
Abstract
Background
There seems to be a possible link between nephrotic syndrome (NS) and lymphoproliferative syndrome, but it remains poorly understood.
Methods
This multicentric and retrospective study focuses on children, who developed idiopathic NS and malignant or benign proliferation between 2000 and 2021.
Results
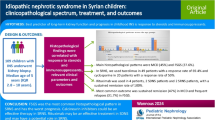
Eleven patients were included, with a median age of 4 years. Only one had a steroid-resistant nephrotic syndrome (SRNS). The maintenance therapy before the proliferation was in majority tacrolimus or mycophenolate mofetil (MMF), but three patients did not receive treatments. The proliferation was mainly a Hodgkin’s lymphoma (45%) or a lymphoproliferative disease (36%), in a median time after the NS of two years. Viruses were found in seven cases (EBV in five cases and HHV-8 in two).
Conclusion
The association between proliferative syndrome and idiopathic NS may not be fortuitous, possibly with a common lymphocytic disturbance. Genetic analyses could improve the comprehension of these manifestations in the future.
Graphical abstract
A higher resolution version of the Graphical abstract is available as Supplementary information

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Nephrotic syndrome (NS) has been known to pediatric nephrologists for several decades, but the pathophysiological mechanism has yet to be elucidated. Current hypotheses involve dysimmunity due to HLA system polymorphisms and/or triggered by a cross-reaction after EBV infection [1].
Few articles in the literature describe cancers that occur in patients with idiopathic NS. The rare cases described shared no common features: fibroadenoma, seminoma, malignant neuroma, and ovarian cancer [2, 3]. On the other hand, the association between NS with minimal change disease (MCD) and Hodgkin’s lymphoma has already been described in children [4, 5]. Nephrotic syndrome is considered to be paraneoplastic and could occur in less than 1% of the cases of Hodgkin's lymphoma [4, 5]. The link between these two pathologies remains poorly understood. Lymphocyte dysfunction could lead to cytokine secretion that alters the permeability of the glomerular basement membrane. It can be assumed that there is a common genetic predisposition to lymphoproliferative syndromes and NS in some children. In addition, EBV, which is potentially oncogenic, is also implicated in NS [1, 6].
Our study consisted of investigating benign and malignant proliferations that develop after the diagnosis of idiopathic NS. The aim of this study was to describe clinical features, management, and outcomes of patients with NS who presented a malignant or benign proliferation.
Methods
This is a multicenter retrospective observational cohort study. The pediatricians of the French Society of Pediatric Nephrology (SNP) were surveyed using a questionnaire which included a data collection form to be completed. There was no time limit for the period of inclusion.
We included patients younger than 18 years of age who developed idiopathic NS and malignant or benign proliferation concomitantly with or subsequent to the NS. Patients who had received a kidney transplant were excluded from the study. We recorded demographic data, medical history, and treatments received by the patients.
All patients diagnosed were treated according to the former SNP protocol with prednisone 60 mg/m2/day for 4 weeks, followed by prednisone 60 mg/m2 every other day for 8 weeks, and then by a reduction of 15 mg/m2 every other day at 2-week intervals (total treatment duration 18 weeks) [7].
Steroid responsiveness was defined, according to the French guidelines [7], as remission induced by oral prednisone (60 mg/m2 per day) over 4 weeks, followed by three methylprednisolone pulses of 1 g/1.73 m2 every other day in the case of persistent proteinuria by day 30. Conversely, steroid resistance was defined by persistent proteinuria after 4 weeks of oral prednisone plus three methylprednisolone pulses.
The presence of EBV in tumors was examined by in situ hybridization (EBER-1 probe) by PCR or by immunohistochemistry with detection of latent viral proteins (LMP-1). Detection of HHV8 RNA was made by PCR. It is unknown whether other viruses have been tested.
Results
Eleven (11) patients from 6 French pediatric nephrology centers (Toulouse, Bordeaux, Nantes, Paris Necker, Paris Robert Debré, Strasbourg) met the inclusion criteria between 2000 and 2021. The incidence of NS was about 90 to 100 new patients per year in all the 6 participating centers. Therefore, the estimated incidence of lymphoproliferation found in this study could be around 5 per 1000 children with idiopathic NS per year. These patients developed NS between the ages of 11 months and 16 years (median age 3 years, IQR 1–6). None of these patients have been reported previously.
Eight of 11 children underwent kidney biopsies that were performed within one year of the diagnosis of NS except for two, which were respectively performed 43 months and 53 months after diagnosis. The kidney histology showed MCD in 6/7 and focal segmental glomerulosclerosis (FSGS) in 1/7. Patient characteristics are presented in Table 1.
The patients had no personal history of immune or oncological disease. Only one patient had a family history of a sister with Sjogren’s syndrome. Few patients developed dysimmunities after the diagnosis of NS. One patient developed hyperthyroidism, and one developed hypogammaglobulinemia which required supplementation following rituximab therapy. Only one patient had a severe herpetic stomatitis 1 month before developing EBV-related lymphoproliferative syndrome (Table 2).
For 3 patients (27%), the diagnoses of NS and lymphoproliferative syndrome were almost simultaneous. Steroid-sensitive nephrotic syndrome (SSNS) and Hodgkin’s lymphoma were diagnosed at the same time and 2 months apart respectively in a 15-year-old male (patient 6) and a 12-year-old female patient (patient 3). Finally, for the third patient (patient 2) who was 1 year old at the time of diagnosis, it was difficult to distinguish between a primary EBV infection complicated by steroid-resistant nephrotic syndrome (SRNS) or NS in which the first attack was complicated by a primary EBV infection with lymphoproliferative syndrome.
Proliferation was difficult to diagnose in some cases. A female patient (patient 5) receiving MMF presented with recurrent aseptic arthritis treated by antibiotics during 6 months before Hodgkin’s lymphoma was identified. Laboratory tests showed inflammatory syndrome, hypergammaglobulinemia, anemia, and a slight elevation of lactate dehydrogenase. Another female patient (patient 1) developed abdominal pain, vomiting, and elevation of transaminases 1 month after the sixth dose of rituximab to treat NS. She had also intermittent arthralgias of the shoulders. She had hypogammaglobulinemia related to rituximab. The blood count and the bone marrow aspiration were normal. Hepatic biopsy performed 2 years after the onset of symptoms found a dense oligoclonal lymphocyte T infiltration. One girl patient (patient 8) had occlusive syndrome and presented with abdominal mass, 6 years after the diagnosis of NS treated by several immunosuppressive therapies. She had ileo-ileal intussusception, and finally the biopsy of intestinal tissues found a smooth muscle tumor related to EBV. One boy (patient 7) had dysphagia, and he presented with a deterioration of general condition 1 year after onset of NS. A circumferential parietal thickening of the esophagus was observed with digestive endoscopy. Biopsies found a polymorphic and heterogeneous inflammatory infiltration in favor of benign T cell lymphoproliferative disease. One female patient (patient 4) had nonspecific gastrointestinal symptoms (diarrheas, abdominal pain) without biological inflammatory syndrome 2 years after NS diagnosis. Digestive endoscopy was considered normal. Digestive biopsies found a B cell polymorphic lymphoproliferative disorder associated with EBV. Kaposi’s sarcoma appeared in a male patient (patient 11) 6 years after the diagnosis of NS. He had been treated by cyclophosphamide, by ergamisol, and then by ciclosporin.
A Hodgkin’s lymphoma was found in a patient (patient 10) with discovery of a cervical mass 2 years after the diagnosis of NS. Finally, another patient (patient 9) presented with mediastinal mass and cough 1 year after NS onset and Hodgkin’s lymphoma was diagnosed.
Potentially oncogenic viruses were identified in 7 patients in the cohort (63%). EBV was implicated in the diagnosis of three lymphoproliferative syndromes, one digestive smooth muscle tumor (EBV-SMT), and one Hodgkin’s lymphoma. HHV8 was associated with the development of Kaposi’s sarcoma, but was also isolated in a child who developed Hodgkin’s lymphoma. Lymphoproliferative syndromes could be due to B cell proliferation (n = 2, 50%) or T cell proliferation (n = 2, 50%).
All the cases of Hodgkin’s lymphoma were treated with chemotherapy, sometimes in association with radiotherapy or autotransplantation. Among the patients with lymphoproliferative syndromes, one patient (female) was treated with an mTOR inhibitor (sirolimus), and the other three received rituximab infusions. The patient who presented with an EBV-SMT underwent complete surgical excision and received four rituximab infusions. Finally, the patient with Kaposi’s sarcoma was treated with sirolimus (patient 11). Immunosuppression was discontinued in 7 patients during the treatment, and the others did not receive immunosuppression at the time of proliferation.
At least three patients presented with relapses of NS after the diagnosis of proliferation. Two relapses were treated with rituximab and corticosteroids (patient 8 and patient 11); another one was treated with corticosteroids only (patient 2).
All patients remained in tumor remission after a median follow-up time of 2 years.
Despite atypical clinical histories, only four patients (36%) benefited from further immunological or genetic investigation. Results were only available for one girl, but none of the identified variants was considered involved in these diseases.
Discussion
We studied 11 patients who developed a proliferative syndrome after the diagnosis of NS. The time of onset was extremely variable, ranging from the concomitant diagnosis of NS and lymphoproliferative syndrome to the occurrence of proliferative syndrome 6 years after the diagnosis of NS. The majority had either nodular sclerosing Hodgkin’s lymphoma (n = 5) or benign lymphoproliferative syndrome (n = 4). The other two tumors detected were virus-related: one Kaposi’s sarcoma related to HHV8 (n = 1) and one smooth muscle tumor related to EBV (n = 1).
Ten patients in the cohort (91%) had SSNS. Seven of these patients went into remission with oral corticosteroids (63%), and 3 required methylprednisolone pulses (27%). Genetic analysis was not performed for the female patient with SRNS because of calcineurin inhibitor sensitivity.
The proliferative syndromes identified in this study were of lymphocytic origin for 82% of the cases (n = 9). For 3 patients, the diagnosis of NS and lymphoproliferative syndrome were almost simultaneous. This homogeneity supports the hypothesis of a common etiopathogenicity between these proliferative syndromes and the NS. However, two different pathologies are possible, a concomitant NS caused by the immune dysregulation of the lymphoproliferative disease (like Hodgkin’s lymphoma), and a lymphoproliferative disease following immunosuppression for the NS. Although the relationship between immune system disturbances and podocyte injury remains unclear, known mechanisms include inhibition of delayed-type hypersensitivity, abnormalities in isotype switching, and T cell polarization that results from abnormal transcriptional activation [8]. Genetic polymorphisms have been found in the HLA complex and in the CALHM6 gene of the calcium homeostasis modulator 6 family involved in the modulation of the immune response [8]. Finally, the reappearance of memory B cells after rituximab injection correlates with a high risk of relapse [9].
In addition, viruses were involved for 7 patients of the cohort (64%), EBV for 5 and HHV8 for 2. The involvement of oncogenic viruses such as EBV has also been described in idiopathic NS [1, 10].
Two tumors detected in this study are usually diagnosed in severely immunocompromised patients: Kaposi’s sarcoma, which develops particularly in patients with acquired immunodeficiency syndrome (AIDS), and EBV-SMT, an exceptional entity that occurs mainly in transplanted patients [11]. These diseases were diagnosed 6 years after the diagnosis of NS. In our study, the patient who developed Kaposi’s sarcoma had been treated with levamisole for 7 months, a course of cyclophosphamide, and ciclosporin for 6 years. The patient who developed EBV-SMT had been treated with MMF for 3 years and then with tacrolimus for 4 years. The extensive period of immunosuppressive therapy may have facilitated the development of these diseases, but no immune deficiency was biologically demonstrated in these 2 patients. A genetic study is underway for the child who had EBV-SMT. Only 29 children with EBV-SMT following solid organ transplantation have been described; 38% of them had a history of post-transplant lymphoproliferative disorder (PTLD) [11]. Reduction of immunosuppression, antiviral therapy, chemotherapy, surgical resection of the lesions, and sirolimus are the different treatment options currently available [11].
In our study, there was no evidence of an association between the immunosuppressive drugs received and the development of a proliferative syndrome. Three patients had received no maintenance therapy for NS when the proliferative syndrome was reported. The most common therapies used before the onset of the proliferative syndrome were mycophenolate mofetil (n = 4) or tacrolimus (n = 4). Mycophenolate mofetil and calcineurin inhibitors can rarely cause lymphoproliferations. The known side effects include entities called other iatrogenic immunodeficiency-associated lymphoproliferative disorders (OIIA-LPD) due to immunosuppression caused by these medications [12, 13]. Cyclophosphamide and rituximab were each given to only one patient in the cohort before the occurrence of a proliferative syndrome. When cyclophosphamide was used in routine practice, the tumors detected in patients with NS could be attributed to this treatment because of its cytotoxic nature. At present, cyclophosphamide is no longer used as first-line therapy [14]. Neutropenia and hypogammaglobulinemia are known late-onset adverse events related to rituximab use, especially in young children [15]. In the literature, lymphoproliferative syndrome has not been described in patients who received rituximab therapy.
Thirty-six percent (36%) of the patients in the cohort had in-depth genetic (n = 3) or immunological (n = 1) studies. We only had the results for two female patients. In the first patient (patient 1), few variants were found in whole exome sequencing: NFAT-5 variant, RRAS2 variant, and two DOCK4 variants. None of them was clearly involved in medical history. NFAT-5 (Nuclear factor of activated T cell 5) is a gene involved in the immune system, which encodes a DNA binding protein activated in response to osmotic stress, also known as tonicity-responsive enhancer binding protein (TonEBP). In T cells, NFAT-5 exists constitutionally and the transcriptional regulatory activity can be induced independently by T cell receptor stimulation or by hyperosmotic stress. T cells with reduced NFAT5 function exhibit impaired proliferation and survival [16]. It is important to note that lymphocytes are exposed to physiological hyperosmotic stress [17]. However, NFAT5 deficiency has never been previously described as being associated with human disease [18], and in this case, we cannot retain it as being responsible for the lymphoproliferation. The NFAT-5 variant is a variant of uncertain significance (VUS). The RRAS2 variant was inherited from her father and had never been described before. Each variant of DOCK4 was inherited by each parent, but the function of DOCK4 in immune system is not known. For one patient (patient 6), a NLRP1 variant was found in HLH-EBV (EBV-associated hemophagocytic lymphohistiocytosis) genetic panel. Human NLRP1 was the first protein shown to form an inflammasome, but its physiological mechanism of activation remains unknown [19]. This NRLP1 variant is of uncertain significance (VUS). The results of genetic investigation for patient 8 are not available. Finally, rare immunodeficiency has been looked for in patient 4, but none has been found.
The contribution of genetics could be essential to identifying patients who are more likely to develop a proliferative syndrome after being diagnosed with NS.
The clinical signs were variable and barely specific (gastrointestinal symptoms, adenopathy, pneumopathy, intussusception, etc.), and an impaired general health status was not always predominant. It was also sometimes difficult to make a diagnosis. Special vigilance may be required in the event of unusual persistence of common symptoms in children with NS. In such cases, searching for adenopathies may help guide diagnosis towards a benign or malignant lymphoproliferative syndrome. From an epidemiological perspective, we speculate that lymphoproliferation could occur much more frequently in children with NS than in the general pediatric population. For Hodgkin’s lymphoma, the incidence has been estimated at 7 per million children per year compared to 3 per 1000 children with NS in our study [20]. Therefore, the incidence of Hodgkin’s lymphoma might be around 400 times higher in patients with NS than in the general pediatric population. For all cancers, the incidence has been estimated to be about 150 per million children per year in France compared to 5 per 1000 children with NS in our study. The incidence rate of all cancer might thus be around 30 times higher in children with NS than in the general pediatric population.
Our cohort was retrospective and consisted of only 11 patients. Furthermore, we observed common features without being able to prove a causal link between the NS and the proliferative syndrome. There was a potential recall bias in our study since it was not exhaustive. It relied on the memory and goodwill of pediatricians from the French Pediatric Nephrology Society.
Conclusion
We report 11 patients with NS most of whom were steroid-sensitive and who simultaneously or subsequently developed a proliferative syndrome, mostly of lymphocytic origin. The data did not allow us to investigate the role of the immunosuppressive treatments received. We suggest regular monitoring of EBV/HHV8 PCR in children with NS and reduction of immunosuppression in case of high viral load. We assume that these proliferative syndromes, which are mainly lymphocytic, have the same etiopathogenesis as the NS, which could be related to a lymphocytic disturbance in the immune system.
Abbreviations
- AIDS:
-
Acquired immunodeficiency syndrome
- DNA:
-
Deoxyribonucleic acid
- EBV:
-
Epstein-Barr virus
- EBV-SMT:
-
Epstein-Barr virus-associated smooth muscle tumors
- HLA:
-
Human leukocyte antigen
- HHV-8:
-
Human herpesvirus-8
- MCD:
-
Minimal change disease
- MMF:
-
Mycophenolate mofetil
- NFAT-5:
-
Nuclear factor of activated T cell 5
- NS:
-
Nephrotic syndrome
- OIIA-LPDs:
-
Other iatrogenic immunodeficiency-associated lymphoproliferative disorder
- PTLD:
-
Post-transplant lymphoproliferative disorder
- TonEBP:
-
Tonicity-responsive enhancer binding protein
- VUS:
-
Variant of uncertain significance
References
Dossier C, Jamin A, Deschênes G (2017) Idiopathic nephrotic syndrome: the EBV hypothesis. Pediatr Res 81:233–239
Kyrieleis HA, Löwik MM, Pronk I, Cruysberg HR, Kremer JA, Oyen WJ, van den Heuvel BL, Wetzels JF, Levtchenko EN (2009) Long-term outcome of biopsy-proven, frequently relapsing minimal-change nephrotic syndrome in children. Clin J Am Soc Nephrol 4:1593–1600
Rüth EM, Kemper MJ, Leumann EP, Laube GF, Neuhaus TJ (2005) Children with steroid-sensitive nephrotic syndrome come of age: long-term outcome. J Pediatr 147:202–207
Farruggia P, Trizzino A, Maringhini S, Grigoli A, Sapia C, D’Alessandro M, Tropia S, D’Angelo P (2010) Hodgkin lymphoma and nephrotic syndrome in childhood. Indian J Pediatr 77:1147–1149
Stéphan JL, Deschênes G, Pérel Y, Bader-Meunier B, Brunat-Mentigny M, Lejars O, Lamagnères JP (1997) Nephrotic syndrome and Hodgkin disease in children: a report of five cases. Eur J Pediatr 156:239–242
Audard V, Larousserie F, Grimbert P, Abtahi M, Sotto JJ, Delmer A, Boue F, Nochy D, Brousse N, Delarue R, Remy P, Ronco P, Sahali D, Lang P, Hermine O (2006) Minimal change nephrotic syndrome and classical Hodgkin’s lymphoma: report of 21 cases and review of the literature. Kidney Int 69:2251–2260
« pnds_-_syndrome_nephrotique_idiopatique_de_lenfant_2016–04–29_15–02–42_382.pdf » (2016) https://www.has-sante.fr/upload/docs/application/pdf/2016-04/pnds_-_syndrome_nephrotique_idiopatique_de_lenfant_2016-04-29_15-02-42_382.pdf
Noone DG, Iijima K, Parekh R (2018) Idiopathic nephrotic syndrome in children. Lancet 392:61–748
Dufek S, Cheshire C, Levine AP, Trompeter RS, Issler N, Stubbs M, Mozere M, Gupta S, Klootwijk E, Patel V, Hothi D, Waters A, Webb H, Tullus K, Jenkins L, Godinho L, Levtchenko E, Wetzels J, Knoers N, Teeninga N, Nauta J, Shalaby M, Eldesoky S, Kari JA, Thalgahagoda S, Ranawaka R, Abeyagunawardena A, Adeyemo A, Kristiansen M, Gbadegesin R, Webb NJ, Gale DP, Stanescu HC, Kleta R, Bockenhauer D (2019) Genetic identification of two novel loci associated with steroid-sensitive nephrotic syndrome. J Am Soc Nephrol 30:1375–1384
Sato M, Kamei K, Ogura M, Ishikura K, Ito S (2018) Relapse of nephrotic syndrome during post-rituximab peripheral blood B-lymphocyte depletion. Clin Exp Nephrol 22:110–116
Dossier C, Sellier-Leclerc AL, Rousseau A, Michel Y, Gautheret-Dejean A, Englender M, Madhi F, Charbit M, Ulinski T, Simon T, Jacqz-Aigrain E, Deschênes G (2014) Prevalence of herpesviruses at onset of idiopathic nephrotic syndrome. Pediatr Nephrol 29:2325–2331
Jossen J, Chu J, Hotchkiss H, Wistinghausen B, Iyer K, Magid M, Kamath A, Roayaie S, Arnon R (2015) Epstein-Barr virus-associated smooth muscle tumors in children following solid organ transplantation: a review. Pediatr Transplant 19:235–243
Taliaferro A, Samhouri Y, Rice J, Khan CM, Cillo JE (2021) Rare oral presentation of a mycophenolate mofetil-related other iatrogenic immunodeficiency-associated lymphoproliferative disorder (MMF-OIA-LPD) lesion: a case report and literature review. J Oral Maxillofac Surg 79:398–403
Crane GM, Powell H, Kostadinov R, Rocafort PT, Rifkin DE, Burger PC, Ambinder RF, Swinnen LJ, Borowitz MJ, Duffield AS (2015) Primary CNS lymphoproliferative disease, mycophenolate and calcineurin inhibitor usage. Oncotarget 6:33849–33866
Fujinaga S, Ozawa K, Sakuraya K, Yamada A, Shimizu T (2016) Late-onset adverse events after a single dose of rituximab in children with complicated steroid-dependent nephrotic syndrome. Clin Nephrol 85:340–345
Boland BS, Widjaja CE, Banno A, Zhang B, Kim SH, Stoven S, Peterson MR, Jones MC, Su HI, Crowe SE, Bui JD, Ho SB, Okugawa Y, Goel A, Marietta EV, Khosroheidari M, Jepsen K, Aramburu J, López-Rodríguez C, Sandborn WJ, Murray JA, Harismendy O, Chang JT (2015) Immunodeficiency and autoimmune enterocolopathy linked to NFAT5 haploinsufficiency. J Immunol 194:2551–2560
Go WY, Liu X, Roti MA, Liu F, Ho SN (2004) NFAT5/TonEBP mutant mice define osmotic stress as a critical feature of the lymphoid microenvironment. Proc Natl Acad Sci U S A 101:10673–10678
Lee N, Kim D, Kim WU (2019) Role of NFAT5 in the immune system and pathogenesis of autoimmune diseases. Front Immunol 10:270
Chavarría-Smith J, Mitchell P, Ho A, Daugherty M, Vance R (2016) Functional and evolutionary analyses identify proteolysis as a general mechanism for NLRP1 inflammasome activation. PLoS Pathogens 12:e1006052
Institute of Medicine (US) and National Research Council (US) National Cancer Policy Board. Childhood cancer survivorship: improving care and quality of life. Hewitt M, Weiner SL, Simone JV, editors (2003) Washington (DC): National Academies Press (US)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Graphical abstract
(PPTX 48.7 kb)
Rights and permissions
About this article

Cite this article
Cébron, C., Godron-Dubrasquet, A., Aladjidi, N. et al. Benign and malignant proliferation in idiopathic nephrotic syndrome: a French cohort study. Pediatr Nephrol 37, 1837–1843 (2022). https://doi.org/10.1007/s00467-021-05386-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-021-05386-0