
Abstract
Background and aims
EUS-guided choledochoduodenostomy (EUS-CDS) is an effective option for biliary drainage in malignant biliary obstruction. Lumen apposing metal stents (LAMS) are increasingly been used for EUS-CDS. It is unknown how LAMS compare to tubular self-expandable metal stents (SEMS) for EUS-CDS. Our aim is to compare the clinical outcomes of LAMS versus SEMS for EUS-CDS.
Patients and methods
Single-center retrospective cohort study of consecutive patients with unresectable malignant biliary obstruction who underwent EUS-CDS after failed ERCP for initial biliary drainage between 2011 and 2019. Clinical outcomes were compared between patients who had conventional covered SEMS and LAMS placed for EUS-CDS. Outcome measures included unplanned procedural events, technical success, clinical success, adverse events and reinterventions. Survival was analyzed by the Kaplan–Meier method.
Results
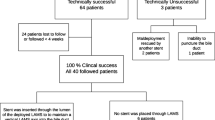
During the study period 57 patients met inclusion criteria (37 LAMS, 20 SEMS). All EUS-CDS were technically successful (LAMS group 95% CI 90.3–100%, SEMS group 95% CI 83.2–100%). There were no differences between groups in unplanned procedural events (4 LAMS deployment issues, 2 mild bleeding in SEMS group; 10 vs 10.8%), clinical success (37/37 [100%] vs 19/20 [95%]), and short-term adverse events (5/37 [13.5%] vs 4/20 [20%], p = 0.71). Complete follow-up data were available in 41 patients for a mean of 376 ± 145 days. Endoscopic reintervention was required for duodenal stent placement (n = 9) or biliary stent dysfunction (n = 4), with no difference between LAMS and SEMS group (6/37 [16.2%] vs 7/20 [35%]). There were no differences in overall survival between both groups.
Conclusions
EUS-guided choledochoduodenostomy after failed ERCP has equally high technical and clinical success rates with either LAMS or SEMS in patients with malignant biliary obstruction. No differences in adverse events, reinterventions and survival were seen with either type of stent. The cost-effectiveness of LAMS vs SEMS for EUS-guided choledochoduodenostomy remains to be proven.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Malignant tumors involving the bile duct typically present with obstructive jaundice. Persistent obstructive jaundice impairs patient quality of life and may potentially lead to serious complications, including liver and renal failure [1]. Although surgical resection is the only curative treatment, a minority of patients with pancreatobiliary malignancies undergo resection, because tumor stage or patient comorbidities often preclude surgery. In most cases of malignant biliary obstruction, palliative biliary drainage is the required treatment approach. Endoscopic retrograde cholangiopancreatography (ERCP) is well established as the preferred non-operative modality for biliary drainage because of a high technical success rate and acceptable adverse event rate [2].
When ERCP cannulation fails or when retrograde endoscopic biliary access is precluded by duodenal strictures or surgically altered anatomy, percutaneous transhepatic biliary drainage (PTBD) or surgical bypass are the traditional alternative drainage methods. However, PTBD and bypass surgery are both associated with marked adverse event rates. Over the last three decades, the palliative role of surgery and PTBD in malignant biliary obstruction has declined in favor of less invasive endoscopic approaches. In addition to ERCP, endoscopic ultrasound-guided biliary drainage (EUS-BD) has emerged as an effective modality for biliary drainage [3, 4]. EUS-BD has increasingly been performed as an alternative to PTBD in patients with unresectable malignant biliary obstruction and failed ERCP [3]. Technical and clinical success rates over 90% have been reported for EUS-BD [5]. However, the adverse event rate is significant (26%) and there is a small but definite mortality risk (0.4%) [5]. This high adverse event rate is thought to reflect the learning curve of EUS-BD, the heterogeneity of techniques used, and the lack of dedicated accessories. EUS-BD includes several approaches involving intrahepatic or extrahepatic biliary access combined with transmural or transpapillary stent placement [6]. EUS-guided choledochoduodenostomy (EUS-CDS) is among the most commonly taken EUS-BD approaches for distal malignant biliary obstruction.
In the last few years, efforts to facilitate EUS-BD and to decrease the risk of adverse events have led to the development of dedicated accessories. A lumen apposing metal stent (LAMS) specifically designed to create anastomoses to the gastrointestinal tract has become available for EUS-CDS, following its widespread dissemination for EUS-guided drainage of pancreatic collections and the gallbladder. LAMS have largely replaced other stent choices for EUS-guided gallbladder drainage in patients with acute cholecystitis unfit for surgery [7, 8]. Recent reports of EUS-CDS using a dedicated biliary LAMS show promising results [9,10,11,12,13,14] Single-step (free-hand) or single-exchange (over-the-wire) LAMS insertion is possible using an electrocautery enhanced delivery system, which appears to simplify EUS-CDS [11]. EUS-CDS with traditional tubular self-expandable metal stents (SEMS) however, involves multi-step dilation of the puncture tract. Even if LAMS insertion for EUS-CDS appears to be simpler than traditional SEMS insertion, there remain concerns over the long-term patency of LAMS placed for EUS-CDS. The overall reported adverse event rate of EUS-CDS with LAMS may be as high as 37% in studies with longer follow-up [14]. To date, no comparative study between LAMS and conventional tubular SEMS for EUS-CDS is available. In this study we aimed to compare the safety and efficacy or LAMS versus SEMS for EUS-CDS in unresectable distal malignant biliary obstruction after failed ERCP.
Patients and methods
This is a single-center retrospective cohort study comparing the safety and efficacy of LAMS versus SEMS for EUS-CDS in the management of unresectable distal malignant biliary obstruction. The project was approved by the Institutional Review Board in February 2020. Dual informed consent for ERCP and EUS-BD was routinely obtained from patients with biliary obstruction or their families in our Unit. All authors had access to the study data and have reviewed and approved the final manuscript.
Patients
Patients were identified from a prospectively maintained single-center interventional endoscopy database. Consecutive patients who underwent EUS-CDS between January 2011 and January 2019 were identified. Patients with unresectable distal malignant biliary obstruction who underwent EUS-CDS with a metal stent (SEMS or LAMS) for biliary drainage because of previous failed ERCP were included for analysis. Patients with unresectable distal malignant biliary obstruction who underwent EUS-CDS because of stent dysfunction following prior ERCP with stent placement were excluded from the analysis.
Procedures
All procedures were performed by experienced endoscopists in an endoscopy suite with a therapeutic echoendoscope. All patients were sedated using endoscopist-directed intravenous administration of midazolam and propofol, unless critically ill. No patient received prophylactic antibiotics in our cohort. For the technique of EUS-CDS, the echoendoscope was passed into the duodenum to visualize common bile duct. A 19-gauge needle (Expect; Boston Scientific, Marlborough, Mass) preloaded with water-soluble contrast material was used to puncture the common bile duct and entry was confirmed by contrast material injection. The needle was flushed with saline solution, and a 0.035-inch or 0.025-inch, 450-cm long guidewire was passed into the common bile duct.
Commercially available fully covered SEMS either with (BCS Hanarostent, M.I.Tech, Seoul, Korea) or without (Wallflex, Boston Scientific, Marlborough, Mass, USA) internal antimigration flaps (Fig. 1) or LAMS (Axios and Hot Axios, Boston Scientific, Marlborough, Mass, USA) (Fig. 2) were used. Stents were inserted over-the-guidewire into the common bile duct and deployed transmurally within the duodenum under combined EUS, fluoroscopic and endoscopic visualization, as previously reported. The free-hand LAMS insertion technique was not routinely used in this cohort. Coaxial double pigtails stents were placed inside the SEMS or LAMS for additional anchorage at the discretion of the endoscopist. EUS-BD with SEMS was introduced in our center in September 2003 whereas LAMS was first placed for EUS-CDS in March 2012. There was a gradual shift from SEMS towards increased LAMS use, with no strict criteria for one stent type or another. However, technical factors, such a needle puncture within 2-cm of the hepatic duct confluence, or a guidewire taking a downward course, favored the choice of LAMS over SEMS. Conversely, when the common bile duct diameter was less than 12-mm, SEMS were preferred over LAMS for EUS-CDS.

EUS-guided choledocoduodenostomy using self-expandable metal stent. A Fluoroscopic view. B Final endoscopic appearance of stent deployed in the duodenal bulb

EUS-guided choledocoduodenostomy using lumen apposing metal stent. A Fluoroscopic view. B Final endoscopic appearance of lumen apposing metal stent deployed in the duodenum
Outcome measures
The main outcome measures were the technical success, clinical success and short-term adverse event rates. Our secondary outcome measures were reintervention rates and patient survival.
Definitions
Technical success was defined as the correct transduodenal stent placement, with both ends of the stent (internal intraductal and external intraduodenal) properly placed and an adequate bile outflow verified by fluoroscopy and/or endoscopy.
Clinical success was defined as a 50% decrease in bilirubin from the last available pre-procedure value within 1 week (± 2 days) following EUS-CDS or a serum bilirubin below 2 mg/dL within one month.
Unplanned procedural event was defined according to Teoh et al. [15] as any deviation in planned procedural steps, including but not limited to guidewire dislodgement and stent misdeployment, regardless of its impact on technical success or post-procedural adverse events.
Short-term adverse event was defined as any adverse event potentially related to the procedure within the first two weeks following EUS-CDS. Adverse events and their severity were defined and graded according to the ASGE lexicon [16].
Reintervention was defined as any therapeutic percutaneous or endoscopic procedure performed because of biliary or gastric outlet obstruction, bleeding, stent migration, regardless of the cause, whether underlying disease-related or stent-related.
Follow-up
Follow-up visits were performed at the discretion of the treating physician, with periodic clinic visits, laboratory analysis and imaging, as necessary.
Those patients who were followed-up until death or who had any clinical follow-up in the 4 months prior to December 2019 were defined as complete follow-up. Patients who did not meet either of these two criteria were defined as lost to follow-up.
Data retrieval
Data on baseline demographics, diagnosis, endoscopic procedures and technical details were retrieved from the prospective endoscopy database maintained at our center. Post-procedural follow-up data were retrospectively obtained from electronic medical records, including endoscopic and imaging procedures. Data from patients admitted to and cared for at outside medical centers who continued follow-up in these centers, were obtained by transfer of medical records, shared healthcare network electronic medical records, direct discussion with the attending physician and/or telephone interview with the patient. The available data were censored in December 2019.
Statistical analysis
Statistical analysis was performed using Stata (StataCorp. 2013. College Station, Texas). Categorical variables were described as percentages, continuous variables with normal distribution as mean and standard deviation, and continuous variables with non-normal distributions as medians and interquartile range.
Pearson's χ2 test or Fisher's exact test (in case the expected frequencies in the contingency tables are less than 5) were applied to assess differences between the categorical variables.
Results
Patients included and baseline characteristics
Between January 2011 and January 2019, 57 patients (49.1% female, median age 81.4 years), with malignant biliary obstruction without an indwelling biliary stent and incomplete or failed previous ERCP underwent EUS-CDS in our Unit. The cause for ERCP failure was duodenal obstruction making the papilla inaccessible or significantly hampering cannulation of the papilla in 19 (33.3%), malignant involvement with distortion of the papilla in 16 (28.1%), and failed cannulation with (n = 15; 26.3%) or without (n = 7; 12.3%) pre-cut in the remaining.. Pancreatic adenocarcinoma was the most common underlying diagnosis (80.7%). Based on the American Society of Anesthesiology (ASA) classification 54.4% (31/57) of patients were ASA grades III or IV. Patient demographic data are shown in Table 1.
Procedure description
EUS-CDS was performed during the same session of failed ERCP in all cases. Table 2 shows procedural details. All EUS-CDS (100%) were technically successful (LAMS group 95% CI 90.3–100%; SEMS group 95% CI 83.2–100%). A 10-mm diameter and 60-mm long fully covered SEMS was used in 17/20 patients. Stent sizes were not registered in the remaining three. SEMS with antimigration flaps were employed in 11 (55%) patients, and SEMS without antimigration flaps in 9 (45%). LAMS were employed in 37 cases, Hot Axios in 30 cases and (cold) Axios in the remaining 7, 5 of which were reported in a previous pilot study [9]. Coaxial double pigtail stents were placed through 22 of the 37 LAMS and through 13 of the 20 SEMS. In 19 patients with concurrent symptomatic gastric outlet obstruction, different types of uncovered duodenal metal stents were placed during the same hospital admission, either within the same session, or within 72-h of the EUS-CDS procedure.
Unplanned procedural events were registered in 6 cases. In two cases of SEMS insertion, self-limited mild bleeding was observed which required no treatment in one case and requiring adrenaline injection in another. LAMS-related unplanned procedural events were registered in 4 cases, including 2 distal flange dislodgements and 2 misdeployments. All these 4 LAMS-related unplanned procedural events were salvaged by insertion of a coaxial stent.
In the first two weeks after EUS-CDS, 9 patients (15.8%) had adverse events, 5 (13.5%; 95% CI 46.7–29.5%) in the LAMS group and 4 (20%; 95% CI 5.7–43.7%) in the SEMS group (p = 0.71), with no significant differences between both groups. None of the patients presented post-procedure pancreatitis. Four patients, 2 in each group, developed mild cholangitis or cholecystitis. Two patients with LAMS and 1 patient with SEMS presented bile leakage requiring surgical revision and drainage placement. Thus, the incidence of severe short-term adverse events was 5.3% (3/57) overall.
Clinical success was achieved in 56 of these 57 patients (98.2% for the entire cohort), with no differences between patients with LAMS and SEMS (100% vs 95%, p = n.s).
Follow up
Forty-one patients had complete follow up. Patients with complete follow-up were followed for a mean of 376 ± 145 days. At the end of follow up, 6 patients with SEMS and 16 patients with LAMS had died from their underlying disease. One patient with SEMS and 5 with LAMS completed the follow up period without adverse events and were still alive at the end of data collection. 13 patients required reintervention during this period. There were no differences in overall survival between both groups.
Reintervention was required in 6 patients (16.2%; 95% CI 6.2–32%) in the LAMS group and 7 patients (35%; 95%CI 8.7–49.1%) in the SEMS group. All 13 patients were endoscopically managed. Five out of six LAMS patients who required reintervention and 4/7 SEMS patients developed symptomatic gastric outlet obstruction requiring duodenal stent placement. Additionally, one LAMS and three SEMS patients developed EUS-CDS dysfunction. The dysfunctional LAMS was managed by coaxial pig tail placement, as previously reported [17]. Two dysfunctional SEMS were converted to transpapillary stent placement by EUS-CDS stent removal and through-the-fistula antegrade guidewire passage (two-stage rendezvous). Obstruction due to an adherent clot secondary to delayed bleeding was managed by coaxial pigtail insertion in the remaining case of EUS-CDS with SEMS dysfunction. There were no differences in reintervention rates between LAMS and SEMS groups.
Discussion
We retrospectively evaluated a large cohort of patients with distal malignant biliary obstruction and failed initial ERCP who underwent EUS-CDS, using SEMS or LAMS for biliary drainage. We found that stent placement was technically successful in all cases and that this closely translated into clinical success (jaundice resolution). Adverse events within two weeks of EUS-CDS, however, were not negligible at 15.8%. Reinterventions were required in 34% of patients with complete follow-up, largely due to new-onset gastric outlet obstruction (n = 9), but also because of EUS-CDS dysfunction (n = 4). We failed to find any evidence of the superiority of LAMS over SEMS for EUS-CDS in terms of technical success, clinical success, and adverse events. Conversely, the need for reintervention was not higher in LAMS versus SEMS, particularly reinterventions triggered by stent dysfunction.
Our data are consistent with previous studies on EUS-CDS reporting high technical and clinical success rates with either LAMS (Table 3) [9,10,11,12,13,14] or SEMS (Table 4) [18,19,20,21,22,23,24,25]. Despite the assumed easier stent placement of LAMS compared to SEMS or their potential for longer stent patency, this did not translate into any improved measurable clinical outcomes in our study. Given that the cost of LAMS is two to three times higher than that of SEMS, this lack of proven superiority raises concerns. The question of the relative performance of LAMS versus SEMS for EUS-CDS warrants further scrutiny, as EUS-BD is likely to play a greater role in the palliation of malignant biliary obstruction in the future. Three recent randomized trials comparing EUS-BD using SEMS to ERCP found similar technical and clinical success, with improved post-procedure adverse events and patient quality of life in the EUS-BD group [19, 22, 26]. In all these three randomized trials, EUS-CDS was performed with different types of covered SEMS.
There are several limitations to our study. As a retrospective study conducted at a single high-volume center over a relatively long timespan, inherent biases are present and lack of generalizability is a strong possibility. EUS-CDS had been performed with SEMS at our center for more than a decade before dedicated biliary LAMS became available. Thus, biliary LAMS may have greater impact on EUS-CDS outcomes in practice settings where endoscopists are less familiar with EUS-CDS with SEMS. Furthermore, no uniform type of LAMS (cautery enabled or not) or placement technique (over-the-wire or free-hand) was used throughout the study period by the two operators involved. Earlier versions of the Axios stent may have been more prone to unplanned procedural events than subsequent, improved versions. The relative merits of each stent type in different patient subsets based on the degree of common bile duct dilation or other factors could not be analyzed. A significant proportion of patients referred from outside institutions lacked follow-up data, again introducing bias.
After EUS-CDS reintervention was necessary in 13 of the 38 patients with complete follow-up, mostly for duodenal stent placement (24%) and to a lesser extent for recurrent biliary obstruction (10%) Kunda et al. reported a reintervention rate of 9.3% in a 54 patients case series with LAMS EUS-CDS [9], which is comparable to our results. However, 75% of cases or recurrent biliary obstruction in our cohort occurred in SEMS patients. The placement of coaxial pigtails in 45/57 EUS-CDS might have contributed to prevent cholangitis caused by LAMS angulation in our series.
In conclusion, this is the first cohort of EUS-CDS in patients with unresectable distal malignant biliary obstruction and failed ERCP comparing clinical outcomes between SEMS and LAMS. Our study suggests equivalent outcomes for EUS-CDS for biliary drainage in patients with either type of stent in terms of technical or clinical success, unplanned procedural events, adverse events and reinterventions. As it has been the case with other interventional EUS procedures such as drainage of walled-off pancreatic necrosis, the superiority of LAMS over other type of stents has been difficult to prove [27]. Advantages of SEMS over LAMS include lower cost and their ability to be placed via CDS into the CBD even with lesser degrees of dilation. Advantages of LAMS over SEMS include one-step insertion with the attendant possibility -yet unproven- of increased procedural safety. Long-term outcomes with either type of stent also warrant further scrutiny, as changing management algorithms of malignant biliary obstruction increasingly tend to consider EUS-CDS for patients with longer life expectancy.
References
Chu D, Adler DG (2010) Malignant biliary tract obstruction: evaluation and therapy. JNCCN J Natl Compr Cancer Netw 8(9):1033–1044
Baron TH, Grimm IS, Swanstrom LL (2015) Interventional approaches to gallbladder disease. N Engl J Med 373(4):357–365
Sharaiha RZ, Khan MA, Kamal F, Tyberg A, Tombazzi CR, Ali B, Tombazzi C, Kahaleh M (2017) Efficacy and safety of EUS-guided biliary drainage in comparison with percutaneous biliary drainage when ERCP fails: a systematic review and meta-analysis. Gastrointest Endosc 85(5):904–914. https://doi.org/10.1016/j.gie.2016.12.023
Sharaiha RZ, Kumta NA, Desai AP, DeFilippis EM, Gabr M, Sarkisian AM, Salgado S, Millman J, Benvenuto A, Cohen M, Tyberg A, Gaidhane M, Kahaleh M (2016) Endoscopic ultrasound-guided biliary drainage versus percutaneous transhepatic biliary drainage: predictors of successful outcome in patients who fail endoscopic retrograde cholangiopancreatography. Surg Endosc 30(12):5500–5505
Fabbri C, Luigiano C, Lisotti A, Cennamo V, Virgilio C, Caletti G, Fusaroli P (2014) Endoscopic ultrasound-guided treatments: are we getting evidence based—a systematic review. World J Gastroenterol 20(26):8424–8448
Gupta K, Perez-Miranda M, Kahaleh MK, Artifon ELA, Itoi T, Freeman ML, De-Serna C, Sauer B, Giovannini M (2014) Endoscopic ultrasound-assisted bile duct access and drainage: multicenter, long-term analysis of approach, outcomes, and complications of a technique in evolution. J Clin Gastroenterol 48(1):80–87
Walter D, Will U, Sanchez-Yague A, Brenke D, Brenke D, Hampe J, Wollny H, López-Jamar JME, Jechart G, Vilmann P, Gornals JB, Ullrich S, Fähndrich M, De Tejada AH, Junquera F, Gonzalez-Huix F, Siersema PD, Vleggaar FP (2015) A novel lumen-apposing metal stent for endoscopic ultrasound-guided drainage of pancreatic fluid collections: a prospective cohort study. Endoscopy 47(1):63–67
Teoh AYB, Binmoeller KF, Lau JYW (2014) Single-step EUS-guided puncture and delivery of a lumen-apposing stent for gallbladder drainage using a novel cautery-tipped stent delivery system. Gastrointest Endosc 80(6):1171
Kunda R, Pérez-Miranda M, Will U, Ullrich S, Brenke D, Dollhopf M, Meier M, Larghi A (2016) EUS-guided choledochoduodenostomy for malignant distal biliary obstruction using a lumen-apposing fully covered metal stent after failed ERCP. Surg Endosc 30(11):5002–5008
Anderloni A, Fugazza A, Troncone E, Auriemma F, Carrara S, Semeraro R, Maselli R, Di Leo M, D’Amico F, Sethi A, Repici A (2019) Single-stage EUS-guided choledochoduodenostomy using a lumen-apposing metal stent for malignant distal biliary obstruction. Gastrointest Endosc 89(1):69–76. https://doi.org/10.1016/j.gie.2018.08.047
Jacques J, Privat J, Pinard F, Fumex F, Chaput U, Valats JC, Cholet F, Jezequel J, Grandval P, Legros R, Lepetit H, Albouys J, Napoleon B (2020) EUS-guided choledochoduodenostomy by use of electrocautery-enhanced lumen-apposing metal stents: a French multicenter study after implementation of the technique (with video). Gastrointest Endosc. https://doi.org/10.1016/j.gie.2020.01.055
Jacques J, Privat J, Pinard F, Fumex F, Valats JC, Chaoui A, Cholet F, Godard B, Grandval P, Legros R, Kerever S, Napoleon B (2019) Endoscopic ultrasound-guided choledochoduodenostomy with electrocautery-enhanced lumen-apposing stents: a retrospective analysis. Endoscopy 51(6):540–547
El Chafic AH, Shah JN, Hamerski C, Binmoeller KF, Irani S, James TW, Baron TH, Nieto J, Romero RV, Evans JA, Kahaleh M (2019) EUS-guided choledochoduodenostomy for distal malignant biliary obstruction using electrocautery-enhanced lumen-apposing metal stents: first US, multicenter experience. Dig Dis Sci 64(11):3321–3327. https://doi.org/10.1007/s10620-019-05688-2
Tsuchiya T, Teoh AYB, Itoi T, Yamao K, Hara K, Nakai Y, Isayama H, Kitano M (2018) Long-term outcomes of EUS-guided choledochoduodenostomy using a lumen-apposing metal stent for malignant distal biliary obstruction: a prospective multicenter study. Gastrointest Endosc 87(4):1138–1146. https://doi.org/10.1016/j.gie.2017.08.017
Teoh AY, Perez-Miranda M, Kunda R, Lee SS, Irani S, Yeaton P, Sun S, Baron TH, Moon JH, Holt B, Khor CJL, Rerknimitr R, Bapaye A, Chan SM, Choi HJ, James TW, Kongkam P, Lee YN, Parekh P, Ridtitid W, Serna-Higuera C, Tan DMY, Torres-Yuste R (2019) Outcomes of an international multicenter registry on EUS-guided gallbladder drainage in patients at high risk for cholecystectomy. Endosc Int Open 7(8):E964–E973
Cotton PB, Eisen GM, Aabakken L, Baron TH, Hutter MM, Jacobson BC, Mergener K, Nemcek A, Petersen BT, Petrini JL, Pike IM, Rabeneck L, Romagnuolo J, Vargo JJ (2010) A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc 71(3):446–454
Mosquera-Klinger G, De-La-Serna-Higuera C, Pérez-Miranda M (2019) Endoscopic sump syndrome secondary to EUS-guided choledochoduodenostomy with a lumen-apposing metal stent. Rev Esp Enfermedades Dig 111(1):74–76
Khashab M, El Zein M, Sharzehi K, Marson F, Haluszka O, Small A, Nakai Y, Park DY, Kunda R, Teoh AY, Peñas I, Perez-Miranda M, Kumbhari V, Van der Merwe S, Artifon EL, Ross AS (2016) EUS-guided biliary drainage or enteroscopy-assisted ERCP in patients with surgical anatomy and biliary obstruction: an international comparative study. Endosc Int Open 4(12):E1322–E1327
Bang JY, Navaneethan U, Hasan M, Hawes R, Varadarajulu S (2018) Stent placement by EUS or ERCP for primary biliary decompression in pancreatic cancer: a randomized trial (with videos). Gastrointest Endosc 88(1):9–17
Paik WH, Lee TH, Park DH, Choi JH, Kim SO, Jang S, Kim DU, Shim JH, Song TJ, Lee SS, Seo DW, Lee SK, Kimet MH (2018) EUS-guided biliary drainage versus ERCP for the primary palliation of malignant biliary obstruction: a multicenter randomized clinical trial. Am J Gastroenterol 113(7):987–997. https://doi.org/10.1038/s41395-018-0122-8
Iwashita T, Doi S, Yasuda I (2014) Endoscopic ultrasound-guided biliary drainage: a review. Clin J Gastroenterol 7(2):94–102
Dhir V, Itoi T, Khashab MA, Park DH, Yuen Bun Teoh A, Attam R, Messallam A, Varadarajulu S, Maydeoet A (2015) Multicenter comparative evaluation of endoscopic placement of expandable metal stents for malignant distal common bile duct obstruction by ERCP or EUS-guided approach. Gastrointest Endosc 81(4):913–923
Artifon ELA, Marson FP, Gaidhane M, Kahaleh M, Otoch JP (2015) Hepaticogastrostomy or choledochoduodenostomy for distal malignant biliary obstruction after failed ERCP: is there any difference? Gastrointest Endosc 81(4):950–959
Poincloux L, Rouquette O, Buc E, Privat J, Pezet D, Dapoigny M, Bommelaer G, Abergelet A (2015) Endoscopic ultrasound-guided biliary drainage after failed ERCP: cumulative experience of 101 procedures at a single center. Endoscopy 47(9):794–801
Cho DH, Lee SS, Oh D, Song TJ, Park DH, Seo DW, Lee SK, Kimet MH (2017) Long-term outcomes of a newly developed hybrid metal stent for EUS-guided biliary drainage (with videos). Gastrointest Endosc 85(5):1067–1075
Park JK, Woo YS, Noh DH, Il YJ, Bae SY, Yun HS, Lee JK, Lee KT, Lee KH (2018) Efficacy of EUS-guided and ERCP-guided biliary drainage for malignant biliary obstruction: prospective randomized controlled study. Gastrointest Endosc 88(2):277–282. https://doi.org/10.1016/j.gie.2018.03.015
Mohan B, Jayaraj M, Asokkumar R, Shakhatreh M, Pahal P, Ponnada S, Navaneethan U, Adler DG (2019) Lumen apposing metal stents in drainage of pancreatic walled-off necrosis, are they any better than plastic stents? A systematic review and meta-analysis of studies published since the revised Atlanta classification of pancreatic fluid collections. Endosc Ultrasound 8(2):82–90
Funding
No financial support was needed to conduct this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Manuel Perez-Miranda is a consultant for Boston Scientific and M.I.Tech and has lectured for Boston Scientific and Olympus. Dra. Marina de Benito Sanz, Dr. Rodrigo Nájera Muñoz, Dr. Carlos de la Serna, Dr. Esteban Fuentes-Valenzuela, Dr. Ignacio Fanjul, Dr. Carlos Chavarría, Dr. Francisco Javier Garcia-Alonso, Dr. Ramón Sanchez-Ocana, Dra. Ana Yaiza Carbajo and Dr. Sergio Bazaga have no potential conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
de Benito Sanz, M., Nájera-Muñoz, R., de la Serna-Higuera, C. et al. Lumen apposing metal stents versus tubular self-expandable metal stents for endoscopic ultrasound-guided choledochoduodenostomy in malignant biliary obstruction. Surg Endosc 35, 6754–6762 (2021). https://doi.org/10.1007/s00464-020-08179-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-08179-y