
Abstract
Background
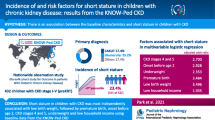
Among children who receive a kidney transplant, short stature is associated with a more complicated post-transplant course and increased mortality. Short stature prior to transplant may reflect the accumulated risk of multiple factors during chronic kidney disease (CKD); however, its relationship with post-transplant kidney function has not been well characterized.
Methods
In the Chronic Kidney Disease in Children (CKiD) cohort restricted to children who received a kidney transplant, short stature (i.e., growth failure) was defined as age-sex-specific height < 3rd percentile. The outcome was time to estimated glomerular filtration rate (eGFR) < 45 ml/min/1.73 m2 after transplant. Parametric survival models, including adjustment for disease severity, socioeconomic status (SES), and parental height by inverse probability weighting, described the relative times to eGFR< 45 ml/min/1.73 m2.
Results
Of 138 children (median CKD duration at transplant: 13 years), 20% (28) had short stature before the transplant. The median time to eGFR < 45 ml/min/1.73 m2 after kidney transplantation was 6.6 years and those with short stature had a significantly faster time to the poor outcome (log-rank p value 0.004). Children with short stature tended to have lower SES, nephrotic proteinuria, higher blood pressure, and lower mid-parental height before transplant. After adjusting for these variables, children with growth failure had 40% shorter time to eGFR < 45 ml/min/1.73 m2 than those with normal stature (relative time 0.60, 95%CI 0.32, 1.03).
Conclusions
Short stature was associated with a faster time to low kidney function after transplant. SES, disease severity, and parental height partially explained the association. Clinicians should be aware of the implications of growth failure on the outcome of this unique population, while continued attempts are made to define modifiable factors that contribute to this association.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Short stature, also referred to as growth failure, is commonly observed at all levels of impaired kidney function among children with chronic kidney disease (CKD), and the prevalence increases in advanced CKD stages [1]. Similarly, the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) has shown that among pediatric kidney transplant recipients, lower estimated glomerular filtration rate (eGFR) 30 days after transplant was associated with lower height z-scores [2]. Growth failure is associated with increased mortality, hospitalizations, and infections [3, 4] after kidney transplantation. A recent retrospective analysis of 2008 children after their first kidney transplantation in the US Renal Data System (USRDS) database documented a higher risk of all-cause mortality, as well as cardiac- and infection-related death in patients who had short stature [5]. The relationship between short stature prior to transplant and post-transplant kidney function, however, has not been well characterized in previous literature.
The underlying cause of growth failure in children is multifactorial. Nutritional status and severity of chronic diseases have been well described as important risk factors [6, 7]. In children with CKD, growth can be impaired by various physiological mechanisms, including renal osteodystrophy, metabolic acidosis, and perturbations in the growth hormone axis [8]. Additionally, lower socioeconomic status (SES) is associated with lower height z-score across diverse populations [9,10,11]. Therefore, we hypothesized that short stature reflects the accumulated risk of overall nutritional status, disease severity, SES, and potential metabolic imbalances during the course of CKD progression and that these same risk factors may, at least partially explain poor graft outcomes in short children after transplantation. Based on this hypothesis, we aimed to evaluate short stature as a marker to identify patients at an increased risk of low kidney function (i.e., time to eGFR < 45 ml/min/1.73 m2) after transplant in the Chronic Kidney Disease in Children (CKiD) cohort. CKiD is a long-standing and well-characterized cohort that is now empowered to link detailed pre-transplant factors to post-transplant outcome. It provides a unique opportunity to evaluate the risks of a low post-transplant eGFR that is associated with short stature in advanced CKD stages. Understanding this relationship may assist clinicians to distinguish vulnerable patients at high risk and to tailor care and treatment plans.
Materials and methods
Study design and population
The CKiD study is a multicenter, prospective cohort study conducted at 54 pediatric nephrology centers across North America since 2003. Eligible children were between 1 and 16 years with mild to moderate CKD based on an eGFR of 30–90 ml/min/1.73 m2 at enrollment. Details of the study visits have been previously described [12]. Briefly, data collected at the regular visits included kidney function, growth, socioeconomic status, cardiovascular health, and neurocognitive development. These in-person study visits ceased after documented initiation of renal replacement therapy (RRT), either dialysis or transplantation. After RRT, participants were followed by annual short data collection protocols (interviews) completed over phone, in person, or online. Data collected were self-reported RRT status, health care utilization status, mediation use, physical symptoms, and quality of life. In parallel, clinical coordinators extracted serum creatinine and anthropometric data from medical charts corresponding to clinical visits.
Our study sample comprised children who received a first kidney transplant before age 21 with available serum creatinine data after kidney transplantation. Since the primary aim of the study was to investigate growth and kidney function after kidney transplant, children who did not have anthropometric data collected within 3 years prior to receiving a kidney transplant were excluded from this analysis.
Outcome
The primary outcome of interest was time from kidney transplant to serum creatinine-based eGFR < 45 ml/min/1.73 m2. The CKiD bedside equation [13] was used since external studies have demonstrated its validity in a post-transplant population [14]. To account for variability in eGFR immediately after kidney transplant, we excluded observations within 3 months after kidney transplant. For participants with any observed eGFR value less than 45 ml/min/1.73 m2, the event time was estimated by linear interpolation between two post-transplant eGFR data points. In our study sample, there were 18 children with the first observed eGFR after transplant below 45 ml/min/1.73 m2 (i.e., “prevalent event”). For these participants, these eGFR values were measured several years after transplant (median 3.5, IQR 3.2-4.1 years) compared to the rest of the study sample (median 0.9, IQR 0.4-2.0 years). To address this missing data problem, eGFR at 3 months after transplant was imputed based on their pre-transplant characteristics using a single imputation model informed by the observed participants. We assessed the robustness of our simple imputation model against multiple imputation with consistent results. To investigate potential differences between those with a “prevalent event” (n = 18) and an “incident event” (n = 25 with an observed GFR < 45 ml/min/1.73 m2), pre-transplant characteristics were compared and no significant differences were found between these subgroups. For the 18 children, imputed eGFR was the anchor for linear interpolation to their first observed data point when eGFR < 45 ml/min/1.73 m2. Participants free of the event were censored at the last post-transplant visit.
Exposures
Height and weight were based on the mean of two repeated measurements using a stadiometer and standing scale at regular study visits before kidney transplant. After kidney transplant, height and weight data were obtained from medical chart review. We calculated age-sex-specific height percentile and z-score using US Centers for Disease Control and Prevention (CDC) growth charts with the US general population as the reference [15]. Since participants should have attained adult height at around age 20, we used the CDC reference for 20-year-olds to calculate height z-score for participants who were older than 20 years (n = 5, maximum age 20.6 years) at the time of transplant. In this study, short stature was defined as the last height prior to kidney transplant below the third percentile of general population with same age and sex (i.e., height z-score < −1.88).
Pre-transplant characteristics
At the baseline visit, demographic, SES, kidney disease characteristics, birth history, and medication use of the study participants were collected. SES characteristics included maternal education, household income, private health insurance, and enrollment in federal food assistance program. Birth history included gestational age, low birth weight (< 2500 g), and small for gestational age. Kidney disease characteristics included CKD diagnoses (glomerular vs. non-glomerular), duration of CKD, having dialysis before transplant, duration of the dialysis, and urine protein and creatinine ratio (uP/C). Proteinuria (urine protein/creatinine) was categorized as minimal (< 0.2 mg/mg), elevated (0.2–2 mg/mg), or nephrotic (> 2 mg/mg). Pre-transplant GFR was estimated by height (ht, in meter), serum creatinine (Scr), cystatin C, and blood urea nitrogen (BUN) using the equation: eGFR = 39.8 × (ht(m)/Scr)0.456(1.8/cystatin C)0.418(30/BUN)0.0791.076male(ht(m)/1.4)0.179 [16]. Longitudinal eGFR was used to calculate average annual percent of change as a metric of pre-transplant kidney function decline [17]. Additionally, systolic and diastolic blood pressure were measured at regular visits and standardized by age, gender, and height to the normal population [18]. Pre-transplant urine protein/creatinine ratio, GFR level and rate of change, and blood pressure were used as indicators of disease severity in this analysis. At each pre-transplant study visit, participants were asked whether they were “currently taking growth hormone/vitamin D supplements/alkali therapy.” Any use of growth hormone/vitamin D supplements/alkali therapy was defined as ever reported use from baseline to when the last height was measured before transplant. Self-reported heights of children’s biological parents were collected at baseline. Mid-parental height was calculated by the equation [19] as a predictor of children’s projected adult height.
Statistical analyses
Pre-transplant characteristics including demographics, SES, CKD characteristics, birth history, and medication use were summarized by short stature. Differences in pre-transplant characteristics between the two groups was assessed using t tests and chi-square tests. To account for imbalances in pre-transplant characteristics between the two groups, propensity scores were used to construct stabilized inverse probability weights [20]. Specifically, multivariate logistic regression was used to determine the propensity for short stature (as the dependent variable) with SES factors, baseline uP/C, blood pressure, low birth weight, and mid-parental height being predictors. The cumulative incidence of eGFR < 45 ml/min/1.73 m2 after transplant among children with and without short stature were estimated using non-parametric methods in the unweighted and weighted study samples. To estimate relative times between the two groups, parametric survival methods using a conventional log-normal distribution were fit to the unweighted and weighted populations, respectively. In the adjusted model, 95% confidence intervals of parameter estimates were obtained from 1000 bootstrapped samples [21]. All analyses were performed using SAS 9.4 (SAS Institute, Inc.) and R 3.4.3.
Results
Of 891 CKiD participants enrolled with CKD, a total of 192 reported receiving a kidney transplant as of September 2016. Of these, 152 provided serum creatinine data during their post-transplant period. Fourteen children were excluded because they either received a transplant after 21 years of age or did not have growth data collected within 3 years before transplant. Thus, 138 children were included in the present analysis. These study participants have a median of 13 years [IQR 9-16] of CKD duration at the time when they received kidney transplantation. The estimated median time to eGFR< 45 ml/min/1.73m2 was 6.6 years after kidney transplantation.
Table 1 describes pre-transplant characteristics stratified by short stature. Of 138 eligible participants, 28 children had short stature prior to receiving their kidney transplant. Among the short stature group, 74% had lower maternal education, 36% reported a low household income, and 36% did not have any private health insurance. In contrast, in the normal stature group, the corresponding proportions were 67%, 29%, and 28%, respectively. Additionally, children having short stature reported higher proportion of low birth weight and had higher blood pressure at baseline. Other demographic and CKD characteristics, as well as BMI z-scores prior to transplant, did not differ between exposure groups. Mid-parental height was lower in the short stature group, indicating the effect of genetics. Thirty-nine percent of children having short stature received growth hormone prior to the transplant, whereas only 28% with normal stature received growth hormone. Similarly, more children received alkali therapy in the short stature group. Table 2 presents the summary statistics in the respective study groups after we applied inverse probability weights to achieve balance in potentially confounding variables. The application of inverse probability weights demonstrated no significant differences in the pre-transplant characteristics including SES, disease characteristics, and mid-parental height and allowed for a comparison of time-to-event that is not confounded by these factors.
Figure 1 displays times to eGFR < 45 ml/min/1.73 m2 by non-parametric step functions and parametric survival curves, in the unweighted (left panel) and weighted (right panel) samples. Twenty-five percent of children with short stature experienced eGFR < 45 ml/min/1.73 m2 by 1.5 years; among children with normal stature, 25% experienced the outcome by 3.7 years (log-rank p value 0.004).

Unweighted (left panel) and inverse probability weighted (right panel) step functions of the time to estimated glomerular filtration rate (eGFR) < 45 ml/min/1.73 m2 after kidney transplant, by short stature (N = 138). Cumulative incidence curves were based on parametric survival models with log-normal distribution for each group with location (β) and scale (σ) and denoted as LN(β,σ)
Parametric survival models were fit without and with inverse probability weights (i.e., naïve and adjusted) to evaluate the relationship between time to eGFR < 45 ml/min/1.73 m2 and short stature. In the naïve analysis, those with growth failure had a relative time of 0.51 (95%CI 0.28, 0.91). This is interpreted as participants with growth failure prior to transplant had a 49% shorter time to the low eGFR outcome, and this effect was statistically significant. The effect estimate was attenuated in the weighted sample, suggesting that SES factors, CKD characteristics, and mid-parental height (as a proxy for genetic influence) partially explained the observed association of short stature with low eGFR after transplant. The association persisted after the adjustment and was borderline significance with a relative time of 0.60 (95% CI 0.32, 1.03). In other words, those with short stature had a 40% shorter time to eGFR < 45 ml/min/1.73 m2 after transplant, compared to children with normal stature, when both groups had the same distribution of observed pre-transplant characteristics (i.e., adjusted for covariates).
Discussion
In this unique pediatric population in which anthropometric and socioeconomic data were collected prior to kidney transplant during the CKD phase, we explored the association of short stature with outcome after transplant. Kidney transplant outcomes were based on longitudinal post-transplant eGFR data, with poor outcome defined as eGFR < 45 ml/min/1.73 m2. Our results showed that short stature was associated with faster time to the poor outcome and can be potentially used as an indicator to identify high-risk patients.
Informed by previous publications [22,23,24,25], we hypothesized that short stature was an indicator reflecting the composite effect of low SES, disease severity, over all nutritional status, disturbances in mineral homeostasis, and chronic inflammation prior to kidney transplant. The attenuated association comparing the adjusted model with the crude model suggests that SES, CKD characteristics, and parental height explain, at least in part, the faster time to low eGFR after transplant for those with growth failure. Importantly, after the adjustment, the association persisted and children with short stature had a 40% faster progression to the poor outcome. We thus speculate that mineral metabolic disorder, chronic inflammation, and poor nutrition may also contribute to the increased risk of poor transplant prognosis among children with growth failure.
To investigate the potential role of mineral metabolic disorders and outcomes in this population, we conducted an ad hoc analysis and found that those with short stature had higher levels of C-terminal FGF23 (median level 408 vs. 272 RU/mL, p < 0.001). This is consistent with the known CKD and ESRD related risks associated with these biomarkers [26,27,28,29,30] and provide preliminary evidence of pre-transplant levels conferring risk post-transplant. It should be noted that the FGF23 measurements occurred at heterogeneous time prior to transplant and should be considered exploratory data. Future studies should incorporate laboratory biomarkers to describe pre-transplant mineral disturbances in the context of post-transplant outcomes.
In our population, there was a higher proportion of children who received growth hormone therapy before transplant among those with short stature (39% vs. 28%), but 61% were untreated. This may indicate suboptimal treatment and poor growth outcomes after therapy, and information in regard of GH therapy compliance and the impact of therapy on a monthly or yearly basis are needed for further investigation. Nevertheless, since growth hormone therapy is an efficacious and safe treatment for growth failure in children with CKD, increasing its utilization and effectiveness early in the course of CKD may lead to better outcomes after transplantation. Furthermore, this also provides hints that chronic inflammation might serve as the underlying link since it can exacerbate perturbations in the growth hormone/insulin-like growth factor 1 axis [31, 32] and it too can accelerate deterioration of graft function [33, 34].
There were several strengths of this study that identified short stature as a potentially meaningful risk factor for poor transplant prognosis in children. Firstly, SES, disease severity, and parental height were relatively strong confounders and were taken into account by inverse probability weighting. After the adjustment, a persistent association of growth failure with the outcome remained. Our analysis was also strengthened by the CKiD study design which collected longitudinal data during both the CKD stage and post-transplant phase of pediatric kidney disease in order to prospectively link exposures to outcomes. Lastly, we developed an applied methodology to estimate poor kidney transplant outcomes based on longitudinal GFR data after transplant. This method allows us to define a subclinical study endpoint (i.e., time to eGFR < 45 ml/min/1.73m2) and incorporate prevalent events into our analysis.
There were several limitations to our analysis. First, the study population was a subset of a CKD cohort and detailed transplant data were not available. We acknowledge that the relationship between short stature and post-transplant kidney function may be influenced by major transplantation characteristics which were not available in this analysis, including allograft mismatch, donor source, delayed graft function, non-adherence to transplant medication, and rejection episodes. As a sensitivity analyses, we considered height percentile less than the 25th percentile, as well as a continuous variable (height z-scores) and the results were consistent, but attenuated, compared to using the more typical definition of height less than the third percentile. Secondly, the subclinical endpoint of eGFR < 45 ml/min/1.73 m2 was considered a reasonable and clinically meaningful proxy for poor graft outcome, but graft failure may not be imminent for these individuals. In addition, the event time was estimated based on a combination of observed and imputed eGFR values and may not be precise. Nevertheless, this subclinical study endpoint is helpful for clinicians to identify patients at a higher risk in a preemptive manner and consider interventions to improve prognosis. To address how the event time was estimated, we compared more complex models using multiple imputation by chained equations and found very similar outcomes as our simple approach. Lastly, this subset of the CKiD study was relatively small compared to kidney transplant registries in which outcomes are typically assessed. Therefore, to establish short stature as a risk factor for kidney transplant prognosis, future studies should validate the relationship in an independent cohort where sufficient number of clinical events, donor’s source, body size, as well as other important transplant characteristics, are available.
In summary, this analysis suggested that short stature prior to kidney transplant was associated with a higher risk of lower kidney function after transplant among pediatric recipients. This relationship was partially, but not entirely, explained by pre-transplant SES, disease severity, and parental height. Clinicians should be aware of the implications of growth failure on transplant outcomes in this unique population. Future research should continue to identify modifiable factors that contribute to poor transplant outcomes and effective interventions to minimize or delay risk.
References
Wong H, Mylrea K, Feber J, Drukker A, Filler G (2006) Prevalence of complications in children with chronic kidney disease according to KDOQI. Kidney Int 70(3):585–590
Fine R, Martz K, Stablein D (2010) What have 20 years of data from the North American pediatric renal transplant cooperative study taught us about growth following renal transplantation in infants, children, and adolescents with end-stage renal disease? Pediatr Nephrol 25(4):739–746
Wong CS, Gipson DS, Gillen DL, Emerson S, Koepsell T, Sherrard DJ, Watkins SL, Stehman-Breen C (2000) Anthropometric measures and risk of death in children with end-stage renal disease. Am J Kidney Dis 36(4):811–819
Furth SL, Hwang W, Yang C, Neu AM, Fivush BA, Powe NR (2002) Growth failure, risk of hospitalization and death for children with end-stage renal disease. Pediatr Nephrol 17(6):450–455
Ku E, Fine RN, Hsu CY, McCulloch C, Glidden DV, Grimes B, Johansen KL (2016) Height at first RRT and mortality in children. Clin J Am Soc Nephrol 11(5):832–839
Zemel BS, Riley EM, Stallings VA (1997) Evaluation of methodology for nutritional assessment in children: anthropometry, body composition, and energy expenditure. Annu Rev Nutr 17(1):211–235
Prista A, Maia JAR, Damasceno A, Beunen G (2003) Anthropometric indicators of nutritional status: implications for fitness, activity, and health in school-age children and adolescents from Maputo, Mozambique. Am J Clin Nutr 77(4):952–959
Greenbaum LA, Warady BA, Furth SL (2009) Current advances in chronic kidney disease in children: growth, cardiovascular, and neurocognitive risk factors. Semin Nephrol 29(4):425–434
Abubakar A (2012) Socioeconomic status, anthropometric status and developmental outcomes of East-African children. In: Handbook of anthropometry. 2012th ed. Springer, New York, pp 2679–2693
Gurzkowska B, Kułaga Z, Litwin M, Gurzkowska B, Kułaga Z, Litwin M (2014) The relationship between selected socioeconomic factors and basic anthropometric parameters of school-aged children and adolescents in Poland. Eur J Pediatr 173(1):45–52
Gross R, Lima FD, Freitas CJ, Gross U (1990) The relationships between selected anthropometric and socio-economic data in schoolchildren from different social strata in Rio de Janeiro, Brazil. Rev Saude Publica 24(1):11–19
Furth SL, Cole SR, Moxey-Mims M, Kaskel F, Mak R, Schwartz G, Wong C, Muñoz A, Warady BA (2006) Design and methods of the chronic kidney disease in children (CKiD) prospective cohort study. Clin J Am Soc Nephrol 1(5):1006–1015
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20(3):629–637
de Souza V, Cochat P, Rabilloud M, Selistre L, Wagner M, Hadj-Aissa A, Dolomanova O, Ranchin B, Iwaz J, Dubourg L (2015) Accuracy of different equations in estimating GFR in pediatric kidney transplant recipients. Clin J Am Soc Nephrol 10(3):463–470
Center for Disease Control and Prevention (2000) Clinical Growth Charts. http://www.cdc.gov/growthcharts/ . Accessed 13 December 2017
Schwartz GJ, Schneider MF, Maier PS, Moxey-Mims M, Dharnidharka VR, Warady BA, Furth SL, Muñoz A (2012) Improved equations estimating GFR in children with chronic kidney disease using an immunonephelometric determination of cystatin C. Kidney Int 82(4):445–453
Pierce CB, Cox C, Saland JM, Furth SL, Muñoz A (2011) Methods for characterizing differences in longitudinal glomerular filtration rate changes between children with glomerular chronic kidney disease and those with nonglomerular chronic kidney disease. Am J Epidemiol 174(5):604–612
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents (2004) The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 114(2):555–576
Nwosu BU, Lee MM (2008) Evaluation of short and tall stature in children. Am Fam Physician 78(5):597–604
Ng DK, Moxey-Mims M, Warady BA, Furth SL, Muñoz A (2016) Racial differences in renal replacement therapy initiation among children with a nonglomerular cause of chronic kidney disease. Ann Epidemiol 26(11):780–787
Cole SR, Hernán MA (2008) Constructing inverse probability weights for marginal structural models. Am J Epidemiol 168(6):656–664
Rees L, Mak RH (2011) Nutrition and growth in children with chronic kidney disease. Nat Rev Nephrol 7(11):615–623
Apostolou A, Printza N, Karagiozoglou-Lampoudi T, Dotis J, Papachristou F (2014) Nutrition assessment of children with advanced stages of chronic kidney disease—a single center study. Hippokratia 18(3):212–216
Wesseling K, Bakkaloglu S, Salusky I (2008) Chronic kidney disease mineral and bone disorder in children. Pediatr Nephrol 23(2):195–207
Hidalgo G, Ng DK, Moxey-Mims M, Minnick ML, Blydt-Hansen T, Warady BA, Furth SL (2013) Association of income level with kidney disease severity and progression among children and adolescents with CKD: a report from the chronic kidney disease in children (CKiD) study. Am J Kidney Dis 62(6):1087–1094
Portale AA, Wolf M, Jüppner H, Messinger S, Kumar J, Wesseling-Perry K, Schwartz GJ, Furth SL, Warady BA, Salusky IB (2014) Disordered FGF23 and mineral metabolism in children with CKD. Clin J Am Soc Nephrol 9(2):344–353
Van Husen M, Fischer AK, Lehnhardt A, Klaassen I, Möller K, Müller-Wiefel KMJ (2010) Fibroblast growth factor 23 and bone metabolism in children with chronic kidney disease. Kidney Int 78(2):200–206
Wolf M, Molnar MZ, Amaral AP, Czira ME, Rudas A, Ujszaszi A, Kiss I, Rosivall L, Kosa J, Lakatos P, Kovesdy CP, Mucsi I (2011) Elevated fibroblast growth factor 23 is a risk factor for kidney transplant loss and mortality. J Am Soc Nephrol 22(5):956–966
Wesseling-Perry K, Tsai EW, Ettenger RB, Jüppner H, Salusky IB (2011) Mineral abnormalities and long-term graft function in pediatric renal transplant recipients: a role for FGF-23? Nephrol Dial Transplant 26(11):3779–3784
Seifert ME, Ashoor IF, Chiang ML, Chishti AS, Dietzen DJ, Gipson DS, Janjua HS, Selewski DT, Hruska KA (2016) Fibroblast growth factor-23 and chronic allograft injury in pediatric renal transplant recipients: a Midwest pediatric nephrology consortium study. Pediatr Transplant 20(3):378–387
Rees L (2016) Growth hormone therapy in children with CKD after more than two decades of practice. Pediatr Nephrol 31(9):1421–1435
Wong SC, Dobie R, Altowati MA, Werther GA, Farquharson C, Ahmed SF (2015) Growth and the growth hormone-insulin like growth factor 1 axis in children with chronic inflammation: current evidence, gaps in knowledge, and future directions. Endocr Rev 37(1):62–110
Van Ree RM, Oterdoom LH, De Vries AP, Gansevoort RT, van der Heide JJ, van Son WJ, Ploeg RJ, de Jong PE, Gans RO, Bakker SJ (2006) Elevated levels of C-reactive protein independently predict accelerated deterioration of graft function in renal transplant recipients. Nephrol Dial Transplant 22(1):246–253
Fink JC, Onuigbo MA, Blahut SA, Christenson RH, Mann D, Bartlett ST, Weir MR (2002) Pretransplant serum C-reactive protein and the risk of chronic allograft nephropathy in renal transplant recipients: a pilot case-control study. Am J Kidney Dis 39(5):1096–1101
Acknowledgements
Data in this manuscript were collected by the Chronic Kidney Disease in children prospective cohort study (CKiD) with clinical coordinating centers (Principal Investigators) at Children’s Mercy Hospital and the University of Missouri-Kansas City (Bradley Warady, MD) and Children’s Hospital of Philadelphia (Susan Furth, MD, PhD), Central Biochemistry Laboratory (George Schwartz, MD) at the University of Rochester Medical Center, and data coordinating center (Alvaro Muñoz, PhD) at the Johns Hopkins Bloomberg School of Public Health.
Funding
The CKiD Study is supported by grants from the National Institute of Diabetes and Digestive and Kidney Diseases, with additional funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Heart, Lung, and Blood Institute (U01-DK-66143, U01-DK-66174, U01DK-082194, U01-DK-66116). Supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award number UL1TR002378. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The CKiD website is located at http://www.statepi.jhsph.edu/ckid.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study protocol was approved by the institutional review board of each participating center. All participants and their families provided informed consent.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, Y., Greenbaum, L.A., Warady, B.A. et al. Short stature in advanced pediatric CKD is associated with faster time to reduced kidney function after transplant. Pediatr Nephrol 34, 897–905 (2019). https://doi.org/10.1007/s00467-018-4165-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-018-4165-2