
Abstract
Autosomal dominant non-syndromic hearing loss (ADNSHL) displays gene-specific progression of hearing loss, which is amenable to sequential audioprofiling. We sought to refine the natural history of ADNSHL by examining audiometric data in 5-year increments. 2175 audiograms were included from four genetic causes of ADNSHL—KCNQ4 (DFNA2), GSDME (DFNA5), WFS1 (DFNA6/14/38), and COCH (DFNA9). Annual threshold deterioration (ATD) was calculated for each gene: for the speech-frequency pure tone average, the ATD, respectively, was 0.72 dB/year, 0.94 dB/year, 0.53 dB/year, and 1.41 dB/year, with the largest drops occurring from ages 45–50 (0.89 dB/year; KCNQ4), 5–10 (1.42 dB/year; GSDME), 40–45 (0.83 dB/year; WFS1), and 50–55 (2.09 dB/year; COCH). 5-year interval analysis of audiograms reveals the gene specific natural history of KCNQ4, GSDME, WFS1 and COCH-related progressive hearing loss. Identifying ages at which hearing loss is most rapid informs clinical care and patient expectations. Natural history data are also essential to define outcomes of clinical trials that test novel therapies designed to correct or ameliorate these genetic forms of hearing loss.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hearing loss is the most common neurosensory deficit, affecting approximately half of the population by the age of 80 (Morton 1991). Its causality is multifactorial, with many environmental and genetic factors implicated in its development (Gordon 2008; Angeli et al. 2012). About half of cases are ascribed to genetics, with the relative percentage higher in childhood as compared to adulthood. Inheritance is typically simple Mendelian. There is significant variability in the audiometric phenotype of genetic deafness, reflecting its extreme heterogeneity.
In 2008, we developed AudioGene, a supervised support vector machine learning algorithm that uses audiometric data to predict genotypes (Hildebrand et al. 2008; Hildebrand et al. 2009). As an example of its clinical utility, at the time of its development targeted genetic screening using AudioGene resulted in the discovery of several novel variants in the KCNQ4 gene (Hildebrand et al. 2008). Comprehensive massively parallel sequencing panels are now the standard of care for the diagnosis of genetic hearing loss obviating the need for a priori gene selection for targeted sequencing. Nevertheless, AudioGene remains valuable as a tool to provide phenotypic correlation for novel potentially causative variants identified through massively parallel sequencing (Taylor et al. 2013) and in developing gene-specific natural history data for hearing outcomes in persons segregating genetic hearing loss. By grouping gene-specific audiograms into age-defined bins (for example, 20-year bins), AudioGene defines an audioprofile surface (APS), a method of representing audiometric data that incorporates sound frequency, decibels of hearing loss, and age in three dimensions. Graphed as a three-dimensional surface, average hearing thresholds can be displayed over a lifetime for gene-specific types of hearing loss. The KCNQ4 APS, for example, shows average thresholds over time for persons with KCNQ4-related hearing loss. This specificity allows clinicians to make direct comparison of patient thresholds to expected thresholds for a particular gene, thus making AudioGene a useful tool for providing counseling and treatment options for patients with hearing loss (Weininger et al. 2019).
Our objective in this study was to utilize additional audiometric data to refine the natural history of select types of genetic hearing loss. We focused on autosomal dominant nonsyndromic hearing loss (ADNSHL) as it is generally progressive with clinically significant hearing loss becoming apparent after language acquisition (post-lingual). Indeed, ADNSHL has been particularly amenable to audioprofiling due to its progressive nature and for some loci, unique patterns of hearing loss (e.g., WFS1-associated hearing loss at the DFNA6/14/38 locus) (Shearer et al. 1993), although more recently interest has also grown in audioprofiling progressive autosomal recessive forms of hearing loss (Oonk et al. 2016).
Herein, we sought to develop audioprofiles for selected forms of ADNSHL based on 5-year increments (with each increment or bin having at least 10 audiograms) and using these data determine the greatest frequency-specific annual threshold deteriorations (ATD) (dB/year). We reasoned that by identifying ages at which hearing loss is most rapid, clinical care and patient expectations would be improved, and outcomes of clinical trials using novel therapies to correct or ameliorate these genetic forms of hearing loss could be appropriately structured and evaluated.
Materials and methods
Data source
Audiograms associated with ADNSHL were collected for AudioGene from patients diagnosed at our institution, publications and collaborators, as previously described (Hildebrand et al. 2009; Taylor et al. 2013, 2016). At the time of writing, the AudioGene v4.0 database included 3393 audiograms from 1488 patients, grouped into 34 distinct genetic loci. We limited gene-specific analysis to those genes with at least 10 audiograms per 5 year age bin in 10 consecutive age bins. For genes meeting this criteria, we searched for additional audiograms by reviewing all manuscripts associated with any variant within these genes classified as likely pathogenic or pathogenic in the Deafness Variation Database (Azaiez et al. 2018). The standard audiogram recorded pure tone audiometry at 250, 500, 1000, 2000, 4000, and 8000 Hz; however, there was occasional variability between institutions. For inclusion in the database, at least 4 separate frequencies must have been tested. Each audiogram had an associated genetic variant, which was reviewed to ensure a classification of likely pathogenic or pathogenic using criteria established by the American College of Medical Genetics and Genomics (Oza et al. 2018). Variants were also classified according to their mutational signature (loss-of-function (LoF) versus missense) and location within a protein domain when relevant. The data for variant interpretation were reported to the Deafness Variation Database (http://deafnessvariationdatabase.org/).
Preprocessing
Audiograms were pre-processed prior to inclusion in this database. For audiograms with data from both ears, the better hearing ear was used at each frequency. Linear interpolation and extrapolation from 2nd or 3rd order polynomials fit to each audiogram were used to approximate missing values.
Audiometric data clustering
Audioprofiles for genes in which at least 10 of the 5-year bins contained at least 10 audiograms were plotted based on hearing loss in dB versus age at time of audiogram. Frequencies were classified as low (250, 500 Hz), middle (1000, 2000 Hz), and high (4000, 8000) (Shearer, Hildebrand and Smith, 1993). Calculation of pure tone average (PTA) at the speech frequencies was taken from the average of 500, 1000, 2000, and 4000 Hz (Agrawal et al. 2008). Audioprofiles in 5-year age bins for each gene were generated from low, middle, and high frequencies using GraphPad Prism v9.0.0 (San Diego, CA). To generate average threshold deterioration (ATD) for each age bin, polynomial curves were fitted; 2nd- or 3rd-order curves were selected based on root mean square error (RMSE) values. ATDs were calculated in 5-year clusters as: \(\frac{mean\left(threshol{d}_{older age interval}\right)-mean\left(threshol{d}_{younger age interval}\right)}{mean\left(ag{e}_{older age interval}\right)-mean\left({age}_{younger age interval}\right)}\). Three-dimensional audioprofile surfaces (APS) were generated for each locus from the included audiograms as previously described (Taylor et al. 2016) with the MathWorks MATLAB R2020b programming platform (Natick, MA). The scripts used are available on GitHub (https://github.com/clcg/audioprofile-surfaces). Multiple surfaces were fit to 1st, 2nd, and 3rd-degree polynomials along the z-axis, and each APS was ranked according to its RMSE during k-fold cross validation.
Results
Database
Of the 34 loci included in the database, KCNQ4 (DFNA2A), GSDME (DFNA5), WFS1 (DFNA6/14/38), and COCH (DFNA9) met criteria for inclusion. From the AudioGene v4.0 database, we reviewed 14 unique variants for KCNQ4, 4 unique variants for GSDME, 15 unique variants for WFS1, and 10 unique variants for COCH. For KCNQ4, 3 LoF variants were excluded from further analysis, and the remaining 11 were missense. Each GSDME variant affected splicing of exon 8, as previously described (Op de Beeck et al. 2012; Booth et al. 2018). All included WFS1 and COCH variants were missense. From 281 articles associated with likely pathogenic and pathogenic variants in the Deafness Variation Database in these four genes, 16 articles contained new audiograms not previously included in the database (Namba et al. 2012; Bai et al. 2014; Wang et al. 2014; Wang et al. 2018; Chai et al. 2014; Li-Yang et al. 2015; Niu et al. 2017; Choi et al. 2017; Huang et al. 2017; Booth et al. 2018; Parzefall et al. 2018; Cheng et al. 2018; Jung et al. 2018; Kobayashi et al. 2018; Shin et al. 2019; Mehregan et al. 2019). From these articles, we reviewed an additional 7 variants for KCNQ4, 8 variants for GSDME, 17 variants for WFS1, and 1 variant for COCH. In total, by ACMG criteria 17 variants were excluded for being variants of uncertain significance (VUS), 28 were likely pathogenic, 19 were pathogenic, and one variant for GSDME was a complex rearrangement and thus ACMG variant criteria were not applied. Numbers of variants are summarized by gene together with total number of audiograms in Table 1. Variant specific in silico pathogenicity scores, minor allele frequencies, ACMG classification and criteria, and protein domain are summarized in Supplemental Table S1. Number of families, audiograms per family, and reported ethnicity and country of origin for each family are reported in Supplemental Table S2. In total, there were 514 audiograms for KCNQ4, 368 for GSDME, 358 for WFS1, and 935 for COCH (Table 1, Fig. 1).

Audioprofiles and audioprofile surfaces
Low, middle, and high frequency audioprofiles are shown in Fig. 2. RMSE for 2nd- and 3rd-order polynomial curves for low frequency (250, 500 Hz), middle frequency (1000, 2000 Hz), high frequency (4000, 8000 Hz), and speech PTA (500, 1000, 2000, and 4000 Hz) are reported in Supplemental Table S3. ATDs for each frequency group are reported in Table 2. The full table of frequencies across age bins is reported in Supplemental Table S3. RMSE for APS with 3rd-degree polynomials of the z-axis for KCNQ4, GSDME, WFS1 and COCH were 7.36, 14.38, 12.86, and 8.48, respectively. RMSE for APS with 2nd-degree polynomials of the z-axis for KCNQ4, GSDME, WFS1 and COCH were 7.87, 13.85, 12.06, and 7.76, respectively. RMSE for APS with 1st-degree polynomials of the z-axis for KCNQ4, GSDME, WFS1 and COCH were 8.71, 15.54, 13.18, and 9.24, respectively. The APS with the lowest RMSE for each gene is included in Supplemental Figure S1 and can be viewed in three dimensions online at the AudioGene website (https://audiogene.eng.uiowa.edu/pages/naturalhistory).

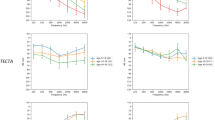
5-year audioprofile plots of hearing loss by low (250, 500 Hz), middle (1000, 2000 Hz), and high frequency (4000, 8000 Hz) groups for KCNQ4 (DFNA2) (A), GSDME (DFNA5) (C), WFS1 (DFNA6/14/38) (E), and COCH (DFNA9) (G). The error bars on plots A, C, E, and G are 95% confidence intervals. Audioprofiles at low, middle, and high frequency groups fit to 3rd degree polynomial curves are shown below each 5-year audioprofile (B, D, F, and H); each dot on the polynomial audioprofile plots represents a value from an individual audiogram. dB HL decibel hearing level. (Beisel 2005; Burgess et al. 2016; Cryns et al. 2003; Hosoya et al. 2016; Laer et al. 1998)
For speech PTA, the overall ATDs for KCNQ4, GSDME, WFS1 and COCH were 0.72 dB/year, 0.94 dB/year, 0.53 dB/year, and 1.41 dB/year, respectively. The greatest declines in hearing for speech PTAs were 0.89 dB/year from 45 to 50 for KCNQ4, 1.42 dB/year from 5 to 10 for GSDME, 0.83 dB/year from 40 to 45 for WFS1, and 2.09 dB/year from 50 to 55 for COCH. The age intervals with the greatest hearing deterioration at low frequencies were 70–75 (1.10 dB/year), 10–15 (1.10 dB/year), 40–45 (0.49 dB/year), and 60–65 (2.10 dB/year), respectively. The age intervals with the greatest hearing deterioration at middle frequencies were 50–55 (0.83 dB/year), 10–15 (1.19 dB/year), 35–40 (0.78 dB/year), and 55–60 (2.12 dB/year), respectively. The age intervals with the greatest hearing deterioration at high frequencies were 30–35 (1.26 dB/year), 10–15 (2.11 dB/year), 50–55 (1.47 dB/year), and 45–50 (2.10 dB/year), respectively. The greatest drops by frequency were 1.29 dB/year at 8000 Hz from 25 to 30 for KCNQ4, 2.60 dB/year at 8000 Hz from 5 to 10 for GSDME, 1.77 dB/year at 8000 Hz from 65 to 70 for WFS1, and 2.21 dB/year at 1000 Hz from 55 to 60 for COCH. ATDs are reported for each age bin at each frequency in Table 2 and Supplemental Table S4.
Discussion
Hearing loss can result from a large number of genetic or environmental causes (Gordon 2008; Angeli et al. 2012). With hundreds of loci implicated in inherited hearing loss, the diagnosis of “genetic deafness” offers little prognostic information in the absence of an associated cause. Even when gene-specific information is available, drawing conclusions about prognosis and annual rate of decline of hearing, if any, requires either significant longitudinal follow-up in a single family or numerous audiograms from multiple sources.
This study’s 5-year audioprofiles were constructed from the largest reported combined data set of audiograms for non-syndromic autosomal dominant genetic deafness and provide the most precise temporal resolution (in 5-year bins) for the 4 genes studied. Each gene demonstrated a unique pattern of hearing loss. By the 7th decade of life, all of the audioprofiles reached at least a severe hearing loss (> 70 dB hearing loss) at high frequencies, with GSDME (DFNA5) showing the most rapid decline of high frequency hearing in a single age bin. WFS1 (DFNA6/14/38) was the only gene to demonstrate a predominantly low frequency hearing loss, which eventually became severe across all frequencies by the 7th decade of life.
WFS1 encodes an integral glycoprotein essential for normal function of the endoplasmic reticulum (Zatyka et al. 2008). Pathogenic missense variants in this gene are associated with autosomal dominant predominantly low frequency hearing loss. Outside of WFS1, there have been only single variants in other genes causative of low frequency nonsyndromic sensorineural hearing loss, such as a splice site variant of the DIAPH1 gene segregating in a large Costa Rican family (Lynch et al. 1997) and an 8 base pair duplication within the CCDC50 gene segregating in a Spanish family (Modamio-Høybjør et al. 2007). In studies of individual families with low frequency autosomal dominant nonsyndromic hearing loss, progression to high frequency hearing loss eventually occurs (Bespalova et al. 2001). This progression is consistent with the superimposition of typical presbycusis (Osterhammel and Osterhammel 1979). Age-related typical audiograms (ARTAs) from two affected WFS1 families over 10 year age intervals generate similar data, with hearing loss only in the low frequencies in the younger ages, while a flat or high frequency-predominant hearing loss was demonstrated in the oldest age bins (Huygen et al. 2003). These temporal changes illustrate the importance of longitudinal audioprofiles, as the phenotype of hearing loss with respect to frequency can change drastically with age.
Low frequency hearing loss in families with WFS1-associated ADNSHL has previously been reported to begin before 10 years of age (Young et al. 2001; Fukuoka et al. 2007). Our study supports this finding, with normal hearing at high frequencies, mild hearing loss at middle frequencies, and moderate hearing loss at low frequencies in the 5–9 year age bin. The hearing loss remains stable until the 3rd decade of life, at which point hearing begins declining at all frequencies. WFS1 audioprofiling also highlights a limitation of contemporary physiologic newborn hearing screenings that rely on distortion product otoacoustic emission or automated auditory brainstem response testing. These tests typically do not measure frequencies below 1000 Hz, and an isolated low frequency hearing loss of any degree will likely be missed. Physiologic newborn hearing screening also has a variable sensitivity for hearing losses of up to 40 dB at any frequency (Norton et al. 2000), contributing to the markedly delayed median age of diagnosis for children born with minimal and mild hearing loss as compared to their peers with more severe hearing loss (Durieux-Smith et al. 2008). The audioprofile of COCH-associated ADNSHL, for example, demonstrates mild hearing loss at high frequencies and normal hearing at low and middle frequencies in the 15–19 year old age bin, a phenotype that may be missed on newborn screening.
KCNQ4, GSDME, and COCH each demonstrated predominantly high frequency hearing loss, which progressed at varying degrees. The audioprofile for KCNQ4, a gene expressing a voltage-gated potassium channel at the DFNA2A locus (Nie 2008), begins in childhood as a mild low frequency hearing loss sloping to a moderate hearing loss at high frequencies and progresses by the 5th decade of life to moderate-to-severe low frequency hearing loss sloping to profound hearing loss at high frequencies. Previous studies of KCNQ4-associated ADNSHL have suggested stable hearing at low frequencies (Naito et al. 2013); however, our data demonstrate that these individuals develop a severe hearing loss at low frequencies by the 6th decade of life. By comparison, presbycusis is not associated with low frequency hearing loss, even at the oldest ages (Osterhammel and Osterhammel 1979). This study’s audioprofiles are similar to individual familial ARTAs reported by Huygen, Pennings, and Cremers (Huygen et al. 2003). For each of the families affected by missense variants in KCNQ4 in their study and in our combined KCNQ4 missense audioprofile, while a high frequency hearing loss predominated at the youngest ages, there was a generally constant and equal decline in all frequencies over time.
GSDME (DFNA5) encodes for a member of the gasdermin protein family, and is involved in the apoptosis pathway (Li et al. 2019). Its audioprofile displays a similar pattern to KCNQ4, except the hearing loss is less severe in the first decade of life. Each included variant had the same predicted mechanism (skipping of exon 8), resulting in a truncated protein with abnormal pro-necrotic function that has been implicated in the induction of cell death (Van Rossom et al. 2012). Hearing loss associated with GSDME has been described as beginning between 7 and 30 years of age (Huizing et al. 1966; Cheng et al. 2007; Booth et al. 2018) with significant intrafamilial variability (Chai et al. 2014). Such intrafamilial variability is typical of other genes associated with adult-onset hearing loss, including RIPOR2, EYA4, and MYO6 (Oonk et al. 2013; Frykholm et al. 2015; de Bruijn et al. 2021). ARTAs for a single Dutch family affected by GSDME ADNSHL in 5–10 year intervals were previously reported by Huygen, Pennings, and Cremers (Huygen et al. 2003). In this family, the most severe drops in high frequency hearing occurred between 0 and 10 years of age followed by 10–20 years of age, with a much slower decline afterward. ARTAs generated for a separate Dutch family (Bischoff et al. 2004) and a family of unspecified European descent (Booth et al. 2020) demonstrated a constant decline in hearing over time at all frequencies after beginning as a predominantly high frequency hearing loss. These studies did not demonstrate the large decrease from 0 to 20 years of age in the family described by Huygen and colleagues. In aggregate, our cohort demonstrated the most rapid decline of high frequency hearing 5–15 years of age. This averaged 2 dB lost per year, which is an important point to emphasize when counseling affected patients, as they will need frequent audiologic follow-up with adjustment of their hearing aids during this critical period. Afterward, a relatively steady decline takes place from the 3rd decade of life.
COCH (DFNA9) encodes for cochlin, the major noncollagenous protein in the extracellular matrix of the cochlea and vestibule (Robertson et al. 1997; Ikezono et al. 2001; Jung et al. 2019; Verdoodt et al. 2021). COCH-related deafness is unique among other forms of ADNSHL due to its association with vestibular dysfunction and recurrent episodes of dizziness in some patients (Usami et al. 2003). Its audioprofile shows a predominantly high frequency hearing loss, though the onset is later in life than DFNA2 or DFNA5—from age 0 to 15, none of the patients had progressed to severe hearing loss, making onset of hearing loss later than the other studied ADNSHL genes (Robertson et al. 1998; Kamarinos et al. 2001). ARTAs in 10–20 year intervals for a single family affected by COCH ADNSHL (Huygen et al. 2003) demonstrated a large drop in hearing from 30 to 50 years of age followed by a much slower progression from 50 to 70 years of age. The rate of hearing deterioration in our audioprofile also significantly increased during the 4th decade of life but continued to progress to a profound hearing loss at all frequencies by the 8th decade of life at a relatively constant rate.
In a cohort of 470 patients diagnosed with autosomal dominant hearing loss, TECTA (DFNA8/12) (n = 47), WFS1 (DFNA6/14/38) (n = 32), MYO6 (DFNA22) (n = 29), KCNQ4 (DFNA2A) (n = 26), COL11A2 (DFNA13) (n = 16), and COCH (DFNA9) (n = 12) were the most common non-syndromic diagnoses (Molecular Otolaryngology and Renal Research Laboratories, unpublished data). KCNQ4, WFS1, and COCH are represented in the 4 genes analyzed in our data set, but GSDME (DFNA5) was diagnosed rarely in this cohort (n = 7). The relatively high number of audiograms from this locus is explained by the source of the audiograms; the majority of audiograms for GSDME in AudioGene come from two large Dutch families, one in which 37 members with hearing loss were identified as sharing a nucleotide substitution (Bischoff et al. 2004) and another totaling more than 60 members with hearing loss (Huizing et al. 1966). The family described by Huizing and colleagues, later discovered to segregate an intronic insertion/deletion variant within GSDME causing exon 8 skipping (Laer et al. 1998), is one of the largest for any type of hearing loss reported in the literature.
Accurate prognostic information of genetic deafness prevents unnecessary treatments, directs timing of potentially beneficial therapy, and is valuable for the affected patients themselves and their families (Dahl et al. 2013; Downie et al. 2019; Thorpe and Smith 2020). Cochlear implantation is beneficial for certain types of genetic hearing loss (Wu et al. 2011) and less helpful in others (Wu et al. 2015), depending on the biology of the affected gene. In particular, genes associated with pathology in the spiral ganglion are predicted to be poor responders to cochlear implants (Eppsteiner et al. 2012). Location of pathology associated with the 4 genes from our study is summarized in Table 3. Currently, age at implantation is not considered when cochlear implantation candidacy is evaluated. Rather, the most important audiologic assessment before considering cochlear implantation is speech perception, with diminishing returns for higher pre-operative speech perception performance (Boisvert et al. 2020). For each gene included in this study, reports of cochlear implantation have been descriptive and limited to small numbers of patients (Vermeire et al. 2006; Hildebrand et al. 2008; Nadol et al. 2015; Wu et al. 2015; Liu et al. 2019). Our data may be helpful for future studies in determining recruitment age of subjects and offering a natural history comparison group to those who receive implants.
One goal of research into the genetics of hearing loss is to provide gene-specific treatments that prevent or even restore the loss of hearing. Several approaches have been proposed for experimental delivery of gene therapy to the cochlea; however, to date, only viral vectors have shown promising results in animal models (Lustig and Akil 2012). Inoculation of adeno-associated viral (AAV) vectors directly into the murine cochlea via canal fenestration and injection through the round window membrane offers consistently robust transduction and minimal side effects (Yoshimura et al. 2018). There are several limitations and considerations for the gene therapy of deafness. For example, the protein must be amenable to the biology of gene replacement, with therapy slowing or reversing the disease process, and the therapy must be deliverable to the correct location. Furthermore, despite the versatility of AAV vectors, their use is limited by potential for immune reaction and their relatively small maximum package capacity of approximately 5.2 kb (Hermonat et al. 1997), although the use of simultaneous dual and triple AAV therapy allows for delivery of larger genomic packages (Akil 2020). Pertinent factors have been summarized for each of the 4 genes included in this study in Table 3. The pathogenesis of KCNQ4, GSDME, and WFS1-related hearing loss are associated with inner hair cells, and each hearing loss-specific transcript is smaller than 5 kb. Thus, patients affected by deafness from these three genes may 1 day be candidates for gene therapy. Our data will aid in design and recruitment of clinical trials targeting cochlear gene therapy, as it allows the identification of age groups that can derive the most benefit from treatment, and offers a potential comparison group in a clinical trial for patients undergoing gene therapy.
There are several limitations to our study. Only 4 genes met our criteria for inclusion based on number of audiograms available at each age bin; more audiograms are needed for the other loci. The audiograms in our cohort were from multiple sources, with some variation in frequencies tested, requiring preprocessing of the data. There were some instances of a single patient having multiple audiograms in the database (conducted at different times), while most patients only contributed a single audiogram. In our database, linear interpolation and extrapolation were used to approximate missing values at each frequency between 0.125 and 8 kHz. To minimize the use of interpolated data, we limited our data analysis to the most commonly tested frequencies: 0.25, 0.5, 1, 2, 4, and 8 kHz. Due to a variety of factors including reliability of the patient and physical interactions of pure tone sound waves in the ear canal, there can be variance between audiograms. This test–retest variability has been reported to be ~ 5 dB from 0.5 to 12.5 kHz for ~ 10% of patients (Valente, Valente and Goebel, 1992; Schmuziger et al. 2004). Data for this study were collected retrospectively, which can introduce bias regarding which audiograms were included. For patients who have a profound, maximal hearing loss at all frequencies, they probably will not undergo additional audiograms later in life. A publication bias may exist from audiograms demonstrating a maximal profound hearing loss, as these may be described qualitatively rather than shown in a figure. Nonetheless, we expect that the large size of our database overcomes this variability. Finally, the audiograms were categorized into genetically similar groups with similar mutation types, but as-of-yet unknown environmental and genetic factors may contribute to discrepancies in hearing loss in different populations (Walls et al. 2020).
Conclusion
Natural history data for ADNSHL demonstrate unique gene-specific audioprofiles that can inform clinical care and patient expectations by identifying ages and frequencies at which hearing loss is most rapid. These audioprofiles also will be informative to determine whether cochlear implantation delays progression of hearing loss and in the design of clinical trials testing novel therapies to correct or ameliorate hearing loss.
Data availability
Data supporting this study’s findings are available within the article and its supplementary materials.
Code availability
Code used to generate 3-D audioprofile surfaces using the MathWorks MATLAB programming platform (Natick, MA) is publicly available at https://github.com/clcg/audioprofile-surfaces.
References
Agrawal Y, Platz E, Niparko J (2008) Prevalence of hearing loss and differences by demographic characteristics among US adults: data from the national health and nutrition examination survey, 1999–2004. Arch Intern Med 168(14):1522. https://doi.org/10.1001/archinte.168.14.1522
Akil O (2020) Dual and triple AAV delivery of large therapeutic gene sequences into the inner ear. Hear Res 394:107912. https://doi.org/10.1016/j.heares.2020.107912
Angeli S, Lin X, Liu XZ (2012) Genetics of hearing and deafness. Anat Rec Adv Integr Anat Evol Biol 295(11):1812–1829. https://doi.org/10.1002/ar.22579
Azaiez H et al (2018) Genomic landscape and mutational signatures of deafness-associated genes. Am J Hum Genet 103(4):484–497. https://doi.org/10.1016/j.ajhg.2018.08.006
Bai X et al (2014) Identification of a novel missense mutation in the WFS1 gene as a cause of autosomal dominant nonsyndromic sensorineural hearing loss in all-frequencies. Am J Med Genet Part A 164(12):3052–3060. https://doi.org/10.1002/ajmg.a.36760
Beisel KW (2005) Differential expression of KCNQ4 in inner hair cells and sensory neurons is the basis of progressive high-frequency hearing loss. J Neurosci 25(40):9285–9293. https://doi.org/10.1523/JNEUROSCI.2110-05.2005
Bespalova IN et al (2001) Mutations in the Wolfram syndrome 1 gene (WFS1) are a common cause of low frequency sensorineural hearing loss. Hum Mol Genet 10(22):2501–2508. https://doi.org/10.1093/hmg/10.22.2501
Bischoff AMLC et al (2004) A novel mutation identified in the DFNA5 gene in a Dutch family: a clinical and genetic evaluation. Audiol Neurotol 9(1):34–46. https://doi.org/10.1159/000074185
Boisvert I et al (2020) Cochlear implantation outcomes in adults: a scoping review. PLoS ONE. https://doi.org/10.1371/journal.pone.0232421
Booth KT et al (2018) Exonic mutations and exon skipping: lessons learned from DFNA5. Hum Mutat 39(3):433–440. https://doi.org/10.1002/humu.23384
Booth KT, Azaiez H, Smith RJH (2020) DFNA5 (GSDME) c.991-15_991-13delTTC: founder mutation or mutational hotspot? Int J Mol Sci 21(11):3951. https://doi.org/10.3390/ijms21113951
Burgess BJ et al (2016) Histopathology of the human inner ear in the p. L114P COCH mutation (DFNA9). Audiol Neurotol 21(2):88–97. https://doi.org/10.1159/000443822
Chai Y et al (2014) A novel splice site mutation in DFNA5 causes late-onset progressive non-syndromic hearing loss in a Chinese family. Int J Pediatr Otorhinolaryngol 78(8):1265–1268. https://doi.org/10.1016/j.ijporl.2014.05.007
Cheng J et al (2007) A novel DFNA5 mutation, IVS8+4 A>G, in the splice donor site of intron 8 causes late-onset non-syndromic hearing loss in a Chinese family. Clin Genet 72(5):471–477. https://doi.org/10.1111/j.1399-0004.2007.00889.x
Cheng H et al (2018) Whole exome sequencing identifies a pathogenic mutation in WFS1 in two large Chinese families with autosomal dominant all-frequency hearing loss and prenatal counseling. Int J Pediatr Otorhinolaryngol 106:113–119. https://doi.org/10.1016/j.ijporl.2018.01.005
Choi HJ et al (2017) Whole-exome sequencing identified a missense mutation in WFS1 causing low-frequency hearing loss: a case report. BMC Med Genet 18(1):151. https://doi.org/10.1186/s12881-017-0511-7
Cryns K et al (2003) The WFS1 gene, responsible for low frequency sensorineural hearing loss and Wolfram syndrome, is expressed in a variety of inner ear cells. Histochem Cell Biol 119(3):247–256. https://doi.org/10.1007/s00418-003-0495-6
Dahl H-HM et al (2013) Etiology and audiological outcomes at 3 years for 364 children in Australia. PLoS ONE 8(3):e59624. https://doi.org/10.1371/journal.pone.0059624
de Bruijn SE et al (2021) A RIPOR2 in-frame deletion is a frequent and highly penetrant cause of adult-onset hearing loss. J Med Genet 58(2):96–104. https://doi.org/10.1136/jmedgenet-2020-106863
Downie L et al (2019) Exome sequencing in infants with congenital hearing impairment: a population-based cohort study. Eur J Hum Genet. https://doi.org/10.1038/s41431-019-0553-8
Durieux-Smith A, Fitzpatrick E, Whittingham J (2008) Universal newborn hearing screening: a question of evidence. Int J Audiol 47(1):1–10. https://doi.org/10.1080/14992020701703547
Eppsteiner RW et al (2012) Prediction of cochlear implant performance by genetic mutation: the spiral ganglion hypothesis. Hear Res 292(1–2):51–58. https://doi.org/10.1016/j.heares.2012.08.007
Frykholm C et al (2015) Phenotypic variability in a seven-generation Swedish family segregating autosomal dominant hearing impairment due to a novel EYA4 frameshift mutation. Gene 563(1):10–16. https://doi.org/10.1016/j.gene.2015.02.022
Fukuoka H et al (2007) Mutations in the WFS1 gene are a frequent cause of autosomal dominant nonsyndromic low-frequency hearing loss in Japanese. J Hum Genet 52(6):510–515. https://doi.org/10.1007/s10038-007-0144-3
Gordon AG (2008) Genes, hearing and deafness: from molecular biology to clinical practice. Int Psychogeriatr. https://doi.org/10.1017/S1041610208007357
Hermonat PL et al (1997) The packaging capacity of adeno-associated virus (AAV) and the potential for wild-type-plus AAV gene therapy vectors. FEBS Lett 407(1):78–84. https://doi.org/10.1016/S0014-5793(97)00311-6
Hildebrand MS et al (2008) Audioprofile-directed screening identifies novel mutations in KCNQ4 causing hearing loss at the DFNA2 locus. Genet Med 10(11):797–804. https://doi.org/10.1097/GIM.0b013e318187e106
Hildebrand MS et al (2009) A contemporary review of audiogene audioprofiling: a machine-based candidate gene prediction tool for autosomal dominant nonsyndromic hearing loss. Laryngoscope 119(11):2211–2215. https://doi.org/10.1002/lary.20664
Hosoya M et al (2016) Distinct expression patterns of causative genes responsible for hereditary progressive hearing loss in non-human primate cochlea. Sci Rep 6(1):22250. https://doi.org/10.1038/srep22250
Huang B et al (2017) A novel pore-region mutation, c.887G > A (p.G296D) in KCNQ4, causing hearing loss in a Chinese family with autosomal dominant non-syndromic deafness 2. BMC Med Genet 18(1):36. https://doi.org/10.1186/s12881-017-0396-5
Huizing EH, van Bolhuis AH, Odenthal DW (1966) Studies on progressive hereditary perceptive deafness in a family of 335 members: I. Genetical and general audiological results. Acta Otolaryngol 61(1–6):35–41. https://doi.org/10.3109/00016486609127040
Huygen PL, Pennings RJ, Cremers CW (2003) Characterizing and distinguishing progressive phenotypes in nonsyndromic autosomal dominant hearing impairment. Audiol Med 1(1):37–46. https://doi.org/10.1080/16513860310003049
Ikezono T et al (2001) Identification of the protein product of the Coch gene (hereditary deafness gene) as the major component of bovine inner ear protein. Biochim Biophys Acta (BBA) Mol Basis Dis 1535(3):258–265. https://doi.org/10.1016/S0925-4439(00)00101-0
Jung J et al (2018) Whole-exome sequencing identifies two novel mutations in KCNQ4 in individuals with nonsyndromic hearing loss. Sci Rep 8(1):16659. https://doi.org/10.1038/s41598-018-34876-9
Jung J et al (2019) Cleaved cochlin sequesters pseudomonas aeruginosa and activates innate immunity in the inner ear. Cell Host Microbe 25(4):513-525.e6. https://doi.org/10.1016/j.chom.2019.02.001
Kamarinos M et al (2001) Identification of a novelCOCH mutation, I109N, highlights the similar clinical features observed in DFNA9 families. Hum Mutat 17(4):351–351. https://doi.org/10.1002/humu.37
Kobayashi M et al (2018) WFS1 mutation screening in a large series of Japanese hearing loss patients: massively parallel DNA sequencing-based analysis. PLoS ONE. https://doi.org/10.1371/journal.pone.0193359
Laer LV et al (1998a) Nonsyndromic hearing impairment is associated with a mutation in DFNA5. Nat Genet 20(2):194–197. https://doi.org/10.1038/2503
Li Y-Q et al (2019) The deafness gene GSDME: its involvement in cell apoptosis, secondary necrosis, and cancers. Naunyn-Schmiedeberg’s Arch Pharmacol 392(9):1043–1048. https://doi.org/10.1007/s00210-019-01674-7
Liu W-H et al (2019) Mutation screening in non-syndromic hearing loss patients with cochlear implantation by massive parallel sequencing in Taiwan. PLoS ONE. https://doi.org/10.1371/journal.pone.0211261
Li-Yang M-N et al (2015) IVS8+1 DelG, a novel splice site mutation causing DFNA5 deafness in a Chinese family. Chin Med J 128(18):2510–2515. https://doi.org/10.4103/0366-6999.164980
Lustig LR, Akil O (2012) Cochlear gene therapy. Curr Opin Neurol 25(1):57–60. https://doi.org/10.1097/WCO.0b013e32834f038c
Lynch ED et al (1997) Nonsyndromic deafness DFNA1 associated with mutation of a human homolog of the drosophila gene diaphanous. Science 278(5341):1315–1318. https://doi.org/10.1126/science.278.5341.1315
Mehregan H et al. (2019) Novel mutations in KCNQ4, LHFPL5 and COCH genes in Iranian families with hearing impairment. Arch Iran Med 22(4): 189–197. Available at: http://www.ncbi.nlm.nih.gov/pubmed/31126177. Accessed 17 Jan 2021
Modamio-Høybjør S, Mencia A, Goodyear R, del Castillo I, Richardson G, Moreno F, Moreno-Pelayo MA (2007) A mutationin CCDC50, a gene encoding an effector of epidermal growth factor-mediated cell signaling, causes progressive hearing loss. Am J Hum Genet 80(6):1076–1089. https://doi.org/10.1086/518311
Morton NE (1991) Genetic epidemiology of hearing impairment. Ann NY Acad Sci 630:16–31. https://doi.org/10.1111/j.1749-6632.1991.tb19572.x
Nadol JB, Handzel O, Amr S (2015) Histopathology of the human inner ear in a patient with sensorineural hearing loss caused by a variant in DFNA5. Otol Neurotol 36(10):1616–1621. https://doi.org/10.1097/MAO.0000000000000888
Naito T et al (2013) Comprehensive genetic screening of KCNQ4 in a large autosomal dominant nonsyndromic hearing loss cohort: genotype-phenotype correlations and a founder mutation. PLoS ONE 8(5):e63231. https://doi.org/10.1371/journal.pone.0063231
Namba K et al (2012) In silico modeling of the pore region of a KCNQ4 missense mutant from a patient with hearing loss. BMC Res Notes 5:145. https://doi.org/10.1186/1756-0500-5-145
Nie L (2008) KCNQ4 mutations associated with nonsyndromic progressive sensorineural hearing loss. Curr Opin Otolaryngol Head Neck Surg 16(5):441–444. https://doi.org/10.1097/MOO.0b013e32830f4aa3
Niu Z et al (2017) Exome sequencing identifies a novel missense mutation of WFS1 as the cause of non-syndromic low-frequency hearing loss in a Chinese family. Int J Pediatr Otorhinolaryngol 100:1–7. https://doi.org/10.1016/j.ijporl.2017.06.008
Norton SJ et al (2000) Identification of neonatal hearing impairment: evaluation of transient evoked otoacoustic emission, distortion product otoacoustic emission, and auditory brain stem response test performance. Ear Hear 21(5):508–528. https://doi.org/10.1097/00003446-200010000-00013
Oonk AMM et al (2013) Progressive hereditary hearing impairment caused by a MYO6 mutation resembles presbyacusis. Hear Res 299:88–98. https://doi.org/10.1016/j.heares.2012.12.015
Oonk AMM et al (2016) Features of autosomal recessive non-syndromic hearing impairment: a review to serve as a reference. Clin Otolaryngol 41(5):487–497. https://doi.org/10.1111/coa.12567
Op de Beeck K, Van Laer L, Van Camp G (2012) DFNA5, a gene involved in hearing loss and cancer: a review. Ann Otol Rhinol Laryngol 121(3):197–207. https://doi.org/10.1177/000348941212100310
Osterhammel D, Osterhammel P (1979) High-frequency audiometry: age and sex variations. Scand Audiol 8(2):73–80. https://doi.org/10.3109/01050397909076304
Oza AM et al (2018) Expert specification of the ACMG/AMP variant interpretation guidelines for genetic hearing loss. Hum Mutat 39(11):1593–1613. https://doi.org/10.1002/humu.23630
Parzefall T et al (2018) Identification of a rare COCH mutation by whole-exome sequencing: implications for personalized therapeutic rehabilitation in an Austrian family with non-syndromic autosomal dominant late-onset hearing loss. Wien Klin Wochenschr 130(9–10):299–306. https://doi.org/10.1007/s00508-017-1230-y
Robertson NG et al (1997) Mapping and characterization of a novel cochlear gene in human and in mouse: a positional candidate gene for a deafness disorder, DFNA9. Genomics 46(3):345–354. https://doi.org/10.1006/geno.1997.5067
Robertson NG et al (1998) Mutations in a novel cochlear gene cause DFNA9, a human nonsyndromic deafness with vestibular dysfunction. Nat Genet 20(3):299–303. https://doi.org/10.1038/3118
Schmuziger N, Probst R, Smurzynski J (2004) Test-retest reliability of pure-tone thresholds from 0.5 to 16 kHz using sennheiser HDA 200 and etymotic research ER-2 earphones. Ear Hear 25(2):127–132. https://doi.org/10.1097/01.AUD.0000120361.87401.C8
Shearer AE, Hildebrand MS, Smith RJ (1993) Hereditary hearing loss and deafness overview. GeneReviews®. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20301607.
Shin DH et al (2019) A recurrent mutation in KCNQ4 in Korean families with nonsyndromic hearing loss and rescue of the channel activity by KCNQ activators. Human Mutat 40(3):335–346. https://doi.org/10.1002/humu.23698
Taylor KR et al (2013) AudioGene: predicting hearing loss genotypes from phenotypes to guide genetic screening. Human Mutat. https://doi.org/10.1002/humu.22268
Taylor KR et al (2016) Audioprofile surfaces. Ann Otol Rhinol Laryngol 125(5):361–368. https://doi.org/10.1177/0003489415614863
Thorpe RK, Smith RJH (2020) Future directions for screening and treatment in congenital hearing loss. Precis Clin Med. https://doi.org/10.1093/pcmedi/pbaa025
Usami S et al (2003) Mutations in the COCH gene are a frequent cause of autosomal dominant progressive cochleo-vestibular dysfunction, but not of Meniere’s disease. Eur J Hum Genet 11(10):744–748. https://doi.org/10.1038/sj.ejhg.5201043
Valente M, Valente M, Goebel J (1992) High-frequency thresholds: circumaural earphone versus insert earphone. J Am Acad Audiol 3(6): 410–418. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1486204.
Van Rossom S et al (2012) The splicing mutant of the human tumor suppressor protein DFNA5 induces programmed cell death when expressed in the yeast Saccharomyces cerevisiae. Front Oncol. https://doi.org/10.3389/fonc.2012.00077
Verdoodt D et al (2021) On the pathophysiology of DFNA9: effect of pathogenic variants in the COCH gene on inner ear functioning in human and transgenic mice. Hear Res 401:108162. https://doi.org/10.1016/j.heares.2020.108162
Vermeire K et al (2006) Good speech recognition and quality-of-life scores after cochlear implantation in patients with DFNA9. Otol Neurotol 27(1):44–49. https://doi.org/10.1097/01.mao.0000187240.33712.01
Walls WD et al (2020) A comparative analysis of genetic hearing loss phenotypes in European/American and Japanese populations. Hum Genet 139(10):1315–1323. https://doi.org/10.1007/s00439-020-02174-y
Wang H et al (2014) Targeted high-throughput sequencing identifies pathogenic mutations in KCNQ4 in two large Chinese families with autosomal dominant hearing loss. PLoS ONE. https://doi.org/10.1371/journal.pone.0103133
Wang H et al (2018) Further evidence for “gain-of-function” mechanism of DFNA5 related hearing loss. Sci Rep 8(1):8424. https://doi.org/10.1038/s41598-018-26554-7
Weininger O et al (2019) Computational analysis based on audioprofiles: a new possibility for patient stratification in office-based otology. Audiol Res 9(2):230. https://doi.org/10.4081/audiores.2019.230
Wu C-C et al (2011) Genetic characteristics in children with cochlear implants and the corresponding auditory performance. Laryngoscope 121(6):1287–1293. https://doi.org/10.1002/lary.21751
Wu C-C et al (2015) Identifying children with poor cochlear implantation outcomes using massively parallel sequencing. Medicine 94(27):e1073. https://doi.org/10.1097/MD.0000000000001073
Yoshimura H et al (2018) Enhanced viral-mediated cochlear gene delivery in adult mice by combining canal fenestration with round window membrane inoculation. Sci Rep 8(1):2980. https://doi.org/10.1038/s41598-018-21233-z
Young T-L et al (2001) Non-syndromic progressive hearing loss DFNA38 is caused by heterozygous missense mutation in the Wolfram syndrome gene WFS1. Hum Mol Genet 10(22):2509–2514. https://doi.org/10.1093/hmg/10.22.2509
Zatyka M et al (2008) Sodium-potassium ATPase 1 subunit is a molecular partner of Wolframin, an endoplasmic reticulum protein involved in ER stress. Hum Mol Genet 17(2):190–200. https://doi.org/10.1093/hmg/ddm296
Acknowledgements
This project was supported by National Institutes of Health—National Institute on Deafness and Other Communication Disorders grant R01 DC002842, DC012049 and DC017955 (RJHS) and National Institutes of Health—National Institute on Deafness and Other Communication Disorders grant 5T32DC000040 (RKT).
Author information
Authors and Affiliations
Contributions
RKT, TLC, and RJHS devised the project. RKT, WDW, RC, PH, TLC, and RJHS collected the data. RKT, WDW, RC, TLC, KW, and RJHS performed the calculations and analyzed the data. RKT and AS reviewed the included variants using the American College of Medical Genetics and Genomics (ACMG) criteria. RKT and RJHS wrote the manuscript. All authors discussed the results of the analysis and contributed to the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
None to report.
Ethics approval
Audiograms for AudioGene were collected from patients and data anonymized as approved by the University of Iowa Institutional Review Board (IRB), project identification number 199701065.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
439_2021_2424_MOESM1_ESM.xlsx
Supplementary file1 (XLSX 33 KB) Supplemental Table S1: Variants included in the database of audiograms with their associated ACMG (American College of Medical Genetics and Genomics) criteria, pathogenicity classification, in silico pathogenicity scores, minor allele frequencies, and protein domain. †: this variant is a complex rearrangement and thus ACMG variant criteria were not applied. COCH: NM_004086.3, KCNQ4: NM_004700.4, GSDME: NM_004403.2, WFS1: NM_006005.3, PP2 = PolyPhen-2, MT = MutationTaster, P = Pathogenic, LP = Likely Pathogenic, VUS = Variant of Uncertain Significance, ND = No Data, N/A: Not Applicable, D = Damaging, B = Benign, N = Neutral, C = Conserved, NC = Non-Conserved. Supplemental Table S2: Number of families, audiograms per family, and reported ethnicity and country of origin for each variant included in this study. Multiple rows are used for single variants if there are audiograms from multiple ethnicities for that variant. The source of the audiogram is also reported as from AudioGene, OtoSCOPE (a comprehensive massively parallel sequencing panel for hearing loss), or a separate manuscript’s PMID (PubMed reference number). Supplemental Table S3: 2nd- and 3rd-order polynomial root mean square error (RMSE) values for each value of dB hearing level for each gene at 250, 500, 1000, 2000, 4000, and 8000 Hz. Supplemental Table S4: Annual threshold deterioration (ATD) at each frequency and at the speech pure tone average (the average of 500, 1000, 2000, and 4000 Hz) for each gene and each available age bin, in dB/year.
439_2021_2424_MOESM2_ESM.tif
Supplementary file2 (TIF 385 KB) Supplemental Figure S1: Three-dimensional audioprofile surfaces of KCNQ4 (DFNA2) (A), GSDME (DFNA5) (B), WFS1 (DFNA6/14/38) (C), and COCH (DFNA9) (D) are fitted to third degree polynomials, with frequency in the x-axis, decibel hearing level on the y-axis, and age in the z-axis
Rights and permissions
About this article

Cite this article
Thorpe, R.K., Walls, W.D., Corrigan, R. et al. AudioGene: refining the natural history of KCNQ4, GSDME, WFS1, and COCH-associated hearing loss. Hum Genet 141, 877–887 (2022). https://doi.org/10.1007/s00439-021-02424-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-021-02424-7