
Abstract
Background
Nutritional status assessment in children with nephrotic syndrome (NS) is critical for identifying patients who are at risk of protein-energy wasting (PEW) and for determining their nutritional needs and monitoring nutritional intervention outcomes.
Methods
In a case–control study, we enrolled 40 children (age range: 2–16 years) with NS and 40 apparently healthy children (age and sex-matched) as a control group. Anthropometric data, as well as demographic, clinical, and laboratory data, were collected. A dietary intake assessment using a 3-day food intake record was done, and the quadriceps rectus femoris thickness (QRFT) and quadriceps vastus intermedius thickness (QVIT) were assessed using B-mode ultrasound and compared between both groups.
Results
Children with NS had lower QRFT and QVIT measurements than control groups (p < 0.001). Inadequacy in protein intake occurred in 62.5% and 27.5% of the NS and control groups, respectively (p = 0.002). The thickness of the rectus and vastus muscles by ultrasound was significantly associated with the percentage of protein intake (p < 0.001). The ROC curve revealed that the best cutoff value of QRFT for the prediction of the patient at risk of malnutrition was ≤ 1.195 with an area under curve of 0.907, with p < 0.001.
Conclusion
In children with NS, skeletal muscle ultrasound is a simple and easy-to-use bedside technique for the identification of patients at risk of malnutrition.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nephrotic syndrome (NS) is a common kidney disorder in children that causes proteinuria, hypoalbuminemia, and edema [1]. In healthy children, the annual incidence of NS is estimated to be two to seven new cases per 100,000 under the age of 18 [2].
Malnutrition is more common in children with NS because they are prone to both macro and micronutrient deficiencies, putting them at risk for stunted growth, muscle loss, and cognitive impairment. The disease process, poor dietary intake, and steroid therapy all contribute to nutritional impairment [3]. Nutrition is a modifiable risk factor for mortality in children with kidney abnormalities, and it should be checked on a regular basis.
The expert panel of the International Society of Renal Nutrition and Metabolism (ISRNM) has outlined four diagnostic criteria: biochemical criteria, low body weight, lower muscle mass, and lower protein and calorie intake. When three of the four are met, a diagnosis of protein-energy wasting (PEW) is made [4]. Proteinuria, in addition to the inflammation associated with chronic disease, can contribute to PEW, resulting in an accelerated loss of lean body mass (LBM), which can also have a negative impact on morbidity and mortality [5]. Protein-energy wasting associated with NS (neph-PEW) defines a specific metabolic pattern in patients with NS with elevated phosphorus, uric acid, blood urea, and lean tissue deficiency [6].
Pathophysiological studies have linked NS to a hypercatabolic state characterized by accelerated muscle mass loss as the increased hepatic synthesis is not enough to compensate for the total loss, resulting in a decreased rate of protein turnover of other protein pools and amino acid mobilization from muscle [6, 7].
The stimulatory effects of food and physical activity are critical in maintaining muscle mass. Amino acids and contractile activity are key stimuli for muscle protein synthesis, which is the main controlled variable regulating muscle mass [8]. Long-term steroid treatment in children with NS is known to increase risk of obesity, suppress protein synthesis, and have a detrimental impact on quality of life as well as augment the degradation of myofibrillar proteins [9]. Glucocorticoid-induced skeletal muscle atrophy causes fatigue in daily physical activities as well as a reduction in body movement, resulting in a decreased ability to perform physical activity [9]. Physical inactivity alters body composition and has been linked with increased inflammation and anabolic resistance [10].
The overall assessment of nutritional status is generally grounded on the patient’s history, physical assessment, evaluation of dietary intake, biochemical markers, and screening methods that provide a comprehensive representation of a patient’s protein and energy reserves, in addition to their nutritional risk with the goal of early detection and monitoring in patients at risk of muscle loss [11].
The current gold standard for clinical evaluation of nutritional intake in children with chronic kidney disease (CKD) is the 3-day diet history [12]. However, using it places an undue burden on responders, necessitating strong motivation, literacy, and the ability to analyze typical intake across several days. It also necessitates the participation of qualified nutritionists [13]. Moreover, food records are prone to systematic inaccuracies such as underreporting, as well as the tendency to influence and change eating habits during data collection, reducing the accuracy of consumption estimates [14].
Low muscle mass is one of the diagnostic requirements for malnutrition according to recent definitions [15, 16]. Several methodologies are available for the estimation of muscle mass for early detection and monitoring in patients at risk of muscle loss. Some of these techniques, such as bio-impedance analysis (BIA) and bio-impedance spectroscopy (BIS), allow for the assessment of muscle mass but are hampered by overhydration [17]. Other imaging-based methods (dual-energy X-ray absorptiometry (DEXA), magnetic resonance imaging (MRI), and computed tomography (CT)) are considered the “gold standard” techniques for evaluation of muscle mass, but their use is primarily limited to research purposes due to their high expense, inaccessibility at the bedside, exposure to radiation, and powerful magnetic fields [18].
More recently, muscle ultrasound (US) has become a popular method for bedside body composition analysis due to its portability, low price, easy accessibility, minimal training, and ease of use [19]. Data from these devices would lessen subjectivity in nutritionists’ assessments of muscularity, allowing for more sensitive screening for those at nutritional risk, better monitoring, and evaluation of nutrition interventions in hospitalized patients.
US measurements of quadriceps muscle, the single biggest skeletal muscle group in the body, are strongly correlated to muscle mass as determined by gold standard techniques. Particularly, DEXA data show that quadriceps femoris muscle thickness best correlates with fat-free mass [20] and seems to be as accurate as the estimation of muscle mass by CT or MRI [21]. Recently, it has been proposed that quadriceps femoris US is a valid and simple technique to measure muscle thickness in patients with acute kidney injury (AKI) and kidney failure [22, 23]. The same study found that even significant and fast fluid changes generated by kidney replacement treatment (KRT) in overhydrated patients had no effect on US quadriceps muscle thickness assessments [22].
There are currently no data on the use of the quadriceps femoris muscle US in children with NS. In the current study, we aimed to evaluate the utility of quadriceps femoris muscle US for the identification of children with NS at risk of malnutrition.
Patients and methods
Research design and patients
A case–control study was carried out between the periods of April 2021 and March 2022 at the nephrology unit of the pediatric department of Zagazig University Hospitals. The study included 40 children with NS aged 2 to 16 years who were on prednisone therapy and were initially diagnosed using clinical and laboratory data (generalized edema, serum protein/creatinine ratio > 2.0, dipstick urine protein, and serum albumin < 2.5 g/dL). The children were selected by a simple random method from our patient list. The control group consisted of 40 children who were apparently healthy children and presented to the outpatient general pediatric clinic for minor illnesses and a physical examination without proteinuria or overhydration. Children with co-existent comorbidities such as severe cardiovascular, respiratory, or hepatic disease, or cancer, were excluded from the study.
All children underwent full history-taking, and anthropometric measurements including dry weight and length were used for the calculation of the body mass index (BMI) as kg/m2.
Biochemical measurements
Blood serum cholesterol, serum albumin, total protein, prealbumin, serum creatinine, uric acid (UA), and phosphorus (Pi) were tested using the appropriate chemical analyzer. Estimated glomerular filtration rate (eGFR) was calculated based on the Schwartz formula.
Nutritional status assessment
A prospective 3-day food intake record was documented, which required the patient or family to keep track of everything the patient ate and drank in real time. Food records were analyzed using MyPlate Tracker from the U.S. Department of Agriculture, with a particular emphasis on the distribution of daily energy and protein intake in the children’s diets.
Food record analyses helped to compare the daily energy intake to recommended intake based on the calculations of estimated energy requirements (EERs) using age, sex, weight, and height (50th percentile height for weight) as well as a sedentary physical activity coefficient to estimate total energy needs while on steroids [24].
Percent contributions to total energy intake from protein were compared to the Acceptable Macronutrient Distribution Range (AMDR) for protein. According to the Food and Nutrition Board, Institute of Medicine, AMDR is defined as “a range of intakes for a particular energy source that is associated with reduced risk of chronic disease while providing adequate intakes of essential nutrients.” AMDR for protein range was based on 5–20% and 10–30% of energy intake for children aged 1 to 3 years and 4 to 18 years, respectively [24,25,26,27]. Patients with protein intakes lower than these recommended ranges are identified as being at risk of malnutrition.
US measurements
The thicknesses of the quadriceps rectus femoris (QRF) and vastus intermedius (QVI) were evaluated using B-mode ultrasound (Philips HD7xe) with a high-frequency linear array transducer (7.5 MHz). All cases were examined regarding the right QRF and QVI muscle thicknesses. The patient was lying supine with extended, relaxed knees, and toes directed upward. Maximum thickness of each QVI and QRF muscle was assessed from the femur to the muscle’s inner edge and from the subcutaneous layer to the QRF muscle’s inner border, respectively. Additionally, we kept a standard level where the muscle thickness was measured, at the level of two particular landmarks, the midpoint, and the border between the upper two-thirds and the lower third between the upper pole of the patella and the superior anterior iliac spine [22]. For each individual muscle, multiple measurements were taken, and a mean was calculated and used for further analysis. Special precautions were taken in all cases, including placing the transducer perpendicular to the long axis of the thigh in a fixed orientation and using enough contact gel to guard the muscle from excessive pressure and compression.
Statistical analysis
Statistical Package for Social Sciences was used to conduct the statistical analysis (SPSS version 20.0). According to the type of data, qualitative data is represented by numbers and percentages, while quantitative data is represented by mean and standard deviation. The following tests were used to determine the significance of differences: t-test for comparisons between parametric quantitative independent groups, Mann–Whitney in non-parametric, paired with paired t-test. The significance level was chosen at < 0.05 for significant results and < 0.001 for highly significant results.
Results
Clinical and demographic variables
The study included 40 children with NS and 40 participants within the control group. On comparing demographic data between both groups, there was a statistically non-significant difference between them concerning weight or height, though BMI was significantly higher among the NS group (median 18.85 kg/m2) compared to the control group (16.34 kg/m2). Disease duration ranged from 1 month to 14 years, with a median of 1 year (Table 1).
Biochemical measurements
The NS group had significantly lower serum total protein (mean 4.08 g/dL vs. 6.63 g/dL in the control group), albumin (mean 2.35 g/dL vs. 3.72 g/dL in the control group), and prealbumin (mean 9.18 g/dL vs. 18.39 g/dL in the control group). On the other hand, the NS group had significantly higher total cholesterol (mean 385.58 mg/dL vs. 140.25 mg/dL in the control group), serum uric acid (mean 5.27 mg/dL vs. 2.95 mg/dL in the control group), and serum phosphorus (mean 5.9 mg/dL vs. 3.74 mg/dL in the control group). There is a statistically non-significant difference between groups regarding serum creatinine and eGFR (Table 2).
Ultrasonographic measurements of muscle thickness
On US evaluation of rectus and vastus muscle thickness, both were significantly lower among the NS group. The mean of QRFT was 1.088 cm and 1.27 cm in NS and the control group, respectively, p = 0.01, and the mean of QVIT was 0.999 cm and 1.138 cm in NS and the control group, respectively, p = 0.017. Regarding subcutaneous fat thickness, it was significantly higher among the NS group (0.745 cm) vs. the control group (0.559 cm), p < 0.001 (Table 3).
Nutritional intake and muscle wasting
The percent of daily required energy and protein for the study participants and that actually received by them using food diary records were compared between the two groups. It revealed that the NS group received a significantly higher percent of energy (mean 105.23% vs. 91.55% control) and the median percent contribution to total energy intake from protein was lower in the NS group at 9.25% vs. 20% control, and only 37.5% of patients reached the recommended protein intake according to AMDR vs. 72.5% within the control group, p = 0.002 (Table 4).
Correlation study
The QRFT was significantly positively correlated to serum albumin, total protein, and percent of protein intake, while it was significantly negatively correlated with serum uric acid. Also, QVIT was significantly positively correlated to serum albumin and percent of protein intake, while it was significantly negatively correlated with serum uric acid (Table 5).
Factors associated with muscle loss
Only percent of protein intake was significantly independently associated with QRFT and QVIT in a linear stepwise regression analysis of factors significantly correlated with them (for rectus: unstandardized = 0.028, p < 0.001; for vastus: unstandardized = 0.02, p < 0.001) (Table 6).
Receiver operating characteristic (ROC) curve
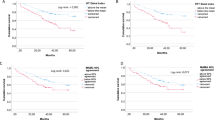
The ROC curve revealed that the best cutoff of QRFT for the prediction of patients at risk of malnutrition was ≤ 1.195 with AUC 0.907, sensitivity 86.1%, specificity 77.3%, positive predictive value 75.6%, negative predictive value 87.2%, and overall accuracy of 81.3% with p < 0.001(Fig. 1).

ROC curve showing performance of rectus in prediction of patient at risk of malnutrition
Discussion
Nutritional status is a crucial determining factor of growth in children with NS, and it must be assessed. There is a higher risk of poor nutritional status in children with NS than in children with other kidney diseases [28].
PEW increases the risk of morbidity and mortality in patients with CKD [29, 30]. The inflammation associated with PEW is a cardiovascular risk factor [12]. PEW in NS, like PEW in CKD, is related to an acceleration in atherosclerosis development, even in children [31]. Patients with severe NS hyperphosphatemia, hyperuricemia, and fluid overload have recognized independent risk factors of cardiovascular events as well [6]. Moreover, PEW causes the patient’s immune system to deteriorate and respond abnormally; as a result, the patient is more vulnerable to infections and their sequelae [32].
ISRNM criteria for PEW are inapplicable to NS, where the requirement of low serum albumin is achieved, yet BMI declines and weight loss is almost never seen, whereas weight increase owing to overhydration is common. Moreover, BMI does not allow for distinction between muscle mass and fat mass. Fluid retention may conceal changes in muscle mass or confound overall weight changes. As a result of these limitations, the loss of muscle mass may be underestimated, causing a failure to precisely distinguish patients who are malnourished or at risk of losing muscle mass and becoming malnourished. Therefore, we have outlined muscle US as a simple bedside method to help with nutritional assessment in this group.
Over the last decade, various methods have been utilized to assess the nutritional status in patients with CKD. However, there is a paucity of data on nutritional status in children with NS, and data concerning US use in NS is limited. To our knowledge, this has been the first clinical study to use this method to permit the early diagnosis of patients with low muscle mass and at risk for the progression to PEW, using a simple tool that can be provided at the patient’s bedside.
In the present study, 40 patients with NS and 40 controls were recruited. BMI was significantly higher in nephrotic children as compared to the healthy control group in agreement with Raikwar et al. and Kuźma-Mroczkowska et al. [33, 34] who concluded that long term (at least 6 months) glucocorticoid therapy is accountable for higher BMI in patients with NS.
In our study, patients with NS had features of hypercatabolism (higher Pi and UA) when compared to the control group. This agrees with a previous study where the NS group presented with elevated phosphorus (p = 0.029), uric acid (p = 0.002), and blood urea (p = 0.049) in comparison with the controls [6]. Hyperphosphatemia and hyperuricemia are well-known hypercatabolism indicators. Feinstein et al. proposed that urinary insulin growth factor 1 excretion and its impacts on higher tubular phosphate retention could be a potential mechanism of phosphorus level elevation in such children [35]. However, as seen in rhabdomyolysis and tumor lysis syndrome, increased cellular mass catabolism could be a further source of serum phosphate [36]. Medications like steroids and diuretics may have a role in uric acid metabolism [10, 37]. Hyperuricemia in children with primary NS was reported as a risk factor for progression to kidney failure [38, 39]. However, in the current study, there is a statistically non-significant difference between groups regarding serum creatinine or eGFR.
Our study revealed that US measurements of rectus and vastus muscle thickness were significantly lower in children with NS than in the control group. This agrees with previous studies that found patients with NS had a significantly lower LBM than the control group by using the BIS [6, 33].
In our case, interstitial edema did not affect muscle size as there was no characteristic ultrasound appearance of hypoechoic muscle edema (which would increase muscle bulk and thickness in its presence) noticed. Only some cases showed subcutaneous edema evident by linear hypoechoic streaks inside echogenic subcutaneous fat. This supports our results regarding significantly lower QRFT and QVIT (absent muscle edema) and higher SC fat thickness (due to SC edema) in the NS group when compared to the control group. This also agrees with another reliability study on quadriceps muscle thickness values measured by US before and after KRT, which found no difference, indicating that even in chronically hyperhydrated patients, US is unaffected by fluid overload and quick and relevant fluid changes [22, 23].
In our study, the NS group received significantly higher percentage of energy and lower percentage of protein, which may be attributed to the consumption of cheap sources of energy like bread in the presence of the extra burden of medication and medical costs in our developing country. Poverty and multiple acute or chronic comorbidities may also play a role in suboptimal nutrient intake [40]. Moreover, one result of the Chronic Kidney Disease in Children (CKiD) study showed that CKD children eat a lot of “empty calorie” foods like fast food, chips (crisps), and other snack foods. Even though they consumed proper macronutrient ranges, their food choices providing the macronutrients were poor on average [41, 42]. In adult studies, a low-protein diet has been shown to help reduce proteinuria [19, 43]. However, in order to ensure proper growth and development in most children and to prevent or treat PEW, increased protein intake closer to 0.8 g/kg/d may be required [44, 45]. Therefore, a balance should exist between cardiovascular/psychological outcomes, risks of being overweight and obesity, and appropriate energy and protein intake [46].
In our study, muscle thickness was significantly positively correlated with serum albumin and percent of protein intake, while it was significantly negatively correlated with serum uric acid, in agreement with Matyjek et al. [6] who found a strong negative correlation between lean tissue mass and blood urea concentration. These findings support the theory that those patients had augmented muscle protein degradation. Moreover, a prior study compared parenteral nutrition with an amino acid intake of 0.8 g/kg/day or 1.2 g/kg/day among 119 critically ill patients and concluded that higher amino acid intake was linked to a significant increase in forearm muscle thickness as measured by ultrasound [47]. On the other hand, another observational study of 29 critically ill patients did not find a correlation between muscle loss and either caloric or protein debt over the first week [48].
According to our findings, the percentage of protein consumed was significantly associated with quadriceps muscle thickness as measured by US. The pathogenesis of muscle wasting in CKD is multifactorial. Inadequate nutrient intake, which is quite common in these patients, is recognized as the most important factor contributing to the development of muscle wasting [18].
The best cutoff of quadriceps muscle thickness as determined by the US in the prediction of patients at risk of malnutrition is 1.195 with an area under curve of 0.907, sensitivity of 86.1%, specificity of 77.3%, positive predictive value of 75.6%, negative predictive value of 87.2%, and overall accuracy of 81.3% with p < 0.001. Hence, muscular US are reliable, practical, and accessible tools beneficial for the estimation of muscle mass and for the follow-up of the nutritional status of patients with NS.
Strength and limitations
The current study has a number of strengths. The main strength is that this is the first study to use muscle US in children with NS for assessment of nutrition status. The findings of our study should serve as a reminder of the importance of routine nutritional assessment in children with NS for early detection, treatment, and nutritional rehabilitation counseling, all of which can contribute to a reduction in mortality. The present study also has some limitations. The sample size and the single-center sample are two limitations. However, the results of this study are quite interesting due to the extremely accurate information offered by ultrasonography. Future research must replicate this method with bigger sample sizes to verify lower limb muscle thickness in nutritional status assessment and to provide reference standards based on age and gender in children with NS. Prospective evaluation of US assessing changes in muscle status as a focus on the outcome of nutritional intervention in PEW treatment is highly recommended. On the other hand, other limitations of the present study are the unmeasured confounding effects that may still exist despite adjusting for potential confounders by multiple regressions and the absence of conclusive evidence from other markers of malnutrition. The validity of the ultrasonic assessment for determining nutritional profiles might be improved by more studies using confirmative samples of malnutrition in children with NS.
Conclusion
In children with NS, quadriceps femoris US could be a simple, precise, and non-invasive means of assessment of muscle wasting in patients with PEW. Consequently, utilizing a US technique in a clinical context should be taken into consideration for a quick screening of PEW risk.
Data availability
The datasets created and/or analyzed during the current work are accessible upon reasonable request from the corresponding author.
References
Downie ML, Gallibois C, Parekh RS, Noone DG (2017) Nephrotic syndrome in infants and children: pathophysiology and management. Paediatr Int Child Health 37:248–258
McCloskey O, Maxwell AP (2017) Diagnosis and management of nephrotic syndrome. Practitioner 261:11–15
Solarin AU, Adekunle MO, Olutekunbi OA, Lamina OM, Aremu OE, Animasahun AB, Njokanma FO (2018) Nutritional assessment of children with nephrotic syndrome in a tertiary institution: a case controlled study. Trop J Nephrol 13:97–103
Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, Franch H, Guarnieri G, Ikizler T, Kaysen G (2008) A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int 73:391–398
Kovesdy CP (2015) Nutritional management of protein-energy wasting in non-dialysis dependent chronic kidney disease: reconciling the dual goals of renoprotection and nutritional management. Acta Nephrol 29:134–140
Matyjek A, Literacki S, Niemczyk S, Rymarz A (2020) Protein energy-wasting associated with nephrotic syndrome–the comparison of metabolic pattern in severe nephrosis to different stages of chronic kidney disease. BMC Nephrol 21:1–11
De Meer K, Kulik W, Melissant CF, Rabelink TJ, Berger R, Kaysen GA (2000) Nephrotic proteinuria has no net effect on total body protein synthesis: measurements with 13C valine. Am J Kidney Dis 35:1149–1154
Bowden Davies KA, Pickles S, Sprung VS, Kemp GJ, Alam U, Moore DR, Tahrani AA, Cuthbertson DJ (2019) Reduced physical activity in young and older adults: metabolic and musculoskeletal implications. Ther Adv Endocrinol Metab 10:2042018819888824
Lee M-K, Jeong HH, Kim M-J, Ryu H, Baek J, Lee B (2022) Nutrients against glucocorticoid-induced muscle atrophy. Foods 11:687
Mandal AK, Mount DB (2015) The molecular physiology of uric acid homeostasis. Annu Rev Physiol 77:323–345
Marcelli D, Wabel P, Wieskotten S, Ciotola A, Grassmann A, Di Benedetto A, Canaud B (2015) Physical methods for evaluating the nutrition status of hemodialysis patients. J Nephrol 28:523–530
Nelms CL, Shaw V, Greenbaum LA, Anderson C, Desloovere A, Haffner D, Oosterveld MJ, Paglialonga F, Polderman N, Qizalbash L (2021) Assessment of nutritional status in children with kidney diseases—clinical practice recommendations from the Pediatric Renal Nutrition Taskforce. Pediatr Nephrol 36:995–1010
Ortega RM, Pérez-Rodrigo C, López-Sobaler AM (2015) Dietary assessment methods: dietary records. Nutr Hosp 31:38–45
Tucker KL (2007) Assessment of usual dietary intake in population studies of gene–diet interaction. Nutr Metab Cardiovasc Dis 17:74–81
Cederholm T, Bosaeus I, Barazzoni R, Bauer J, Van Gossum A, Klek S, Muscaritoli M, Nyulasi I, Ockenga J, Schneider S (2015) Diagnostic criteria for malnutrition–an ESPEN consensus statement. Clin Nutr 34:335–340
Cederholm T, Jensen GL, Correia MITD, Gonzalez MC, Fukushima R, Higashiguchi T, Baptista G, Barazzoni R, Blaauw R, Coats AJS, Crivelli AN, Evans DC, Gramlich L, Fuchs-Tarlovsky V, Keller H, Llido L, Malone A, Mogensen KM, Morley JE, Muscaritoli M, Nyulasi I, Pirlich M, Pisprasert V, de van der Schueren MAE, Siltharm S, Singer P, Tappenden K, Velasco N, Waitzberg D, Yamwong P, Yu J, Van Gossum A, Compher C, GLIM Core Leadership Committee, GLIM Working Group (2019) GLIM criteria for the diagnosis of malnutrition–a consensus report from the global clinical nutrition community. J Cachexia Sarcopenia Muscle 10:207–217
Carrero JJ, Johansen KL, Lindholm B, Stenvinkel P, Cuppari L, Avesani CM (2016) Screening for muscle wasting and dysfunction in patients with chronic kidney disease. Kidney Int 90:53–66
Sabatino A, D’Alessandro C, Regolisti G, di Mario F, Guglielmi G, Bazzocchi A, Fiaccadori E (2020) Muscle mass assessment in renal disease: the role of imaging techniques. Quant Imaging Med Surg 10:1672
Castellino P, Cataliotti A (2002) Changes of protein kinetics in nephrotic patients. Curr Opin Clin Nutr Metab Care 5:51–54
Menon MK, Houchen L, Harrison S, Singh SJ, Morgan MD, Steiner MC (2012) Ultrasound assessment of lower limb muscle mass in response to resistance training in COPD. Resp Res 13:1–10
Arbeille P, Kerbeci P, Capri A, Dannaud C, Trappe SW, Trappe TA (2009) Quantification of muscle volume by echography: comparison with MRI data on subjects in long-term bed rest. Ultrasound Med Biol 35:1092–1097
Sabatino A, Regolisti G, Bozzoli L, Fani F, Antoniotti R, Maggiore U, Fiaccadori E (2017) Reliability of bedside ultrasound for measurement of quadriceps muscle thickness in critically ill patients with acute kidney injury. Clin Nutr 36:1710–1715
Sabatino A, Regolisti G, Delsante M, Di Motta T, Cantarelli C, Pioli S, Grassi G, Batini V, Gregorini M, Fiaccadori E (2019) Noninvasive evaluation of muscle mass by ultrasonography of quadriceps femoris muscle in end-stage renal disease patients on hemodialysis. Clin Nutr 38:1232–1239
Polderman N, Cushing M, McFadyen K, Catapang M, Humphreys R, Mammen C, Matsell DG (2021) Dietary intakes of children with nephrotic syndrome. Pediatr Nephrol 36:2819–2826
Santarpia L, Contaldo F, Pasanisi F (2017) Dietary protein content for an optimal diet: a clinical view. J Cachexia Sarcopenia Muscle 8:345–348
Wolfe RR, Cifelli AM, Kostas G, Kim I-Y (2017) Optimizing protein intake in adults: interpretation and application of the recommended dietary allowance compared with the acceptable macronutrient distribution range. Adv Nutr 8:266–275
Chang SO (2011) Dietary reference intakes for protein: protein requirement and estimation method, AMDR (Amount of Macronutrient Distribution Range), for protein. Korean J Nutr 44:338–343
Shaw V, Polderman N, Renken-Terhaerdt J, Paglialonga F, Oosterveld M, Tuokkola J, Anderson C, Desloovere A, Greenbaum L, Haffner D (2020) Energy and protein requirements for children with CKD stages 2–5 and on dialysis–clinical practice recommendations from the Pediatric Renal Nutrition Taskforce. Pediatr Nephrol 35:519–531
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY (2004) Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Eng J Med 351:1296–1305
Collins AJ, Foley RN, Herzog C, Chavers BM, Gilbertson D, Ishani A, Kasiske BL, Liu J, Mau L-W, McBean M (2010) United States Renal Data System 2009 Annual Data Report. Am J Kidney Dis 55:S1–S420
Skrzypczyk P, Kuźma-Mroczkowska E, Kułagowska J, Brzewski M, Okarska-Napierała M, Pańczyk-Tomaszewska M (2019) Carotid intima-media thickness in children with idiopathic nephrotic syndrome: a single center cross-sectional study. Clin Nephrol 91:353
Gracia-Iguacel C, González-Parra E, Barril-Cuadrado G, Sánchez R, Egido J, Ortiz-Arduán A, Carrero JJ (2014) Defining protein-energy wasting syndrome in chronic kidney disease: prevalence and clinical implications. Nefrología 34:507–519
Raikwar P, Kaur J, Parihar D, Batra APS (2019) Body composition analysis in nephrotic syndrome patients- a case control study in a tertiary care hospital of Haryana. In: GJRA - Global Journal For Research Analysis. https://www.worldwidejournals.com/global-journal-for-research-analysis-GJRA/article/body-composition-analysis-innephrotic-syndrome-patients-a-case-control-study-in-a-tertiary-care-hospital-of-haryana/MTEyODc=/?is=1. Accessed 15 May 2022
Kuźma-Mroczkowska E, Pańczyk-Tomaszewska M, Skrzypczyk P, Artemiuk I, Roszkowska-Blaim M (2016) Body weight changes in children with idiopathic nephrotic syndrome. Dev Period Med 20:16–22
Feinstein S, Becker-Cohen R, Rinat C, Frishberg Y (2006) Hyperphosphatemia is prevalent among children with nephrotic syndrome and normal renal function. Pediatr Nephrol 21:1406–1412
Cairo MS, Bishop M (2004) Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol 127:3–11
Liu C, Zhen Y, Zhao Q, Zhai J-L, Liu K, Zhang J-X (2016) Prednisone lowers serum uric acid levels in patients with decompensated heart failure by increasing renal uric acid clearance. Can J Physiol Pharmacol 94:797–800
Xiao H, Li Q, Wang F, Yao Y, Zhong X (2014) Relationship between hyperuricemia and primary nephrotic syndrome in children. Chin J Pediatr 52:859–862
Song SH, Oh TR, Choi HS, Kim CS, Ryu DR, Kim SG, Park S-H, Ma SK, Kim SW, Bae EH (2021) Hyperuricemia is a risk factor for the progression to end-stage renal disease in minimal change disease. Kidney Res Clin Pract 40:411
Hahn D, Hodson EM, Fouque D (2018) Low protein diets for non-diabetic adults with chronic kidney disease. CDSR. https://doi.org/10.1002/14651858.CD001892.pub4
Chen W, Ducharme-Smith K, Davis L, Hui WF, Warady BA, Furth SL, Abraham AG, Betoko A (2017) Dietary sources of energy and nutrient intake among children and adolescents with chronic kidney disease. Pediatr Nephrol 32:1233–1241
Hui WF, Betoko A, Savant JD, Abraham AG, Greenbaum LA, Warady B, Moxey-Mims MM, Furth SL (2017) Assessment of dietary intake of children with chronic kidney disease. Pediatr Nephrol 32:485–494
Giordano M, De Feo P, Lucidi P, Depascale E, Giordano G, Cirillo D, Dardo G, Santo Signorelli S, Castellino P (2001) Effects of dietary protein restriction on fibrinogen and albumin metabolism in nephrotic patients. Kidney Int 60:235–242
Al-Bander H, Kaysen GA (1991) Ineffectiveness of dietary protein augmentation in the management of the nephrotic syndrome. Pediatr Nephrol 5:482–486
Eskandarifar A, Fotoohi A, Mojtahedi SY (2017) Nutrition in pediatric nephrotic syndrome. J Pediatr Nephrol 5:1–3
Rodig NM, McDermott KC, Schneider MF, Hotchkiss HM, Yadin O, Seikaly MG, Furth SL, Warady BA (2014) Growth in children with chronic kidney disease: a report from the Chronic Kidney Disease in Children study. Pediatr Nephrol 29:1987–1995
Ferrie S, Allman-Farinelli M, Daley M, Smith K (2016) Protein requirements in the critically ill: a randomized controlled trial using parenteral nutrition. JPEN J Parenter Enteral Nutr40:795–805
Pardo E, El Behi H, Boizeau P, Verdonk F, Alberti C, Lescot T (2018) Reliability of ultrasound measurements of quadriceps muscle thickness in critically ill patients. BMC Anesthesiol 18:1–8
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
All authors participated in the study conception and design. Material preparation, data gathering, and analysis were performed by MG, YY, MM, AA, LE, AE, and GA. The first draft of the manuscript was written by MG, and all authors commented on prior versions of the manuscript. The final manuscript was reviewed and approved by all authors.
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Pediatrics Department of Zagazig University Hospitals after the approval of the Institutional Review Board (ZU-IRB#6881). Informed consent was obtained from legal guardians. This research was done in agreement with the Code of Ethics of the World Scientific Association (Declaration of Helsinki) for studies including humans.
Conflicts of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gehad, M.H., Yousif, Y.M., Metwally, M.I. et al. Utility of muscle ultrasound in nutritional assessment of children with nephrotic syndrome. Pediatr Nephrol 38, 1821–1829 (2023). https://doi.org/10.1007/s00467-022-05776-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05776-y