
Abstract
Acanthamoeba keratitis (AK) is an infection that is mostly observed in contact lens wearers. It is often misdiagnosed causing delays in the administration of the correct treatment. The aim of this study was to report the outcome of clinical and molecular diagnosis of AK cases during the summer of 2019 in the southern region of Brazil. Three suspected cases of AK were discovered after an ophthalmic examination at a public hospital in the city of Porto Alegre. These cases were then confirmed through laboratory diagnosis (cell culture and molecular analysis by PCR and sequencing). In each of the three clinical sample cell cultures of corneal scraping and molecular analysis confirmed the presence of Acanthamoeba spp., all belonging to the morphological group II and to the genotype T4, which is the most common genotype associated with AK. In addition, Acanthamoeba spp. isolated from one of the clinical samples was found to harbor the Candidatus Paracaedibacter acanthamoeba, a bacterial endosymbiont. The presence of Ca. Paracaedibacter acanthamoeba in clinical isolates requires further research to reveal its possible role in the pathogenicity of Acanthamoeba infections.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acanthamoeba is a genus of free-living amoebae (FLA) widely distributed and isolated from water, soil, and air (Schuster and Visvesvara 2004). Trophozoites are the active stage of these microorganisms while the cysts are the resistance form (Khan 2006). Acanthamoeba spp. can cause diseases such as Granulomatous Amoebic Encephalitis, which affects the brain of immunosuppressed individuals, and Acanthamoeba Keratitis (AK), which is associated with healthy individuals, mostly contact lenses (CL) wearers (Khan 2006). Symptoms of AK include severe eye pain disproportionate to clinical signs, foreign body sensation, decreased vision, and photophobia (de Lacerda and Lira 2021). The gold standard diagnosis of AK is performed by amoeba isolation from corneal scraping followed by molecular analysis (Costa et al. 2017).
However, AK is often misdiagnosed clinically as herpes simplex or fungal infection (Padzik et al. 2018) which leads to a delay in correct diagnosis and treatment. Therefore, the disease can progress to a corneal transplant and lead to blindness when not treated properly (Lorenzo-Morales et al. 2013). The first reported case of Acanthamoeba spp. in CL wearers occurred in 1974 in England (Nagington et al. 1974). In Brazil, the first four cases occurred in 1988 (Nosé et al. 1988). Another study reported 28 cases of Acanthamoeba spp. from 1994 to 2016, in southern Brazil (Santos et al. 2018). The increased number of cases diagnosed every year is probably due to the popularization of CL, lack of hygiene and care, exposure to water, and ineffectiveness of solutions for disinfecting and cleaning them (Aguiar et al. 2013). Acanthamoeba spp. also serves as a reservoir for amoeba-resistant microorganisms (ARM), such as bacteria, viruses, and fungi, being considered the “Trojan horse” of the microbial world (Greub and Raoult 2004). The survival of these microorganisms within the FLA (endosymbionts) can enhance their virulence and pathogenicity (Guimarães et al. 2016; Müller et al. 2016). ARM are protected from biocides (disinfectants, multipurpose solutions for contact lenses, antiseptics, among others), especially if they are within the cysts (Balczun and Scheid 2017).
Some bacteria of the genus Pseudomonas increase the resistance of Acanthamoeba spp. to disinfection solutions by creating a biofilm on the surface of the CL thus increasing the retention of the amoebae (Iovieno et al. 2010). The aim of this study was to report the outcomes of clinical and molecular diagnosis of three cases of AK in patients treated at the Hospital de Clínicas de Porto Alegre (HCPA), RS, from January to March 2019.
Materials and methods
Informed consent
Three patients were interviewed and signed an informed consent (Supplementary Information) accepting to participate. The study had no potential risk and adhered to the tenets of the Declaration of Helsinki involving human research and was approved by the HCPA Research Ethics Committee, Opinion No. 1.405.611/CAEE: 47,915,215.2.0000.5327.
Morphological characterization of Acanthamoeba spp.
All three patients underwent corneal scraping. The material was collected at HCPA, using a swab, stored in saline solution, and kept refrigerated until the cultivation in the laboratory.
The corneal scrape content in saline solution was centrifuged at 1800 rpm for 10 min and transferred to plates with 1.5% non-nutrient agar (NNA) with a layer of Escherichia coli inactivated by heat for the monoxenic culture. The plates were incubated at 30 °C and observed for 15 days under an optical microscope for visualization of trophozoites and cysts.
The material was collected from the plates and placed into culture bottles with PYG medium (2% peptone protease, 0.2% yeast extract, and 1.8% glucose) supplemented with antibiotics (penicillin 100 U/mL and streptomycin 100 μg/mL) for axenic culture.
The morphological characterization of Acanthamoeba spp. was performed through the removal of the cysts from the plates of each clinical sample. An ocular micrometer scale was used under an optical microscope to measure 10 cysts of each clinical sample. The morphological characteristics of the trophozoites and cysts were analyzed (Page 1988), and the analysis of morphological groups I, II, and III was based on cyst size and shape (Khan 2006; Pussard and Pons 1977).
The detection of endosymbionts present in the Acanthamoeba spp. clinical samples was performed through fluorescence microscopy using an Olympus BX41 microscope (Olympus America) containing a filter for DAPI Sigma-Aldrich® (4′6′-diamidino-2-phenylindole dihydrochloride), with maximum absorption of 358 nm (Kapuscinski 1995).
Molecular diagnosis
The DNA extraction and purification from each patient sample and from positive control (a strain of ATCC 30,010 Acanthamoeba castellanii Neff) were performed using the Spin 50 ® Isolation DNA Kit (KASVI) according to the manufacturer’s instructions. The purified DNA was quantified using Nano Spectrophotometer (K23-0002-KASVI).
The detection by PCR of the Acanthamoeba spp. was performed using the set of primers JDP1 (5′-GGCCCAGATCGTTTACCGTGAA-3′) and JDP2 (5′-TCTCACAAGCTGCTAGGGAGTCA-3′), which amplify the ASA.S1 region of the 18S rDNA gene and are specific to the Acanthamoeba genus (Schroeder et al. 2001). The universal primers used for identification of ARM were FD1 (5′-AGAGTTTGATCCTGGCTCAG-3′) and RP2 (5′-ACGGCTACCTTGTTACGACTT-3′), which amplify the 16S rDNA of domain Bacteria (Weisburg et al. 1991).
The amplification reactions were performed in a final volume of 25 µL, containing 10 pmol of each primer, 2.5 mM of dNTPs, 50 mM of MgCl2, 2.5 µL of 10 × buffer and 1 U of Taq polymerase (Ludwig Biotec®). The PCR cycling parameters were set as follows: initial denaturation at 94 °C for 5 min, then 94 °C for 45 s, 60 °C for 40 s, and 72 °C for 1 min and 15 s, and a final extension at 72 °C for 5 min for 18S rDNA gene; and 94 °C for 5 min, then 94 °C for 45 s, 56 °C for 40 s and 72 °C for 1 min and 15 s, and a final extension at 72 °C for 5 min for 16S rDNA.
The electrophoresis of the amplicons was performed on a 1.2% agarose gel, and the PCR products were directly sequenced by the Sanger method using an ABI Prism 3500 Genetic Analyzer sequencer (Applied Biosystems). The chromatogram analysis and trimming of low-quality sequences were performed in Chromas 2.6.6 (http://technelysium.com.au). The forward and reverse sequences were aligned using ClustalW 2.1 (http://www.clustal.org/clustal2/), and the consensus sequences were refined using GeneDoc 2.7 (https://genedoc.software.informer.com/2.7/). The nucleotide sequences generated have been deposited in the Genbank database and were submitted to homology analysis using the NCBI BLAST program (http://www.ncbi.nlm.nih.gov/BLAST), with default parameters.
Nucleotide sequences from reference Acanthamoeba genotypes retrieved from NCBI GenBank were aligned using ClustalW 2.1. The phylogenetic relationship of the aligned sequences was determined using MEGA 7 (Kumar et al. 2018), using the neighbor-joining method, with 1000 bootstrap replications.
Results
Case reports
Case 1
In January 2019, a 24-year-old female sought medical treatment, reporting decreased vision, severe pain, eyelid swelling, redness, and irritation in her right eye. She had been wearing disposable soft CL for 18 months before her admission to the hospital. The patient used a multipurpose solution to clean her lenses, whose formulation had different chemical components, including biocides and surfactants. She reported that the saline solution used for rinsing was kept out of the refrigerator and without respecting the expiration date. The patient used to shower with her lenses on. She usually bought them at the ophthalmology office, however had already purchased them through the internet. Before the appointment at the hospital, the patient had already been treated with allergy ointments and eye drops for a month without clinical improvement. The biomicroscopy exam revealed central stromal infiltrate, signs of perineuritis, and intense conjunctival hyperemia (Fig. 1A).

Clinical signs of Acanthamoeba keratitis. A Eye with mild corneal central edema and perineuritis (patient 1); B central ring infiltrate with hypopium (patient 2); C dense ring infiltrates with great involvement of the central axis of the cornea (patient 3); D corneal transplant (patient 2). Photos: Diane Marinho (ophthalmologist). Original picture
After a corneal scraping, a specific topical treatment for Acanthamoeba spp. was started (chlorhexidine 0.02%, biguanide 0.02%, and brolene). This patient had a favorable clinic response, regaining her vision after 4 months of treatment, without needing a corneal transplant.
Case 2
In February 2019, a 23-year-old male, disposable soft CL wearer for 3 years, sought the ophthalmology service of the hospital. The patient reported pain in his left eye for at least 2 months. He used a multipurpose solution and also a saline solution that were stored outside the refrigerator for about 1 month. The patient reported that he wore lenses during bathing and showering and sometimes would not remove them to sleep. He often washed his lenses case with tap water without drying it, filled it with a multipurpose solution, and then stored the lens. The patient acquired his CL at the eye clinic. About 40 days before the consultation at the hospital, he had already been diagnosed with herpes simplex and started treatment with Aciclovir® without success. The patient complained of pain and irritation in his left eye. A biomicroscopy exam showed a central corneal infiltrate with edema, punctate keratitis, and retro-keratic precipitates (Fig. 1B). The treatment was performed with biguanide 0.02%, chlorhexidine 0.02%, and gatifloxacin 0.3% eye drops. In spite of the treatment, there was an appearance of hypopyon, worsening of the stromal ring infiltrate, and central thinning. The patient underwent a corneal transplant 30 days after the treatment (Fig. 1D). An anatomopathological exam of the graft confirmed AK. Specific treatment was maintained after 6 months of postoperative with no relapse of the disease in the graft. The patient had a complete visual acuity recovery.
Case 3
In March 2019, a 42-year-old male came to the hospital, reporting vision loss, photophobia, and irritation in both eyes during the last 15 days. His visual acuity was assessed by the counting fingers method in both eyes. He had been wearing disposable soft CL for 25 years and used only a multipurpose solution for cleaning and disinfecting his CL acquired in an optical shop. He used to shower while wearing CLs. A biomicroscopy exam revealed a bilateral central corneal infiltrate with a larger epithelial defect in his left eye (Fig. 1C). AK was suspected, and specific topical treatment was started with: brolene 0.1%, chlorhexidine 0.02%, and biguanide 0.02%, used every hour, in addition to gatifloxacin 0.3%. After more than 2 months of treatment, there were no signs of clinical improvement culminating in corneal transplantation in the left eye. An anatomopathological exam of the graft confirmed AK. The right eye had a favorable clinical response with the treatment. Although the corneal scraping in his right eye did not show AK, the patient continued the treatment for approximately 6 months until the total epithelization of the corneal ulcer. A corneal transplant, in his right eye, was performed 1 year after the infection to treat the residual corneal scar. Until the last follow-up visit, there was no relapse of the disease in both grafts, and the patient recovered his visual acuity in both eyes.
Acanthamoeba isolation and morphological characterization
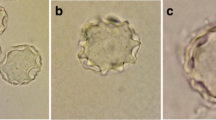
The isolation of Acanthamoeba spp. from corneal scraping allowed the detection of trophozoites (Fig. 2A and C), cysts (Fig. 2B), and endosymbionts (Fig. 2D) in the culture plates from patients 1 and 3 after 48 h. At this point, the culture plates from patient 2 were negative for the Acanthamoeba spp. In fact, the presence of trophozoites and cysts in the clinical sample from patient 2 was only possible through culture using the cornea directly after transplantation.

Morphological analysis of Acanthamoeba spp. A Trophozoite and B cyst culture of patient 1 at the optical microscopy (× 1000); C and D trophozoite carrying endosymbionts culture of patient 3 analyzed by optical microscopy (× 1000) and fluorescence microscopy (DAPI Sigma-Aldrich®), respectively. Scale bar 10 μm
The isolation of Acanthamoeba spp. of corneal scraping from patient 1 (Fig. 2A and B) and patient 3 (Fig. 2C and D) allowed the detection of trophozoites and cysts in the culture plates after 48 h.
The average size of measured cysts was 15.09, 15.86, and 15.02 μm from patients 1, 2, and 3, respectively, and presented endocyst of starry and triangular shapes according to the classification of morphological groups (Schroeder et al. 2001).
Molecular characterization of Acanthamoeba clinical isolates
The presence of Acanthamoeba spp. was detected in all three clinical samples, as demonstrated by the single strong band of 500 bp, generated after amplification of the ASA.S1 region of the 18S rDNA using a genus-specific set of primers (Fig. 3A).

Agarose gel electrophoresis of PCR products. In both agarose gels (1.2%), lane 1 indicates a molecular size marker; lanes 2 and 3: positive control (Acanthamoeba castelanii DNA for 18S and Escherichia coli DNA for 16S); and lane 10: negative control. A Amplicons obtained using specific primers for the Acanthamoeba genus. Lanes 4 and 5: patient 1; lanes 6 and 7: patient 2; lanes 8 and 9: patient 3. B Amplicons obtained using specific primers for the Bacteria domain. Lanes 4 and 5: patient 1; lanes 6 and 7: patient 3; lanes 8 and 9: patient 2. Lanes 2, 4, 6, and 8 are amplicons generated using 50 ng of DNA template, while lanes 3, 5, 7, and 9 are amplicons generated using 100 ng of a DNA template
The nucleotide sequences analyzed with the BLAST program revealed that the three clinical samples have the highest identities (99–100%) with Acanthamoeba 18S rDNA. The nucleotide sequence from patient 1 (MZ404337) was 100% (341/341), identical to the Acanthamoeba sequence MH100838 (E-value 2e-176, 100% query cover, and no gap). The nucleotide sequence from patient 2 (MZ404336) was 99.56% (455/457), identical to the Acanthamoeba sequence MN153014 (E-value 0.0, 100% query cover, and one gap). And the nucleotide sequence from patient 3 (MZ404332) was 99.78% (464/465), identical to the Acanthamoeba sequence MN153013 (E-value 0.0, 100% query cover, and one gap).
In order to determine the genotype of the three clinical isolates, a phylogenetic tree containing sequences from reference Acanthamoeba genotypes was constructed (Fig. 4). The three nucleotide sequences from the clinical samples were clustered with Acanthamoeba castellanii Neff ATCC 50,373 (U07416), which is typed as T4 genotype.

Phylogenetic relationship among the three AK clinical cases and reference Acanthamoeba genotypes. The 18S rDNA sequences from Acanthamoeba spp. were retrieved from the NCBI database. The phylogenetic tree was constructed using the neighbor-joining method, and the distances were computed using the maximum composite likelihood method. Bootstrap values (1000 replicates) are shown next to the branches
Molecular characterization of Acanthamoeba endosymbiont
The presence of a bacterial endosymbiont was detected only on patient 3 sample, as demonstrated by the single strong band of 1500 bp, generated after amplification of a fragment from 16S rDNA using bacteria domain set of primers (Fig. 3B). The nucleotide sequence from the bacterial endosymbiont detected on patient 3 sample (MZ409800) was also analyzed with the BLAST program and matched with bacterial 16S rDNA. This sequence was 99.51% (808/812), identical to the sequence registered in GenBank database CP008941 from Candidatus Paracaedibacter acanthamoebae (E-value 0.0, 100% query cover, and three gaps).
Discussion
The demand for CL has continually increased not only due to the growing prevalence of eye disorders but also due to the increasing popularity of their cosmetic use. Three AK patients reported in this study were soft CL wearers. Soft CL have some advantages over rigid ones, being easier to adjust and much more comfortable. However, cleaning and maintenance of soft CL are more laborious and may offer risks of eye infections if the wearers fail to clean, disinfect, and store them as recommended (Cope et al. 2017). Several studies show that the majority of wearers use soft CL (Gomes et al. 2016; Santos et al. 2018), and, consequently, they are more prone to eye complications and infections.
Proper cleaning of the CL and CL cases with a fresh multipurpose disinfecting solution is a basic hygiene habit to prevent eye infections (Santos et al. 2018). All patients from this study were using a multipurpose solution to clean their CL and storage cases, but this practice was not enough to avoid their AK infection. Although multipurpose solutions have many antimicrobial components, their effectiveness is limited (Lee et al. 2018). Indeed, a few bad hygiene habits were mentioned by the patients from this study. Concerning the saline solution used for CL rinsing, they reported that the solution was kept out of refrigeration and without respecting the expiration date. In relation to CL case care, it was reported that tap water was often used to wash the case without letting it dry, before storing the lenses with the multipurpose solution. These practices have been previously described as risk factors for AK (Brown et al. 2018; Steele and Szczotka-Flynn 2017). Therefore, greater care is needed in relation to the cleaning and maintenance of the CL and storage cases in order to avoid contamination. Three patients used to wear their lenses during showering and swimming. In addition to proper cleaning, other healthy habits that should be followed by CL wearers include not sleeping with the lenses and removing them before showering and swimming (Fabres et al. 2018). Besides, these cases were reported during the summer, a period in which people spend more time in swimming pools and beaches, forgetting the proper care in cleaning and disinfecting their lenses.
Two patients purchased their CL over the Internet or from unreliable providers, which places the individuals at higher risk of eye complications since they tend to participate in more risky behaviors concerning both cleaning and wearing habits. In addition, a decrease in eye examination frequency has been observed in individuals who have these purchasing practices, resulting in a significant delay between symptoms and medical care (Young et al. 2014; Mingo-Botín et al. 2020).
The clinical suspicion of AK takes into consideration the patient history, clinical signs, and symptoms (Khan 2006). Once clinical signs of AK are suspected, it is very important to proceed with laboratory diagnosis confirmation.
In this study, the cell culture of Acanthamoeba was the first step in the laboratory diagnosis. In the three clinical samples, Acanthamoeba spp. belonged to morphological group II, which includes most Acanthamoeba species responsible for meningoencephalitis and keratitis cases. In addition, this group of amoeba is commonly isolated from the environment, where many microorganisms can be phagocytosed and eventually become endosymbionts (Schroeder et al. 2001).
The molecular detection of Acanthamoeba was the second step in the laboratory diagnosis of the three clinical samples analyzed. Both PCR amplification and nucleotide analysis of the 18S rDNA gene corroborated the presence of Acanthamoeba spp. in all clinical samples. When possible, it is interesting to go even further in the etiologic agent characterization, determining it at the species level and especially its genotype. In this sense, the phylogenetic relationship analysis pointed out that the three clinical isolates were T4 genotype, as suggested by their clustering with Acanthamoeba castellanii Neff ATCC 50,373, which is well known as T4 genotype strain. The T4 genotype is the most commonly found in amoebic keratitis (Marciano-Cabral and Cabral 2003).
Another aspect that is interesting to investigate in AK confirmed cases is the potential presence of endosymbionts. The presence of bacterial endosymbionts was investigated in all three clinical samples, and it was only detected in the sample from patient 3. Interactions of free-living amoebae with microorganisms can benefit the protozoan, and many bacteria have developed strategies to resist phagocytosis, survive intracellularly, and multiply inside Acanthamoeba species (Souza et al. 2017).
The endosymbiont organisms can induce a change in the amoeba phenotype, contributing directly to the disease (Balczun and Scheid 2017). Molecular analysis identified the endosymbiont as Ca. Paracaedibacter acanthamoebae (Horn et al. 1999), which belongs to the Holosporales order (Alphaproteobacteria class), a group of intracellular parasites of eukaryotes (Muñoz-Gómez et al. 2019). Ca. Paracaedibacter acanthamoebae have been identified mostly in Acanthamoeba environmental isolates (Rayamajhee et al. 2021), and its clinical implication in Acanthamoeba infections has not been described so far. Although the exacerbation of AK in patient 3 was evident, leading to corneal transplantation in both eyes, the results obtained in this study are not enough to correlate the endosymbiont presence with the AK outcomes of this case. However, the presence of endosymbionts in Acanthamoeba spp. reveals the need for further research in order to elucidate the mechanisms involved in the interaction between the amoeba and its endosymbionts and the possible role in the pathogenicity of Acanthamoeba infections.
References
Balczun C, Scheid PL (2017) Free-living amoebae as hosts for and vectors of intracellular microorganisms with public health significance. Viruses 9(4):65. https://doi.org/10.3390/v9040065
Brown AC, Ross J, Jones DB, Collier SA, Ayers TL, Hoekstra RM, Backensen B, Roy SL, Beach MJ, Yoder JS (2018) Risk factors for Acanthamoeba keratitis—a multistate case–control study, 2008–2011. Eye Contact Lens 44:1–6. https://doi.org/10.1097/ICL.0000000000000365
Cope JR, Collier SA, Nethercut H, Jones JM, Yates K (2016) Yoder JS (2017) Risk behaviors for contact lens–related eye infections among adults and adolescents — United States. MMWR Morb Mortal Wkly Rep 66(32):841–845. https://doi.org/10.15585/mmwr.mm6632a2
Costa AO, Furst C, Rocha LO, Cirelli C, Cardoso CN, Neiva FS, Possamai CO, de Assis SD, Thomaz-Soccol V (2017) Molecular diagnosis of Acanthamoeba keratitis: evaluation in rat model and application in suspected human cases. Parasitol Res 116(4):1339–1344. https://doi.org/10.1007/s00436-017-5411-4
De Lacerda AG, Lira M (2021) Acanthamoeba keratitis: a review of biology, pathophysiology and epidemiology. Ophthalmic Physiol Opt 41(1):116–135. https://doi.org/10.1111/opo.12752
De Aguiar APC, Silveira CO, Winck MAT, Rott MB (2013) Susceptibility of Acanthamoeba to multipurpose lens-cleaning solutions. Acta Parasitol 58(3):304–308. https://doi.org/10.2478/s11686-013-0143-9
Fabres LF, Maschio VJ, Santos DL, Kwitko S, Marinho DR, Araújo BS, Locatelli CI, Rott MB (2018) Virulent T4 Acanthamoeba causing keratitis in Southern Brazil. Acta Parasitol 63(2):428–432. https://doi.org/10.1515/ap-2018-0050
Gomes TS, Magnet A, Izquierdo F, Vaccaro L, Redondo F, Bueno S, Sánchez ML, Angulo S, Fenoy S, Hurtado C, Del Aguila C (2016) Acanthamoeba spp in contact lenses from healthy individuals from Madrid Spain. PLoS One 11(4):e0154246. https://doi.org/10.1371/journal.pone.0154246
Greub G, Raoult D (2004) Microorganisms resistant to free-living amoebae. Clin Microbiol Rev 17(2):413–433. https://doi.org/10.1128/CMR.17.2.413-433.2004
Guimarães AJ, Gomes KX, Cortines JR, Peralta JM, Peralta RH (2016) Acanthamoeba spp as a universal host for pathogenic microorganisms: one bridge from environment to host virulence. Microbiol Res 193:30–38. https://doi.org/10.1016/j.micres.2016.08.001
Horn M, Fritsche TR, Gautom RK, Schleifer KH, Wagner M (1999) Novel bacterial endosymbionts of Acanthamoeba spp. related to the Paramecium caudatum symbiont Caedibacter caryophilus. Environ Microbiol 1(4):357–367. https://doi.org/10.1046/j.1462-2920.1999.00045.x
Iovieno A, Ledee DR, Miller D, Alfonso EC (2010) Detection of bacterial endosymbionts in clinical Acanthamoeba isolates. Ophthalmology 117(3):445–452. https://doi.org/10.1016/j.ophtha.2009.08.033
Kapuscinski J (1995) DAPI: a DNA-specific fluorescent probe. Biotech Histochem 70(5):220–233. https://doi.org/10.3109/10520299509108199
Khan NA (2006) Acanthamoeba: biology and increasing importance in human health. FEMS Microbiol Rev 30(4):564–595. https://doi.org/10.1111/j.1574-6976.2006.00023.x
Kumar S, Stecher G, Li M, Knyaz C, Tamura K (2018) MEGA X: Molecular evolutionary genetics analysis across computing platforms. Mol Biol Evol 35(6):1547–1549. https://doi.org/10.1093/molbev/msy096
Lee SM, Lee JE, Lee DI, Yu HS (2018) Adhesion of Acanthamoeba on cosmetic contact lenses. J Korean Med Sci 33(4):e26. https://doi.org/10.3346/jkms.2018.33.e26
Lorenzo-Morales J, Martin-Navarro CM, López-Arencibia A, Arnalich-Montiel F, Piñero JE, Valladares B (2013) Acanthamoeba keratitis: an emerging disease gathering importance worldwide? Trends Parasitol 29(4):181–187. https://doi.org/10.1016/j.pt.2013.01.006
Marciano-Cabral F, Cabral G (2003) Acanthamoeba spp. as agents of disease in humans. Clin. Microbiol. Rev. 16(2):273–307. https://doi.org/10.1128/CMR.16.2.273-307.2003
Mingo-Botín D, Zamora J, Arnalich-Montiel F, Muñoz-Negrete FJ (2020) Characteristics, behaviors, and awareness of contact lens wearers purchasing lenses over the Internet. Eye Contact Lens 46(4):208–213. https://doi.org/10.1097/ICL.0000000000000702
Müller A, Walochnik J, Wagner M, Schmitz-Esser S (2016) A clinical Acanthamoeba isolate harboring two distinct bacterial endosymbionts. Eur J Protistol 56:21–25. https://doi.org/10.1016/j.ejop.2016.04.002
Muñoz-Gómez SA, Hess S, Burger G, Lang BF, Susko E, Slamovits CH, Roger AJ (2019) An updated phylogeny of the Alphaproteobacteria reveals that the parasitic Rickettsiales and Holosporales have independent origins. Elife 8:e42535. https://doi.org/10.7554/eLife.42535
Nagington J, Watson PG, Playfair TJ, McGill J, Jones BR, Steele AD (1974) Amoebic infection of the eye. Lancet 2(7896):1537–1540. https://doi.org/10.1016/s0140-6736(74)90285-2
Nosé W, Sato EH, Freitas D, Ribeiro MP, Foronda AS, Kwitko S, Belfort R Jr, Burnier M Jr, Font R (1988) Úlcera de córnea por Acanthamoeba – Quatro primeiros casos do Brasil. Arq Bras Oftal 51(6):223–226
Padzik M, Hendiger EB, Chomicz L, Grodzik M, Szmidt M, Grobelny J, Lorenzo-Morales J (2018) Tannic acid-modified silver nanoparticles as a novel therapeutic agent against Acanthamoeba. Parasitol Res 117(11):3519–3525. https://doi.org/10.1007/s00436-018-6049-6
Page FC (1988) A new key to freshwater and soil amoebae. Sci Publ pp.122
Pussard M, Pons R (1977) Morphologie de la paroi kystique et taxonomie du genre Acanthamoeba (Protozoa, Amoebida). Protistologica 13:557–598
Rayamajhee B, Subedi D, Peguda HK, Willcox MD, Henriquez FL, Carnt N (2021) Systematic review of intracellular microorganisms within Acanthamoeba to understand potential impact for infection. Pathogens 10(2):225. https://doi.org/10.3390/pathogens10020225
Santos DL, Kwitko S, Marinho DR, de Araújo BS, Locatelli CI, Rott MB (2018) Acanthamoeba keratitis in Porto Alegre (southern Brazil): 28 cases and risk factors. Parasitol Res 117(3):747–750. https://doi.org/10.1007/s00436-017-5745-y
Schroeder JM, Booton GC, Hay J, Niszl IA, Seal DV, Markus MB, Fuerst PA, Byers TJ (2001) Use of subgenic 18S ribosomal DNA PCR and sequencing for genus and genotype identification of Acanthamoebae from humans with keratitis and from sewage sludge. J Clin Microbiol 39(5):1903–1911. https://doi.org/10.1128/JCM.39.5.1903-1911.2001
Schuster FL, Visvesvara GS (2004) Free-living amoebae as opportunistic and non-opportunistic pathogens of humans and animals. Int J Parasitol 34(9):1001–102. https://doi.org/10.1016/j.ijpara.2004.06.004
Souza TK, Soares SS, Benitez LB, Rott MB (2017) Interaction between methicillin-resistant Staphylococcus aureus (MRSA) and Acanthamoeba polyphaga. Curr Microbiol 74(5):541–549. https://doi.org/10.1007/s00284-017-1196-z
Steele KR, Szczotka-Flynn L (2017) Epidemiology of contact lens-induced infiltrates: an updated review. Clin Exp Optom 100(5):473–481. https://doi.org/10.1111/cxo.12598
Weisburg WG, Barns SM, Pelletier DA, Lane DJ (1991) 16S ribosomal DNA amplification for phylogenetic study. J Bacteriol 173(2):697–703. https://doi.org/10.1128/jb.173.2.697-703.1991
Young G, Young AG, Lakkis C (2014) Review of complications associated with contact lenses from unregulated sources of supply. Eye Contact Lens 40(1):58–64. https://doi.org/10.1097/ICL.0b013e3182a70ef7
Acknowledgements
The authors are grateful to the staff of the Department of Microbiology, Immunology and Parasitology of the Universidade Federal do Rio Grande do Sul and the Ophthalmology Department of the Hospital de Clínicas de Porto Alegre (HCPA) for their assistance.
Funding
The authors are grateful to the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and Fundo de Incentivo à Pesquisa e Eventos (FIPE/HCPA) for the financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Section Editor: Sutherland Maciver
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
dos Santos, D.L., Virginio, V.G., Berté, F.K. et al. Clinical and molecular diagnosis of Acanthamoeba keratitis in contact lens wearers in southern Brazil reveals the presence of an endosymbiont. Parasitol Res 121, 1447–1454 (2022). https://doi.org/10.1007/s00436-022-07474-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00436-022-07474-y