
Abstract
Purpose
The lack of prognostic data impedes implementation of optimal therapy for cervical cancer. For instance, recommended therapy for FIGO IIB cervical cancer is radical hysterectomy or radiochemotherapy. To enlighten different therapeutic approaches, we investigated the benefit of individual therapies or combination thereof in patients with or without infested lymph nodes.
Methods
The German Tumor Centre Regensburg registered 389 patients with FIGO IIB, IIIA, IIIB, and IVA cervical cancer between 2002 and 2015. We estimated hazard ratios (HR) for overall survival against different therapies using univariable and multivariable cox regression. After risk adjustment with respect to clinicopathological parameters, we performed model selection using conditional stepwise reverse selection.
Results
We demonstrated the need for thorough assessment of the nodal status to obtain reliable data for treatment strategy. Our analysis showed significant differences for overall survival in FIGO IIB depending on therapy and nodal status. Outcome was inferior with radiochemotherapy without surgery for patients with N0 compared to surgery and radiochemotherapy combined (HR 3.012; 95% CI 1.075–8.441; p = 0.036); however, for N1, radiochemotherapy without surgery resulted in comparable outcome (HR 0.808; 95% CI 0.189–3.403; p = 0.765), whereas surgery alone yielded in poor outcome (HR 2.889; 95% CI 1.356–6.156; p = 0.006). Regardless of the nodal status, chemotherapy was superior in advanced stage cervical cancer FIGO III to IVA.
Conclusions
Our study suggests that in terms of oncological outcome FIGO IIB cervical cancer patients benefit from a combination of surgery and radiochemotherapy. However, in the presence of lymph node infestation, surgery does not add substantial benefit to the patient.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Globally, cervical cancer is the fourth-most common cause of cancer-related death in women (Vu et al. 2018). In the Western world, organized vaccination and screening programs decreased the cervical cancer incidence (Mendes et al. 2018); however, it remains a significant concern for public health and, hence, improvements in diagnostic and therapy are required (Marshall et al. 2018; Ogilvie et al. 2017; Parkhurst and Vulimiri 2013).
The decreasing incidence rate of cervical cancer in the Western world limits availability of data that provides insight into the success of different disease management strategies. In particular, there is a lack of prognostic data regarding optimal therapy. In Germany, current recommendation for patients with advanced cervical cancer indicates no preference for either surgery or radiochemical intervention (Leitlinienprogramm Onkologie 2014). Furthermore, there are no reliable data for the effectiveness of combination therapy. Nevertheless, there is sufficient data suggesting that the combination of radical hysterectomy and radiotherapy is associated with higher morbidity compared to solely surgical intervention (Leitlinienprogramm Onkologie 2014).
Currently, only one single study compares different treatment modalities in cervical cancer in a prospective randomized setting (Landoni et al. 1997); however, high numbers of R1 and R2 resections in the patient cohort that received surgery limits the significance of this study.
Another important prognostic parameter is lymph node involvement in cervical cancer. Pelvic lymphadenectomy is a standard procedure as part of radical hysterectomy and correlates with improved survival in early stage cervical cancer; however, the FIGO guideline for clinical staging currently does not consider the nodal status (Cheng-Yen et al. 2018a, b).
To address this lack of clinically relevant information concerning optimal therapy, we conducted a retrospective study on female patients diagnosed with advanced stage cervical cancer, and focused on the nodal status as a prognostic factor for therapy and outcome.
Patients and methods
Study design and data source
We accessed the patient database of the clinical cancer registry from Tumor Centre Regensburg (Bavaria, Germany), which has been described elsewhere (Papathemelis et al. 2017, 2018). Our data source contained 1613 cases of female patients from Upper Palatinate or Lower Bavaria who were diagnosed with cervical carcinoma (ICD-10 C53), and registered to the database between January 2002 and December 2015.
Patient inclusion and exclusion criteria
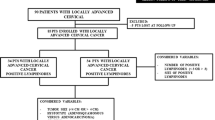
The database of the cancer registry contained 1613 female patients who were diagnosed with cervical cancer. For this study, we included only cases of advanced stage cancer, defined by the FIGO stage and, hence, selected 446 patients with the stages FIGO IIB to FIGO IVA. We selected the type of cancer as an additional inclusion requirement and limited our study cohort to squamous cell carcinomas, adenocarcinoma, and adenosquamous carcinoma. Therefore, we excluded 18 cases of neuroendocrine carcinomas and Mixed Müllerian tumors. Further, we only considered cases of primary tumors, reducing the cohort size to 411 patients. We also excluded cases with previous, simultaneous and synchronous secondary malignant neoplasms. Finally, we only included patients with sufficient follow-up data, yielding in a patient cohort of 389 females (Fig. 1).

Flow-chart depicting exclusion and inclusion criteria of study group
Statistical analysis
Categorical data were expressed as frequency counts and percentages, whereas continuous data were expressed as means, range and standard deviation.
Chi-square test was used for comparisons between individual categorical variables. Overall survival was calculated from the date of cancer diagnosis to the date of death from any cause. Recurrence free survival includes local relapse, as well as subsequent regional and distant metastases. Vital status of all patients was validated using death certificates and information from registration offices. All patient data were maintained according to national and European legislation, and was anonymised for the purpose of this study.
To estimate hazard ratios (HR) for overall and recurrence free survival, univariable and multivariable Cox regression analyses were applied to compare patients according to selected features. Risk-adjustment was performed in multivariable analyses to adjust for confounding factors: age at diagnosis, comorbidity, known cancer in family, histology, grading, FIGO state, and nodal status. Comorbidity was adjusted via Charlson-Comorbidity-Index, categorized in a group with at least one disease and a group without any disease listed in the CCI list (Charlson et al. 1987). Model selection in multivariable Cox regression was performed using conditional stepwise reverse selection. Hazard ratios were considered significant if the corresponding confidence interval (CI) excluded 1, and the p value of the log-rank test was < 0.05. All analyses were performed using IBM SPSS Statistics Version 25.0 (Chicago, EUA).
Results
Characterization of patient cohort
We selected 389 patients from 1613 patients with cervical cancer registered in the database of the Tumor Center Regensburg in Germany (Fig. 1). The majority of the selected patients with FIGO stage IIB–IVA were between 40 and 80 years old (Table 1), with mean age at diagnosis of 57.2 years (median 55.2). The majority did not exceed a score of 2 on the Charlson-Comorbidity-Index (83.3%), meaning they suffered from no other illness than cervix cancer, and did not experience cancer in their family history (88.9%). Most of the patients were diagnosed with squamous cell carcinomas (82.3%) but our cohort also included some cases of adenocarcinoma (14.7%), and a few cases of adenosquamous carcinoma (3.1%). Cancer grading indicated that almost all patients had either G2 (42. 7%) or G3 (54.5%) cancer, whereas less than 3% of the cases were graded either lower or higher or not at all. The nodal status was assessed as N0 in 38.3% and as N1 in 42.7% of all the cases. In the majority of the cases positive lymph node status was assessed by surgical means. For the remaining 19.0%, no data could be retrieved. About half of all cases were classified as FIGO IIB (53.2%), whereas the other half was almost equally distributed among FIGO IIIA, IIIB and IVA.
We focused on patients with advanced cervical cancer classified as FIGO IIB. The majority of all patients in this stage underwent radical hysterectomy and systematic lymphadenectomy followed by additional treatments (Table 2). Among the patients classified with FIGO IIB, 48.7% received both radiotherapy and chemotherapy, 14.2% received only radiotherapy and 19.3% received no further treatment. The remaining patients (17. 8%) did not undergo surgery but received either both radio- and chemotherapy (12.7%) or radiotherapy only (5.1%).
Accuracy of nodal status evaluation increases with number of dissected lymph nodes
A large body of research indicated that the infestation of lymph nodes could provide valuable diagnostic and prospective insights into diseases progression and outcome for cervical cancer (Du et al. 2018). To assess the relevance of the nodal status for patients with FIGO IIB cervical cancer, we first aimed to address the accuracy of determining lymph node infestation.
We evaluated the number of analyzed lymph nodes per patient for each of the category of nodal status, i.e. no infestation (N0), infestation (N1) or unknown status (NX) (Table 3). We found that the fraction of patients with a lymph node infestation increases when more lymph nodes were dissected and analyzed.
Combination of surgery and radiochemotherapy is superior in FIGO IIB cervical cancer without lymph node infestation
Next, we sought out to interrogate the contribution of the lymph node status to overall survival for patients diagnosed with FIGO IIB cervical cancer. In our cohort, we identified 93 females (47.2%) without infested lymph nodes (i.e. N0) (Fig. 2). We performed univariable and multivariable analysis to evaluate the effect of the applied clinical intervention on the overall survival for this subgroup (Table S1). Interestingly, we found statistically significant differences among the chosen treatment modalities. Our data show that a combination of surgery, radio- and chemotherapy, used as reference in multivariable Cox-regression analysis results in the highest overall survival, whereas the combination of radio- and chemotherapy without surgery, yielded in the lowest survival (HR 3.012; 95% CI 1.075–8.441; p = 0.036). Furthermore, we also confirmed this result for recurrence free survival (Table S2; Fig. 2).

Kaplan–Meier plot for overall survival of patients with FIGO IIB cervical cancer depending on clinical intervention in patients without infested Iymphnodes N0 (a) and with infested lymphnodes N1 (b)
Surgery is not beneficial in FIGO IIB cervical cancer with lymph node infestation
We continued and expanded our analysis to the 91 patients (46.2%) in our FIGO IIB cohort with lymph node infestation (i.e. N1). As before, we performed univariable and multivariable regression analysis evaluating the impact of therapy on overall survival (Table 1). Again, we found in this subgroup that a combination of surgery, radio- and chemotherapy yielded the superior overall survival. Remarkably, radio- and chemotherapy without surgery was as effective (HR 0.808; 95% CI 0.189–3.403; p = 0.765). In contrast, radical surgery alone significantly decreased the overall survival (HR 2.889; 95% CI 1.356–6.156; p = 0.006). Again, these results were confirmed when recurrence free survival was analyzed as outcome variable (Table S2).
Chemotherapy is associated with superior overall survival in late stage cervical cancer
In addition to patients with FIGO IIB cervical cancer, we also investigated the correlation of overall survival and lymph node status in patients who were diagnosed with FIGO IIIA, FIGO IIIB, and FIGO IVA cervical cancer (Table S3). Our data shows that the selected treatment was associated with different overall survival outcomes of the patient depending on the nodal status (N0, N1 or NX) (Table S4). Additional analysis revealed that for late stage cervical cancer, chemotherapy provides the best perspectives for survival (Fig. S1). Significant benefit for overall survival was achieved in nodal positive patients with HR 0.319 (95% CI 0.149–0.683; p = 0.003), the effect for N0 patients was smaller and non-significant with HR 0.560 (95% CI 0.274–1.146; p = 0.113).
Discussion
Despite the high prevalence of cervical cancer, prognostic data are very limited and, hence, treatment recommendations are based often on consensus and not evidence (Leitlinienprogramm Onkologie 2014). In this study, we provide important evidence concerning the choice of therapy on advanced and late stage cancer depending on the nodal status of the patient.
The patients in our study underwent partial or systematic pelvic lymph node dissection permitting assessment of the nodal status. We could demonstrate that larger numbers of dissected lymph nodes increase the likelihood to identify lymph node infestation. We also show that nodal status has implications for therapy and outcome in cervical cancer. Consequently, we argue that accurate assessment of the nodal status is important and should be considered for staging of cervical cancer. Nevertheless, it is unclear whether there is minimal amount of dissected lymph nodes to assess correctly the nodal status of the patient. This is also relevant in light towards the current shift in clinical practice to replace systematic pelvic lymph node dissection with sentinel lymph nodes biopsy (Cibula and McCluggage 2018; Cibula et al. 2012).
The lymph node status in our cohort study was mainly assessed via surgery. When no surgical intervention took place at all, the lymph node status was assessed non invasively by CT and/or MRI scans. It is true that this might be the second best procedure behind histopathological evaluation of lymph nodes, nevertheless the sensitivity of CT and MRI as a diagnostic modality for detecting nodal metastasis varies from 60 to 88% with specificity as high as 97% (Selman et al. 2008; Choi et al. 2010; Balleyguier et al. 2011). In line with the value of these diagnostic modalities and according to the latest FIGO Committee report, imaging or pathological findings may be used to assess retroperitoneal lymph nodes (Bhatla et al. 2019).
Our retrospective analysis showed that certain therapy choices are more beneficial for overall survival than others. In the presence of lymph node infestation, surgery does not provide substantial benefit to the patient anymore, and radiochemotherapy is as good as a combination of all three therapies. This could have implications in future treatment strategies concerning cervical cancer. Taking in consideration the relative high morbidity associated with surgery, the lack of benefit suggests that therapy should exclude surgery for this patient subgroup and only apply radiochemotherapy. We are aware that this conclusion is premature, and we argue that additional studies and analysis are required to validate and substantiate our observation.
In addition, our study implies that chemotherapy is associated with superior outcome for patients with late stage cervical cancer. A limitation is the relative low number of patients with FIGO IIIA, FIGO IIIB and FIGO IVA in our cohort. Consequently, we combined all these subgroups during statistical analysis and, hence, cannot exclude that different chemotherapy might benefit one subgroup but not another.
Taken together, we provide evidence for the benefit of radiochemotherapy and surgery for FIGO IIB cervical cancer patients depending on their nodal status. Further, we provide indication for the benefit of chemotherapy in late stage cervical cancer. Our study can only be one of the first steps towards better patient care. More clinical data is needed to identify the best possible treatment strategy for cervical cancer patients.
References
Balleyguier C, Sala E, Da Cunha T, Bergman A, Brkljacic B, Danza F (2011) Staging of uterine cervical cancer with MRI: guidelines of the European Society of Urogenital Radiology. Eur Radiol 21:1102–1110
Bhatla N, Berek JS, Cuello Fredes M, Denny LA, Grenman S, Karunaratne K, Kehoe ST, Konishi I, Olawaiye AB, Prat J, Sankaranarayanan R, Brierley J, Mutch D, Querleu D, Cibula D, Quinn M, Botha H, Sigurd L, Rice L, Ryu HS, Ngan H, Mäenpää J, Andrijono A, Purwoto G, Maheshwari A, Bafna UD, Plante M, Natarajan J (2019) Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet J. https://doi.org/10.1002/ijgo.12749 (Epub ahead of print)
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Cheng-Yen Lai J, Lai KJ, Yi-Yung Yu E, Hung ST, Chu CY, Wang KL (2018a) Sentinel lymphatic mapping among women with early-stage cervical cancer: a systematic review. Taiwan J Obstet Gynecol 57:636–643
Cheng-Yen Lai J, Yang MS, Lu KW, Yu L, Liou WZ, Wang KL (2018b) The role of sentinel lymph node biopsy in early-stage cervical cancer: a systematic review. Taiwan J Obstet Gynecol 57:627–635
Choi H, Ju W, Myung SK, Kim Y (2010) Diagnostic performance of CT, MRI, and PET or PET/CT for detection of metastatic lymph nodes in patients with cervical cancer: meta-analysis. Cancer Sci 101:1471–1479
Cibula D, McCluggage WG (2018) Sentinel lymph node (SLN) concept in cervical cancer: current limitations and unanswered questions. Gynecol Oncol. https://doi.org/10.1016/j.ygyno.2018.10.007
Cibula D, Abu-Rustum NR, Dusek L et al (2012) Prognostic significance of low volume sentinel lymph node disease in early-stage cervical cancer. Gynecol Oncol 124:496–501
Du R, Li L, Ma S, Tan X, Zhong S, Wu M (2018) Lymph nodes metastasis in cervical cancer: incidences, risk factors, consequences and imaging evaluations. Asia Pac J Clin Oncol 14:e380–e385
Landoni F, Maneo A, Colombo A, Placa F, Milani R, Perego P, Favini G, Ferri L, Mangioni C (1997) Randomised study of radical surgery versus radiotherapy for stage Ib–IIa cervical cancer. Lancet 350:535–540
Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF) (2014) S3-Leitlinie Diagnostik, Therapie und Nachsorge der Patientin mit Zervixkarzinom, Langversion, 1.0, 2014, AWMF-Registernummer: 032/033OL. http://leitlinienprogramm-onkologie.de/Leitlinien.7.0.html. Accessed 22 Nov 2018
Marshall C, Rajdev MA, Somarouthu B, Ramaiya NH, Alessandrino F (2018) Overview of systemic treatment in recurrent and advanced cervical cancer: a primer for radiologists. Abdom Radiol. https://doi.org/10.1007/s00261-018-1797-4
Mendes D, Mesher D, Pista A, Baguelin M, Jit M (2018) Understanding differences in cervical cancer incidence in Western Europe: comparing Portugal and England. Eur J Public Health 28:343–347
Ogilvie G, Nakisige C, Huh WK, Mehrotra R, Franco EL, Jeronimo J (2017) Optimizing secondary prevention of cervical cancer: recent advances and future challenges. Int J Gynecol Obstet 138:15–19
Papathemelis T, Scharl S, Kronberger K, Gerken M, Scharl A, Pauer A, Klinkhammer-Schalke M (2017) Survival benefit of pelvic and paraaortic lymphadenectomy in high-grade endometrial carcinoma: a retrospective population-based cohort analysis. J Cancer Res Clin Oncol 143:2555–2562
Papathemelis T, Hassas D, Gerken M, Klinkhammer-Schalke M, Scharl A, Lux MP, Beckmann MW, Scharl S (2018) Is there a benefit of lymphadenectomy for overall and recurrence-free survival in type I FIGO IB G1-2 endometrial carcinoma? A retrospective population-based cohort analysis. J Cancer Res Clin Oncol 144:2019–2027
Parkhurst JO, Vulimiri M (2013) Cervical cancer and the global health agenda: Insights from multiple policy-analysis frameworks. Global Public Health 8:1093–1108
Selman TJ, Mann C, Zamora J, Appleyard TL, Khan K (2008) Diagnostic accuracy of tests for lymph node status in primary cervical cancer: a systematic review and metaanalysis. CMAJ 178:855–862
Vu M, Yu J, Awolude OA, Chuang L (2018) Cervical cancer worldwide. Curr Probl Cancer. https://doi.org/10.1016/j.currproblcancer.2018.06.003
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Papathemelis, T., Knobloch, S., Gerken, M. et al. Impact of nodal status and treatment strategy on overall survival in advanced stage cervical cancer. J Cancer Res Clin Oncol 145, 1369–1376 (2019). https://doi.org/10.1007/s00432-019-02890-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-019-02890-7