
Abstract
Rituximab has emerged as an effective and important therapy in children with complicated frequently relapsing and steroid-dependent nephrotic syndrome to induce long-term disease remission and avoid steroid toxicities. The optimal rituximab regimen is not totally well defined, and there are many varying practices worldwide. We will in this review describe how patient factors, rituximab dose, and use of maintenance immunosuppression affect treatment outcomes. Specifically, low-dose rituximab without concomitant immunosuppression is associated with shorter relapse-free duration while other regimens have comparable outcomes. Patients with more severe disease generally have worse response to rituximab. Although rituximab appears to be generally safe, there are growing concerns of chronic hypogammaglobulinemia and impaired immunity especially in young children. Reliable prognostications and biomarkers for guiding subsequent treatments to avoid excessive treatments are yet to be identified. In this review, we will outline the, as we see it, best approach of rituximab in childhood steroid sensitive nephrotic syndrome at the present state of knowledge.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Idiopathic nephrotic syndrome (NS) is an uncommon childhood disease characterized by nephrotic-range proteinuria, edema, and hypoalbuminemia. The reported incidence of NS depends on ethnicity or country of origin and has considerable variation, ranging from 1.15 to 16.9 per 100,000 persons [1]. Although the majority of these children respond to steroid therapy, 50% patients develop frequent relapses (FR) and/ or steroid dependency (SD) [2]. A range of immunosuppressants including levamisole, cyclophosphamide, calcineurin inhibitor (CNI), and mycophenolate mofetil (MMF) are often used to minimize the steroid burden for children with FRSDNS. However, overall 20–30% children with NS continue to relapse despite multiple immunosuppressive therapies and are classified as complicated FRSDNS [3]. These children are often multi-drug dependent and are at high risk of developing significant toxicities from steroids and other immunosuppressive agents, such as short stature, cosmetic changes, Cushing syndrome, infection, and nephrotoxicity.
Rituximab, a chimeric anti-CD20 monoclonal antibody, was originally used to treat B-cell non-Hodgkin’s lymphoma at a dose of 375 mg/m2 for four infusions. It did then become used in different autoimmune diseases like systemic lupus erythematosus, and in those cases rituximab was mostly prescribed in the dose of 750 mg/m2 for two infusions. Rituximab was first described to induce remission of SDNS in a 16-year-old boy who was treated for autoimmune thrombocytopenic purpura [4]. Since then, three randomized control trials have confirmed the efficacy of rituximab in complicated FRSDNS [5,6,7]. Recently, rituximab is also found to be effective in children as first-line steroid-sparing agent [8]. Rituximab does in most cases lead to a sustained relapse-free period with reduction or even discontinuation of immunosuppression, especially corticosteroids.
Nonetheless, there are substantial variations in rituximab prescription worldwide, ranging from 375 to 1500 mg/m2 per treatment course [9, 10]. Use of maintenance immunosuppression to extend disease remission is also a practice that is used by some centers [11,12,13,14,15]. Importantly, most patients (80%) eventually relapse, showing that the drug effect is not permanent [16]. Repeated treatments are often required. The rituximab-related safety profile is hence of crucial consideration when clinicians decide on repeating therapies.
In this review, we will focus on children with steroid-sensitive nephrotic syndrome, notably complicated FRSDNS. We will discuss the evidence related to dosing regimen and adverse events of rituximab, in order to suggest the optimal regimen and the re-treatment approach.
Factors determining treatment response
The treatment outcomes following rituximab are determined by patient factors, rituximab dose, and the use of maintenance immunosuppression and are summarized in Fig. 1.

Factors affecting treatment outcomes of rituximab therapy. Patient factors, rituximab dose, and concomitant immunosuppression interact with each other and impact on treatment outcomes. FRSDNS, frequently relapsing and/or steroid-dependent nephrotic syndrome; IS, immunosuppression; MMF, mycophenolate mofetil; SRNS, steroid resistant nephrotic syndrome
Patient factors
The clinical course in children with complicated FRSDNS is quite heterogeneous. Multiple patient factors account for a diverse response to rituximab. Notably, patients with a more severe disease are associated with worse response to rituximab. Iijima et al. reported a lower 1-year relapse-free survival in children with complicated FRSDNS [5], compared to those reported by Basu et al. who received rituximab as first-line agent for an uncomplicated disease (37% vs. 90%) [8]. Children with a history of initial steroid resistance are often multi-drug dependent and at risk of more relapses and shorter remission after rituximab [11, 14]. Number of relapses often become fewer and less difficult-to-control with age towards adolescence. Younger age at rituximab initiation was associated with earlier B cell reconstitution and potentially increased relapse risk [17, 18], although an earlier report did not support this observation [15]. Several authors have not been able to identify underlying histology as a significant predictive factor of treatment response [7, 11, 14]. There is great variability in outcomes in different studies suggesting varying steroid responsiveness by ethnicity and country of origin. It ranges from 69% in Pakistani to 98% in South Asians residing in Canada [1]. However, an ethnic effect on the response to rituximab would need to be confirmed in a larger scale, multi-ethnic study.
Rituximab dose
The rituximab dose used for childhood NS was initially adopted from two previously used schedules. Some pediatric nephrologists adopted the original prescription for treatment of lymphoma: four infusions of 375 mg/m2 at 1-week interval. Others used the schedule often applied in autoimmune diseases such as lupus: two doses of 750 mg/m2, 2 weeks apart. Both regimens consist of a total dose of 1500 mg/m2. In recent years, a lower rituximab dose has been advocated with a potential benefit of limiting cost and side effects [6, 19]. Only a few studies have to-date compared the efficacy of various rituximab regimens. Most of these reports were limited by their retrospective nature, a small patient number, and failure to separate the dose effect from the use of concomitant immunosuppression.
Subgroup analyses from earlier retrospective observational studies suggested that patients receiving high-dose rituximab (1125–1500 mg/m2) had a longer remission period [15, 20]. Kemper et al. found the time to first relapse was 10.3 ± 3.5 months and 23.3 ± 18.7 months in children receiving rituximab at 375–750 mg/m2 and 1125–1500 mg/m2, respectively (p < 0.05) [15]. Previous work by Webb et al. also found a shorter median time to relapse in patients receiving one infusion of 750 mg/m2 compared to two infusions (5 vs. 16 months; p = 0.03) [20].
Hogan et al. retrospectively examined the effect of rituximab at dosing levels of 100 mg/m2, 375 mg/m2, and 750 mg/m2 in 61 children with SDNS, with 1-year relapse-free survival rates being 50, 59, and 72%, respectively [18]. The risks of B cell reconstitution and relapse were significantly increased only in the very low-dose group of 100 mg/m2. Data on concurrent immunosuppression was limited in that study.
Maxted et al. evaluated 60 UK children with FRSDNS in a multicenter retrospective cohort study [21]. The author found no statistical difference in the event-free survival at 12 months between different rituximab regimens (375–1500 mg/m2), and suggested that low-dose rituximab at 375 mg/m2 was no less effective than higher dosing ranges. However, the dose distribution was grossly uneven within the cohort and only five out of 60 patients received rituximab at an intermediate dose (750–1000 mg/m2).
Maintenance immunosuppression
Concomitant immunosuppression has been proposed to extend remission without prolonging B cell depletion [11, 12]. This approach may be particularly valuable when using low-dose rituximab and in children who run a complicated clinical course [12, 14, 22]. Sinha et al. described higher rates of sustained remission with pre-emptive mycophenolate mofetil (MMF) if the patients were CNI-dependent, but not in those with uncomplicated SDNS [14]. Basu et al. also concluded that a higher proportion of children with refractory SRNS sustained remission with post-rituximab MMF therapy [22]. Although MMF appears to be a promising option [13], its effect is not confirmed in some reports and thus the drug of choice remains controversial [11, 17]. CNI may be more effective than MMF in maintaining remission [23], but it is associated with nephrotoxicity after protracted use. A multicenter prospective randomized controlled trial is being conducted in Japan to examine the role of MMF as maintenance therapy following rituximab [24]. Currently, a randomized controlled trial from India, the RITURNS II study, is underway to determine the efficacy of maintenance MMF versus repeating rituximab after initial course among children with SDNS (RITURNS II, Clinical Trials Registry Identifier: NCT03899103).
An international, multicenter study on rituximab regimen
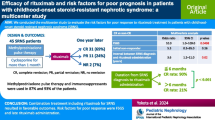
Recently, we conducted an international, multicenter, retrospective cohort study where 511 multi-ethnic children with complicated FRSDNS were recruited from 11 tertiary pediatric nephrology centers in Asia, Europe, and North America [16]. All patients were steroid-sensitive and in remission at first rituximab treatment, with a mean follow-up duration of 4.3 years. Six combinations of rituximab regimens were compared: low dose (375 mg/m2), medium dose (750 mg/m2), and high dose (1125–1500 mg/m2) per course, with or without maintenance immunosuppression (defined as corticosteroid, MMF, and/or CNI for more than 6 months).
Following rituximab, 80% children relapsed with a median relapse-free period of 12.5 months. Both rituximab dose and use of maintenance immunosuppression showed significant interaction on treatment outcomes. Specifically, the relapse-free survival was not different in five of the six treatment groups (10.9–14 months), while children who received the lowest dose rituximab (375 mg/m2) without concomitant immunosuppressive therapy had a shorter relapse-free survival of 8.5 months. Results of the Kaplan-Meier analysis of various regimens are presented in Fig. 2. Our unpublished data also showed that dosing schedule per se did not affect treatment efficacy. For instance, children receiving a total dose of 750 mg/m2, either by a single infusion or 375 mg/m2 for two infusions, had similar outcomes.

Relapse-free survival following different rituximab regimens. (Reprinted from Chan et al. [16], with permission from Elsevier). Kaplan-Meier curves for the relapse-free survival following the first course of rituximab therapy at different dosing levels (low, 375 mg/m2; medium, 750 mg/m2; high, 1125–1500 mg/m2) and stratified by the use of maintenance immunosuppression (mIS)
In line with aforementioned patient factors, each 1-year younger in age at first rituximab and one additional number of prior immunosuppression increased relapse risk by 5% and 19%, respectively. Ethnicity did not appear to affect treatment response in this well-defined patient population with comparable disease severity. Renal histology was not analyzed in the multivariate analysis, because up to 40% children in the cohort did not receive a kidney biopsy. Important data pertaining to B cell population and adverse events were inadequate due to different monitoring protocol and reporting bias.
Safety and long-term consequence
It is crucial to understand the safety of rituximab and its long-term consequences in order to decide on the optimal treatment approach. Whether adverse events are dose- or time-dependent is still poorly studied and remains inconclusive. Existing data however do not suggest that higher rituximab dose or increasing treatment courses lead to more side effects, but these have to be interpreted carefully [16, 25, 26].
Overall, rituximab appears to be safe in children [5, 7,8,9, 15, 20, 25, 27, 28]. Infusion reactions are the most prevalent adverse events. They are often self-limiting with pre-medications and reduction of speed of the infusion [16, 28]. Serious complications do, however, occur occasionally, including rituximab-associated lung injury, fatal hepatitis reactivation, and multifocal leukoencephalopathy [29,30,31,32]. There are reports of severe infections such as fulminant viral myocarditis and atypical Pneumocystis jiroveci pneumonia [33, 34]. Although there is currently no consensus regarding Pneumocystis jiroveci prophylaxis in children with nephrotic syndrome, co-trimoxazole is still recommended by some pediatric nephrologists for 6 months following rituximab. Of note, Kamei et al. found agranulocytosis (absolute neutrophil count of < 500mm3) in 9.6% patients at a median of 66 days after rituximab, and it was more prevalent in young children [35]. These children often developed febrile illness and required interventions such as antibiotics and granulocyte colony-stimulating factor [35]. There are to our knowledge no data on an increased chance for malignancies, if any, in this patient population [36,37,38].
Two important long-term sequelae after rituximab therapy warrant attention: its impact on a developing immunological system and persistent hypogammaglobulinemia. Colucci et al. examined the lymphocyte populations and vaccine competency in 27 children with FRSDNS who were followed for more than 4 years after the first and at least 2 years after the last anti-CD20 infusion [39]. Total memory and switched memory B cells were persistently and significantly reduced in about 75% patients at last follow-up compared to baseline. The clinical significance of this is unknown. Antibodies against HBV and tetanus were reduced, indicating impaired vaccine competence. Eleven patients developed persistent hypogammaglobulinemia at last follow-up, and in four children, the IgG levels were extremely low (less than 160 mg/dL).
Parmentier et al. also described that 25 out of 86 children developed hypogammaglobulinemia, and in 13 patients the low immunoglobulin level persisted beyond 1 year after B cell recovery [26]. The development of this complication was not related to cumulative rituximab dose. About a third of patients had concomitant infection, and one patient was complicated by enterovirus-associated fulminant myocarditis leading to heart transplantation [26, 33]. All these infected children were supplemented by intravenous immunoglobulin (IVIG) infusions. Of note, in both reports, younger age at time of first anti-CD20 treatments was identified to be a significant risk factor for hypogammaglobulinemia (OR 2.14/year, p = 0.006) [26, 39]. This highlights the importance of monitoring immunoglobulin levels and perhaps also vaccine antibody titres. Published guideline does not recommend an absolute level of IgG where immunoglobulin replacement therapy should be commenced [40]. The decision to substitute hypogammaglobulinemia should be based on degree of hypogammaglobulinemia, nature of the infections (serious, persistent, unusual, or recurrent), vaccine competency, and response to antibiotic prophylaxis [40]. Further work is required to clarify the management in asymptomatic, numerical hypogammaglobulinemia.
Although rituximab appears to be safe in a majority of treated children, it is important to note that most data on safety come from older children. More data are needed in young patients as this patient population is more likely to require multiple rituximab treatments, and they might also have a higher chance of neutropenia and hypogammaglobulinemia.
Approach to maintaining remission and subsequent treatments
A significant proportion of patients with FRSDNS relapse 1 year after rituximab [16, 41]. Some of these children may develop frequent relapses or steroid dependence again, and if so require re-initiation of intensive immunosuppression and additional rituximab [41]. Several policies in redoing rituximab have been described to maintain long-term remission.
The most common is re-treatment after a relapse. This is the indication for repeating rituximab in up to 87% of children with complicated FRSDNS [16]. As discussed, maintenance immunosuppression may be a useful option to extend remission, especially with low-dose rituximab [16]. In a follow-up work of the RITURNS study which studied children without previous immunosuppression for their FRSDNS, preliminary results showed that all children relapsed within 6 to 24 months following initial course of rituximab as first-line therapy [42]. Patients receiving MMF as co-therapy after second course of rituximab had a longer remission than those who received rituximab alone (80% relapse-free survival, 84 vs. 30 weeks), and 75% patients remained relapse-free at 2 years. In France, a randomized controlled trial is currently underway to examine whether a novel approach of adding monthly IVIG for 5 months to low-dose rituximab can improve remission rates in SDNS (RITUXIVIG, Clinical Trials Registry Identifier: NCT03560011).
The second way to do it is to monitor the B cell response and to repeat rituximab when they repopulate. The third way is scheduled therapy to induce persistent B cell depletion. Despite growing evidence on various re-dosing strategies, the optimal approach remains controversial and requires a careful consideration between long-term efficacy and safety profile.
Retreatment after B cell reconstitution
Several reports showed that relapses occurred after B cell reconstitution [8, 17, 18, 43]. For this reason, B cell population is the most frequently monitored biomarker, and its recovery is an indication for re-treatment in some protocols [16, 43, 44]. In one study involving 18 children with SDNS, Kim et al. repeated rituximab according to B cell reconstitution in 70% of all treatment cycles. Each patient received an average of 5.2 ± 2.3 rituximab courses over a relatively short period of 2.8 ± 1.1 years. Eight patients had sustained remission, and in 10 patients, relapse rates reduced from 2.8 ± 1.5 to 1.3 ± 0.8 relapses per year.
Delbet et al. compared B cell depletion duration of individual patients between initial and subsequent rituximab treatments in 22 children with NS [45]. About 90% patients had a similar B cell depletion duration during subsequent treatments. Individualized monitoring and even pre-emptive rituximab administration are therefore feasible, once the time to B cell repletion is determined for each patient.
Nonetheless, discrepancies concerning the temporal relationship between relapse and B cell population were frequently observed in the literatures. For example, following B cells recovery at a median of 160 days post-rituximab, Kamei et al. found that only 73% of the 81 children with SDNS relapsed at a median of 309 days [11]. On the other hand, Sato et al. described six out of 82 patients (7.2%) relapsed even in the presence of B cell depletion after rituximab [46]. These patients had poor response to rituximab and developed repeated relapses during B cell depletion despite multiple treatment courses and concomitant immunosuppression [46]. The above findings indicate B cell reconstitution is not a reliable biomarker, and the timing of relapse can be considerably variable and much delayed. A complex interplay between immunity, circulating factors, and podocyte probably accounts for this phenomenon [47].
Not all B cell subsets are equally relevant in the pathogenesis of steroid-sensitive nephrotic syndrome [48]. Colucci et al. conducted an interesting study on B cell subpopulations following rituximab in 28 children with FRSDNS [49]. While total B cells reconstituted at a median of 6 months, there was a sequential re-emergence of transitional, mature, and finally memory B cells. Of note, only 4 patients (15%) relapsed at 9 months even when all B cell subsets recovered in most patients, and only 14 children (50%) eventually relapsed at 24 months. The correlation between relapse and B cell population is thus not substantial. Of all subsets, only reconstitution of switched memory B cell (> 0.067% of total lymphocytes), a subcategory of memory B cells producing IgG, IgA, or IgE antibodies, was predictive of a relapse upon multivariate analysis. Until evaluation of this particular subpopulation becomes widely available, the utility of routine B cell monitoring in guiding re-treatment may be limited.
Repeating rituximab based on B cell reconstitution may lead to sustained remission and avoid steroid use related to relapses. However, a significant proportion of patients may be subjected to excessive or unnecessarily early treatments with long-term safety concerns. Further investigations are required to delineate the relationship between B cell population and relapse before such approach can be regularly adopted.
Retreatment as scheduled therapy
A third approach is a scheduled therapy, where rituximab is repeated periodically at a regular interval, irrespective of B cell and clinical status. The rationale of this strategy is to induce persistent B cell depletion and consequently disease remission. Kimata et al. repeated rituximab (375 mg/m2 each) four times at 3-monthly intervals in five children with SDNS, and induced long-term remission without serious adverse events [50]. Takahashi et al. reported that repeating rituximab at 6-month intervals for 2 years effectively reduced relapse rates and achieved long-term remission in half of the recruited patients with complicated FRSDNS [51]. Nonetheless, significant side effects were observed in a high proportion of children [51], suggesting such frequent rituximab administrations might be excessive for adequate disease control. The effect of persistent B cell depletion in a developing immunological system is unknown and deserves attention.
Practical approach and the way forward
Optimal therapy of FRSDNS should effectively induce long-term remission with minimal toxicity related to steroids, rituximab, and other immunosuppression. Cost is also an important consideration as rituximab is not readily affordable in many countries (2000 Euros per 500 mg rituximab).
Our preferred practice at this present time is to use rituximab in children with complicated FRSDNS after all other treatment options have been tried. This means that the child should typically have tried most treatments including every other day low-dose steroids, levamisole, cyclophosphamide, CNI, and MMF before being eligible for rituximab. Using rituximab as first-line steroid-sparing agent, not surprisingly, has been associated with encouraging results. However, until long-term safety of this approach is established, we do have concern to recommend a liberal use due to potential severe complications.
In our setting where treatment is subsidized, we now prescribe rituximab at a single infusion of 750 mg/m2 (maximum 1000 mg) without maintenance therapy to attain similar efficacy and avoid protracted immunosuppression use. Since about 10% patients may develop an early relapse within first month post-rituximab [5], we taper and discontinue the immunosuppressants gradually over 1 to 2 months following rituximab. In our experience, most of these children achieve long-term remission subsequently once rituximab comes into full effect.
Alternatively, low-dose rituximab (375 mg/m2) with co-medication such as MMF is an attractive approach to prolong remission, reduce cost, and limit potential rituximab adverse events, particularly in resource-limited settings. A single low-dose infusion alone is probably undesirable due to suboptimal efficacy and is at risk of developing anti-rituximab antibodies with recurrent drug exposures [52]. It is noteworthy that in adult protocols and some prospective pediatric trials [5, 8, 19], each 375 mg/m2 dose is limited to a maximum of 500 mg. While this limit should be applied to higher dosing ranges, it may be advisable to adequately dose young people receiving a low-dose regimen (600–700 mg in absolute dose according to their body surface area) to avoid under-dosing and consequently a shorter B cell depletion.
We recommend prescribing rituximab cautiously in the youngest children, given the concerns of drug safety among them. We also do not recommend redosing rituximab based on B cell reconstitution or as a regular schedule, except in a very limited group of children who have a clinical history of very severe relapses needing hospitalization with massive edema and/or acute kidney injury. Many children, after receiving a few courses of rituximab, can be successfully managed with other immunosuppressive agents, and never or only at a much later time require further rituximab treatment. If regular therapy is used, then it should be withheld every 2 to 3 treatment cycles since some patients do naturally run into long-term disease remission.
There are still many remaining questions regarding the optimal rituximab regimen in steroid-sensitive nephrotic syndrome. It is important to be aware that the above recommendations are based on limited data, predominantly from children with complicated FRSDNS. For less severe patients receiving rituximab as a first-line agent, the effects of dose and maintenance immunosuppression are likely different and an alternative approach may be necessary. Treatment regimens should thus be individualized and should balance the disease severity, treatment efficacy, drug safety, tolerance to co-medication, adherence, cost, and family as well as physician preference. In the future, new and reliable biomarkers, such as switched memory B cells, anti-rituximab antibodies, and T lymphocyte activation markers, may help to predict relapse and guide prophylactic treatments [53].
Uncertainties and outstanding research questions
Large scale prospective investigations are required to answer outstanding research questions and can be grouped into a few directions:
-
1.
Prognostication of patients’ response to rituximab.
-
2.
To establish the effective dosing regimen when rituximab is used in children with uncomplicated FRSDNS.
-
3.
To identify the choice and optimal duration of maintenance immunosuppression to adjunct the rituximab effect.
-
4.
To evaluate the long-term efficacy and safety profile for repeated rituximab therapies, especially in young children. This may provide important data to guide subsequent treatments, understand the development of drug resistance, and justify repeated rituximab use.
-
5.
To investigate the implication and formulate the appropriate management of persistent hypogammaglobulinemia.
-
6.
To identify and validate reliable biomarkers to predict relapse and guide timely re-treatment.
Conclusion
Rituximab is an effective and important therapy in children with FRSDNS. New insights suggest patient factors, rituximab dose, and use of concomitant immunosuppression all impact on treatment outcomes. Whereas rituximab appears to be generally safe, cautions and regular monitoring are of particular importance in young children to look for adverse events including neutropenia, persistent hypogammaglobulinemia, and impaired vaccine competence. Treatment protocols should therefore be individualized. International, multi-ethnic, prospective studies are much needed to answer outstanding research questions and identify the optimal strategy for rituximab in this patient population.
Questions
-
1.
What factors determine the treatment response to rituximab?
-
A.
Patient factors, such as disease severity
-
B.
Rituximab dose
-
C.
Maintenance immunosuppression
-
D.
All of the above
-
A.
-
2.
Which of the following regimens has shortest relapse-free survival?
-
A.
Low dose (375 mg/m2) alone
-
B.
Medium dose (750 mg/m2) alone
-
C.
Low dose (375 mg/m2) with maintenance therapy
-
D.
High dose (750 mg/m2) with maintenance therapy
-
A.
-
3.
Which of the following B cell subsets is more relevant to relapse after rituximab?
-
A.
Transitional B cells
-
B.
Mature B cells
-
C.
IgM Memory B cells
-
D.
Switched Memory B cells
-
A.
-
4.
How many patients develop persistent hypogammaglobulinemia following rituximab?
-
A.
Less than 5%
-
B.
5% to 10%
-
C.
10% to 15%
-
D.
More than 15%
-
A.
Keypoints
-
Patient factors, rituximab dose, and use of maintenance immunosuppression all influence treatment outcomes
-
Low-dose rituximab alone is associated with shortest relapse-free survival and higher relapse risk
-
Concomitant immunosuppression, notably MMF, may be useful to extend remission especially with low-dose rituximab
-
Role of B cell monitoring may be limited due to discrepancy between B cell population and relapse after rituximab
-
There are growing concerns of persistent hypogammaglobulinemia and impaired immunity particularly in young children
Answer: 1. D; 2. A; 3. D; 4. D
References
Chanchlani R, Parekh RS (2016) Ethnic differences in childhood nephrotic syndrome. Front Pediatr 4:39
Webb N, Woolley R, Lambe T, Frew E, Brettell E, Barsoum E, Trompeter R, Cummins C, Deeks J, Wheatley K (2019) Long term tapering versus standard prednisolone treatment for first episode of childhood nephrotic syndrome: phase III randomised controlled trial and economic evaluation. Bmj 365:I1800
Iijima K, Sako M, Nozu K (2017) Rituximab for nephrotic syndrome in children. Clin Exp Nephrol 21(2):193–202
Benz K, Dötsch J, Rascher W, Stachel D (2004) Change of the course of steroid-dependent nephrotic syndrome after rituximab therapy. Pediatr Nephrol 19(7):794–797
Iijima K, Sako M, Nozu K, Mori R, Tuchida N, Kamei K, Miura K, Aya K, Nakanishi K, Ohtomo Y (2014) Rituximab for childhood-onset, complicated, frequently relapsing nephrotic syndrome or steroid-dependent nephrotic syndrome: a multicentre, double-blind, randomised, placebo-controlled trial. The Lancet 384(9950):1273–1281
Ravani P, Rossi R, Bonanni A, Quinn RR, Sica F, Bodria M, Pasini A, Montini G, Edefonti A, Belingheri M (2015) Rituximab in children with steroid-dependent nephrotic syndrome: a multicenter, open-label, noninferiority, randomized controlled trial. J Am Soc Nephrol 26(9):2259–2266
Ruggenenti P, Ruggiero B, Cravedi P, Vivarelli M, Massella L, Marasà M, Chianca A, Rubis N, Ene-Iordache B, Rudnicki M (2014) Rituximab in steroid-dependent or frequently relapsing idiopathic nephrotic syndrome. J Am Soc Nephrol 25(4):850–863
Basu B, Sander A, Roy B, Preussler S, Barua S, Mahapatra T, Schaefer F (2018) Efficacy of rituximab vs. tacrolimus in pediatric corticosteroid-dependent nephrotic syndrome: a randomized clinical trial. JAMA Pediatr 172(8):757–764
Prytuła A, Iijima K, Kamei K, Geary D, Gottlich E, Majeed A, Taylor M, Marks SD, Tuchman S, Camilla R (2010) Rituximab in refractory nephrotic syndrome. Pediatr Nephrol 25(3):461–468
Deschênes G, Vivarelli M, Peruzzi L (2017) Variability of diagnostic criteria and treatment of idiopathic nephrotic syndrome across European countries. Eur J Pediatr 176(5):647–654
Kamei K, Ogura M, Sato M, Sako M, Iijima K, Ito S (2016) Risk factors for relapse and long-term outcome in steroid-dependent nephrotic syndrome treated with rituximab. Pediatr Nephrol 31(1):89–95
Ito S, Kamei K, Ogura M, Udagawa T, Fujinaga S, Saito M, Sako M, Iijima K (2013) Survey of rituximab treatment for childhood-onset refractory nephrotic syndrome. Pediatr Nephrol 28(2):257–264
Ito S, Kamei K, Ogura M, Sato M, Fujimaru T, Ishikawa T, Udagawa T, Iijima K (2011) Maintenance therapy with mycophenolate mofetil after rituximab in pediatric patients with steroid-dependent nephrotic syndrome. Pediatr Nephrol 26(10):1823–1828
Sinha A, Bhatia D, Gulati A, Rawat M, Dinda AK, Hari P, Bagga A (2014) Efficacy and safety of rituximab in children with difficult-to-treat nephrotic syndrome. Nephrol Dial Transpl 30(1):96–106
Kemper MJ, Gellermann J, Habbig S, Krmar RT, Dittrich K, Jungraithmayr T, Pape L, Patzer L, Billing H, Weber L (2011) Long-term follow-up after rituximab for steroid-dependent idiopathic nephrotic syndrome. Nephrol Dial Transpl 27(5):1910–1915
Chan EY-H, Webb H, Yu E, Ghiggeri GM, Kemper MJ, Ma AL-T, Yamamura T, Sinha A, Bagga A, Hogan J (2020) Both the rituximab dose and maintenance immunosuppression in steroid-dependent/frequently-relapsing nephrotic syndrome have important effects on outcomes. Kidney Int 97(2):393–401
Fujinaga S, Hirano D, Mizutani A, Sakuraya K, Yamada A, Sakurai S, Shimizu T (2017) Predictors of relapse and long-term outcome in children with steroid-dependent nephrotic syndrome after rituximab treatment. Clin Exp Nephrol 21(4):671–676
Hogan J, Dossier C, Kwon T, Macher M-A, Maisin A, Couderc A, Niel O, Baudouin V, Deschênes G (2018) Effect of different rituximab regimens on B cell depletion and time to relapse in children with steroid-dependent nephrotic syndrome. Pediatr Nephrol 34(2):253–259
Ahn YH, Kim SH, Han KH, Choi HJ, Cho H, Lee JW, Shin JI, Cho MH, Lee JH, Park YS (2018) Efficacy and safety of rituximab in childhood-onset, difficult-to-treat nephrotic syndrome: A multicenter open-label trial in Korea. Medicine (Baltimore) 97(46)
Webb H, Jaureguiberry G, Dufek S, Tullus K, Bockenhauer D (2016) Cyclophosphamide and rituximab in frequently relapsing/steroid-dependent nephrotic syndrome. Pediatr Nephrol 31(4):589–594
Maxted AP, Dalrymple RA, Chisholm D, McColl J, Tse Y, Christian MT, Reynolds BC (2019) Low-dose rituximab is no less effective for nephrotic syndrome measured by 12-month outcome. Pediatr Nephrol 34(5):855–863
Basu B, Mahapatra T, Mondal N (2015) Mycophenolate mofetil following rituximab in children with steroid-resistant nephrotic syndrome. Pediatrics 136(1):e132–e139
Fujinaga S, Someya T, Watanabe T, Ito A, Ohtomo Y, Shimizu T, Kaneko K (2013) Cyclosporine versus mycophenolate mofetil for maintenance of remission of steroid-dependent nephrotic syndrome after a single infusion of rituximab. Eur J Pediatr 172(4):513–518
Horinouchi T, Sako M, Nakanishi K, Ishikura K, Ito S, Nakamura H, Oba MS, Nozu K, Iijima K (2018) Study protocol: mycophenolate mofetil as maintenance therapy after rituximab treatment for childhood-onset, complicated, frequently-relapsing nephrotic syndrome or steroid-dependent nephrotic syndrome: a multicenter double-blind, randomized, placebo-controlled trial (JSKDC07). BMC nephrol 19(1):302
Bonanni A, Calatroni M, D'alessandro M, Signa S, Bertelli E, Cioni M, Di Marco E, Biassoni R, Caridi G, Ingrasciotta G (2018) Adverse events linked with the use of chimeric and humanized anti-CD20 antibodies in children with idiopathic nephrotic syndrome. Br J Clin Pharmacol 84(6):1238–1249
Parmentier C, Delbet J-D, Decramer S, Boyer O, Hogan J, Ulinski T (2019) Immunoglobulin serum levels in rituximab-treated patients with steroid-dependent nephrotic syndrome. Pediatr Nephrol 35(3):455–462
Fujinaga S, Sakuraya K, Yamada A, Urushihara Y, Ohtomo Y, Shimizu T (2015) Positive role of rituximab in switching from cyclosporine to mycophenolate mofetil for children with high-dose steroid-dependent nephrotic syndrome. Pediatr Nephrol 30(4):687–691
Kamei K, Ogura M, Sato M, Ito S, Ishikura K (2018) Infusion reactions associated with rituximab treatment for childhood-onset complicated nephrotic syndrome. Pediatr Nephrol 33(6):1013–1018
Tsutsumi Y, Kanamori H, Mori A, Tanaka J, Asaka M, Imamura M, Masauzi N (2005) Reactivation of hepatitis B virus with rituximab. Expert Opin Drug Saf 4(3):599–608
Chaumais M-C, Garnier A, Chalard F, Peuchmaur M, Dauger S, Jacqz-Agrain E, Deschênes G (2009) Fatal pulmonary fibrosis after rituximab administration. Pediatr Nephrol 24(9):1753–1755
Boren EJ, Cheema GS, Naguwa SM, Ansari AA, Gershwin ME (2008) The emergence of progressive multifocal leukoencephalopathy (PML) in rheumatic diseases. J Autoimmun 30(1-2):90–98
Gea-Banacloche JC (2010) Rituximab-associated infections. Seminars in hematology 47(2):187–198
Sellier-Leclerc A-L, Belli E, Guérin V, Dorfmüller P, Deschênes G (2013) Fulminant viral myocarditis after rituximab therapy in pediatric nephrotic syndrome. Pediatr Nephrol 28(9):1875–1879
Sato M, Ito S, Ogura M, Kamei K, Miyairi I, Miyata I, Higuchi M, Matsuoka K (2013) Atypical Pneumocystis jiroveci pneumonia with multiple nodular granulomas after rituximab for refractory nephrotic syndrome. Pediatr Nephrol 28(1):145–149
Kamei K, Takahashi M, Fuyama M, Saida K, Machida H, Sato M, Ogura M, Ito S (2014) Rituximab-associated agranulocytosis in children with refractory idiopathic nephrotic syndrome: case series and review of literature. Nephrol Dial Transpl 30(1):91–96
Peuvrel L, Chiffoleau A, Quéreux G, Brocard A, Saint-Jean M, Batz A, Jolliet P, Dréno B (2013) Melanoma and rituximab: an incidental association? Derm 226(3):274–278
Velter C, Pagès C, Schneider P, Osio A, Brice P, Lebbé C (2014) Four cases of rituximab-associated melanoma. Melanoma Res 24(4):401–403
Tarella C, Passera R, Magni M, Benedetti F, Rossi A, Gueli A, Patti C, Parvis G, Ciceri F, Gallamini A (2010) Risk factors for the development of secondary malignancy after high-dose chemotherapy and autograft, with or without rituximab: a 20-year retrospective follow-up study in patients with lymphoma. J Clin Oncol 29(7):814–824
Colucci M, Carsetti R, Serafinelli J, Rocca S, Massella L, Gargiulo A, Lo Russo A, Capponi C, Cotugno N, Porzio O (2019) Prolonged impairment of immunological memory after anti-CD20 treatment in pediatric idiopathic nephrotic syndrome. Front Immunol 10:1653
Wijetilleka S, Jayne DR, Mukhtyar C, Ala A, Bright PD, Chinoy H, Harper L, Kazmi MA, Kiani-Alikhan S, Li CK (2019) Recommendations for the management of secondary hypogammaglobulinaemia due to B cell targeted therapies in autoimmune rheumatic diseases. Rheumatology 58(5):889–896
Kamei K, Ishikura K, Sako M, Aya K, Tanaka R, Nozu K, Kaito H, Nakanishi K, Ohtomo Y, Miura K (2017) Long-term outcome of childhood-onset complicated nephrotic syndrome after a multicenter, double-blind, randomized, placebo-controlled trial of rituximab. Pediatr Nephrol 32(11):2071–2078
Basu B, Sander A, Preussler S, Sinha Mahapatra T, Schaefer F (2019) IPN11036-82 Long-term efficacy of rituximab & MMF maintenance - therapy in childhood SDNS. Abstracts of the 18th Congress of the International Pediatric Nephrology Association, Venice (Italy), October 2019. Pediatr Nephrol 34:1821–2260. https://doi.org/10.1007/s00467-019-04325-4
Kim JH, Park E, Hyun HS, Cho MH, Ahn YH, Choi HJ, Kang HG, Ha I-S, Cheong HI (2017) Long-term repeated rituximab treatment for childhood steroid-dependent nephrotic syndrome. Kidney Res Clin Pract 36(3):257
Ramachandran R, Bharati J, Rao I, Kashif AW, Nada R, Minz R, Gupta KL, Kohli HS (2019) Persistent CD-19 depletion by rituximab is cost-effective in maintaining remission in calcineurin-inhibitor dependent podocytopathy. Nephrology (Carlton) 24(12):1241–1247
Delbet JD, Leclerc G, Ulinski T (2019) Idiopathic nephrotic syndrome and rituximab: may we predict circulating B lymphocytes recovery? Pediatr Nephrol 34(3):529–532
Sato M, Kamei K, Ogura M, Ishikura K, Ito S (2018) Relapse of nephrotic syndrome during post-rituximab peripheral blood B-lymphocyte depletion. Clin Exp Nephrol 22(1):110–116
Colucci M, Corpetti G, Emma F, Vivarelli M (2018) Immunology of idiopathic nephrotic syndrome. Pediatr Nephrol 33(4):573–584
Colucci M, Carsetti R, Cascioli S, Serafinelli J, Emma F, Vivarelli M (2019) B cell phenotype in pediatric idiopathic nephrotic syndrome. Pediatr Nephrol 34(1):177–181
Colucci M, Carsetti R, Cascioli S, Casiraghi F, Perna A, Ravà L, Ruggiero B, Emma F, Vivarelli M (2016) B cell reconstitution after rituximab treatment in idiopathic nephrotic syndrome. J Am Soc Nephrol 27(6):1811–1822
Kimata T, Hasui M, Kino J, Kitao T, Yamanouchi S, Tsuji S, Kaneko K (2013) Novel use of rituximab for steroid-dependent nephrotic syndrome in children. Am J Npehrol 38(6):483–488
Takahashi T, Okamoto T, Sato Y, Yamazaki T, Hayashi A, Aoyagi H, Ueno M, Kobayashi N, Uetake K, Nakanishi M (2019) Periodically repeated rituximab administrations in children with refractory nephrotic syndrome: 2-year multicenter observational study. Pediatr Nephrol 34(1):87–96
Ahn YH, Kang HG, Lee JM, Choi HJ, Ha I-S, Cheong HI (2014) Development of antirituximab antibodies in children with nephrotic syndrome. Pediatr Nephrol 29(8):1461–1464
Chan C-Y, Liu ID, Resontoc LP, Ng K-H, Chan Y-H, Lau PY-W, Than M, Jordan SC, Lam K-P, Yeo W-S (2016) T lymphocyte activation markers as predictors of responsiveness to rituximab among patients with FSGS. Clin J Am Soc Nephrol 11(8):1360–1368
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chan, E.Yh., Tullus, K. Rituximab in children with steroid sensitive nephrotic syndrome: in quest of the optimal regimen. Pediatr Nephrol 36, 1397–1405 (2021). https://doi.org/10.1007/s00467-020-04609-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-020-04609-0