
Abstract
Background
To comprehensively evaluate the efficacy and safety of Retzius sparing (RS) for men undergoing robot-assisted laparoscopic prostatectomy (RARP).
Methods
We searched four electronic databases and reference lists of relevant studies for eligible research published before March 11, 2019. After quality assessment, eligible studies were synthesized for relevant outcomes, including positive surgical margin (PSM), continence, incontinence, complication, console time, and hospital stay.
Results
Two randomized clinical trials and four observational studies were included in this study. Quantitative syntheses revealed significantly higher PSM rates in RS-RARP compared with conventional RARP (c-RARP) (odds ratio [OR] 1.68, p = 0.02). Furthermore, we found significantly higher PSM rates at the anterior site in RS-RARP compared with c-RARP (OR 4.34, p = 0.03) and significantly lower incontinence rates in RS-RARP in the first month (OR 0.30, p < 0.001) and 12th month (OR 0.25, p < 0.001).
Conclusions
Our syntheses revealed higher PSM rates in the RS-RARP group, especially in the anterior aspect. However, RS-RARP had superior functional outcome of urinary continence and lower console time than did c-RARP with equivalent complication rates. Thus, we suggest that operators pay more attention to making clear surgical margins if the lesion is in anterior prostate when performing RS-RARP.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Prostate cancer is the second most frequently diagnosed cancer in men worldwide, accounting for 15% of all cancers [1]. In men with clinically localized prostate cancer, treatment varies with life expectancy and risk stratification, including active surveillance, external beam radiation therapy, whole gland ablation, and radical prostatectomy [2]. Radical prostatectomy is one of the curative treatments for men with organ-confined prostate cancer.
The technical development of radical prostatectomy involved laparoscopic radical prostatectomy and robot-assisted radical prostatectomy (RARP). Laparoscopic radical prostatectomy was initially reported in 1992 [3] and modified in 2000 [4]. Subsequently, laparoscopic radical prostatectomy became widespread because it causes less blood loss and requires shorter hospital stays and catheterization durations compared with open radical prostatectomy [5]. After laparoscopy, a new telerobotic surgical system with magnified three-dimensional imaging and articulating instruments was developed and applied to assist laparoscopic radical prostatectomy. The fine movement in the limited retropubic space led to RARP being widely adopted. Conventional RARP (c-RARP) was introduced by Abbou [6] and modified by Menon [7]. In c-RARP, the bladder and prostate are incised and mobilized through dissection of the prevesical space. Postoperative morbidity is a major concern for patients with prostate cancer because it compromises quality of life and makes patients hesitate to undergo operations. Several possible negative consequences of c-RARP exist, such as urinary incontinence, erectile dysfunction, and biochemical recurrence of prostate-specific antigen. Many surgical modifications in the technique attempt to enhance postoperative functional outcomes without compromising cancer control [8].
Retzius-sparing RARP (RS-RARP) was developed in 2010 [9]. In the first report on RS-RARP, 90% of 200 patients were continent within 7 days after catheter removal [10]. Based on the current knowledge of surgical anatomy, the features of this surgery are that it preserves the endopelvic fascia, arcus tendineus, neurovascular bundle, deep dorsal vein plexus, and puboprostatic ligament, which are critical to the mechanism of urinary continence [11]. Recently, other studies have also reported better outcome in urinary continence with RS-RARP [12,13,14,15,16].
The oncological outcomes of RS-RARP remain controversial. For instance, the positive surgical margins (PSMs) of RS-RARP should be a concern despite its better continence [17]. Higher stages of prostate cancer or learning curves may lead to PSMs [15]. Although many studies have reported the benefits of urinary continence after RS-RARP, the effectiveness and safety of the procedure compared with c-RARP in terms of functional and oncological outcomes remain unclear. Therefore, this study aimed to systematically review currently available evidence to compare the therapeutic effectiveness and efficacy of RS-RARP with c-RARP in men with clinically localized prostate cancer.
Materials and methods
For conducting and reporting this systematic review, we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [18]. Our research team included urologists and an experienced researcher in systematic reviews and meta-analyses [19,20,21,22]. The experienced researcher had also participated in research studies on urology and surgical oncology [23, 24]. Because this meta-analysis synthesized data from published articles, this study was exempt from institutional review board approval.
Data sources and search strategy
This study searched for evidence in electronic databases and by hand search. The electronic databases were Embase, PubMed (including MEDLINE), Scopus, and Web of Science. We formulated the primary search strategy in PubMed using the relevant terms “prostatectomy,” “prostate cancer,” and “Retzius” (including “Bocciardi”) in free-text and medical subject heading. The Boolean operator “OR” was used to combine keywords with similar concepts, whereas the Boolean operator “AND” was used to connect keywords with different concepts. The search strategy was designed without any filter for publication data or language restriction. We completed the final searches on March 11, 2019 (Online Appendix 1).
Eligible criteria and evidence selection
To comprehensively select evidence for the synthesis, we defined inclusion and exclusion criteria beforehand. Inclusion criteria were as follows: (1) studies that investigated a population undergoing prostatectomy and (2) interventions that involved RS-RARP. Exclusion criteria were as follows: (1) studies designed as single-arm trials, case series, and case reports; (2) references were editorial comments, corresponding responses, and letters to editor without updated data; and (3) references were gray literature without detail.
After the final comprehensive search, two investigators (T.E.T. and Y.N.K.) individually screened the potential references through two steps. In the first step, title and abstract screening, they included the references fulfilling the inclusion criteria. In the second step, full-text review, they removed the references according to the exclusion criteria. Another investigator resolved disagreements regarding article eligibility through discussions.
Quality assessment
Because this systematic review included randomized clinical trials and observational studies, we used the Cochrane risk-of-bias tool and Newcastle–Ottawa Quality Assessment Scale [25, 26]. The Cochrane risk-of-bias tool was used for the critical appraisal of randomized clinical trials, and the Newcastle–Ottawa Quality Assessment Scale was used for the quality assessment of observational studies. According to the Cochrane risk-of-bias tool, we evaluated sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias in randomized clinical trials. To evaluate the quality of observational studies, we assessed the representability of cohorts, ascertainment of exposure, reporting bias, comparability, assessment of outcomes, follow-up duration, and loss to follow-up in observational studies. Two investigators (T.E.T. and Y.N.K.) independently appraised the studies, and when they encountered any disagreement, the third investigator (J.C.W) participated in the quality assessment process to make a final judgement.
Data extraction
Two investigators (T.E.T. and Y.N.K.) independently extracted the characteristics of studies and outcome data. The third investigator (J.C.W) double-checked the data. The characteristics included publication year, country, study period, number of patients, mean age, body mass index, prostate size, clinical stage, and Gleason score. The outcome data included PSMs, continence, incontinence, complications, console time, and hospital stay. Events and total number of patients were extracted for binary data, and means and standard deviations (SDs) were extracted for continuous data. When the original study reported standard errors (SEs), we calculated the SD according to the formula SE = SD/√n.
Statistical analysis
Our study not only synthesized the evidence in a qualitative manner but also conducted quantitative synthesis. Regarding the quantitative synthesis, we pooled binary data into odds ratios (ORs) and combined continuous data into mean differences (MDs). The binary data syntheses involved the outcomes of PSMs, continence, incontinence, and complications, whereas the continuous data syntheses involved console time and hospital stay. All syntheses were conducted in a random-effects model. The results were reported in effect sizes, 95% confidence intervals (CIs), and I2 with p value of τ2. The I2 is commonly used to demonstrate heterogeneity across synthesized studies, and usually, heterogeneity is indicated when I2 reaches 50%. I2 > 75% reflects high heterogeneity among the synthesized studies. Another method for detecting heterogeneity in meta-analysis is the p value of τ2. A p value of τ2 < 0.10 represents high heterogeneity in the meta-analysis [27]. Furthermore, to examine the quality of the quantitative syntheses, the present study used a funnel plot with Egger’s test for the small study effects. Because some situations might have affected pooled results, we used subgroup analysis. For instance, we further examined pathological stages, study designs, and sites of PSMs for the PSM results. The quantitative syntheses were completed in Review Manager (version 5.3, The Cochrane Collaboration, Oxford, UK), and small study effects were detected in Comprehensive Meta-Analysis (version 2).
Results
Search results
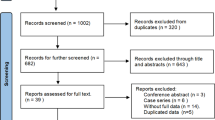
This systematic review identified 333 references from four electronic databases. The references were from Embase (n = 178), PubMed (including MEDLINE; n = 65), Scopus (n = 26), and Web of Science (n = 64). A total of 133 duplications were removed through the Endnote system function and manual screening. The titles and abstracts of the remaining 200 references were screened for eligibility. Subsequently, 168 references were excluded because they were nonrelevant studies (n = 114) without comparisons of Retzius sparing and traditional prostatectomy (n = 45), video (n = 3), or other documents (n = 6) according to the exclusion criteria. Next, the authors retrieved the full texts of the remaining 32 references and excluded 25 after a full-text review. The excluded 23 references were excluded because of documents (n = 10) and gray literature without details (n = 13), as well as no comparisons between RS-RARP and c-RARP (n = 2). The seven remaining references were two randomized clinical trials and four observational studies, which were synthesized in this systematic review. Figure 1 presents the process of evidence selection.

Flow diagram of this systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines
Overview of included studies
The six eligible studies involved 662 patients undergoing prostatectomy: 337 patients were in the c-RARP group and 325 patients were in the RS-RARP group. Table 1 presents information regarding included studies, including sample size, mean age, body mass index, prostate size, prostate-specific antigen, and Gleason score. These studies covered approximately 12 years from July 2005 to April 2017 in Italy [12], the Republic of China (Taiwan) [13], South Korea [28], the United Kingdom [29], and the USA [14,15,16]. The mean ages in each study ranged from 61 to 66. The quality of the included studies is detailed in Online Appendix 2.
Positive surgical margin
Six studies reported PSMs among 662 patients [12,13,14,15,16, 28, 29]. The overall pooling result demonstrated significantly higher PSM rates in RS-RARP compared with c-RARP (OR 1.68, 95% CI 1.08–2.62, p = 0.02) (Fig. 2A). The I2 reflected a low heterogeneity in the pooled result (I2 = 14%; p = 0.32). This study also conducted further analysis on PSMs according to pathological stage, study design (Online Appendix 3), and PSM site (Online Appendix 4). Results revealed no significant differences in PSM rates between c-RARP and RS-RARP in the subsets of pathological stages, observational study design, posterior site, and apical site. However, in the subsets of randomized clinical trial (OR 2.80, 95% CI 1.32–5.91, p = 0.007) and anterior site (OR 4.34, 95% CI 1.18–15.89, p = 0.03), RS-RARP had significantly higher PSM rates than did c-RARP. These results were intermediate to large effect sizes with very low heterogeneity (I2 = 0%). Egger’s test did not detect any small study effects in the pooled result of PSM rates (t = 0.632, p = 0.561) (Fig. 2B; Online Appendix 5).

Pooled results of positive surgical margins: A forest plot and B funnel plot
Functional outcomes
Although all the included studies reported functional outcomes, they reported them differently. Four of the six studies reported short-term continence rate (within 1 month) [12,13,14,15,16], and five reported incontinence rates with different follow-up durations (Fig. 3A) [12, 14,15,16, 28, 29]. Regarding the continence rate, RS-RARP had a significantly higher pad-free rate than did c-RARP (OR 3.61, 95% CI 2.18–5.97, p < 0.001), and RS-RARP also had significantly higher usage rates within one pad than did c-RARP (OR 3.49, 95% CI 2.25–5.43, p < 0.001). These results were consistent among the included studies with 481 patients (I2 = 0%).

Forest plots of functional outcomes: A continence and B incontinence
Incontinence rates were reported in the first month in four studies (n = 402) [12, 14, 15, 28, 29], in the third month in three studies (n = 422) [12, 14,15,16], in the sixth month in three studies (n = 422) [12, 14,15,16], and in the 12th month in two studies (n = 320) [14,15,16]. RS-RARP had significantly lower incontinence rates than c-RARP in the first month (OR 0.30, 95% CI 0.19–0.48, p < 0.001), third month (OR 0.27, 95% CI 0.13–0.55, p < 0.001), sixth month (OR 0.32, 95% CI 0.20–0.50, p < 0.001), and 12th month (OR 0.25, 95% CI 0.15–0.44, p < 0.001). The pooled results demonstrated acceptable heterogeneity with p values > 0.10 in τ2 (Fig. 3B). A test for the subgroup differences confirmed the similar benefits of RS-RARP in terms of incontinence rate from short- to long-term periods (I2 = 0%, p = 0.95).
Secondary outcomes
Of the six included studies, three reported console time (n = 420) (Fig. 4A), five reported complication rate (n = 579) (Fig. 4B), and three reported hospital stay (n = 380) (Fig. 4C). Pooled results exhibited no significant differences in complication rates (OR 0.89, 95% CI 0.37–2.12, p = 0.79) and hospital stay (MD = − 0.23, 95% CI − 0.66 to 0.20, p = 0.29) between RS-RARP and c-RARP. However, RS-RARP had significantly shorter console times than did c-RARP (MD = − 18.19, 95% CI − 30.91 to −5.47, p = 0.005). Although the pooled results of console time were highly heterogeneous (I2 = 95%), the synthesized studies consistently exhibited the same trend.

Forest plots of secondary outcomes: A console time, B complication, and c hospital stay
Discussion
Through a comprehensive review and rigorous data synthesis, our study confirmed that RS-RARP had a higher PSM rate in the anterior aspect than did c-RARP, although RS-RARP leads to superior functional outcomes. These findings were consistent among randomized clinical trials and observational studies.
Regarding PSMs in RS-RARP, Menon et al. indicated that more aggressive disease in their RS-RARP group (≥ pathological T3 disease, 45% in RS-RARP vs. 23% in c-RARP, p = 0.04) might have accounted for higher PSM rates [14, 17]. However, Stonier et al. postulated that doubling the sample size might have achieved significantly higher PSM rates in their RS-RARP group when compared with c-RARP [17]. In our study, the findings supported the assumption of Stonier et al. Through pooling data and a larger sample size, the overall PSM rate was significantly higher in the RS-RARP group than in the c-RARP group. In the subgroup analysis, we noted a trend of higher PSM rates in both subgroups of pathological stage ≤ pT2 or > pT2. Furthermore, we did not detect heterogeneity between subgroups; in other words, more aggressive disease may not be the only reason contributing to higher PSM rates.
According to relevant reports, another factor may affect PSM rates and biochemical recurrence, namely capsular incision [30, 31]. Unfortunately, these reports have not considered RS. Therefore, we attempted to determine other factors for enhancing the understanding of PSM rates between RS-RARP and c-RARP according to the available data and our clinical experience. In our own experience, the margin in the anterior prostate is unclear when performing RS-RARP. Thus, in our meta-analysis, we further analyzed the sites of PSM into three subgroups, and found a significantly higher rate of PSM in the anterior aspect in RS-RARP than in c-RARP. This finding probably reflected the limited view of surgeons performing RS-RARP in the anterior aspect. This result is in line with the preliminary data of Kim et al. al, who showed that the apex and anterior regions accounted for 44% and 38% of PSMs, respectively [32].
Regarding functional benefits, RS-RARP achieves a significantly higher rate of urinary continence than does c-RARP, despite different definitions of urinary continence (completely dry or less than one safety pad used). RS-RARP also has lower incontinence rates than does c-RARP. These results are similar to those of the first team to report RS-RARP, who reported high continence rates in the short term [10]. RS-RARP was developed for improving postoperative functions, and its main features are radical prostatectomy performed through a posterior approach and the prevention of destruction of the Retzius space. The Retzius space contains critical anatomical structures that maintain continence, including the endopelvic fascia, puboprostatic ligaments, and prostatic fascia. Thus, RS-RARP achieving better outcome in urinary continence is reasonable, and we were not surprised by RS-RARP improving immediate continence rates. Furthermore, our finding also revealed that this benefit remains significant until 12 months after prostatectomy. This long-term benefit was homogeneously (I2 = 0%) reported in two studies, although one of them showed no significant difference in incontinence rates between RS-RARP and c-RARP at 1 year after operation [14,15,16]. This finding corresponds with the concern of Stonier et al. [17] and confirms the long-term benefit of RS-RARP.
In the secondary findings, because radical prostatectomy was performed through a posterior approach, RS-RARP required less console time. Using this approach, RS-RARP minimizes tissue dissection and avoids ligation of the deep venous complex. Moreover, no significant differences were found in complication rates and hospital stays between RS-RARP and c-RARP. These findings indicated that RS-RARP may be comparable with c-RARP in terms of safety and cost.
Previous synthesis
Before this systematic review and meta-analysis, two syntheses on this topic have been published [17, 33]. One was in the form of editorial comments [17], and the other was a systematic review with meta-analysis [33]. The editorial comments qualitatively synthesized three studies with 370 cases and confirmed the evidence of early return to continence with RS-RARP. Furthermore, the comments raised a critical concern about PSMs in RS-RARP, although they had no quantitative synthesis. The systematic review included one randomized clinical trial (n = 120), five observational studies (n = 876), a case series (n = 5), and two case reports (n = 2), yet only four studies (n = 500) contributed to the quantitative synthesis. The attached meta-analysis concluded that RS-RARP is associated with early continence recovery without higher risks in PSM. Unfortunately, this conclusion concerning PSM was based on relatively high heterogeneity (I2 = 50%), although the study separated its analysis of PSM by pathological stage.
The present study attempted to investigate this topic more deeply than previous syntheses through gathering all comparative studies comparing RS-RARP with c-RARP. Subsequently, we comprehensively identified two randomized clinical trials and four observational studies with 662 cases. Through a reasonable quantitative synthesis with subgroup analysis, our study reduced the heterogeneity in PSM. We appropriately used cases of each pathological stage as denominators in subgroups as well as presented overall pooled results of PSM rates between RS-RARP and c-RARP. Moreover, our meta-analysis successfully determined a critical factor—the site of PSM—for PSMs in RS-RARP. Therefore, this study provides stronger and more informative evidence on RS-RARP for clinical practice.
Limitations
Although our study has some advantages, four limitations should be considered. First, surgeon experience is a critical topic for surgical study, and our analysis could not control its effects. Therefore, future studies should investigate how experience of RS-RARP influences results. Second, the six included studies had different inclusion criteria, exclusion criteria (Online Appendix 6), and baseline characteristics, and such heterogeneities might have biased the PSM results. Third, information on the capsular incision, a potential factor associated with PSM, was not available in the included studies; therefore, the available evidence could not be used to analyze how capsular incision affected the pooled results of PSM rates between RS-RARP and c-RARP. Finally, the available evidence provided limited results on the prognosis of RS-RARP, which consequently we were unable to investigate.
Conclusion
The present meta-analysis revealed higher PSMs in the RS-RARP group, especially in the anterior aspect. However, RS-RARP has better outcome in urinary function and less console time than c-RARP with equivalent complication rates. We suggest that operators pay more attention to making clear surgical margins if the lesion is in the anterior prostate when performing RS-RARP. Additional studies are required to determine how to modify RS-RARP to clarify margins in the anterior prostate. Before a modified RS-RARP is developed, shared decision-making may be required in clinical practice, especially for RS-RARP for anterior prostate cancer. RS-RARP has the potential to be the future of prostate cancer surgery.
Abbreviations
- CI:
-
Confidence interval
- c-RARP:
-
Conventional robot-assisted laparoscopic radical prostatectomy
- MD:
-
Mean difference
- OR:
-
Odds ratio
- RS-RARP:
-
Retzius space-sparing robot-assisted laparoscopic prostatectomy
- SD:
-
Standard deviation
- SE:
-
Standard error
References
Jemal A, Center MM, DeSantis C, Ward EM (2010) Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomark Prev 19:1893–1907
Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, Fossati N, Gross T, Henry AM, Joniau S, Lam TB, Mason MD, Matveev VB, Moldovan PC, van den Bergh RCN, Van den Broeck T, van der Poel HG, van der Kwast TH, Rouviere O, Schoots IG, Wiegel T, Cornford P (2017) EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol 71:618–629
Schuessler WW, Schulam PG, Clayman RV, Kavoussi LR (1997) Laparoscopic radical prostatectomy: initial short-term experience. Urology 50:854–857
Guillonneau B, Vallancien G (2000) Laparoscopic radical prostatectomy: the Montsouris experience. J Urol 163:418–422
Tooher R, Swindle P, Woo H, Miller J, Maddern G (2006) Laparoscopic radical prostatectomy for localized prostate cancer: a systematic review of comparative studies. J Urol 175:2011–2017
Abbou CC, Hoznek A, Salomon L, Olsson LE, Lobontiu A, Saint F, Cicco A, Antiphon P, Chopin D (2001) Laparoscopic radical prostatectomy with a remote controlled robot. J Urol 165:1964–1966
Tewari A, Peabody J, Sarle R, Balakrishnan G, Hemal A, Shrivastava A, Menon M (2002) Technique of da Vinci robot-assisted anatomic radical prostatectomy. Urology 60:569–572
Jacobs EF, Boris R, Masterson TA (2013) Advances in robotic-assisted radical prostatectomy over time. Prostate Cancer 2013:902686
Galfano A, Ascione A, Grimaldi S, Petralia G, Strada E, Bocciardi AM (2010) A new anatomic approach for robot-assisted laparoscopic prostatectomy: a feasibility study for completely intrafascial surgery. Eur Urol 58:457–461
Galfano A, Di Trapani D, Sozzi F, Strada E, Petralia G, Bramerio M, Ascione A, Gambacorta M, Bocciardi AM (2013) Beyond the learning curve of the Retzius-sparing approach for robot-assisted laparoscopic radical prostatectomy: oncologic and functional results of the first 200 patients with ≥ 1 year of follow-up. Eur Urol 64:974–980
Hemal AK, Menon M (2018) Robotics in genitourinary surgery. Springer, Berlin
Asimakopoulos AD, Topazio L, De Angelis M, Agro EF, Pastore AL, Fuschi A, Annino F (2018) Retzius-sparing versus standard robot-assisted radical prostatectomy: a prospective randomized comparison on immediate continence rates. Surg Endosc 33(7):2187–2196
Chang LW, Hung SC, Hu JC, Chiu KY (2018) Retzius-sparing robotic-assisted radical prostatectomy associated with less bladder neck descent and better early continence outcome. Anticancer Res 38:345–351
Dalela D, Jeong W, Prasad MA, Sood A, Abdollah F, Diaz M, Karabon P, Sammon J, Jamil M, Baize B, Simone A, Menon M (2017) A pragmatic randomized controlled trial examining the impact of the Retzius-sparing approach on early urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol 72:677–685
Menon M, Dalela D, Jamil M, Diaz M, Tallman C, Abdollah F, Sood A, Lehtola L, Miller D, Jeong W (2018) Functional recovery, oncologic outcomes and postoperative complications after robot-assisted radical prostatectomy: an evidence-based analysis comparing the Retzius sparing and standard approaches. J Urol 199:1210–1217
Sayyid RK, Simpson WG, Lu C, Terris MK, Klaassen Z, Madi R (2017) Retzius-sparing robotic-assisted laparoscopic radical prostatectomy: a safe surgical technique with superior continence outcomes. J Endourol 31:1244–1250
Stonier T, Simson N, Davis J, Challacombe B (2019) Retzius-sparing robot-assisted radical prostatectomy (RS-RARP) vs standard RARP: it’s time for critical appraisal. BJU Int 123:5–7
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(264–269):w264
Chang SH, Kang YN, Chiu HY, Chiu YH (2018) A systematic review and meta-analysis comparing pigtail catheter and chest tube as the initial treatment for pneumothorax. Chest 153:1201–1212
Kao CC, Lin YS, Chu HC, Fang TC, Wu MS, Kang YN (2018) Association of renal function and direct-acting antiviral agents for HCV: a network meta-analysis. J Clin Med 7:314
Lin EY, Kuo YK, Kang YN (2018) Effects of three common lumbar interbody fusion procedures for degenerative disc disease: a network meta-analysis of prospective studies. Int J Surg (Lond, Engl) 60:224–230
Lin TM, Chi JE, Chang CC, Kang YN (2019) Do etoricoxib and indometacin have similar effects and safety for gouty arthritis? A meta-analysis of randomized controlled trials. J Pain Res 12:83–91
Chen LS, Chen WC, Kang YN, Wu CC, Tsai LW, Liu MZ (2019) Effects of transabdominal preperitoneal and totally extraperitoneal inguinal hernia repair: an update systematic review and meta-analysis of randomized controlled trials. Surg Endosc 33:418–428
Huang YJ, Kang YN, Huang YM, Wu AT, Wang W, Wei PL (2019) Effects of laparoscopic vs robotic-assisted mesorectal excision for rectal cancer: an update systematic review and meta-analysis of randomized controlled trials. Asian J Surg 42(6):657–666
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, Cochrane Bias Methods G, Cochrane Statistical Methods G (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ (Clin Res Ed) 343:d5928
Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25:603–605
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ (Clin Res Ed) 327:557–560
Lim SK, Kim KH, Shin TY, Han WK, Chung BH, Hong SJ, Choi YD, Rha KH (2014) Retzius-sparing robot-assisted laparoscopic radical prostatectomy: combining the best of retropubic and perineal approaches. BJU Int 114:236–244
Eden CG, Moschonas D, Soares R (2018) Urinary continence four weeks following Retzius-sparing robotic radical prostatectomy: the UK experience. J Clin Urol 11:15–20
Koutlidis N, Duperron C, de la Vega MF, Mourey E, Michel F, Cormier L (2014) Capsular incision in normal prostatic tissue during robot-assisted radical prostatectomy: a new concept or a waste of time? World J Urol 32:1235–1240
Philippou Y, Harriss E, Davies L, Jubber I, Leslie T, Bell RW, Bryant RJ, Hamdy FC, Verill C, Lamb AD (2018) Prostatic capsular incision during radical prostatectomy has important oncological implications. A systematic review and meta-analysis. BJU Int. https://doi.org/10.1111/bju.14522
Kim LHC, Santok GD, Raheem AA, Alabdulaali I, Choi YD, Rha KH (2016) Incidence and location of positive surgical margin following Retzius-Sparing Robot-Assisted Radical Prostatectomy and its significance on oncological outcome. BJU Int 118:8
Dirie NI, Pokhrel G, Guan W, Mumin MA, Yang J, Masau JF, Hu H, Wang S (2018) Is Retzius-sparing robot-assisted radical prostatectomy associated with better functional and oncological outcomes? Literature review and meta-analysis. Asian J Urol 6(2):174–182
Acknowledgement
This manuscript was edited by Wallace Academic Editing.
Funding
No funding was requested for this systematic review and meta-analysis.
Author information
Authors and Affiliations
Contributions
TET conceptualized the study, screened the full text of the included studies, extracted the data, critically appraised the studies, drafted the manuscript, and approved the final manuscript; CCW interpreted the results, supervised the study, and approved the final manuscript; YNK designed the study, systematically searched the literature, screened the citations, extracted and analyzed the data, interpreted the results, drafted and critically revised the manuscript, and approved the final manuscript. JCW screened the full text of the included studies, checked the data, supervised the study, critically revised the manuscript, and approved the final manuscript.
Corresponding authors
Ethics declarations
Disclosures
Ting-En Tai, Chien-Chih Wu, Yi-No Kang, and Jeng-Cheng Wu have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Tai, TE., Wu, CC., Kang, YN. et al. Effects of Retzius sparing on robot-assisted laparoscopic prostatectomy: a systematic review with meta-analysis. Surg Endosc 34, 4020–4029 (2020). https://doi.org/10.1007/s00464-019-07190-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07190-2