was evaluated separately on the basis of each factor and the variations were determined. (viii) The chance-constraint programming method was used for modeling. (ix) Schedules were created by transferring these levels of variability to the modeling process.
3 Preliminaries
3.1 An outlook of chance-constrained programming
Chance-constrained programming developed by Charnes and Cooper (1959) is used to model the uncertainty of a problem. The basic logic of CCP is to transform the probabilistic constraints to the deterministic equivalents. The structure of a chance-constraint is as follows:
In this inequality, \(a_{i}\) is independent and normally distributed parameter, \(a_{i} \sim N\left( {\mu_{{a_{i} }} ,\sigma_{{a_{i} }}^{2} } \right)\). Equation 1 means that total parameter \(\mathop \sum \nolimits_{i = 1}^{N} a_{i} x_{i}\) is less than or equal to \(b\) with at least a pre-determined confidence level \(\alpha\) specified by the decision maker. Equation 1 can be transformed into deterministic equivalent as follows:
In Eq. 2, \(A\) defines a standard normal variation with a mean of zero and a variance of one. Then, the stochastic chance-constrained inequality is transformed as follows:
where \((\phi )\) represents the standard normal cumulative distribution function. Finally, the chance-constrained inequalities are transformed deterministically into the following inequality:
Using this transformation, the stochastic non-linear equation is converted to the deterministic equivalent. In this way, we can easily model the stochastic mathematical model for any problem.
3.2 An overview of CP
Constraint programming is an alternative programming technique created for optimal solution of linear programming and easy identification of logical expressions. In constraint programming, difficult-to-define constraints in linear programming are easily identified using logical expressions (Apt 2003). Constraint programming method has objective functions with decision variables, linear constraint sets and domain of decision variables as an integer programming. One of the other main concepts of CP is the constraints. The constraints are related to the relationship between some variables and their domains (Bukchin and Raviv 2018). The global constraints (e.g., pack) are the constraints that are used to some powerful algorithms to reduce the decision variable areas.
Constraint programming starts the solution with an empty assignment. It then continues to assign a value to the variable by decreasing the fields of the decision variables and multiplying the constraints to obtain the objective function value. The propagation is used to filter the variable domains by eliminating inconsistent values. As soon as a variable domain is changed, constraint related to that variable are propagated. Domain reduction is a process that removes the non-assigned variable values that do not satisfy any constraint. Thus, it obtains a consistent assignment at every iteration of domain reduction. If the search cannot reduce any area, an additional restriction is added to the model. The trackback mechanism is executed to try some other branches. The entire decision variable is expected to be assigned to a single value, and if not, the search continues recursively (Bukchin and Raviv 2018).
3.3 Multi-criteria decision-making
Individuals or businesses may encounter situations such as deciding between solution options in their daily life. In these cases, multi-criteria decision-making methods come to the fore. Multi-criteria decision-making methods are used by researchers in different thematic areas in the literature. In project selection (Meade and Presley 2002; Gür et al. 2016), transportation and logistics (Jharkharia and Shankar 2007; Taş et al. 2017), industry 4.0 (Sevinc et al. 2018), personnel selection (Bedir and Eren 2015) in the decision support system (Andra and Hajjah 2020) is used.
3.3.1 Analytic network process
In the analytic network process method, there are criteria that affect the decision, the relationships between them, dependencies and feedbacks in the decision problem. All these come together to form the network model structure (Saaty and Vargas 2006).
3.3.2 PROMETHEE
PROMETHEE (Preference Ranking Organization Method for Enrichment Evaluations) is a method of ranking and prioritizing. Using the PROMETHEE I method, it is possible to determine the partial priorities by comparing the alternatives in line with the specified criteria, and by the PROMETHEE II method, it is possible to determine the clear priorities by comparing the alternatives according to the specified criteria (Brans and De Smet 2016). The solution process of the PROMETHEE method is shown in Appendix 2.
4 Problem background
In this study, the problem of scheduling in the operating room is discussed. The purpose of operating room planning here is to schedule the operations of patients on the waiting list throughout the planning horizon and to use the operating rooms as effectively as possible. Among the types of uncertainty that affect the scheduling processes of the operating room, the uncertainty of operation times was taken into account. Uncertainties experienced during operation times cause disruptions in planning. This results in the postponement or cancelation of the cases. In the problem, a case study was made using the data set in the literature (Gür et al. 2019). Factors causing the source of uncertainty in the operation time of the elective patients on the waiting list were examined. Multi-criteria decision-making methods were used in the solution phase. ANP method was used to evaluate these factors and PROMETHEE method was used to determine the level of variability. Figure 2 shows the diagram of the solution process of the problem.

Diagram of proposed model
Looking at Fig. 2, first of all, the factors that cause uncertainty in operation times were determined in line with the opinions of experts, and these factors were weighted with the ANP method. These priority weights were transferred to the Promethee method, and in this step, each operation was evaluated based on each criterion, that is the patient's health history. At the end of this evaluation, the variability in operation times for each patient was calculated. This variability was transferred to the model for the scheduling phase, and the model solution was performed. According to this scheduling, the discharge procedures of the patient whose treatment is completed are carried out in real life by directing him/her according to his/her wards or ICU (intensive care unit) needs.
4.1 Factors affecting operation time variability
Considering a group of patients or a series of operations, each operation has its own characteristics related to the medical structure of the patient. In other words, when each patient is evaluated individually, the life style in real life affects the duration of the operation. When the uncertainties in the operation period arising due to the nature of the operating room scheduling process are examined, it is seen that there are many factors that cause these uncertainties. These factors differ as surgeon, patient and other (Internet Source 2020). Although the operating rooms have a homogeneous structure, the differentiation of each operation process causes an increase in uncertainty. For this reason, when these factors that differentiate the structure and duration of the operation are considered and the uncertainty situation is considered specifically on the basis of each operation, it is seen that the rate of utilization of operating rooms changes. These factors are the surgeon's experience, the difficulty of the operation, the patient's weight, age, using of smoking and alcohol, disease history, adequacy of equipment and materials, and weekly working hours. Table 2 includes these factors.
For example, the evaluation of real-life factors such as the patient's history of illness, smoking/alcohol, etc. has an effect on how much they affect the variability on operation times and how much they shape the schedules.
4.2 Interactions and relationships between factors
According to the solution process of the ANP method, the factors that affect the problem were determined by taking the opinions of experts and a network structure was created according to the interactions between them. The network structure is shown in Fig. 3.

Interaction structure between criteria
Figure 3 shows the relationship between criteria. Here, sub-criteria are specified under each criterion. There is a mutual interaction between these criteria, the power of the ANP method to model this interaction was utilized. As the criteria can affect the criteria within its own group, it can also affect the criteria under other main criteria. As an example of the interaction between the criteria, the age criterion of the patient can affect the history of the disease and similarly increase the difficulty of the operation. The network structure has been established considering these and similar interactions. Pairwise comparison matrices have been established according to the network structure shown in Fig. 1. While making this evaluation, the opinions of experts were consulted and calculations were made with the help of the super decision package program. The experts were making evaluations in the study consist of three people, a specialist doctor and an academician working in the health institution. A pairwise comparison matrix was created with the opinions obtained from these experts. These pairwise comparison matrices were combined with the geometric mean method. In calculating the weights of the criteria, observed that the consistency ratios of all pairwise comparison matrices were less than 0.1.
4.3 Comparative evaluation of the factors
Pairwise comparison matrices of the factors are established. Table 3 contains an example comparison matrix. While making these evaluations, Saaty's 1–9 (1996) scale was used. Each factor was compared according to the opinions of the expert team of 4 doctors. As a result of this comparison, the importance weights of the factors were obtained. These weights are shown in Table 4.
When Table 4 is examined, the most important factor affecting the operation time variability is determined to be the difficulty of operation with a weight of 0.58083. The difficult nature of the operation performed in the operating room requires surgeons to complete it by moving more slowly and precisely. In this case, it causes prolongation of the operation time. Similar comments can be made for other factors.
4.4 Data matrix and determination of coefficients of variation
In the PROMETHEE method, the data matrix is first created. For the data matrix, the operations in Table 6 and the criterion weights obtained from the ANP method were used. The preference function has been determined for each criterion. The most important advantage of the PROMETHEE method can obtain very effective results. Different function types can be used for each evaluation criterion. The functions used in this study are v-shape and usual preference functions. Evaluation systems have been established for these functions on the basis of criteria. While entering the age of each patient for the age criterion, the disease history; using of smoking and alcohol; the availability of equipment and materials; The yes/no question was answered for the obesity status criteria. On the basis of each operation, the surgeon's specialty, operation difficulty and weekly working hours were evaluated. Thus, the CV value of each operation was obtained with the sequence obtained. In the solution process, uncertainty was modeled with the CV value according to the operation. Table 5 shows the values of 10 random patients according to the factors and their CV value in return.
10 patients are shown randomly among the patients on the waiting list in Table 5. The variability value determined as a result of calculations of these 10 patients is included. Patients of the same age who have different conditions in terms of other factors also have a different value for variability. For example, although OP44 and OP55 operations are of the same age, the variability values are very different from each other. The reason for this situation is that the values in other factors are different. The surgeon's experience was different for both patients, and the high criterion weight of this factor caused a significant difference in variability. Thus, each patient will be considered separately in the planning. In this case, it increases the accuracy of the plans made. To make a complete order in the PROMETHEE method, fi (\(\Phi )\) values are subtracted from each other (Annex 2). This calculation causes negative values in the PROMETHEE II ranking. In the modeling process, the obtained results were normalized to reflect these values. For normalization, the addition was made so that the smallest negative value equaled 0 and this value was added to each subsequent value. The values obtained as a result of this could be transferred to the model. Looking at the variability values in the last column in Table 5, a value of 1 indicates that the variability is high, that is, the medical characteristics of the patient will have a serious effect on the operation time.
4.5 Creation of schedules
The main purpose of the operating room scheduling problem type is to determine the strategies that will enable these units to be used effectively. The solution process becomes difficult due to the existence of uncertainty sources in the plans prepared in the operating room scheduling problem. The reason for the uncertainty of operation times in this study is that it has a significant effect on the allocation of operating rooms to patients. Because these times are less or more than expected causes less or more use of operating rooms (Pang et al. 2018). For this reason, the resources/factors that will cause uncertainty have been evaluated. For each surgery, the solution process was carried out according to the factor affecting the operation time.
This study focuses on operating rooms which are considered as one of the most important units in a hospital. There are various requirements for the allocation of operations to operating rooms, such as the establishment of the maximum working hours allowed by labor legislation, and the availability of equipment and devices required in each operating room. There are many external factors in hospitals, it contains a lot of uncertainty due to its structure. Therefore, the assumptions considered in the study are as follows:
-
o
It is not possible to start a trade before the planned start time or before the end time of the previous trade.
-
o
The scheduled program on the service cannot be changed, i.e., it is prohibited to reorganize or add to the procedure during the day.
-
o
The number of operations to be performed in the hospital is clear (constant) and emergency situations are not considered.
-
o
Sufficient number of personnel and all necessary resources are available to carry out the operations.
-
o
Working hours in the hospital are between 08: 00–12:00 and 13:00–17: 00.
-
o
Surgery is not performed on weekends; therefore, operating rooms are kept closed during this time.
In the operating room schedules to be created under these assumptions, it was desired to ensure the highest level of patient and staff satisfaction as well as the goals of the study. Thus, both the performance level provided by the personnel and the efficiency of the operating rooms will be increased. The application steps are schematized to convey the flow of the study. Thus, the critical points from the handling of the problem to the solution process were listed.
4.5.1 The notations
The notations used in the model are shown below. The time slots and the operating room index were converted into a single index and named as operating room-time slots (80 = 8 × 10).
Notation | ||
i | Number of operations | i = 1,..,120 |
j | number of operating room-time slots | j = 1,..,80 |
s | number of specialties | s = 1,..,6 |
t | number of operating room-time slot group | t = 1,..,8 |
M | A large enough number | |
Notation of modeling expressions | ||
\({X}_{i}\) | \(i. \text{ operation assignment status}\) | \(\forall i\) |
\({Y}_{ij}\) | \(\left\{\begin{array}{ll}1, \quad If \; operation\; i\; is\; performed\; in\; operating\; room\; j \\ 0, \quad otherwise\end{array}\right.\) | \(\forall i, \forall j\) |
\({Z}_{js}\) | \(\left\{\begin{array}{ll}1,\quad If\; expert\; s\; works\; in\; operating\; room\; j\\ 0, \quad otherwise\end{array}\right.\) | \(\forall j, \forall s\) |
\({V}_{ts}\) | \(\left\{\begin{array}{ll}1,\quad If\, expert\, s\, works\, in\, group t\\ 0, \quad otherwise\end{array}\right.\) | \(\forall t, \forall s\) |
\({p}_{i}\): | operation time i, including cleaning and preparation times | \(\forall i\) |
\({U}_{j}\) | Daily using time of operating room j | \(\forall j\) |
\({d}_{s}:\) | the set from experts s which prefers to be assigned to the time slot | \(\forall s\) |
Deviation variables | ||
\({u}_{j}^{-}\) | The amount of negative deviation to total available time from operating room-time slot | \(\forall j\) |
\({u}_{j}^{+}\) | The amount of positive deviation to total available time from operating room-time slot | \(\forall j\) |
\({r}_{s}^{-}\) | The amount of negative deviation from preferring time slot by experts s | \(\forall s\) |
\({r}_{s}^{+}\) | The amount of positive deviation from preferring time slot by experts s | \(\forall s\) |
\({p}_{t}^{-}\) | The amount of negative deviation from assigned experts in operating room–time slot j | \(\forall t\) |
\({p}_{t}^{+}\) | The amount of positive deviation from assigned experts in operating room–time slot j | \(\forall t\) |
4.5.2 Chance-constrained model
The constraint programming model used in the study is based on the Gür et al. (2019) study.
4.5.3 Constraints and goals
Equation (5) states that each operation is assigned to the whole operating room and time slots only once. Operating-time slot boundaries to which the i. operation can be assigned. The total number of operations is 120, with a separate number of each expertise. Equation (6) ensures that we have, at most, six different specialties in all operating rooms at any time slot. Thus, operations can be carried out with the same equipment and technical personnel in the time slot. An index, such as k, is added at the constraint. The constraint for the number of operations of each expertise is written, the number of operations of the previous expertise is also subtracted at each time, and the remaining number of operations is collected in index k.
Equations (7), (8), and (9) could assign an expert in all operating rooms throughout the entire time slot. Thus, in operating rooms separated by the same expert, operations could be carried out without any wait or interruption due to equipment and technical personnel changes throughout the whole week. Equation (7) describes the relationship between the decision variables \({x}_{i}\) and \({Y}_{ij}\). The equation ensures that the variable \({Y}_{ij}\) equals the value 1 if operation i is assigned to the jth time slot, and 0 otherwise. Equations (8) and (9) operations are grouped according to their expertise and then blocked with the t-index according to the operating room-time slot group. Thus, an expertise is only assigned to the operating room-time slot group on a column basis.
Minimizing the deviations between achievable time and working time is desirable for targets aimed at overloading the operating rooms and minimizing the use of the operating room. If the operation i is assigned within the operating room-time slot j, it is aimed to multiply the relevant expertise by the processing time and run it within the desired time period. Equation (10) aims to minimize operating room overtime and less use of the operating room. It ensures to minimize deviations between reachable time and working time in this goal. In other words, it is aimed to use the operating rooms in a balanced and effective manner.
Equation (11) allows surgeons in the operating room to perform operations related to their fields of speciality within the operating time slot they want. If the surgeon is assigned to an operating time slot she/he does not want, the equation equals 0. The C index groups those who want to choose an operating time slot among surgeons. In this constraint, the deviation in the positive direction is minimized and the assignment to undesired time slots is prevented. Equation (12) aims to allocate each operating room to only one speciality for a week. Thus, an speciality always works in the same operating room weekly. For example, operations belonging to the orthopedic surgery speciality are performed in the assigned operating room throughout the week. For this reason, the positive deviation of this variable is minimized so that the surgeries of that speciality are performed in the same room as much as possible. The deviation in the positive direction in this constraint is minimized. For the objective function, Eqs. (15), (14), and (13) are used, respectively.
4.5.4 Linearized chance-constrained model
Constraint programming models have been used by researchers in the literature in recent years. In a constraint programming model, a goal, constraints, and targets have identified that need to be minimized or desired to be at the highest level. As in mathematical programming, there are decision variables and parameters and mathematical expressions. It also allows decision makers to model logical situations.
Constraint programming is one of the basic tools that can be useful in developing various practical systems. The most important feature of the mathematical programming method is that it contains mathematical constraints and can be of logical or symbolic type. Restrictions of this logical or symbolic type are also called global constraints. In addition, it is possible to define a variable consisting of a combination of mathematical expressions and logical constraints (Focacci et al. 2003). The constraint programming model used in the study is based on the model proposed by Gür et al. (2019).
Constraints and goals
To reflect the uncertainties in real life, deterministic operation times were converted to stochastic ones. Ağpak and Gökçen (2007) proposed a new linear approximation inequality (24), and it is used in the proposed model as follows:
The expression given in Eq. (21) is written non-linearly to model the uncertainty in operation c. This constraint is linearized with the (25) constraint.
In this constraint (16), it is stated that each operation is assigned to all operating room and time slots only once. With this constraint (17), it is desirable to have maximum 6 different specialties in all operating rooms in each time frame. With these constraints (18), (19), and (20), it is possible to assign an expertise in every operating room for all time periods. In this way, operations can be performed in the operating room devoted to the same expertise without waiting or disruptions caused by the change of equipment and technical personnel all week. In this constraint (18), if operation i is assigned within operating room-time slot j, has this value stored in the \({Y}_{ij}\) decision variable with the corresponding i and j index values. With these constraints (19) and (20), operations are grouped according to their specialties and then blocked with t-index according to operating room-time group. Thus, only one expertise is assigned to the operating room-time slot group on a column basis.
In the ((21) and (25)) constraints, which aim to optimize the balanced use of operating rooms, it is desirable to minimize deviations between available time and working time. If the operation i is assigned within the operating room-time slot j, it is aimed to multiply the relevant expertise by the processing time and run it within the desired time period. In these constraints (21) and (25), negative and positive deviations are minimized for balanced utilization of operating rooms.
With this constraint (22), it is aimed to perform the operations of a specialist surgeon in the desired time periods in each operating room. When the constraint is executed, it is synchronized to 0 by typing the time periods that we do not want to be assigned. The index c is expressed as a cluster of specializations that wish to make preference. In this constraint, the deviation in the positive direction is minimized and the assignment to undesired time slots is prevented. With this constraint (23) it is aimed to allocate each operating room to different expertise for weeks. Thus, a specialization works throughout the week in the same operating room at all times. In this constraint, the deviation in the positive direction is minimized. For the objective function, Eqs. (15), (14) and (13) are used, respectively.
5 A case study
The data used in the study were developed by Gür et al. (2019). These data include the number of operations including preparation and cleaning times, the number of available operating rooms and capacities, prepared using historical data. The data for each surgery include the surgical specialty group, the duration of the operation that will determine the actual start and stop time of the operation. In this study where block scheduling is planned, the empty blocks reflect the operating rooms that are not available at that time slot. In the solution process, each block is requested to be assigned to a surgical group. Table 2 shows the operating times. The operations of the specialties and their operation times are given. There are 120 operations in the hospital according to the 2-week data taken from the waiting list (Table 6). There are 6 specialties and 8 operating rooms in this hospital. The model, which allows for block scheduling, has 10 time slots for assignments. Each time period represents a four-hour working time and a total of two times a day is thought to coincide. Table 7 shows the CV value for each operation determined in the PROMETHEE method. In the model, considering the uncertainty experienced in real life operation times, chance-constraint programming model and solution techniques are combined. In the solution process, a chance-constraint algorithm has been formed using the application power of goal programming and constraint programming methods. The operating room utilization rate was considered as performance measurement.
The values in Table 7 show the cv value for each operation. When the CV value of operation 67 is 0, when evaluated on the basis of criteria, we can think that the variability in the operation process is low and it does not change the operation time too much. For the 10th operation, which is the opposite situation, when it is considered according to the criteria, it is seen that it is effective under many factors that may affect the operation time. For this reason, it can be interpreted that there is a lot of variability.
Numerical results were obtained with the help of ILOG CPLEX 12.10. With chance-constraint constraint programming, a solution was proposed for the operating room scheduling problem. Uncertainties in operating times, which are frequently encountered in operating room scheduling problems, are taken into consideration (Table 8). Assuming that the operation times have a certain mean and variance, it is desired to ensure the reliability of the times. It is modeled in the solution process by scenario of different situations encountered in real life. This model was solved linear and non-linear.
It is desired to have a specialization in the same operating room all week. With this scenario, which is desired to be realized in real life by adding different constraints to the model, the same expertise has been assigned in an operating room for all time periods (Table 9). Thus, the operations of the specialties can be realized without changing the equipment and technical personnel.
The positive deviation in the constraint related to the fact that the operating rooms belong to the same expertise primarily in the objective function and the negative and positive deviation related to the time constraint involving the use of the operating rooms are minimized. The model was coded and solved by IBM ILOG CPLEX program.
In the constraints, assignment constraint given in Eq. (5), block scheduling constraint given in Eq. (6), block closure constraints in (7), (8), (9) equations, capacity/time constraint of operating room (10) equations, constraint of belonging to the same expertise of operating room in (12) equations.
6 Discussion and managerial insights
Operating room scheduling is a difficult problem type due to the complexity of the problem solving process (Gür and Eren 2018a, b). The complexity of this type of problem stems from the high uncertainties and the presence of multiple stakeholders in its structure. As a result, what is essentially desired is to achieve an effective and efficient utilization rate with different techniques used in the solution process. In the solution processes, schedules are obtained under many assumptions. No matter how much real life is tried to be reflected, it is very difficult to take into account more than one factor at the same time. Gür et al. (2019) made a deterministic approach with constraint programming under assumptions and enabled the scheduling of surgical operations. This study is also considered as a continuation. We continued through the deterministic model in Gür et al. (2019)'s study. The deterministic model is given in Appendix 1. In this study, it was aimed to prevent delays, patient postponements, case cancelations, or inefficiencies such as overtime caused by uncertainties in the operation time of the patients. For this reason, it has been tried to make the utilization rate of operating rooms efficient.
Considering the duration of operations, which is one of the biggest uncertainties in the operating room scheduling problem, it is known that these durations may vary from many different factors. Variable operation times, directly affect the rate of utilization of operating rooms. This study focused on determining these factors. In line with the opinions of the experts and as a result of the literature research, the factors that cause the uncertainty of the operation times are determined as the experience of the surgeon, the difficulty of the operation, the age and weight of the patient, using of smoking and alcohol, the history of the disease, the availability of equipment and materials, and the weekly working hours. When each patient is considered under these factors, it is seen that the operation time differs for each patient. When planning is made without considering this situation, deviations in the accuracy rates of the plans are possible. Considering these variations, it is thought that the plans made are more robust and appealing more than real life. When Table 10 is examined, it is seen that the utilization rates of both linear and non-linear results of the study are compared. According to this table, the increase in alpha value has led to more effective use of operating rooms. In this case, considering the variability rates separately according to the patients also contributes. Most of the operating rooms are operating at full capacity with the results obtained. It has been tried to prevent overtime and less use as much as possible. From the perspective of hospital managers, it is possible to comment that the costs arising from both idle time and overtime will decrease.
In the study, it is tried to reflect the variability of these times with alpha value in programming with chance constraint. The utilization rates of the operating rooms were determined by reflecting the decrease or increase of these times with the increase or decrease in the alpha value. Arenas et al., (2002), Cappanera et al., (2016) and also Barrera et al., (2018) pointed out that the most important goal desired in operating rooms is to use the operating room as efficiently as possible. However, this does not mean that all operating rooms should be open and used only at a certain time of the day and remain idle the rest of the time. The situation mentioned in scenario is encountered In other words, it is used only for a certain part of the day and the operating room is idle for the rest of the time.
The study's focus on the uncertainty of operation times is associated with the need to use operating rooms efficiently. A comparison of the results of this study and other similar studies (Gür et al. 2019) on the utilization rate of operating rooms, which is considered a performance criterion, is shown in Fig. 4.

Utilization rates comparison
In this study and Gür et al. (2019) study, the utilization rate of operating rooms is taken into account as a performance criterion. In the study, the utilization rate is obtained by dividing the working time in a day within the planning horizon and the actual time. These values were reflected in the graph as an average value by taking the arithmetic average.
This study was carried out by Gür et al. (2019). Gür et al. (2019) study takes into account the most basic situation, and there is no variability in operation times. This study focuses on the fact that in real life, each patient's operation time is specific according to their health history. For this reason, considering the variability in operation times in this study, Gür et al. (2019) study that even if the utilization rates are low, the most appropriate situation is reflected in real life. When Fig. 4 is examined, Gür et al. (2019) study that since the operation time is constant, the average number of operations to be performed in the operating room within a day in the planning horizon is also constant. However, considering the variability in this study, it is possible that there will be an increase in operation times or an increase in waiting rates. Therefore, there will be a decrease in the number of operations to be performed in operating rooms. Therefore, it is natural that the utilization rate is lower in this study compared to the deterministic model. Taking into account the health history of the patient in this study caused the variability to differ. For this reason, considering the situation under the name of variability, operating rooms are still used effectively. The results of the non-linear and the linear models of this study are very close and exhibit similar behavior as having the same hills and dips in the same schedule. Furthermore, Gür et al. (2019) Obtaining a close course shows that the results of this study are effective.
In this study, considering the variability in operation times and examining the utilization rates of operating rooms, it is seen that effective results are produced for hospitals. Hospital managers need to plan their strategies by taking into account the disruptions that may occur in operating rooms in these environments where variability is high. For this reason, since the efficiency of the entire system must be optimized, this study emphasizes that the health history of the patients should not be ignored and its important impact on variability. Considering the studies in the literature, it is seen in this study that as the variability in operation times increases, more accurate results are produced in the actual use of operating rooms. It is thought that modeling the variability and the factors that cause uncertainty in the operating times taken into account in this study provides a balance of timely responses to patients on the waiting list. When looking at the literature, no other study was found that specifically took this variability into account. The study makes a significant contribution to both the literature and real life by taking each patient into special consideration and modeling the variability according to health history, as well as creating applicable schedules.
In this study, uncertainties in operation times due to the reasons experienced in operating rooms were taken into consideration. Causes such as case cancelations, prolongation of the operations of the operating rooms and the surgical team, and emergency cases cause uncertainty in the operation times (Pang et al. 2018; Liu et al. 2018; Wang et al. 2018). The uncertainties in the operation times considered in the study are modeled as chance constraint. A stochastic model is proposed by taking advantage of the modeling power of goal programming and constraint programming. It is aimed to ensure the reliability of the uncertainties experienced during the operation times. The reasons for uncertainty during the operation times were investigated. It has been observed that there are many factors that cause uncertainties. When these factors are considered on the basis of each operation, it is seen that the operation process is customized. Thus, when the uncertainty situation is considered separately for each operation, its effect on the utilization rates is shown in the schedules. In this study, the utilization rates of operating rooms were pointed out as performance criteria. The results show that as the alpha value increases, utilization rates increase. At the same time, the variability of the operation times according to the medical condition of each patient shows that the results obtained are more reliable and the plans made are more robust. This situation shows that effectiveness is increased for hospital managers. As the alpha value changes in chance-constraint programming, the utilization rates in operating rooms also change. In this case, the alpha value, which provides the most efficient utilization rate, gives us the result that the operations are scheduled in the most appropriate way. Effective use of these units, which generate the most income for hospital managers, is important for increasing satisfaction. Reallife situations are tried to be reflected, constraints are established, and targets are set. By using the flexibility of the goal programming method, it is allowed to deviate from the model. Thus, these constraints were removed from being strict constraints and the situation was allowed to reflect the real-world variations. While creating the model, we tried to create a weekly schedule at the same time without complicating the structure of the problem with the time slot index. It is possible to increase the yields obtained from the operating rooms with the prepared schedules. When the activity performed in the operating rooms is examined within a wide time frame, it affects the activities in many other parts of the hospital. Therefore, the efficiency and efficiency of the schedules to be made come to the forefront.
7 Conclusion
One of the problems in today's hospitals is that surgeons are not able to enter the operations in a timely manner, causing the existing capacity of the hospital to be used effectively and decreasing the quality of service provided to the patients. At the same time, the inefficiency and inefficiency of the manual operating room schedules in the hospitals decreases the performance of the operating rooms and, thus, the performance of the hospital. From this point of view, the problem of operating room scheduling is discussed in this study. It is known that these units, which are among the most important units of the hospital, contain a lot of uncertainty in terms of their structure. Since it has been stated that there is a significant effect on resource allocation in the literature, this study focuses on the uncertainties over operation times. In the literature, there is no study that investigates the factors that cause uncertainty in operation times and reflects the variability on patient basis by taking these factors into consideration. This situation highlights the originality of the study. At the same time, it is thought that planning close to real life can be made when taken into consideration by the researchers. At this point, the study has a significant contribution to both literature and real life. It is aimed to increase the service quality of the operating rooms. At the same time, one of the aims of systematizing this scheduling, which is often done manually in the hospital, is to increase the patient/staff satisfaction by ensuring the efficient use of hospital resources.
A solution is proposed with chance-constraint constraint programming approaches for the effective use of operating rooms. Unlike the literature, the study combines the chance-constraint approach with goal programming and constraint programming methods. To reflect real life, the goal programming method that allows the stretching of hard constraints and constraint programming methods that allow the reflection of logical constraints are preferred. Data were obtained from a literature about the number of operating rooms, the number of operations on the waiting list and the number of surgical clinics of these operations. In addition to the effective and balanced use of the operating room, an operating room was required to be dedicated to only one specialty during all time periods.
The goals set was achieved by making effective planning to prevent inefficiencies that arise due to various reasons in the hospital and at the same time coordinating the hospital team and units. This shows that the methods help to systematize the process and are the means for achieving the desired objectives.
Further studies may take into account the special conditions of physicians in their working situations with the addition of different constraints. In addition, according to the preferences of surgeons, multi-criteria decision-making methods can be used for prioritization or a variety of situations can be considered, such as the reflection of staff-specific circumstances to constraints.
Availability of data and materials
There is no availability of data and materials in the study.
References
Ağpak K, Gökçen H (2007) A chance-constrained approach to stochastic line balancing problem. Eur J Oper Res 180(3):1098–1115. https://doi.org/10.1016/j.ejor.2006.04.042
Ahmadian MA, Varmazyar M, Fallahi AA (2019) Simulation-based general regression neural network-metaheuristic approach for operating theater room scheduling problem under uncertainty. Available at SSRN 4352098. https://doi.org/10.2139/ssrn.4352098
Andra A, Hajjah A (2020) Promethee method for decision support system. J Appl Bus Technol 1(1):60–68. https://doi.org/10.35145/jabt.v1i1.24
Apt K (2003) Principles of constraint programming. Cambridge University Press, Cambridge
Arenas M, Bilbao A, Caballero R, Gómez T, Rodriguez M, Ruiz F (2002) Analysis via goal programming of the minimum achievable stay in surgical waiting lists. J Oper Res Soc 53(4):387–396. https://doi.org/10.1057/palgrave.jors.2601310
Atalay KD, Apaydin A (2011) Deterministic equivalents of chance constrained stochastic programming problems. Anadolu Univ Sci Technol B Theor Sci 1(1):1–18
Azar M, Carrasco RA, Mondschein S (2022) Dealing with uncertain surgery times in operating room scheduling. Eur J Oper Res 299(1):377–394. https://doi.org/10.1016/j.ejor.2021.09.010
Barrera J, Carrasco RA, Mondschein S, Canessa G, Rojas-Zalazar D (2018) Operating room scheduling under waiting time constraints: the Chilean GES plan. Ann Oper Res. https://doi.org/10.1007/s10479-018-3008-7
Bedir N, Eren T (2015) AHP—PROMETHEE method with integration of personnel selection problem: a case study for the retail sector. Soc Sci Res J 4(4):46–58
Belkhamsa M, Jarboui B, Masmoudi M (2018) Two metaheuristics for solving no-wait operating room surgery scheduling problem under various resource constraints. Comput Ind Eng 126:494–506. https://doi.org/10.1016/j.cie.2018.10.017
Brans JP, De Smet Y (2016) PROMETHEE methods. In: Multiple criteria decision analysis. Springer, New York, pp 187–219. https://doi.org/10.1007/978-1-4939-3094-4_6
Breuer DJ, Lahrichi N, Clark DE, Benneyan JC (2020) Robust combined operating room planning and personnel scheduling under uncertainty. Oper Res Health Care 27:100276. https://doi.org/10.1016/j.orhc.2020.100276
Bukchin Y, Raviv T (2018) Constraint programming for solving various assembly line balancing problems. Omega 78:57–68. https://doi.org/10.1016/j.omega.2017.06.008
Cappanera P, Visintin C, Banditori F (2016) Addressing conflicting stakeholders’ priorities in surgical scheduling by goal programming. Flex Serv Manuf J. https://doi.org/10.1007/s10696-016-9255-5
Cardoen B, Demeulemeester E, Beliën J (2010) Operating room planning and scheduling: a literature review. Eur J Oper Res 201(3):921–932. https://doi.org/10.1016/j.ejor.2009.04.011
Charnes A, Cooper WW (1959) Chance-constrained programming. Manage Sci 6(1):73–79. https://doi.org/10.1287/mnsc.6.1.73
Dai Z, Perera SC, Wang JJ, Mangla SK, Li G (2023) Elective surgery scheduling under uncertainty in demand for intensive care unit and inpatient beds during epidemic outbreaks. Comput Ind Eng 176:108893. https://doi.org/10.1016/j.cie.2022.108893
Davoudkhania M, Hamidb M, Tavakkoli-Moghaddamb R, Bastanb M, Mahdi M (2019) A two-step stochastic optimization and simulation approach for scheduling operating rooms in an ophthalmology surgery department. In: International conference on industrial engineering and operations management, p 43
Erdem E, Qu X, Shi J (2012) Rescheduling of elective patients upon the arrival of emergency patients. Decis Support Syst 54(1):551–563. https://doi.org/10.1016/j.dss.2012.08.002
Eren T, Gür Ş (2018) Evaluation of the factors affecting the performance of operating room by fuzzy AHP. Harran Univ J Eng 3(3):197–204
Focacci F, Laburthe F, Lodi A (2003) Local search and constraint programming. In: Handbook of metaheuristics. Springer, pp 369–403. https://doi.org/10.1007/0-306-48056-5_13
Gerami F, Saidi-Mehrabad M (2017) Stochastic reactive scheduling model for operating rooms considering the moral and human virtues. Appl Ecol Environ Res 15(3):563–592
Guerriero F, Guido R (2011) Operational research in the management of the operating theatre: a survey. Health Care Manag Sci 14(1):89–114. https://doi.org/10.1007/s10729-010-9143-6
Guo C, Bodur M, Aleman DM, Urbach DR (2019) Logic-based benders decomposition and binary decision diagram based approaches for stochastic distributed operating room scheduling. INFORMS J Comput. https://doi.org/10.1287/ijoc.2020.1036
Gür Ş, Eren T (2018a) Application of operational research techniques in operating room scheduling problems: literature overview. J Healthc Eng. https://doi.org/10.1155/2018/5341394
Gür Ş, Eren T (2018b) Scheduling and planning in service systems with goal programming: Literature review. Mathematics 6(11):265. https://doi.org/10.3390/math6110265
Gür Ş, Hamurcu M, Eren T (2016) Using analytic network process and goal programming methods for project selection in the public institution. Les Cahiers Du MECAS 13:36–51
Gür Ş, Eren T, Alakaş HM (2019) Surgical operation scheduling with goal programming and constraint programming: a case study. Mathematics 7(3):251. https://doi.org/10.3390/math7030251
Gür Ş, Pınarbaşı M, Alakaş HM, Eren T (2022) Operating room scheduling with surgical team: a new approach with constraint programming and goal programming. Central Eur J Oper Res. https://doi.org/10.1007/s10100-022-00835-z
Hamid M, Nasiri MM, Werner F, Sheikhahmadi F, Zhalechian M (2019) Operating room scheduling by considering the decision-making styles of surgical team members: a comprehensive approach. Comput Oper Res 108:166–181. https://doi.org/10.1016/j.cor.2019.04.010
Hasannia-Kolagar, S., Asadi-Gangraj, E., Paydar, M. M., & Nikbakhsh, N. (2021). Robust Bi-Objective Operating Rooms Scheduling Problem Regarding the Shared Resources. Scientia Iranica.
Huang C, Ye S, Shuai S, Wei M, Zhou Y, Aibin A, Aibin M (2023) Emergency surgical scheduling model based on moth-flame optimization algorithm. In: 2023 ınternational conference on computing, networking and communications (ICNC). IEEE, pp 89–94
Internet Source (2020) https://www.medikalnews.com/cerrahin-hizi-ameliyat-suresi-ve-kalitesi/ Accessed 15 Nov 2020
Jebali A, Diabat A (2015) A stochastic model for operating room planning under capacity constraints. Int J Prod Res 53(24):7252–7270. https://doi.org/10.1080/00207543.2015.1033500
Jebali A, Diabat A (2017) A Chance-constrained operating room planning with elective and emergency cases under downstream capacity constraints. Comput Ind Eng 114:329–344. https://doi.org/10.1016/j.cie.2017.07.015
Jharkharia S, Shankar R (2007) Selection of logistics service provider: an analytic network process (ANP) approach. Omega 35(3):274–289. https://doi.org/10.1016/j.omega.2005.06.005
Kamran MA, Karimi B, Dellaert N, Demeulemeester E (2019) Adaptive operating rooms planning and scheduling: a rolling horizon approach. Oper Res Health Care 22:100200. https://doi.org/10.1016/j.orhc.2019.100200
Kayvanfar V, Akbari Jokar MR, Rafiee M, Sheikh S, Iranzad R (2021) A new model for operating room scheduling with elective patient strategy. INFOR Inf Syst Oper Res. https://doi.org/10.1080/03155986.2021.1881359
Kumar A, Costa AM, Fackrell M, Taylor PG (2018) A sequential stochastic mixed integer programming model for tactical master surgery scheduling. Eur J Oper Res 270(2):734–746. https://doi.org/10.1016/j.ejor.2018.04.007
Landa P, Aringhieri R, Soriano P, Tànfani E, Testi A (2016) A hybrid optimization algorithm for surgeries scheduling. Oper Res Health Care 8:103–114. https://doi.org/10.1016/j.orhc.2016.01.001
Latorre-Núñez G, Lüer-Villagra A, Marianov V, Obreque C, Ramis F, Neriz L (2016) Scheduling operating rooms with consideration of all resources, post anesthesia beds and emergency surgeries. Comput Ind Eng 97:248–257. https://doi.org/10.1016/j.cie.2016.05.016
Lee S, Yih Y (2014) Reducing patient-flow delays in surgical suites through determining start-times of surgical cases. Eur J Oper Res 238(2):620–629. https://doi.org/10.1016/j.ejor.2014.03.043
Lin YK, Li MY (2021) Solving operating room scheduling problem using artificial bee colony algorithm. Healthcare 9(2):152. https://doi.org/10.3390/healthcare9020152
Liu H, Zhang T, Luo S, Xu D (2018) Operating room scheduling and surgeon assignment problem under surgery durations uncertainty. Technol Health Care 26(2):297–304
Meade LM, Presley A (2002) R&D project selection using the analytic network process. IEEE Trans Eng Manage 49(1):59–66. https://doi.org/10.1109/17.985748
M’Hallah R, Visintin F (2019) A stochastic model for scheduling elective surgeries in a cyclic master surgical schedule. Comput Ind Eng 129:156–168. https://doi.org/10.1016/j.cie.2019.01.030
Miao H, Wang JJ (2023) Distributed surgical scheduling across collaborating hospitals considering stochastic duration and emergency demand. Comput Ind Eng 183:109462. https://doi.org/10.1016/j.cie.2023.109462
Molina-Pariente JM, Hans EW, Framinan JM (2018) A stochastic approach for solving the operating room scheduling problem. Flex Serv Manuf J 30(1–2):224–251. https://doi.org/10.1007/s10696-016-9250-x
Monteiro T, Meskens N, Wang T (2015) Surgical scheduling with antagonistic human resource objectives. Int J Prod Res 53(24):7434–7449. https://doi.org/10.1080/00207543.2015.1082040
Moosavi A, Ozturk O (2020) Metaheuristics for the operating theater planning and scheduling: a systematic review. Artif Intell. https://doi.org/10.48550/arXiv.2008.04970
Najjarbashi A, Lim GJ (2020) A decomposition algorithm for the two-stage chance-constrained operating room scheduling problem. IEEE Access 8:80160–80172. https://doi.org/10.1109/ACCESS.2020.2991031
Namba Y, Ito M, Takashima R (2023) A robust optimization for a single operating room scheduling problem with uncertain durations
Nasiri MM, Shakouhi F, Jolai F (2019) A fuzzy robust stochastic mathematical programming approach for multi-objective scheduling of the surgical cases. Opsearch. https://doi.org/10.1007/s12597-019-00379-y
Nazif H (2018) Operating room surgery scheduling with fuzzy surgery durations using a metaheuristic approach. Adv Oper Res 2018:1–8. https://doi.org/10.1155/2018/8637598
Neyshabouri S, Berg BP (2017) Two-stage robust optimization approach to elective surgery and downstream capacity planning. Eur J Oper Res 260(1):21–40. https://doi.org/10.1016/j.ejor.2016.11.043
Noorizadegan M, Seifi A (2018) An efficient computational method for large scale surgery scheduling problems with chance constraints. Comput Optim Appl 69(2):535–561. https://doi.org/10.1007/s10589-017-9947-0
Otten M, Braaksma A, Boucherie RJ (2019) Minimizing earliness/tardiness costs on multiple machines with an application to surgery scheduling. Oper Res Health Care 22:100194. https://doi.org/10.1016/j.orhc.2019.100194
Pang B, Xie X, Song Y, Luo L (2018) Surgery scheduling under case cancellation and surgery duration uncertainty. IEEE Trans Autom Sci Eng 16(1):74–86. https://doi.org/10.1109/TASE.2018.2834486
Park J, Kim BI, Eom M, Choi BK (2021) Operating room scheduling considering surgeons’ preferences and cooperative operations. Comput Ind Eng 157:107306. https://doi.org/10.1016/j.cie.2021.107306
Rahimi I, Gandomi AH (2020) A comprehensive review and analysis of operating room and surgery scheduling. Arch Comput Methods Eng. https://doi.org/10.1007/s11831-020-09432-2
Rahimi A, Hejazi SM, Zandieh M, Mirmozaffari M (2023) A novel hybrid simulated annealing for no-wait open-shop surgical case scheduling problems. Appl Syst Innov 6(1):15. https://doi.org/10.3390/asi6010015
Saadouli H, Jerbi B, Dammak A, Masmoudi L, Bouaziz A (2015) A stochastic optimization and simulation approach for scheduling operating rooms and recovery beds in an orthopedic surgery department. Comput Ind Eng 80:72–79. https://doi.org/10.1016/j.cie.2014.11.021
Saaty TL (1996) Decision making with dependence and feedback: the analytic network process, vol 4922. RWS Publ.
Saaty TL, Vargas LG (2006) Decision making with the analytic network process, vol 282. Springer Science+ Business Media, LLC. https://doi.org/10.1007/978-1-4614-7279-7
Schouten AM, Flipse SM, van Nieuwenhuizen KE, Jansen FW, van der Eijk AC, van den Dobbelsteen JJ (2023) Operating room performance optimization metrics: a systematic review. J Med Syst 47(1):19. https://doi.org/10.1007/s10916-023-01912-9
Sevinc A, Gür Ş, Eren T (2018) Analysis of the difficulties of SMEs in industry 4.0 applications by analytical hierarchy process and analytical network process. Processes 6(12):264. https://doi.org/10.3390/pr6120264
Sigurpalsson AO, Runarsson TP, Saemundsson RJ (2019) Stochastic master surgical scheduling under ward uncertainty. In: International conference on human-centred software engineering. Springer, Cham, pp 163–176. https://doi.org/10.1007/978-3-030-39694-7_13
Silva TA, de Souza MC (2020) Surgical scheduling under uncertainty by approximate dynamic programming. Omega 95:102066. https://doi.org/10.1016/j.omega.2019.05.002
Taş M, Özlemiş ŞN, Hamurcu M, Eren T (2017) Selection of monorail projects by using analytic hierarchy process and goal programming combined model. Harran Univ Eng J 2(2):24–34. https://hdl.handle.net/20.500.12587/7065
Tsang MY, Shehadeh KS, Curtis FE, Hochman B, Brentjens TE (2022) Stochastic optimization approaches for an operating room and anesthesiologist scheduling problem. arXiv:2204.11374. https://doi.org/10.48550/arXiv.2204.11374
Vali-Siar MM, Gholami S, Ramezanian R (2018) Multi-period and multi-resource operating room scheduling under uncertainty: a case study. Comput Ind Eng 126:549–568. https://doi.org/10.1016/j.cie.2018.10.014
Van Oostrum JM, Bredenhoff E, Hans EW (2010) Suitability and managerial implications of a master surgical scheduling approach. Ann Oper Res 178(1):91–104. https://doi.org/10.1007/s10479-009-0619-z
Vandenberghe M, De Vuyst S, Aghezzaf EH, Bruneel H (2019) Surgery sequencing to minimize the expected maximum waiting time of emergent patients. Eur J Oper Res 275(3):971–982. https://doi.org/10.1016/j.ejor.2018.11.073
Vandenberghe M, Vuyst SD, Aghezzaf EH, Bruneel H (2020) Stochastic surgery selection and sequencing under dynamic emergency break-ins. J Oper Res Soc. https://doi.org/10.1080/01605682.2020.1718559
Varmazyar M, Akhavan-Tabatabaei R, Salmasi N, Modarres M (2020) Operating room scheduling problem under uncertainty: application of continuous phase-type distributions. IISE Trans 52(2):216–235. https://doi.org/10.1080/24725854.2019.1628372
Wang Y, Tang J, Fung RY (2014) A column-generation-based heuristic algorithm for solving operating theater planning problem under stochastic demand and surgery cancellation risk. Int J Prod Econ 158:28–36. https://doi.org/10.1016/j.ijpe.2014.07.015
Wang J, Guo H, Bakker M, Tsui KL (2018) An integrated approach for surgery scheduling under uncertainty. Comput Ind Eng 118:1–8. https://doi.org/10.1016/j.cie.2018.02.017
Wang S, Li J, Mehrotra S (2019) Chance-constrained bin packing problem with an application to operating room planning. Optimization. https://doi.org/10.1287/ijoc.2020.1010
Wang K, Yu C, Qin H (2022) An adaptive-learning-based genetic algorithm for collaborative scheduling of distributed operating rooms. Appl Soft Comput 131:109755. https://doi.org/10.1016/j.asoc.2022.109755
Wang JJ, Dai Z, Zhang W, Shi JJ (2023) Operating room scheduling for non-operating room anesthesia with emergency uncertainty. Ann Oper Res 321(1–2):565–588. https://doi.org/10.1007/s10479-022-04870-6
Xiao Y, Yoogalingam R (2022) A simulation optimization approach for planning and scheduling in operating rooms for elective and urgent surgeries. Oper Res Health Care 35:100366. https://doi.org/10.1016/j.orhc.2022.100366
Xiao G, van Jaarsveld W, Dong M, van de Klundert J (2016) Stochastic programming analysis and solutions to schedule overcrowded operating rooms in China. Comput Oper Res 74:78–91. https://doi.org/10.1016/j.cor.2016.04.017
Yuniartha DR, Hans FR, Masruroh NA, Herliansyah MK (2023) Adapting duration categorical value to accommodate duration variability in a next-day operating room scheduling. Informa Med Unlocked 37:101180. https://doi.org/10.1016/j.imu.2023.101180
Zhang J, Dridi M, El Moudni A (2019) A two-level optimization model for elective surgery scheduling with downstream capacity constraints. Eur J Oper Res 276(2):602–613. https://doi.org/10.1016/j.ejor.2019.01.036
Zhang J, Dridi M, El Moudni A (2020) Column-generation-based heuristic approaches to stochastic surgery scheduling with downstream capacity constraints. Int J Prod Econ. https://doi.org/10.1016/j.ijpe.2020.107764
Zhu S, Fan W, Yang S, Pei J, Pardalos PM (2019) Operating room planning and surgical case scheduling: a review of literature. J Comb Optim 37(3):757–805. https://doi.org/10.1007/s10878-018-0322-6
Zhu S, Fan W, Yang S, Pardalos PM (2023) Scheduling operating rooms of multiple hospitals considering transportation and deterioration in mass-casualty incidents. Ann Oper Res 321(1–2):717–753. https://doi.org/10.1007/s10479-022-05094-4
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Data curation, ŞG; Methodology, SG, MP, HMA; Writing—original draft preparation, SG, MP, HMA, and TE; Validation, HMA, MP, and TE.
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest in the study.
Informed consent
In this study, there is no need to obtain informed consent as the personal rights of the patients were not shared.
Ethics approval and consent to participate
The study does not require an ethics approval and consent to participate.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1: Deterministic model
\(\sum_{k=1}^{r}\sum_{j=1}^{m}{x}_{ijk}=1 \quad \forall i,\) | (26) |
\(\sum_{j=1}^{m}\sum_{s=1}^{S}{y}_{jks} \le 6 \quad \forall k,\) | (27) |
\(\sum_{j=1}^{m}{y}_{jks} \le 6 \quad \forall k,\forall s,\) | (28) |
\(\sum_{i=1}^{n}{x}_{ijk} \le M* {y}_{jks } \quad \forall k,\forall s,\forall i,\) | (29) |
\(\sum_{k=1}^{r}{y}_{jks} \le M* {z}_{js} \quad \forall j,\forall s,\) | (30) |
\(\sum_{i=1}^{n}{p}_{i}{x}_{ijk}+{u}_{kj}^{-} -{u}_{kj}^{+}={U}_{kj} \quad \forall j,\forall k,\) | (31) |
\(\sum_{s=1}^{S}\sum_{k=1}^{r}{y}_{jks}+{k}_{j}^{-}-{k}_{j}^{+}=6 \quad \forall j,\) | (32) |
\(\sum_{k\in {d}_{s}}{y}_{jks}+{r}_{s}^{-}-{r}_{s}^{+}=0 \quad \forall s,\) | (33) |
\(\sum_{s=1}^{S}{z}_{js}+{p}_{j}^{-}-{p}_{j}^{+}=1 \quad \forall j.\) | (34) |
Appendix 2: PROMETHEE method steps (Park et al. 2021)
Step | Description |
|---|---|
Step 1 | Decision points and evaluation factors should be determined. The data set is created |
Step 2 | Preference functions are determined according to the criteria, alternatives are determined according to the characteristics sought in the criteria and preference functions are created. (Annex 1) |
Step 3 | Using the preference functions specified for the criteria, common preference functions are determined for alternative pairs \(P\left(a,b\right)=\left\{\begin{array}{c}0, f(a)\le f(b)\\ p[f\left(a\right),f\left(b\right), f(a)>f(b)\end{array}\right.\) \(p\left[f\left(a\right), f\left(b\right)\right]=p\left[x\right]\) \(p\left[x\right]=f\left(a\right)-f(b)\) |
Step 4 | At this step, preference indexes are determined for each alternative pair according to common preference functions \(\pi \left(a,b\right)={\sum }_{j=1}^{n}{w}_{j}*{P}_{j}(a,b)\) \(\pi \left(b,a\right)={\sum }_{j=1}^{n}{w}_{j}*{P}_{j}(b,a)\) |
Step 5 | At this stage, positive superiority (\({\phi }^{+}\)) and negative superiority (\({\phi }^{-}\)) are calculated for alternatives \(\mathrm{Pozitifak}{\i}\mathrm{m}: {\phi }^{+}\left(a\right)=\sum \pi (a,b)\) \(\mathrm{Negatifak}{\i}\mathrm{m}: {\phi }^{-}\left(a\right)=\sum \pi (b,a)\) |
Step 6 | Partial priorities are determined with PROMETHEE I. Partial priorities enable the determination of preference of existing alternatives, alternatives that are not different from each other and alternatives that cannot be compared with each other If any of the following situations occur, option A is preferred to option B \({\phi }^{+}\left(a\right)>{\phi }^{+}\left(b\right) ve {\phi }^{-}\left(a\right)<{\phi }^{-}\left(b\right)\) \({\phi }^{+}\left(a\right)>{\phi }^{+}\left(b\right) ve {\phi }^{-}\left(a\right)={\phi }^{-}\left(b\right)\) \({\phi }^{+}\left(a\right)={\phi }^{+}\left(b\right) ve {\phi }^{-}\left(a\right)<{\phi }^{-}\left(b\right)\) If the following conditions are met, option A and option B are indistinguishable from each other \({\phi }^{+}\left(a\right)={\phi }^{+}\left(b\right) ve {\phi }^{-}\left(a\right)={\phi }^{-}\left(b\right)\) If the following conditions are met, option A and option B are indistinguishable from each other \({\phi }^{+}\left(a\right)>{\phi }^{+}\left(b\right) ve {\phi }^{-}\left(a\right)>{\phi }^{-}\left(b\right)\) \({\phi }^{+}\left(a\right)<{\phi }^{+}\left(b\right) ve {\phi }^{-}\left(a\right)<{\phi }^{-}\left(b\right)\) |
Step 7 | Full priorities for existing alternatives with PROMETHEE II are calculated with the formula given below. With the exact priority values calculated, all alternatives are evaluated on the same plane and the exact ranking is determined \(\phi \left(a\right)={\phi }^{+}\left(a\right)-{\phi }^{-}\left(a\right)\) |
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gür, Ş., Alakaş, H.M., Pınarbaşı, M. et al. Stochastic operating room scheduling: a new model for solving problem and an approach for determining the factors that affect operation time variations. Soft Comput 28, 3987–4007 (2024). https://doi.org/10.1007/s00500-023-09369-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00500-023-09369-1