
Abstract
Background
In Canada, bariatric surgery continues to remain the most effective treatment for severe obesity and its comorbidities. As the number of bariatric surgeries continues to grow, the need for consensus guidelines for optimal perioperative care is imperative. In colorectal surgery, enhanced recovery after surgery (ERAS) protocols were created for this purpose. The objective of this review is to develop evidence-based ERAS guidelines for bariatric surgery.
Methods
A literature search of the MEDLINE database was performed using ERAS-specific search terms. Recently published articles with a focus on randomized controlled trials, systematic reviews, and meta-analyses were included. Quality of evidence and recommendations were evaluated using the GRADE assessment system.
Results
Canadian bariatric surgeons from six provinces and ten bariatric centers performed a review of the evidence surrounding ERAS in bariatric surgery and created consensus guidelines for 14 essential ERAS elements. Our main recommendations were (1) to encourage participation in a presurgical weight loss program; (2) to abstain from tobacco and excessive alcohol; (3) low-calorie liquid diet for at least 2 weeks prior to surgery; (4) to avoid preanesthetic anxiolytics and long-acting opioids; (5) unfractionated or low-molecular-weight heparin prior to surgery; (6) antibiotic prophylaxis with cefazolin ± metronidazole; (7) reduced opioids during surgery; (8) surgeon preference regarding intraoperative leak testing; (9) nasogastric intubation needed only for Veress access; (10) to avoid abdominal drains and urinary catheters; (11) to prevent ileus by discontinuing intravenous fluids early; (12) postoperative analgesia with acetaminophen, short-term NSAIDS, and minimal opioids; (13) to resume full fluid diet on first postoperative day; (14) early telephone follow-up with full clinic follow-up at 3–4 weeks.
Conclusions
The purpose of addressing these ERAS elements is to develop guidelines that can be implemented and practiced clinically. ERAS is an excellent model that improves surgical efficiency and acts as a common perioperative pathway. In the interim, this multimodal bariatric perioperative guideline serves as a common consensus point for Canadian bariatric surgeons.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The prevalence of obesity has been increasing in Canada with obesity affecting an estimated 20% of Canadians [1]. Bariatric surgery continues to be the most effective treatment for obesity and obesity-related comorbidities for individuals with severe obesity or a body mass index (BMI) greater than 35 kg/m2 [2]. However, bariatric surgery has historically been underutilized in Canada, with only 0.1% of 1.5 million eligible patients receiving bariatric surgery per year [3]. As a result, Canadian bariatric programs began expanding to improve access to surgery and have achieved a four-times increase in volume between 2007 and 2013 [4]. Currently, the two main bariatric procedures offered across Canada are the Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG).
Although the rate of bariatric surgical complications have decreased over time, there are areas in the process of care that can be improved [5, 6]. Enhanced recovery after surgery (ERAS) pathways were initially developed for elective colorectal surgery to improve perioperative outcomes [7,8,9,10,11,12]. ERAS programs are multimodal approaches that involve evidence-based, perioperative interventions that maintain physiological function, enhance mobilization, reduce pain, and facilitate early oral nutrition [13]. Despite clear benefits in colorectal surgery, ERAS for bariatric surgery has not been widely implemented in Canada as there is a lack of consensus on ERAS guidelines.
This article is an initiative undertaken by expert bariatric surgeons across all major Canadian centers to develop consensus guidelines for optimal perioperative care in bariatric surgery based on the best available evidence.
Materials and methods
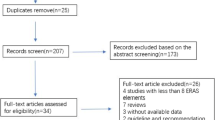
A literature search of the MEDLINE database was performed from database inception to August 2018 using search terms: “bariatric surgery,” “sleeve gastrectomy,” “gastric bypass,” “fast track,” and “enhanced recovery.” Search terms for specific ERAS elements were also included. Particular emphasis was placed on recently published articles of good quality with a focus on systematic reviews, meta-analyses, and randomized controlled trials (RCTs). Conference proceedings were excluded. Quality of evidence and recommendations were evaluated using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system [14]. Ethics approval and consent were not required for this type of study.
A group of Canadian bariatric surgeons from six different provinces and ten bariatric centers performed a review of the evidence surrounding ERAS in bariatric surgery and created consensus guidelines for 14 essential ERAS elements (Table 1).
Results
Recommendations, evidence, and grade of recommendations are summarized in Table 1.
Preadmission information and counseling
Information and counseling should be provided well before the bariatric procedure. This can be done through one-on-one sessions with the patient or through group sessions with the patient and their relatives. Preparation for bariatric surgery and hospital admission creates realistic expectations about hospitalization, analgesia, mobilization, and discharge [15]. We also recommend offering patients prehabilitation and exercise counseling, although evidence specific to bariatric surgery is lacking. A meta-analysis of patients undergoing cardiac and abdominal surgery found that prehabilitation led to lower complications and a shorter length of stay [16], while another systematic review found no physiological improvement with prehabilitation and limited clinical benefit [17]. However, in both of these reviews, the majority of patients were older than 60 years, which is much older than the typical bariatric surgery patient [18]. Further research in prehabilitation specific to bariatric surgery is needed to support this recommendation.
Patients are also encouraged to participate in a presurgical weight loss program. A meta-analysis performed in 2011 [19] and an updated review in 2015 [20] both demonstrated that preoperative weight loss was associated with a reduction in postoperative complications. Furthermore, a study of the Scandinavian Obesity Registry also demonstrated a reduction in complications [21]. Whether patients should be required to achieve specific levels of mandatory weight loss remains unclear [20].
Patient optimization and bowel preparation
Tobacco cessation of at least 3 months is highly recommended prior to bariatric surgery. Although studies specific to bariatric surgery are lacking, tobacco smoking has consistently been demonstrated to increase the risk of pulmonary complications, wound infections, and thromboembolism after surgery [22]. Specific to bariatric surgery, there is evidence of increased risk of anastomotic ulceration after RYGB in tobacco users [23, 24]. Furthermore, a systematic review demonstrated that smoking cessation of 4 weeks or longer decreased the risk of postoperative complications [22]. To ensure compliance, tobacco testing with urine cotinine may be considered [25].
Patients are also advised to abstain from excessive alcohol intake, including binge drinking. Moderate alcohol consumption below Canada’s low-risk drinking guidelines is permissible [26]. In elective surgery, alcohol consumption is associated with increased perioperative risk [27]. There is also a higher risk of alcohol abuse after RYGB, and patients should be aware of this, especially those with a history of alcohol abuse [28].
With Canada’s planned legalization of cannabis, questions remain about the safety of cannabis in bariatric surgery. A review on this topic found little evidence on cannabis in bariatric surgery patients, although there is some evidence that chronic cannabis use has negative health effects [29]. Our recommendation is that patients with significant cannabis use should be carefully selected.
Chronic opioid use is common among bariatric surgery patients due to obesity-related symptoms. A retrospective cohort study found that after bariatric surgery in chronic opioid users, the majority continued to use opioids and at a higher dose [30], demonstrating that weight loss does not appear to reduce opioid usage. These patients should be assessed by a chronic pain specialist to optimize pain management prior to surgery. Treating postoperative pain in chronic opioid users is difficult and preoperative counseling may be necessary to ensure patients are properly educated.
Mechanical bowel preparations are not required prior to bariatric surgery. Although there is recent evidence supporting a combination of mechanical bowel preparation with antibiotics to reduce surgical site infection (SSI) in elective colorectal surgery [31], this does not apply to bariatric surgery. Combined mechanical bowel and oral antibiotic preparations prevent SSI by reducing fecal bacterial load and bacterial concentration within the colon [31]. However, bariatric surgery is performed only on the upper gastrointestinal tract, which has no fecal load and much lower bacterial counts [32].
Preoperative fasting and carbohydrate loading
A low-calorie diet (LCD, 1000–1200 kcal/day) or very low-calorie diet (VLCD, 400–800 kcal/day) is recommended for at least 2 weeks before surgery and up to 3–4 weeks for patients with a higher BMI. The main purpose of this preoperative diet is to reduce the size of the liver which reduces the technical difficulty of the bariatric procedure. This is supported by a systematic review that demonstrated an average reduction in liver volume of 14% with LCDs ranging from 2 to 12 weeks [33]. Another systematic review which only included VLCDs, ranging from 10 to 63 days, found that liver volume decreased by 5–20%. However, this meta-analysis found no difference in surgical complications [34]. Despite this, an RCT on two-week VLCD and RYGB found a reduction in 30-day complications (13.2% vs. 5.8%, p = 0.04) as well as the surgeon’s perceived difficulty of the procedure [35].
For preoperative fasting, our guidelines follow anesthesia society recommendations of 2 h for clear fluids and 6 h for solids before induction of anesthesia [36]. Carbohydrate loading prior to surgery has also been a part of the colorectal ERAS pathway; however, evidence in bariatric surgery is limited and not currently recommended, especially in patients with diabetes where evidence is lacking.
Preanesthetic medications
Currently, ERAS guidelines have been published for the practice of anesthesia in gastrointestinal surgery [37, 38]. Based on these guidelines, patients with higher-risk comorbidities should be seen at a preadmission clinic by anesthesia to optimize their perioperative care [37].
Preanesthetic administration of long-acting opioids increases the risk of postoperative respiratory depression and hypoventilation, especially in patients with obesity who have a higher incidence of obstructive sleep apnea and obesity hypoventilation syndrome [39]. Furthermore, anxiolytics such as benzodiazepines should be avoided as evidence does not support effectiveness in reducing preoperative anxiety [40]. Our consensus is to avoid long-acting sedatives and opioids as their effects can be unpredictable and delay postoperative recovery. Furthermore, a RCT comparing non-opioid to opioid-based anesthesia during LSG found comparable efficacy with regard to pain scores [41]. A preoperative dose of dexamethasone for postoperative nausea and vomiting is also recommended, although evidence specific to bariatric surgery is lacking [42].
Thromboprophylaxis
Patients with obesity have been shown to have an increased risk for venous thromboembolism [43]. Thromboembolic complications represent 50% of mortality associated with bariatric surgery [13, 44]. To prevent these events, thromboembolic prophylaxis is now a common practice in patients undergoing bariatric surgery. Currently, low-molecular-weight heparins have been shown to be just as effective, if not more effective than unfractionated heparin in preventing postoperative venous thromboembolism [45, 46]. Our group consensus recommends the use of unfractionated heparin of at least 5000 units or weight-adjusted low-molecular-weight heparin prior to surgery. However, the group did not reach consensus on the use of compression stockings or pneumatic compression devices in preventing vein thromboembolisms [47].
Preoperative skin preparation and antimicrobial prophylaxis
Removal of body hair is a preoperative procedure that improves adhesion of the dressing and decreases surgical site contamination [48]. However, the process and method of removing hair can cause micro-insults to the skin which increases the risk of SSIs. The current group consensus recommends removing hair by clipping rather than by shaving, to reduce the risk of infection as the preferred method. This is supported by a Cochrane systematic review which analyzed three RCTs (n = 3193) comparing shaving to clipping and found higher rates of SSI with shaving compared to clipping (RR 2.02, 95% CI, 1.21–3.36) [48].
For preoperative skin preparation, a RCT that included 849 participants showed that subjects assigned to the chlorhexidine–alcohol group had a lower SSI rate overall compared to the povidone–iodine group (9.5% vs. 16.1%; P = 0.004; RR 0.59; 95% CI, 0.41–0.85) [49]. Therefore, skin preparation with chlorhexidine–alcohol is our current recommendation.
For antimicrobial prophylaxis, our recommendation is cefazolin which should be dosed pre-operatively [50] with metronidazole as an adjunct for patients undergoing RYGB [51]. A recent study demonstrated that cefazolin 2 g IV administered prior to skin incision achieves protective adipose tissue levels for the duration of the bariatric procedure [50]. Metronidazole is also recommended as an adjunct for patients undergoing RYGB due to increased enteric anaerobic contamination compared to SG; however, there is no evidence supporting this [52]. For patients with true penicillin allergies, vancomycin or clindamycin can be used as an alternative.
Anesthesia
Anesthetic considerations are detailed in ERAS guidelines designed for gastrointestinal surgeries [38]. However, the optimal anesthetic protocol should follow the mainstay principles of reduced opioid use which will help decrease patient recovery time. As well, the use of short-acting agents and the liberal use of antiemetics intraoperatively should decrease postoperative antiemetic therapy and the duration of stay in hospital [53].
Patients should receive a balanced volume of IV fluids intraoperatively. One study examined the outcomes of intraoperative fluid replacement in laparoscopic bariatric surgery and found that conservative (15 mL/kg) versus liberal (40 mL/kg) IV fluid administration did not change postoperative creatinine or creatine kinase [54]. Therefore, a conservative volume of IV fluids is recommended over a liberal approach to prevent fluid overload.
Although there has been some advocacy for combined epidural with general anesthesia for abdominal surgery, our consensus statement does not recommend epidural analgesia in primary laparoscopic bariatric surgery. Although there is no evidence in bariatric surgery, a RCT comparing epidural analgesics with patient-controlled analgesia in laparoscopic colorectal surgery found that epidural analgesia lead to no improvement in pain but longer hospital stays (3.7 vs. 2.8 days) and slower return of bowel function [55].
Hypothermia increases a patient’s risk for wound infection and delays healing; therefore, intraoperative normotherapy with preoperative warming in the holding area is recommended [56]. The use of heated insufflation during surgery is not recommended as a Cochrane systematic review demonstrated minimal increases in core temperatures with no reduction in adverse outcomes [57].
Intraoperative leak testing
There are currently no standard guidelines and requirements to perform intraoperative leak testing in bariatric surgery. However, early recognition and treatment of anastomotic or staple line leaks are important to reducing complications and length of stay. In a retrospective cohort study, routine intraoperative leak testing was performed in 1329 LSG cases but yielded zero positive results [58]. In another prospective series, 342 LRYGB cases underwent air leak testing with six positive cases, requiring reinforcement of the gastrojejunal anastomosis [59]. However, there is no evidence supporting that intraoperative leak testing reduces the incidence of postoperative leaks. Therefore, it is our recommendation that routine intraoperative leak testing is not required but is up to the surgeon’s preference. The method in which intraoperative leak testing is performed varies and can be performed by air or methylene blue during intraoperative endoscopy. The use of an orogastric tube to administer air or methylene blue is not recommended as a retrospective study demonstrated a lower rate of leak detection (8 vs. 4%) than with intraoperative endoscopy [60].
Nasogastric intubation
Historically, routine nasogastric intubation following abdominal surgery was the standard of care. However, research has shown that there is a limited role for nasogastric tubes in abdominal surgery or in bariatric surgery [61, 62]. A Cochrane systematic review, which included 37 studies (n = 5711), demonstrated that patients who were did not have nasogastric tubes had an earlier return of bowel function (p < 0.001), lower rates of respiratory complications (p = 0.09), and lower rates of ventral hernias (p = 0.09) [63]. Despite this, nasogastric intubation may be helpful to decompress the stomach during Veress needle insertion [64]. Our recommendation is that nasogastric intubation may be used during Veress needle access but has no role postoperatively.
Abdominal and urinary drainage
Routine abdominal drainage is not recommended [65]. This is supported by a Cochrane review of intra-abdominal drains for the prophylaxis of anastomotic leaks in colorectal surgery [66]. In this review, three RCTs with 908 participants showed no statistically significant difference in anastomotic dehiscence in patients with and without intra-abdominal drains [66]. However, drains may be considered for complicated or revisional cases as there are much higher leak rates in these cases [67].
Current group consensus is that Foley catheters are not necessary for routine bariatric surgery cases. Insertion of urinary catheters can prolong hospital stays due to issues with urinary retention [68]. One study demonstrated that early Foley catheter removal after bariatric surgery, as part of an ERAS clinical pathway, leads to shorter hospital stays [69]. Therefore, we do not recommend Foley catheters.
Prevention of postoperative ileus
To prevent postoperative ileus, it is important to avoid excessive intravenous fluids through early discontinuation of intravenous infusions and early return to oral fluid intake [70]. According to one RCT in major abdominal surgery, optimal postoperative fluid management should be individualized and goal-directed [71]. Regarding prokinetic agents, a Cochrane systematic review of 39 RCTs (n = 4615) demonstrated insufficient evidence to recommend prokinetic agents for the treatment of postoperative ileus [72]. However, alvimopan, a gamma-opioid receptor antagonist, has been shown to improve recovery times in patients postoperatively compared to placebo [72,73,74]. Other agents such as bisacodyl have been found to be effective in accelerating gastrointestinal motility following elective colorectal surgery and is an option to treat postoperative ileus [75]. Oral magnesium oxide is another intervention that has demonstrated benefit in preventing postoperative ileus [76, 77]. Our current recommendation is to avoid fluid overload by initiating early enteral feeds and discontinuation of intravenous infusions when possible. Overall, no current prokinetic agent has been shown to be effective in the treatment of postoperative ileus; however, alvimopan, bisacodyl, or magnesium oxide may be considered.
Another method to prevent postoperative ileus is to encourage early ambulation and the current group consensus is to ambulate within 4 h of surgery. A RCT in patients undergoing laparotomy and intestinal resection demonstrated that patients randomized to rehabilitation with early ambulation spent fewer days in hospital compared to traditional care (5.4 vs. 7.1 days, p = 0.01) [78]. Another prospective study showed that early ambulation, as part of a fast-track care package after bariatric surgery, leads to a shorter length of stay [69].
Postoperative analgesia
Initiating and providing effective postoperative pain management is crucial in a patient’s recovery process and important in achieving a reasonable discharge date. Following surgery with moderate to severe pain, opioids are frequently prescribed; however, it is recommended to minimize the use of opioids to decrease the associated side effects including nausea, vomiting, respiratory depression, and ileus [79]. A multimodal analgesic approach should be employed, including acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs), as studies have shown evidence of clinically superior outcomes when used in combinations [80]. However, for patients undergoing bariatric surgery, it is recommended that NSAIDs be used sparingly and for short durations, as NSAIDs increase the risk of marginal ulcers and may lead to poor anastomotic healing [81].
Early pain control can be achieved using subcutaneous or intravenous narcotics [82]; however, patients should be transitioned to oral medications as soon as possible. At the time of discharge, patients are frequently prescribed a short course of oral hydromorphone, Percocet, or tramadol [83]. Prescribed medications can be taken orally and liquid formulations or crushed pills may be required. Furthermore, the liberal use of antiemetics is important to reduce postoperative nausea and vomiting. The combination of ondansetron and dexamethasone has been shown to decrease the risk of postoperative nausea and vomiting [84]. In summary, postoperative pain control can be achieved through a multimodal pain approach and postoperative nausea and vomiting can be managed through the use of various antiemetics.
Postoperative nutrition
Postoperatively, patients may begin to sip on clear fluids the evening following the surgery once they are fully awake. A systematic review and meta-analysis of 13 trials (n = 1173 participants) showed no benefit in keeping a patient NPO following gastrointestinal surgery [85]. Moreover, providing a patient a full diet does not confer increased morbidity compared to NPO [86]; therefore, a full fluid diet should be initiated on postoperative day one [85, 86].
Discharge and follow-up
Following surgery, most patients will undergo a recovery process, as an inpatient, that culminates to their discharge. Criteria for discharge vary for different services, but on a whole is based on the main principles of meeting normal hemodynamics, establishing good pain control, tolerating diet, ambulating well, and being agreeable to leave. Our recommendation is to perform bloodwork as needed on postoperative day one if there are concerns about electrolyte abnormalities, blood loss, or early infection.
Upon discharge, a patient navigator should follow up with a phone call within 24–48 h to determine how the patient is managing at home. A follow-up clinic appointment is normally arranged 3–4 weeks after discharge and once again in 3 months.
Discussion
There are currently few published studies on enhanced recovery after surgery in bariatric surgery. The purpose of an ERAS protocol is to improve postoperative outcomes by reducing complications and morbidities associated with the procedure [87]. By addressing these 14 essential ERAS elements, it will help to develop guidelines that can be implemented and practiced clinically.
Compared to traditional care in bariatric surgery, the benefits of ERAS are to reduce variability in clinical practice, cost, and postoperative complications; ultimately improving the quality of care provided to patients. There has been keen interest for a Canadian protocol for a fast-track concept to improve surgical efficiency and create a common perioperative pathway.
The most recently published bariatric ERAS guidelines by Thorell et al. in 2016 [13] highlight recommendations and collaboration between different developed countries with the exception of North America [13]. Overall, ERAS is an excellent model that improves surgical efficiency and perioperative complications. In the interim, this bariatric perioperative guideline serves as a common consensus point for Canadian bariatric surgeons.
References
Twells LK, Gregory DM, Reddigan J, Midodzi WK (2014) Current and predicted prevalence of obesity in Canada: a trend analysis. C Open 2:E18–E26. https://doi.org/10.9778/cmajo.20130016
Sjöström L (2013) Review of the key results from the Swedish obese subjects (SOS) trial—a prospective controlled intervention study of bariatric surgery. J Intern Med 273:219–234. https://doi.org/10.1111/joim.12012
Padwal RS, Chang H-J, Klarenbach S, Sharma AM, Majumdar SR (2012) Characteristics of the population eligible for and receiving publicly funded bariatric surgery in Canada. Int J Equity Health 11:54. https://doi.org/10.1186/1475-9276-11-54
Canadian Institute for Health Information (2014) Bariatric Surgery in Canada. Can Inst Heal Inf
Chang SH, Stoll CRT, Song J, Varela JE, Eagon CJ, Colditz GA (2014) The effectiveness and risks of bariatric surgery an updated systematic review and meta-analysis, 2003–2012. JAMA Surg 149:275–287. https://doi.org/10.1001/jamasurg.2013.3654
Chen SY, Stem M, Schweitzer MA, Magnuson TH, Lidor AO (2015) Assessment of postdischarge complications after bariatric surgery: a National surgical quality improvement Program analysis. Surgery 158:777–786. https://doi.org/10.1016/j.surg.2015.04.028
Muller S, Zalunardo MP, Hubner M, Clavien PA, Demartines N (2009) A fast-track program reduces complications and length of hospital stay after open colonic surgery. Gastroenterology 136:842–847.e1. https://doi.org/10.1053/j.gastro.2008.10.030
Šerclová Z, Dytrych P, Marvan J, Nová K, Hankeová Z, Ryska O, Šlégrová Z, Burešová L, Trávníková L, Antoš F (2009) Fast-track in open intestinal surgery: Prospective randomized study (Clinical Trials Gov Identifier no. NCT00123456). Clin Nutr 28:618–624. https://doi.org/10.1016/j.clnu.2009.05.009
Khoo CK, Vickery CJ, Forsyth N, Vinall NS, Eyre-Brook IA (2007) A prospective randomized controlled trial of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer. Ann Surg 245:867–872. https://doi.org/10.1097/01.sla.0000259219.08209.36
Wind J, Hofland J, Preckel B, Hollmann MW, Bossuyt PMM, Gouma DJ, Van Berge Henegouwen MI, Fuhring JW, Dejong CHC, Van Dam RM, Cuesta MA, Noordhuis A, De Jong D, Van Zalingen E, Engel AF, Goei TH, De Stoppelaar IE, Van Tets WF, Van Wagensveld BA, Swart A, Van Den Elsen MJLJ, Gerhards MF, De Wit LT, Siepel MAM, Van Geloven AAW, Juttmann JW, Clevers W, Bemelman WA (2006) Perioperative strategy in colonic surgery; LAparoscopy and/or FAst track multimodal management versus standard care (LAFA trial). BMC Surg 6:1–8. https://doi.org/10.1186/1471-2482-6-16
Basse L, Raskov HH, Hjort Jakobsen D, Sonne E, Billesbølle P, Hendel HW, Rosenberg J, Kehlet H (2002) Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 89:446–453. https://doi.org/10.1046/j.0007-1323.2001.02044.x
Basse L, Jacobsen DH, Billesbolle P (2000) A clinical pathway to accelerated recovery afther colonic resection. Ann Surg 232:51
Thorell A, MacCormick AD, Awad S, Reynolds N, Roulin D, Demartines N, Vignaud M, Alvarez A, Singh PM, Lobo DN (2016) Guidelines for perioperative care in bariatric surgery: enhanced recovery after surgery (ERAS) society recommendations. World J Surg 40:2065–2083. https://doi.org/10.1007/s00268-016-3492-3
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schünemann HJ (2009) GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Br Med J 9:8–11. https://doi.org/10.1136/bmj.39489.470347.AD
Elliott JA, Patel VM, Kirresh A, Ashrafian H, Le Roux CW, Olbers T, Athanasiou T, Zacharakis E (2013) Fast-track laparoscopic bariatric surgery: a systematic review. Updates Surg 65:85–94. https://doi.org/10.1007/s13304-012-0195-7
Valkenet K, van de Port IGL, Dronkers JJ, De Vries WR, Lindeman E, Backx FJG (2011) The effects of preoperative exercise therapy on postoperative outcome: a systematic review. Clin Rehabil 25:99–111. https://doi.org/10.1177/0269215510380830
Lemanu DP, Singh PP, MacCormick AD, Arroll B, Hill AG (2013) Effect of preoperative exercise on cardiorespiratory function and recovery after surgery: a systematic review. World J Surg 37:711–720. https://doi.org/10.1007/s00268-012-1886-4
Buchwald H, Avidor Y, Braunwald E, Al E (2004) Bariatric surgery: a systematic review and meta-analysis. JAMA 292:1724–1737
Cassie S, Menezes C, Birch DW, Shi X, Karmali S (2011) Effect of preoperative weight loss in bariatric surgical patients: a systematic review. Surg Obes Relat Dis 7:760–767. https://doi.org/10.1016/j.soard.2011.08.011
Gerber P, Anderin C, Thorell A (2015) Weight loss prior to bariatric surgery: an updated review of the literature. Scand J Surg 104:33–39. https://doi.org/10.1177/1457496914553149
Anderin C, Gustafsson UO, Heijbel N, Thorell A (2015) Weight loss before bariatric surgery and postoperative complications: data from the scandinavian obesity registry (SOReg). Ann Surg 261:909–913. https://doi.org/10.1097/SLA.0000000000000839
Mills E, Eyawo O, Lockhart I, Kelly S, Wu P, Ebbert JO (2011) Smoking cessation reduces postoperative complications: a systematic review and meta-analysis. Am J Med 124:144–154. https://doi.org/10.1016/j.amjmed.2010.09.013
Spaniolas K, Yang J, Crowley S, Yin D, Docimo S, Bates AT, Pryor AD (2018) Association of long-term anastomotic ulceration after Roux-en-Y gastric bypass with tobacco smoking. JAMA Surg 153(9):20–22
Coblijn UK, Lagarde SM, de Castro SMM, Kuiken SD, van Wagensveld BA (2015) Symptomatic marginal ulcer disease after Roux-en-Y gastric bypass: incidence, risk factors and management. Obes Surg 25:805–811. https://doi.org/10.1007/s11695-014-1482-9
Paci E, Pigini D, Bauleo L, Ancona C, Forastiere F, Tranfo G (2018) Urinary cotinine concentration and self-reported smoking status in 1075 subjects living in central Italy. Int J Environ Res Public Health 15(4):804
Butt P, Beirness D, Gliksman L, Paradis C, Stockwell T (2011) Alcohol and health in Canada: A summary of evidence and guidelines for low-risk drinking
Nath B, Li Y, Carroll JE, Szabo G, Tseng JF, Shah SA (2010) Alcohol exposure as a risk factor for adverse outcomes in elective surgery. J Gastrointest Surg 14:1732–1741. https://doi.org/10.1007/s11605-010-1350-4
PleckaÖstlund M, Backman O, Marsk R, Stockeld D, Lagergren J, Rasmussen F, Nas̈lund E (2013) Increased admission for alcohol dependence after gastric bypass surgery compared with restrictive bariatric surgery. JAMA Surg 148:374–377. https://doi.org/10.1001/jamasurg.2013
Rummell CM, Heinberg LJ (2014) Assessing marijuana use in bariatric surgery candidates: should It be a contraindication? Obes Surg 24:1764–1770. https://doi.org/10.1007/s11695-014-1315-x
Raebel MA, Newcomer SR, Reifler LM, Boudreau D, Elliott TE, DeBar L, Ahmed A, Pawloski PA, Fisher D, Donahoo WT, Bayliss EA (2013) Chronic use of opioid medications before and after bariatric surgery. JAMA 310:1369–1376. https://doi.org/10.1001/jama.2013.278344
Scarborough JE, Mantyh CR, Sun Z, Migaly J (2015) Combined mechanical and oral antibiotic bowel preparation reduces incisional surgical site infection and anastomotic leak rates after elective colorectal resection: an analysis of colectomy-targeted ACS NSQIP. Ann Surg 262:331–337. https://doi.org/10.1097/SLA.0000000000001041
Walter J, Ley R (2011) The human gut microbiome: ecology and recent evolutionary changes. Annu Rev Microbiol 65:411–429. https://doi.org/10.1146/annurev-micro-090110-102830
van Wissen J, Bakker N, Doodeman HJ, Jansma EP, Bonjer HJ, Houdijk APJ (2016) Preoperative methods to reduce liver volume in bariatric surgery: a systematic review. Obes Surg 26:251–256. https://doi.org/10.1007/s11695-015-1769-5
Holderbaum M, Casagrande DS, Sussenbach S, Buss C (2018) Effects of very low calorie diets on liver size and weight loss in the preoperative period of bariatric surgery: a systematic review. Surg Obes Relat Dis 14:237–244. https://doi.org/10.1016/j.soard.2017.09.531
Van Nieuwenhove Y, Dambrauskas Z, Campillo-Soto A, Van Dielen F, Wiezer R, Janssen I, Kramer M, Thorell A (2011) Preoperative very low-calorie diet and operative outcome after laparoscopic gastric bypass: a randomized multicenter study. Arch Surg 146:1300–1305. https://doi.org/10.1001/archsurg.2011.273
Lambert E, Carey S (2016) Practice guideline recommendations on perioperative fasting: a systematic review. J Parenter Enter Nutr 40:1158–1165. https://doi.org/10.1177/0148607114567713
Scott MJ, Baldini G, Fearon KCH, Feldheiser A, Feldman LS, Gan TJ, Ljungqvist O (2015) Enhanced recovery after surgery (ERAS) for gastrointestinal surgery, part 1: pathophysiological considerations. Acta Anaesthesiol Scand 59(10):1212–1231
Feldheiser A, Aziz O, Baldini G, Cox BPBW, Fearon KCH, Feldman LS, Gan TJ (2015) Enhanced recovery after surgery (ERAS) for gastrointestinal surgery, part 2: consensus statement for anaesthesia practice. Acta Anaesthesiol scand 60(3):289–334
Izrailtyan I, Qiu J, Overdyk FJ, Erslon M, Gan TJ (2018) Risk factors for cardiopulmonary and respiratory arrest in medical and surgical hospital patients on opioid analgesics and sedatives. PLoS ONE 13(3):e0194553
Walker KJ, Smith AF (2009) Premedication for anxiety in adult day surgery (Review). Cochrane Database Syst Rev 7(4):CD002192
Mansour MA, Ahmed AA (2013) Nonopioid versus opioid based general anesthesia technique for bariatric surgery : a randomized double—blind study. Saudi J Anaesth 7(4):387
Srinivasa S, Kahokehr AA, Yu T (2011) Preoperative glucocorticoid use in major abdominal surgery. Ann Surg 254:183–191. https://doi.org/10.1097/SLA.0b013e3182261118
Rocha AT, Vasconcellos AG, Luz ER, No Araújo DM, Alves ES, Lopes AA (2006) Risk of venous thromboembolism and efficacy of thromboprophylaxis in hospitalized obese medical patients and in obese patients undergoing bariatric surgery. Obes Surg 16:1645–1655. https://doi.org/10.1381/096089206779319383
Overby DW, Kohn GP, Cahan MA, Galanko JA, Colton K, Moll S, Farrell TM (2009) Prevalence of thrombophilias in patients presenting for bariatric surgery. Obes Surg 19:1278–1285. https://doi.org/10.1007/s11695-009-9906-7
Critique SI (2012) Comparative effectiveness of unfractionated and low-molecular-weight heparin for prevention of venous thromboembolism following bariatric surgery. Arch Surg 147:994–998
Mismetti P, Laporte S, Darmon J-Y, Buchmuller A, Decousus H (2001) Meta-analysis of low molecular weight heparin in the prevention of venous thromboembolism in general surgery. Br J Surg 88:913–930. https://doi.org/10.1046/j.0007-1323.2001.01800.x
Dogan K, Kraaij L, Aarts EO, Koehestanie P, Hammink E (2015) Fast-track bariatric surgery improves perioperative care and logistics compared to conventional care. 25(1):28–35
Tanner J, Woodings D, Moncaster K (2008) Preoperative hair removal to reduce surgical site infection (Review). J Perioper Pract 18(6):232–243
Rabih O, Darouiche MD (2010) Chlorhexidine–alcohol versus povidone– iodine for surgical-site antisepsis. J Med 362(1):18–26
Chen X, Brathwaite CEM, Barkan A, Hall K, Chu G, Cherasard P, Wang S, Nicolau DP, Islam S, Cunha BA (2017) Optimal cefazolin prophylactic dosing for bariatric surgery : no need for higher doses or intraoperative redosing. 27(3):626–629
Bratzler DW, Houck PM, Infection S (2005) Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Clin Infect Dis 189:395–404. https://doi.org/10.1016/j.amjsurg.2005.01.015
Willis AT, Fergusion IR, Jones PH, Phillips KD, Tearle PV, Fiddian RV, Graham DF, Harland DHC, Hughes DFR, Knight D, Mee WM, Pashby N, Sachdeva AK, Sutch I, Kilbey C (1977) Metronidazole in prevention and treatment of bacteroides infections in elective colonic surgery. Br Med J 6061(1):607–610
Tufanogullari B, White PF, Kianpour D, Lacour T, Griffin J, Skrivanek G (2008) Surgery : the effect on recovery outcome variables. Aneath Anal 106(6):1741–1748
Wool DB, Lemmens HJM, Brodsky JB, Solomon H, Chong KP, Morton JM (2010) intraoperative fluid replacement and postoperative creatine phosphokinase levels in laparoscopic bariatric patients. Obes Surg 20(6):698–701
Levy BF, Scott MJ, Fawcett W, Fry C, Rockall TA (2011) Randomized clinical trial of epidural, spinal or patient-controlled analgesia for patients undergoing laparoscopic colorectal surgery. Br J Surg 98(8):1068–1078
Kurz A, Sessler DI (1996) Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. N Engl J Med 334(19):1209–1216
Birch DW, Dang JT, Switzer NJ, Manouchehri N, Shi X, Hadi G, Karmali S (2016) Heated insufflation with or without humidification for laparoscopic abdominal surgery. Cochr Database Syst Rev. https://doi.org/10.1002/14651858.cd007821.pub3
Sethi M, Zagzag J, Patel K, Magrath M, Somoza E, Parikh MS, Saunders JK, Bradley AU, Marina FS, Ren-fielding GAFCJ (2016) Intraoperative leak testing has no correlation with leak after laparoscopic sleeve gastrectomy. Surg Endosc 30:883–891. https://doi.org/10.1007/s00464-015-4286-7
Nimeri A, Ghabra S, Dehni N, Elamin D, Al Hadad M, Ibrahim M (2015) Intraoperative endoscopy decreases postoperative complications in laparoscopic Roux-en-y gastric bypass. Obes Surg 25:1711–1715. https://doi.org/10.1007/s11695-015-1604-z
Alaedeen D, Madan A, Ro CY, Khan KA, Martinez JMTD (2009) Intraoperative endoscopy and leaks after laparoscopic Roux-en-Y gastric bypass. Am Surg 75:485–488
Huerta S, Arteaga JR, Sawicki MP, Liu CD, Livingston EH, Angeles L, Nelson R, Tse B, Edwards S (2005) Assessment of routine elimination of postoperative nasogastric decompression after Roux-en- Y gastric bypass. Surgery 132(5):844–848
Nelson R, Tse B, Edwards S (2005) Systematic review of prophylactic nasogastric decompression after abdominal operations. J Surg Swiss Surg 92(6):673–680
Verma R, Rl N (2010) Prophylactic nasogastric decompression after abdominal surgery (Review). doi: 10.1002/14651858.CD004929.pub3.www.cochranelibrary.com
Agarwala N, Liu CY (2005) Safe entry techniques during laparoscopy : Left upper quadrant entry using the ninth intercostal space—a review of 918 procedures. J Mimim Invasive Gynecol 12(1):55–61
Dallal RM, Bailey L, Nahmias N (2007) Back to basics–clinical diagnosis in bariatric surgery. Routine drains and upper GI series are unnecessary. Surg Endosc 21(12):2268–2271
Rolph R, Jmn D, Alagaratnam S, Ng P, Novell R (2016) Intra-abdominal drains for the prophylaxis of anastomotic leak in elective colorectal surgery (Review). doi: 10.1002/14651858.CD002100.pub2.www.cochranelibrary.com
Radtka JF, Puleo FJ, Wang L, Cooney RN (2010) Revisional bariatric surgery: who, what, where, and when? Surg Obes Relat Dis 6:635–642. https://doi.org/10.1016/j.soard.2010.04.005
Tammela T, Kontturi M, Lukkarinen O (2009) Postoperative urinary retention : I. incidence and predisposing factors. Scand J Urol Nephrol 20(3):197–201
Ronellenfitsch U, Schwarzbach M (2012) The effect of clinical pathways for bariatric surgery on perioperative quality of care. Obes Surg 22(5):732–739
Hop WCJ, Kok NFM, Lim A, Brouwer KJ, Jeekel J (2007) Randomized clinical trial of the impact of early enteral feeding on postoperative ileus and recovery. J Surg Swiss Surg 94(5):555–561
Pearse R, Harrison DA, Macdonald N, Gillies MA, Blunt M, Ackland G, Grocott MPW, Ahern A, Griggs K, Scott R, Hinds C, Rowan K, Study O (2015) Effect of a perioperative, cardiac output–guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery:a randomized clinical trial and systematic review. JAMA 311(21):2181–2190
Traut U, Brügger L, Kunz R, Haug K, Bucher H, Mt K, Traut U, Brügger L, Kunz R, Pauli-magnus C, Haug K, Bucher H, Koller MT (2009) Systemic prokinetic pharmacologic treatment for postoperative adynamic ileus following abdominal surgery in adults (Review) Systemic prokinetic pharmacologic treatment for postoperative adynamic ileus following abdominal surgery in adults. 4–6. https://doi.org/10.1002/14651858.cd004930.pub3.copyright
Wolff BG, Michelassi F, Gerkin TM, Techner L, Gabriel K, Du W, Wallin BA, Rothenberger DA, Van De Water JM, Dayton MT, Moody FG (2004) Alvimopan, a novel, peripherally acting μ opioid antagonist: results of a multicenter, randomized, double-blind, placebo-controlled, phase III trial of major abdominal surgery and postoperative ileus. Ann Surg 240:728–735
Delaney CP, Weese JL, Hyman NH, Bauer J, Techner L, Gabriel K, Du W, Schmidt WK, Wallin BA (2005) Phase III trial of alvimopan, a novel, peripherally acting, Mu opioid antagonist, for postoperative ileus after major abdominal surgery. Dis Colon Rectum 48:1114–1129. https://doi.org/10.1007/s10350-005-0035-7
Zingg U, Miskovic D, Pasternak I, Meyer P, Hamel CT, Metzger U (2008) Effect of bisacodyl on postoperative bowel motility in elective colorectal surgery: a prospective, randomized trial. Int J Colorectal Dis 23:1175–1183. https://doi.org/10.1007/s00384-008-0536-7
Hansen CT, Sørensen M, Møller C, Ottesen B, Kehlet H (2007) Effect of laxatives on gastrointestinal functional recovery in fast-track hysterectomy: a double-blind, placebo-controlled randomized study. Am J Obstet Gynecol 196:1–7. https://doi.org/10.1016/j.ajog.2006.10.902
Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N, McNaught CE, MacFie J, Liberman AS, Soop M, Hill A, Kennedy RH, Lobo DN, Fearon K, Ljungqvist O (2013) Guidelines for perioperative care in elective colonic surgery: enhanced recovery after surgery (ERAS®) society recommendations. World J Surg 37:259–284. https://doi.org/10.1007/s00268-012-1772-0
Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW (2003) Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postoperative care after laparotomy and intestinal resection. Dis Colon Rectum 46:851–859. https://doi.org/10.1007/s10350-004-6672-4
White P (2005) The changing role of non-opioid analgesic techniques in the management of postoperative pain. Anesth Analg 101(5S):S5–S22
Romsing J, Moiniche S, Dahl JB (2002) Rectal and parenteral paracetamol, and paracetamol in combination with NSAIDs, for postoperative analgesia. Br J Anaesth 88:215–226. https://doi.org/10.1093/bja/88.2.215
Gorissen KJ, Benning D, Berghmans T, Snoeijs MG, Sosef MN, Hulsewe KWE, Luyer MDP (2012) Risk of anastomotic leakage with non-steroidal anti-inflammatory drugs in colorectal surgery. Br J Surg 99:721–727. https://doi.org/10.1002/bjs.8691
Goudie TA, Allan MW, Lonsdale M, Burrow LM, Macrae WA, Grant IS (1985) Continuous subcutaneous infusion of morphine for postoperative pain relief. Anaesthesia 40:1086–1092
Rawal N, Amilon A (2001) Postoperative analgesia at home after ambulatory hand surgery: a controlled comparison of tramadol, metamizol and paracetamol. Anesth Analg 92(2):347–351
Henzi I, Walder B, Trame MR (2000) Dexamethasone for prevention of postoperative nausea and vomiting: a quantitative systematic review. Anesth Analg 1993:186–194
Lewis SJ, Andersen HK, Thomas S (2009) Early enteral nutrition within 24 h of intestinal surgery versus later commencement of feeding: a systematic review and meta-analysis. J Gastrointest Surg 13:569–575. https://doi.org/10.1007/s11605-008-0592-x
Lassen K, Kjæve J, Fetveit T, Tranø G, Sigurdsson HK, Horn A, Revhaug A (2008) Allowing normal food at will after major upper gastrointestinal surgery does not increase morbidity: a randomized multicenter trial. Ann Surg 247:721–729. https://doi.org/10.1097/SLA.0b013e31815cca68
Mattei P, Rombeau JL (2006) Review of the pathophysiology and management of postoperative ileus. World J Surg 30:1382–1391. https://doi.org/10.1007/s00268-005-0613-9
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Jerry T. Dang, Vivian G. Szeto, Ahmad Elnahas, James Ellsmere, Allan Okrainec, Amy Neville, Samaad Malik, Ekua Yorke, Dennis Hong, Laurent Biertho, Timothy Jackson, and Shahzeer Karmali have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dang, J.T., Szeto, V.G., Elnahas, A. et al. Canadian consensus statement: enhanced recovery after surgery in bariatric surgery. Surg Endosc 34, 1366–1375 (2020). https://doi.org/10.1007/s00464-019-06911-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-06911-x