
Abstract
Background
To date, a surgical method for single-incision laparoscopic cholecystectomy (SILC) has not been standardized. Therefore, this study aimed to introduce a standardized surgical method for SILC, in addition to reporting our experience over 10 years.
Methods
Patients who underwent SILC at a single institution between April 2010 and December 2019 were included in this study. We analyzed the patient demographics and surgical outcomes according to the surgical method used: phase 1 (Konyang standard method, KSM) comprising initial 3-channel SILC, phase 2 (modified KSM, mKSM) comprising 4-channel SILC with a snake retractor, and phase 3 (commercial mKSM, C-mKSM) using a commercial 4-channel port.
Results
Of 1372 patients (mean age, 51.3 years; 781 [56.9%] women), 418 (30.5%) surgeries were performed for acute cholecystitis (AC), 33 (2.4%) were converted to multiport or open cholecystectomy, and 49 (3.6%) developed postoperative complications. The mean operation time (OT) and length of postoperative hospital stay (LOS) were 51.9 min and 2.6 days, respectively. Overall, 325 patients underwent SILC with the KSM, 660 with the mKSM, and 387 with the C-mKSM. In the C-mKSM group, the number of patients with AC was the lowest (26.8% vs. 38.2% vs. 20.4%, p < 0.001) and the OT (51.7 min vs. 55.4 min vs. 46.1 min, p < 0.001), estimated blood loss (24.5 mL vs. 15.5 mL vs. 6.1 mL, p < 0.001), and LOS (2.8 days vs. 2.5 days vs. 2.3 days, p = 0.001) were significantly improved. The surgical outcomes were better in the non-AC group than in the AC group.
Conclusion
Based on our 10 year experience, C-mKSM is a safe and feasible method of SILC in selected patients, although there were lower percentage of patients with AC compared to other groups.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Laparoscopic cholecystectomy (LC) has been the treatment of choice for benign gallbladder (GB) disease since it was first performed by Muhe in 1985 [1, 2]. Since then, as the surgical technique has evolved and surgeons have gained more experience, many surgeons have tried to reduce the number and size of incisions. In 1997, single-incision LC (SILC) was introduced [3]. Previous studies have reported that SILC has a longer operation time as well as a higher risk of bile duct injury and incisional hernia than conventional multiport LC (CMLC); however, it has better cosmetic outcomes and less postoperative pain [4,5,6,7]. Despite increasing interest among many hepatobiliary surgeons, SILC is associated with several surgical difficulties, including a non-ergonomic instrumental array (switching of right and left hands), impingement of the instruments due to a narrow incision, and difficulty in securing a critical view of safety (CVS) [8,9,10]. To overcome these difficulties, many surgeons have introduced their own methods of performing SILC using different surgical instruments and techniques. However, since the surgical method for SILC is not standardized yet, it can be difficult for beginners. Additionally, there are no definite indications for SILC. Although several experienced surgeons have reported on the feasibility of SILC in acute cholecystitis (AC) [11, 12], there are still controversies regarding the safety of SILC in AC.
We previously reported the evolution of the surgical method of SILC, which is called the Konyang standard method (KSM) [13]. The present study aimed to introduce a standardized surgical method for SILC, as well as report our experience and surgical outcomes over 10-year period.
Materials and methods
Patients
Overall, 1372 patients underwent SILC at Konyang University Hospital from April 2010 to December 2019 by three hepatobiliary surgeons. Initially, we excluded patients over 70 years of age, with systemic disease, abnormal cystic duct, or complications of AC. However, after 50 cases had undergone the procedure, SILC was applied to all benign gallbladder diseases, except those where there was a suspicion of malignancy.
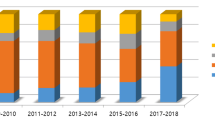
Our surgical method has evolved over time. In the first phase, SILC was performed using a handmade 3-channel port made from surgical gloves. We refer to this as the KSM. Between April 2010 and September 2012, 325 patients underwent SILC with the KSM. In the second phase, SILC was performed using a handmade 4-channel port with a snake liver retractor to expose Calot’s triangle. We refer to this as the modified KSM (mKSM). From October 2012 to August 2016, 660 patients underwent SILC with the mKSM. In the third phase, SILC was performed using a commercial 4-channel port (glove port). We refer to this as the commercially modified KSM (C-mKSM). From September 2016 to December 2019, 387 patients underwent SILC with the C-mKSM.
This study was approved by the Institutional Review Board of Konyang University Hospital, and the requirement of obtaining informed consent was waived due to the retrospective study design (IRB No. 2021-02-004).
Surgical technique of SILC
A glove port (NELIS, Bucheon-si, Gyeonggi-do, Republic of Korea), cable, flexible video laparoscope (Olympus, Tokyo, Japan), snake liver retractor (Artisan, Medford, NJ, USA), laparoscopic long instrument (Richard Wolf, GmbH, Knittlingen, Germany), suction-irrigation with cautery instrument (Endopath Electrosurgery Probe Plus II System, Ethicon, Johnson & Johnson, Somerville, NJ, USA), 5 mm clip applier (The Endo Clip III, Coviden, Mansfield, MA, USA), and 5 and 10 mm Hem-o-Lok clips (Weck Closure Systems, Research Triangle Park, NC, USA) were used during the C-mKSM.
For the C-mKSM, the patient was placed supine in a 15° reverse Trendelenburg position, with the right side tilted upward. The operator stood on the left side of the patient, the scopist stood below the operator, and the assistant stood on the opposite side. A 20 mm trans-umbilical incision was made, and a glove port was inserted. The pneumoperitoneum was created by CO2 insufflation. The flexible laparoscope was inserted into the left lower channel, snake retractor into the right lower channel below the laparoscope, grasper into the left upper channel located on the right side of the laparoscope, while the dissector, scissors, and suction-irrigation with the cautery instrument were inserted into the right upper channel below the grasper (Fig. 1). The operator used the grasper in the right hand for cephalad traction on the body or fundus of the gallbladder in a superolateral direction in order to make the cystic duct perpendicular to the common bile duct (CBD). The assistant used a snake liver retractor that ran under the camera to lift the undersurface of the liver around the portal hepatis to expose Calot’s triangle (Fig. 2A). Then, dissection of the anterior peritoneum along the boundary of Calot’s triangle was performed meticulously using a dissector and cautery hook in the left hand of the operator. When dissecting the posterior aspect of Calot’s triangle, the right and left hands were switched, the GB was pulled with the dissector in the left hand, while the grasper in the right hand was used to dissect the fat and connective tissues (Fig. 2B). After confirming the CVS by dissecting the cystic duct and artery completely (Fig. 2C), the cystic artery was ligated and divided using a 5 mm clip applier, and the cystic duct was ligated and divided using 5 or 10 mm Hem-O-Lok clips with the left hand of the operator. After resection of the cystic artery and duct, the gallbladder was pulled in a cephalad direction using a grasper in the right hand. The connective tissues between the gallbladder bed and hepatic surface were dissected with electrocautery held in the left hand. After bleeding control, the specimen was pulled out through the umbilical incision without an endo-bag at the end of the surgery.

Arrangement of the laparoscope and instruments in commercially modified Konyang standard method. A The illustration shows the 4-channel glove port and devices that enter each channel. B and C The illustration and image show the arrangement of the laparoscope and instruments

Surgical view when applying the modified Konyang standard method. A View after superolateral traction of the gallbladder by the grasper in the right hand and application of the snake liver retractor. B Posterior aspect of Calot’s triangle when the right and left hands are switched. The gallbladder is pulled with the dissector in the left hand, while the grasper in the right hand is used to perform dissection. C Critical view of safety. The infundibulum is pulled laterally with grasper in the right hand and undersurface of the liver is elevated with the snake liver retractor, while the dissector in the left hand is used to perform dissection
Demographic characteristics and surgical outcomes
The general condition and physical fitness of each patient were evaluated using the American Society of Anesthesiologists physical status (PS) classification [14]. The surgery duration was calculated as the time taken from the skin incision to skin closure. Blood loss estimates were obtained from the surgical records. Postoperative hospital stay was defined as the number of days of hospital stay after SILC. Postoperative complications were graded according to the Clavien–Dindo classification [15]. A complication with a level greater than grade II according to the Clavien–Dindo classification was defined as a postoperative major complication. Incisional hernia was defined as a hernia at the umbilical incision site, which was confirmed postoperatively by physical examination and imaging studies.
Statistical analysis
Continuous variables were summarized as means and standard deviations (SD) and were compared using Student’s t-test or analysis of variance. Categorical variables were presented as counts and percentages and were compared using the chi-square test. All tests were two-sided, and statistical significance was set at p values < 0.05. The analyses were performed using SPSS version 24 (SPSS Inc., Chicago, IL, USA).
Results
Study population
Overall, 1372 patients underwent SILC; the patient demographics, disease characteristics, and surgical outcomes are listed in Table 1. The mean age was 51.3 years, and there were 591 (43.1%) men and 781 (56.9%) women. Of the 1372 patients, 331 (24.1%) had GB stones, 119 (8.7%) had GB polyps, 460 (33.5%) had chronic cholecystitis, and 418 (30.5%) had AC. A total of 102 (7.4%) patients had a body mass index (BMI) ≥ 30 kg/m2, and 96 (7.0%) patients had an ASA physical status classification ≥ III. In addition, 313 (22.8%) patients had a history of abdominal surgery. Preoperative percutaneous transhepatic gallbladder drainage (PTGBD) insertion was performed in 137 (10.0%) patients. Preoperative endoscopic sphincterotomy (EST) for CBD stones was performed in 125 (9.1%) patients.
The mean operation time was 51.9 min, and mean estimated blood loss (EBL) was 15.0 mL. Among the 1372 patients, six (0.4%) patients had one additional port insertion, 26 (1.9%) patients had two additional ports, while open conversion was performed in only one (0.1%) patient. Seven (0.5%) adjacent organ injuries were detected during the surgery: three in the CBD, two in the duodenum, and two in the hepatic artery. Drain insertion during the operation was performed in 18 (1.3%) patients. No intraoperative transfusion was performed. Postoperative complications occurred in 49 (3.6%) patients. The mean postoperative hospital stay was 2.6 days. Pathologically, 1104 (80.5%) patients had chronic cholecystitis, 183 (13.4%) had AC, including emphysematous or gangrenous cholecystitis, and five (0.4%) had GB cancer. Postoperative incisional hernia at the umbilical site occurred in five (0.4%) patients. Follow-up for incisional hernia was not routinely performed after SILC. All five patients developed an umbilical incisional hernia 3–6 months after SILC, and were diagnosed with symptom such as abdominal pain and palpable mass on umbilical site. After diagnosis, hernia repair was performed. No postoperative 30-day mortality was observed.
Patients’ characteristics according to the phase of surgery
Of the 1372 patients, 325 underwent SILC with the KSM, 660 with the mKSM, and 387 with the C-mKSM. A comparison of the baseline characteristics and surgical variables according to the phase of surgery is presented in Table 2. In the C-mKSM group, the proportion of patients diagnosed with AC preoperatively (26.8% vs. 38.2% vs. 20.4%, p < 0.001) and ASA ≥ 3 (7.7% vs. 9.1% vs. 2.8%, p = 0.001) were the lowest compared with that in the KSM and mKSM groups. Additionally, the preoperative PTGBD insertion rate was also the lowest in the C-mKSM group (9.8% vs. 13.9% vs. 3.4%, p < 0.001). The patients in the C-mKSM group showed the most improved surgical outcomes, regarding operation time (57.1 min vs. 55.4 min vs. 46.1 min; p < 0.001), EBL (24.5 mL vs. 15.5 mL vs. 6.1 mL; p < 0.001), postoperative hospital stay (2.8 days vs. 2.5 days vs. 2.3 days; p = 0.001), postoperative overall complication (5.2% vs. 4.5% vs. 0.5%; p < 0.001), and major complication (3.1% vs. 2.6% vs. 0.3%; p = 0.012). Incisional hernia was not observed in the C-mKSM group (0.3% vs. 0.6% vs. 0.0%; p = 0.286).
Patients’ characteristics with or without acute cholecystitis
418 patients were preoperatively diagnosed with AC. The demographic and disease characteristics and surgical outcomes for patients with and without AC are provided in Table 3. Patients with AC were older (55.0% vs. 49.6%, p < 0.001) than those without AC, and were more likely to have an ASA ≥ 3 (12.9% vs. 4.4%, p < 0.001). Additionally, the preoperative PTGBD insertion rate (32.8% vs. 0.0%, p < 0.001) and EST rate (18.2% vs. 5.1%, p < 0.001) were higher in patients with AC. The surgical outcomes were better in patients without AC compared to those with AC in terms of the operation time (58.9 min vs. 48.8 min, p < 0.001), EBL (23.0 mL vs. 11.5 mL, p < 0.001), conversion rate (5.7% vs. 0.9%, p < 0.001), postoperative hospital stay (2.8 days vs. 2.4 days, p < 0.001), postoperative overall complication (6.5% vs. 2.3%, p < 0.001), and major complication (5.0% vs 0.7%, p < 0.001). There was no significant difference in the incidence of incisional hernia (0.7% vs. 0.2%, p = 0.151).
Details of the postoperative complications and cause of conversion
Postoperative complications were classified according to the Clavien–Dindo classification, and 48 complications were reported (Table 4). Most cases were classified as Clavien–Dindo grades I and II, which included wound infection, pneumonia, and fluid collection. Grade IIIa complications included three re-operations, three percutaneous drainage insertions for complicated fluid collection, two endoscopic nasobiliary drainage procedures for bile leakage, and one endoscopic stone extraction for a CBD stone. Re-operations included one adhesiolysis for mechanical ileus, one primary repair of the CBD for bile leakage, and one primary repair of the duodenum for duodenal perforation. Clavien–Dindo classification grades IV and V complications were not observed in our study population. In the C-mKSM group, only two cases of postoperative complications were reported.
The reasons for conversion are listed in Table 5. The most common causes of conversion were severe adhesions with inflammation (n = 20) and GB bed bleeding (n = 8). According to the phase of surgery, the conversion rate was lowest in the C-mKSM group (1.5% vs. 3.7% vs. 1.0%; p = 0.069). Bile duct and hepatic artery injury occurred in two cases each in the mKSM and C-mKSM groups.
Discussion
SILS provides the benefits of minimal invasiveness, better cosmetics, and less pain than traditional multiport laparoscopic surgery. However, SILS is associated with several technical difficulties. First, the “chopstick” effect caused by the parallel arrangement of instruments in the umbilicus is considered as an obstacle to surgery [16]. The chopstick effect means that all instruments operate in only one axis, resulting in a restriction in the degree of freedom of each instrument. Second, it is difficult to triangulate SILS. During laparoscopic surgery, trocars are typically placed in triangles for smooth manipulation with adequate visualization. This is called triangulation. The triangulation allows the instruments to work at a 60° manipulation angle with the target tissue, along with avoiding the problems of collision of the instruments and abdominal wall interference [17, 18]. Third, it is difficult to avoid collisions between the camera and instruments because of the narrow incision in SILS.
We applied several improvements to C-mKSM to overcome the difficulties of SILS. We used the cross-hand method to avoid the chopsticks effect. Basically, the main procedures such as dissection and clipping are performed by the right hand, while the left hand is used for traction of the GB in CMLC. However, the left hand plays a major role in mKSM. Since most surgeons are right-handed, it is not easy to switch hands; however, it is not too difficult to dissect or clip with the left hand. The proper alignment of instruments and camera is also important to avoid collision of the instruments and create proper working angles of the instruments. The instruments should be located on the right side of the laparoscope, and the main instruments of the left hand should be placed below the instruments of the right hand as much as possible. Finally, we can maximize the working field by lifting the liver using a snake liver retractor. Using the flexible laparoscope also enables a better view of the operating field while avoiding conflict between the laparoscope and instruments. Several studies have reported the usefulness of a flexible laparoscope or endoscope for SILC [19, 20].
To secure the CVS, visualization of Calot’s triangle is the most important step in laparoscopic cholecystectomy. Many studies have introduced their own surgical techniques to visualize Calot’s triangle. Fronza et al. [21] used transparietal Prolene sutures passed through a Keith needle. The sutures were passed through the infundibulum and/or the fundus of the GB and manipulated extracorporeally to provide additional exposure of Calot's triangle. Podolsky et al. [22] placed a second rigid grasper transfascially without a trocar in the inferior position within a single incision. This allowed a three-instrument technique to mimic multiport cholecystectomy. Recently, Funamizu et al. [23] reported that the exposure of the GB improved after tying of the GB fundus by ENDOLOOP and pulling it out of the peritoneal cavity. In the mKSM, we used a snake retractor to secure the CVS. Unlike previous reports, the mKSM method has the advantages of avoiding damage to the structures, such as the GB or abdominal wall, as well as reducing the operation time because it is easy to apply.
Bile duct injury (BDI) remains the most serious intraoperative complication following LC. Recent population-based studies reported BDI rates from 0.19 to 0.23% [24, 25]. When CMLC was performed for AC for 10 years at our institution, the BDI rate was 0.5% (6/1178), which was similar to that when SILC was performed for AC in the present study (0.5%, 2/418). In the current study, we experienced only three cases (0.2%, 3/1372) of BDI in SILC. According to the Strasberg classification [26], two cases were classified as type D injury and one case as type E2 injury. Type D injuries in both cases occurred during dissection of the Calot triangle and were identified at the time of index procedure. Type E2 injury was recognized in the immediate postoperative period. After insertion of percutaneous drainage for external bile drainage and control of inflammation, reoperation (hepaticojejunostomy) was performed on postoperative day 21.
Intraoperative cholangiography (IOC) was not conducted in all study population, including those with BDI. Whether routine IOC prevents BDI during LC remains controversial. One of the main drawbacks of IOC is the requirement for cannulation of the bile duct with a concomitant increased risk of bile duct injury [27]. In particular, when performing SILC, bile duct cannulation may be technically more difficult. There are several other drawbacks of IOC, such as longer operation time, associated costs, and the infrequency of BDI [28]. Moreover, we performed preoperative magnetic resonance cholangiopancreatography on several patients to confirm biliary anomalies. Consequently, IOC is not routinely performed during SILC in our institution.
The safety of SILC in patients with AC remains controversial. Ikumoto et al. [11] reported the SILC results in 100 patients with AC. The mean operation time was 87.4 min, and the conversion rate was 12%. Byun et al. [29] also reported the surgical outcomes of 220 (15.3%) patients with AC who underwent SILC. The mean operation time was 44.7 min, and the postoperative complication rate was 3.6%. In the present study, 418 (30.5%) patients underwent SILC for AC. Despite the high number and proportion of patients with AC compared to previously reported studies [11, 29,30,31], the surgical outcomes were relatively acceptable in the present study. However, a comparison of postoperative outcomes between AC and other diseases yielded insufficient results to confirm the safety of SILC in AC. Further studies are needed to compare SILC with CMLC to confirm the safety and effectiveness of SILC in patients with AC.
As our surgical method for SILC has evolved, surgical outcomes have also improved. It is clear that advances in the surgical techniques, such as the application of a snake liver retractor or flexible laparoscope, have had a significant impact on the improvement of surgical outcomes. Overcoming the learning curve as the surgeon’s experience accumulates is also an important factor in improving surgical outcomes. The three periods are divided over time as well as evolution of surgical methods; hence, it is believed that the learning curve had a significant impact on the surgical outcomes. Furthermore, in our study, the proportion of AC patients as well as the number of patients with a high ASA (≥ III) and prior abdominal surgery were decreased in phase 3 (C-mKSM) when compared to other phases. We conducted a study on the risk factors for conversion to analyze the causes for the increase in the insertion of additional ports in phase 2 [32]. The study showed that AC or GB empyema on pathology is a risk factor for conversion. On the basis of this study, CMLC was considered in patients with AC or GB empyema in phase 3, since SILC is likely to result in inadequate visualization of Calot’s triangle and greater bleeding risk. Therefore, the improvement in the surgical outcomes depending on the phase of the surgery demonstrates that setting strict indications for SILC according to the patient’s condition or characteristics of the disease can help to improve the surgical outcomes. We plan to conduct a study to determine the optimal indications for SILC.
This study has several limitations. First, since this was a retrospective, single-center study, our results may be biased. Second, we did not conduct an analysis of the surgical results according to the preoperative variables. Further studies are needed to define the optimal indications for SILC. Third, we compared the perioperative outcomes between AC and other diseases only in the SILC group. Additional studies comparing SILC and CMLC for AC are necessary to confirm the safety of SILC for AC. Finally, comparison of surgical outcomes according to three periods is limited by confounding factors such as learning curve and different indications.
In conclusion, based on our 10 year experience, C-mKSM is a safe and feasible method of SILC in selected patients, although there were lower percentage of patients with AC compared to other groups.
References
Mühe E (1991) Laparoscopic cholecystectomy. Zeitschrift fur Gastroenterologie Verhandlungsband 26:204–206
Begos DG, Modlin IM (1994) Laparoscopic cholecystectomy: from gimmick to gold standard. J Clin Gastroenterol 19:325–330
Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I (1997) One-wound laparoscopic cholecystectomy. Br J Surg 84:695
Lurje G, Raptis DA, Steinemann DC, Amygdalos I, Kambakamba P, Petrowsky H, Lesurtel M, Zehnder A, Wyss R, Clavien PA, Breitenstein S (2015) Cosmesis and body image in patients undergoing single-port versus conventional laparoscopic cholecystectomy: a multicenter double-blinded randomized controlled trial (SPOCC-trial). Ann Surg 262:728–734
Haueter R, Schütz T, Raptis DA, Clavien PA, Zuber M (2017) Meta-analysis of single-port versus conventional laparoscopic cholecystectomy comparing body image and cosmesis. Br J Surg 104:1141–1159
Arezzo A, Passera R, Bullano A, Mintz Y, Kedar A, Boni L, Cassinotti E, Rosati R, Fumagalli Romario U, Sorrentino M, Brizzolari M, Di Lorenzo N, Gaspari AL, Andreone D, De Stefani E, Navarra G, Lazzara S, Degiuli M, Shishin K, Khatkov I, Kazakov I, Schrittwieser R, Carus T, Corradi A, Sitzman G, Lacy A, Uranues S, Szold A, Morino M (2017) Multi-port versus single-port cholecystectomy: results of a multi-centre, randomised controlled trial (MUSIC trial). Surg Endosc 31:2872–2880
Pisanu A, Reccia I, Porceddu G, Uccheddu A (2012) Meta-analysis of prospective randomized studies comparing single-incision laparoscopic cholecystectomy (SILC) and conventional multiport laparoscopic cholecystectomy (CMLC). J Gastrointest Surg 16:1790–1801
Qiu Z, Sun J, Pu Y, Jiang T, Cao J, Wu W (2011) Learning curve of transumbilical single incision laparoscopic cholecystectomy (SILS): a preliminary study of 80 selected patients with benign gallbladder diseases. World J Surg 35:2092–2101
Chow A, Purkayastha S, Aziz O, Paraskeva P (2010) Single-incision laparoscopic surgery for cholecystectomy: an evolving technique. Surg Endosc 24:709–714
Chaudhary S, Bhullar JS, Subhas G, Mittal VK, Kolachalam R (2013) Single-incision laparoscopic cholecystectomy (SILC) using non-articulating instruments and conventional trocars-single surgeon experience. J Gastrointest Surg 17:809–813
Ikumoto T, Yamagishi H, Iwatate M, Sano Y, Kotaka M, Imai Y (2015) Feasibility of single-incision laparoscopic cholecystectomy for acute cholecystitis. World J Gastrointest Endosc 7:1327–1333
Chuang SH, Chen PH, Chang CM, Lin CS (2013) Single-incision vs three-incision laparoscopic cholecystectomy for complicated and uncomplicated acute cholecystitis. World J Gastroenterol 19:7743–7750
Kim MK, Choi IS, Moon JI, Lee SE, Yoon DS, Kwon SU, Choi WJ, Sung NS, Park SM (2018) Evolution of the Konyang standard method for single incision laparoscopic cholecystectomy: the result from a thousand case of a single center experience. Ann Surg Treat Res 95:80–86
Mayhew D, Mendonca V, Murthy BVS (2019) A review of ASA physical status—historical perspectives and modern developments. Anaesthesia 74:373–379
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, de Santibanes E, Pekolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, Cameron JL, Makuuchi M (2009) The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 250:187–196
Yin H, Wang Z, Xu J, Guan Y, Zhai B, Zhao L (2011) A specific instrument to facilitate single-incision laparoscopic cholecystectomy: an initial experience. Surg Innov 18:289–293
Supe AN, Kulkarni GV, Supe PA (2010) Ergonomics in laparoscopic surgery. J Min Access Surg 6:31–36
Trejo A, Jung MC, Oleynikov D, Hallbeck MS (2007) Effect of handle design and target location on insertion and aim with a laparoscopic surgical tool. Appl Ergon 38:745–753
Matsui Y, Ryota H, Sakaguchi T, Nakatani K, Matsushima H, Yamaki S, Hirooka S, Yamamoto T, Kwon AH (2014) Comparison of a flexible-tip laparoscope with a rigid straight laparoscope for single-incision laparoscopic cholecystectomy. Am Surg 80:1245–1249
Binenbaum SJ, Teixeira JA, Forrester GJ, Harvey EJ, Afthinos J, Kim GJ, Koshy N, McGinty J, Belsley SJ, Todd GJ (2009) Single-incision laparoscopic cholecystectomy using a flexible endoscope. Arch Surg 144:734–738
Fronza JS, Linn JG, Nagle AP, Soper NJ (2010) A single institution’s experience with single incision cholecystectomy compared to standard laparoscopic cholecystectomy. Surg 148:731–734
Podolsky ER, Curcillo PG 2nd (2010) Reduced-port surgery: preservation of the critical view in single-port-access cholecystectomy. Surg Endosc 24:3038–3043
Funamizu N, Okamoto T, Kumamoto T, Kazama T, Watanabe A, Fujioka S, Yanaga K (2019) Effective method of gallbladder retraction for single-incision laparoscopic cholecystectomy. Asian J Endosc Surg 12:222–226
Mangieri CW, Hendren BP, Strode MA, Bandera BC, Faler BJ (2019) Bile duct injuries (BDI) in the advanced laparoscopic cholecystectomy era. Surg Endosc 33:724–730
Barrett M, Asbun HJ, Chien HL, Brunt LM, Telem DA (2018) Bile duct injury and morbidity following cholecystectomy: a need for improvement. Surg Endosc 32:1683–1688
Strasberg SM, Hertl M, Soper NJ (1995) An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg 180:101–125
Massarweh NN, Flum DR (2007) Role of intraoperative cholangiography in avoiding bile duct injury. J Am Coll Surg 204:656–664
Ausania F, Holmes LR, Ausania F, Iype S, Ricci P, White SA (2012) Intraoperative cholangiography in the laparoscopic cholecystectomy era: why are we still debating? Surg Endosc 26:1193–1200
Byun GY, Lee SR, Koo BH (2018) Safety of single-incision laparoscopic cholecystectomy for acute cholecystitis. ANZ J Surg 88:755–759
Sato N, Kohi S, Tamura T, Minagawa N, Shibao K, Higure A (2015) Single-incision laparoscopic cholecystectomy for acute cholecystitis: a retrospective cohort study of 52 consecutive patients. Int J Surg 17:48–53
Koizumi N, Kobayashi H, Takagi T, Fukumoto K (2017) Is single-incision laparoscopic cholecystectomy feasible for acute cholecystitis? A consecutive study of 60 cases. Surg Laparosc, Endosc Percutaneous Tech 27:379–383
Kim SG, Moon JI, Choi IS, Lee SE, Sung NS, Chun KW, Lee HY, Yoon DS, Choi WJ (2016) Risk factors for conversion to conventional laparoscopic cholecystectomy in single incision laparoscopic cholecystectomy. Ann Surg Treat Res 90:303–308
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Min Ho Um, Seung Jae Lee, In Seok Choi, Ju Ik Moon, Sang Eok Lee, Nak Song Sung, Sung Uk Kwon, In Eui Bae, Seung Jae Rho, Sung Gon Kim, Dae Sung Yoon, and Won Jun Choi have no conflict of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Um, M.H., Lee, S.J., Choi, I.S. et al. Completion of single-incision laparoscopic cholecystectomy using the modified Konyang standard method. Surg Endosc 36, 4992–5001 (2022). https://doi.org/10.1007/s00464-021-08856-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-021-08856-6