
Abstract
Background
Appropriate tissue tension and clear visibility of the dissection area using traction are essential for effective and safe endoscopic submucosal dissection (ESD). We developed a robotic assistive traction device for flexible endoscopy and compared its safety and efficiency in ESD between experienced and novice endoscopists.
Methods
Robotic ESD was performed by experienced and novice endoscopist groups (n = 2, each). The outcomes included time to complete each ESD step, total procedure time, size of the dissected mucosa, rate of en bloc resection, and major adverse events. Furthermore, incision and dissection speeds were compared between groups.
Results
Sixteen gastric lesions were resected from nine live pigs. The submucosal incision speed was significantly faster in the expert group than in the novice group (P = 0.002). There was no significant difference in the submucosal dissection speed between the groups (P = 0.365). No complications were reported in either group.
Conclusions
When the robot was assisting in the ESD procedure, the dissection speed improved significantly, especially in the novice surgeons. Our robotic device can provide simple, effective, and safe multidirectional traction during ESD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Endoscopic submucosal dissection (ESD) is a well-established, minimally invasive treatment for premalignant and early malignant gastrointestinal lesions [1]. Although ESD facilitates a higher rate of en bloc resection compared to other endoscopic resections, it is technically demanding and presents a high risk of complications [2, 3]. The biggest cause of complications is that the visibility of the dissection plane is not secured because of the mucosal flap [4]. Appropriate tissue tension and clear visibility of the tissue to be dissected using traction are essential for effective and safe ESD [5]. Although it is ideal to gather experiences through practice and to undergo training with a master for skill development, it is not accessible to everyone [6]. It is necessary to develop a device that can assist unskilled individuals in performing high-level ESD with a minimum learning curve. We developed a robotic assistive traction device for flexible endoscopy. An ex vivo pilot study showed that our robot improved the safety of ESD performed by novice endoscopists [7]. Our team revised the previous prototype, naming it “ROSE” (RObot for surgical endoscope). This study compared the safety and efficiency of performing ESD between skilled and unskilled endoscopists who used ROSE in a live porcine model.
Materials and methods
Study design
This was a randomized, controlled, pilot study comparing the outcomes of robot-assisted ESD (R-ESD) in an in vivo porcine stomach. ESD was performed by a group of experienced endoscopists (n = 2) and a group of novice endoscopists who lacked ESD experience (n = 2). Experienced endoscopists had > 5 years of experience performing > 200 ESDs. In contrast, the novices had performed diagnostic endoscopy > 500 times, but only observed ESD procedures.
Prior to performing the procedure, all participants were enrolled in a learning session that comprised 30 minute detailed instructions on the ESD steps, operation of endoscopic and robotic devices, and electrosurgical units. The participants then underwent a 30-min practice session on the robotic system before R-ESD. In total, 16 experiments were performed: six R-ESDs by the experienced endoscopists and 10 by the novice endoscopists. No expert help or advice was provided during the experiment. The experiments were performed on nine 110-kg, 6-month-old female hybrid pigs. These pigs were fed a semi-fluid diet for 12 h and were fasted for 12 h before the experiments. Experiments were repeated 1–2 times for each pig.
The outcomes analyzed included the time to complete each step of R-ESD (incision, pre-dissection, grasping, and dissection), total procedure time, size of the dissected mucosa, rate of en bloc resection, and occurrence of perforations or major bleeding during the procedure. This study was approved by the Animal Test Center, College of Medicine, Korea University (Institution Review Board No. Korea 2017–0056).
Robot for surgical endoscope (ROSE)
ROSE comprises a surgical manipulator, an intuitive user interface (UI), and an actuation console to control the robotic arm (Fig. 1). The diameter of the minimalized robotic arm is 16 mm, which allows it to pass through a commercial overtube (Guardus Overtube-gastric; US Endoscopy, Mentor, OH, USA). The robotic arm and UI were attached to a standard endoscope (GIF-Q260; Olympus Medical Systems, Co., Tokyo, Japan). A motor, control board, and power supply are installed in the actuation console apparatus. The robotic arm has three degrees of freedom and grippers and can move along the circumference of the distal end of the endoscope. As the UI has the same structure and degrees of freedom as the robotic arm, it allows the robotic arm to be intuitively controlled. ROSE can be used simultaneously with commercial endoscopic surgical instruments such as an electric dual knife (Dual Electrosurgical Knife, Olympus Medical Systems, Co.).

Overview of the RObot for surgical endoscope (ROSE). A ROSE comprises of a surgical manipulator (robotic arm), an intuitive user interface (UI), and an actuation console to control the robotic arm. B Close view of surgical manipulator adapted to the endoscope and intuitive user interface. The UI has the same structure and degree of freedom as the robot arm, allowing intuitive control of the robot arm
Robot-assisted endoscopic submucosal dissection procedure
R-ESD was performed according to a clinically established pattern. The pig was positioned in the supine position, and an overtube was inserted. The endoscope attached to the robotic assistive device was passed through the overtube and inserted into the stomach. An imaginary lesion with a diameter of 5–7 cm was marked on the distal stomach with a dual knife. The mucosal layer was lifted from the muscular layer using saline solution along with indigo carmine, and a circumferential mucosal incision was made using a dual knife. The partial area of the lesion was pre-dissected to allow grasping with the robotic assistive device. After the grasping step, the mucosal flap was kept elevated by the robotic assistive device during dissection. Resection was completed at a power of 80 W on the ERBE VIO 200D (ERBE Elektromedizin GmbH, Tübingen, Germany). Major adverse events, such as bleeding or perforation, were recorded.
Results
In the experiments conducted on nine live pigs, 16 gastric lesions were resected en bloc. Six procedures were performed by two experienced endoscopists, and ten procedures were performed by two novices. Both groups succeeded in en bloc resection in all the cases. There were no significant differences in the average size of the ESD specimens in each group (Table 1). Because the sizes of the dissected samples were different, the “area per time required” was calculated and compared. The dissected area per dissection time was defined as the dissection speed (cm2/min), and the incised length per incision time was defined as the incision speed (cm2/min). The mean incision speed was significantly faster in the experienced group than in the novice group (3.25 vs. 0.64 cm2/min, P = 0.002). The experienced group showed a faster submucosal dissection speed than the novice group, without statistical significance (3.21 vs. 2.30 cm2/min; P = 0.365). There was no significant difference between the two groups in the grasp time, which is the time taken to grasp the flap with the robotic arm after pre-cutting. No perforation or major bleeding occurred during the procedure. The procedure is illustrated in Video 1.
Discussion
In Japan and Korea, ESD is generally taught using the master-apprentice model [8]. The trainee is educated systematically through observation and assistance in ESD procedures and performing supervised ESD in patients with small lesions in the distal stomach. It is difficult to apply this model in Western countries because there are not as many cases as in East Asian countries [6]. It is necessary to develop a device that can assist unskilled individuals in performing high-level ESD with a minimal learning curve [9].
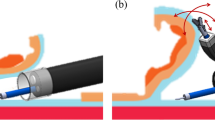
The most difficult part of the ESD procedure for novices is elevation of the flap and visualization of the submucosal dissection plane. We developed a robot-assisted system that can operate in a preexisting flexible endoscopic paradigm. Our robotic arm can be mounted simply by attaching it to the tip of a flexible endoscope. It not only provides multidirectional traction, but also provides a clear visualization of the submucosal layer (Fig. 2).

ESD procedure with ROSE. A Grasping pre-dissected lesion with the robotic arm. B Elevating the flap with the robotic arm and visualizing the submucosal dissection plane. C The dissection plane was exposed through left side traction. D As robot arm of the ROSE system has 3 degrees of freedom, it can easily continue with the dissection by providing more upward tension without having to re-grab the flap
When R-ESD was performed in this study, no significant complications such as bleeding or perforation occurred. R-ESD may potentially increase the safety of performing ESD in learners by facilitating exposure to the submucosal dissection plane. The robot can lift the mucosal flap so that the approach angle between the dual knife and the dissection plane is close to parallel, thus reducing the risk of adverse events.
The ROSE system exhibited several significant advantages. The difference in dissection speed between beginners and experienced participants was significantly reduced compared to the difference in incision speed. It seems that the beginner's dissection speed increased significantly with the help of the robot. Considering that the endoscopists only received approximately 30 min of training for operating the robot, it seems that the operation of the robot was intuitive and not difficult to control. When using the conventional ESD method, novices could not accurately visualize the dissection plane, and thus experienced difficulties in dissection. In this study, as shown in Table 1, there was no significant difference between beginners and experienced users in terms of grasp time. That is, the advantage of this device is that even beginners can grasp flaps and visualize the dissection plane without much difficulty.
Additionally, if the mucosal flap widens as the dissection proceeds, it requires a process of releasing the flap held by the robotic arm, then grabbing it from the inside of the plane, and lifting it in order to secure the dissection plane. Because the robotic arm of ROSE system has three degrees of freedom, endoscopists can easily continue dissection without re-grabbing the flap (Fig. 3A and Video 1]. The robotic arm of the ROSE system can perform roll motion along the circumference of the front end of the endoscope; hence, it shows good adaptability to the location of the lesion (Fig. 3B).

Surgical manipulator of ROSE. A Three degrees of freedom that can be operated on ROSE. B Workspace of the surgical manipulator. It can move along the circumference of the front end of the endoscope to cover a wide range
This study had some limitations. Comparison between conventional and robot-assisted methods was not performed in either of the endoscopist groups. However, the main end point of this study was to evaluate whether a person without sufficient ESD training could perform ESD as safely and quickly as an expert group with the help of robotic devices. In our previous study using this robotic model's prototype, the experienced group did not show a significant difference in procedure speed or safety between the conventional and robot-assisted methods [7]. On the other hand, when the robot-assisted method was used in the novices, the procedure speed and safety were significantly improved compared to those of the conventional method [7]. We started this experiment on the premise that it is the beginner’s group who would receive greater help from a robotic device. We further improved the robotic device so that beginners could use it easily and intuitively. In this feasibility study, rather than a comparison with the conventional method, the focus was on how a beginner could perform ESD skillfully as an expert using our new robotic device.
There was a limitation of scope movement due to the robotic device. The scope movement was relatively restricted after the robot grasped the flap, as this robot was attached to the scope. To improve this problem, we upgraded the robot arm to move smoothly from side to side through roll motion [Video 1]. If tension is applied by roll motion in consideration of the dissection direction, ESD can be performed more efficiently. Making improvement in roll motion in robot and adequate endoscopist training for robot ESD are further required. Owing to the size of the robotic arm, dissection was performed, while the distance between the endoscope and the dissection plane was relatively large. Performing ESD in a narrow space, such as the duodenum or retroflexion of the endoscope with a robot installed, seems to be challenging. The robotic arm should be further miniaturized.
In this study, the experiment was performed in the distal stomach, where ESD was relatively easy. However, in a more difficult location, it could be more challenging to control the robot stably. Therefore, the robot may need further improvements, and future ESD experiments should be conducted in diverse locations with more samples.
In conclusion, ROSE can provide simple, effective, and safe multidirectional traction and countertraction during ESD. While performing robotic ESD, experienced endoscopists expressed satisfaction, and novices could perform ESD safely and efficiently. We expect our device to help trainees perform ESD in places where ESD education is difficult to obtain. The device must be made smaller, and its safety and efficacy in humans should be assessed in future studies.
References
Chiu PW (2014) Novel endoscopic therapeutics for early gastric cancer. Clin Gastroenterol Hepatol 12:120–125
Watanabe K, Ogata S, Kawazoe S, Watanabe K, Koyama T, Kajiwara T, Shimoda Y, Takase Y, Irie K, Mizuguchi M, Tsunada S, Iwakiri R, Fujimoto K (2006) Clinical outcomes of EMR for gastric tumors: historical pilot evaluation between endoscopic submucosal dissection and conventional mucosal resection. Gastrointest Endosc 63:776–782
Kato M, Gromski M, Jung Y, Chuttani R, Matthes K (2013) The learning curve for endoscopic submucosal dissection in an established experimental setting. Surg Endosc 27:154–161
Yamamoto K, Michida T, Nishida T, Hayashi S, Naito M, Ito T (2015) Colorectal endoscopic submucosal dissection: Recent technical advances for safe and successful procedures. World J Gastrointest Endosc 7:1114–1128
Ho KY, Phee SJ, Shabbir A, Low SC, Huynh VA, Kencana AP, Yang K, Lomanto D, So BY, Wong YY, Chung SC (2010) Endoscopic submucosal dissection of gastric lesions by using a master and slave transluminal endoscopic robot (MASTER). Gastrointest Endosc 72:593–599
Draganov PV, Coman RM, Gotoda T (2014) Training for complex endoscopic procedures: how to incorporate endoscopic submucosal dissection skills in the west? Expert Rev Gastroenterol Hepatol 8:119–121
Kim BG, Choi HS, Park SH, Hong JH, Lee JM, Kim SH, Chun HJ, Hong D, Keum B (2019) A pilot study of endoscopic submucosal dissection using an endoscopic assistive robot in a porcine stomach model. Gut Liver 13:402–408
Draganov PV, Wang AY, Othman MO, Fukami N (2019) AGA institute clinical practice update: endoscopic submucosal dissection in the United States. Clin Gastroenterol Hepatol 17(16–25):e11
Chiu PW, Phee SJ, Bhandari P, Sumiyama K, Ohya T, Wong J, Poon CC, Tajiri H, Nakajima K, Ho KY (2015) Enhancing proficiency in performing endoscopic submucosal dissection (ESD) by using a prototype robotic endoscope. Endosc Int Open 3:E439–442
Funding
This work was supported by the National Research Foundation of Korea (NRF) Grant funded by the Korea government (MSIT) (Grant No. NRF-2020R1A2C4002621). This study was supported by a Grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (Grant No. HI14C3477).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf. Sang Hyun Kim, Byung Gon Kim, Hyuk Soon Choi, Daehie Hong, Se Hyun Jang, Kihun Hong, Jin Woo Choi, Seung Han Kim, Jae Min Lee, Eun Sun Kim, Bora Keum, Yoon Tae Jeen, Hong Sik Lee, and Hoon Jai Chun have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 Video 1. Movement of the robotic arm and endoscopic submucosal dissection with RObot for surgical endoscope (AVI 803589 kb)
Rights and permissions
About this article

Cite this article
Kim, S.H., Kim, B.G., Choi, H.S. et al. Endoscopic submucosal dissection using a detachable assistant robot: a comparative in vivo feasibility study (with video). Surg Endosc 35, 5836–5841 (2021). https://doi.org/10.1007/s00464-021-08510-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-021-08510-1