
Abstract
Purpose
Some medical treatment for metastatic colorectal cancer (CRC) may have marginal survival benefit, but cause toxicities. The purpose of this study is to determine metastatic CRC patients’ tradeoffs in making a decision to undergo new medical treatment.
Methods
We conducted a survey of patients with a diagnosis of advanced CRC who were currently receiving or completed one chemotherapy regimen. First, patients were asked to rate the importance of 15 medical treatment-related adverse events that may arise as a consequence of chemotherapy or biological therapy in their treatment decision-making. Then, the patient identified his or her top five most important events and solicited preferences in hypothetical metastatic CRC treatment vignettes using the standard gamble technique.
Results
A total of 107 patients responded to the survey. From the list of medical treatment-related adverse events, patients identified clinically serious ones such as stroke, heart attack, and gastrointestinal perforation as the most important in their medical treatment decision-making, yet placed lower willingness to tolerate symptom-related events such as pain, fatigue, and depression. Generally, patients who were older, stage III versus IV and who had prior radiotherapy, lower educational attainment, and lower household income (all p <0.05) were less willing to tolerate any medical treatment-related adverse events after adjusting for other demographic and clinical characteristics.
Conclusions
Variations in patients’ willingness to tolerate different treatment-related adverse events underscore the need for improved communications between physicians and patients about the risks and benefits of their medical treatment, which helps make a more personalized decision for metastatic CRC treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Medical treatment decisions in advanced cancers including metastatic colorectal cancer (CRC) are complex. Survival time may not be the single most important outcome considered when initiating treatment because the disease cannot be cured, and the potential for extending survival has significantly improved, but is still limited (Leighl et al. 2004; Kaldjian et al. 2008; Wright et al. 2008). Randomized clinical trials show a statistically significant extension of survival by 2–5 months on average for these new metastatic CRC agents individually, and together might add up to a 1–2-year improvement in survival (Hurwitz et al. 2004; Ramlau et al. 2012; Grothey et al. 2013). Many patients with advanced CRC often choose to pursue aggressive treatment (Hurwitz et al. 2004; Leighl et al. 2011), even when their chance of improvement in survival can be small by such a treatment (Prigerson et al. 2015; O’Connor et al. 1999; Zafar et al. 2013). These patients appear willing to take additional risks of adverse events from receiving aggressive medical treatment, but prior research suggests that many patients overestimate treatment benefit or underestimate risks of adverse events (Weeks et al. 2012).
For metastatic CRC, medical treatment-related adverse events include acute but temporary effects, such as nausea and vomiting or skin rashes, to more serious adverse events including cardiovascular toxicities or gastrointestinal (GI) perforation, both shown to lower quality-of-life and overall survival (Semenza 2008; Galfrascoli et al. 2011; Choueiri et al. 2011). Given these risks combined with uncertain benefits of medical treatment (chemotherapy or biological therapy), advanced cancer patients and their clinicians face significant uncertainty in how best to manage their disease and its symptoms, and minimize adverse events in the real world before taking into account factors such as patient age, past treatment experience, and patient preferences.
Ideally, treatment decisions should balance risks and benefits while reflecting patients’ personal preference and value (CMS 2014). Most patients and their families desire detailed information about cancer treatment options, but are often overwhelmed by the information provided (Leighl et al. 2004; Harris 1998; Audrey et al. 2008). This requires improved (optimized) patient–physician communication regarding the likely treatment benefits and risks, usually for those with advanced cancer about therapies that often have small survival benefits (Audrey et al. 2008; Gattellari et al. 2001; Street and Voigt 1997). We need to develop new tools that accurately convey the risks efficiently. A substantial proportion of advanced cancer patients either do not receive a comprehensive and individualized explanation of these risk–benefit tradeoffs, or do not fully understand them (Arora et al. 2008). These decisions are further complicated by limited or absent communication about palliative care and end-of-life issues (Epner and Baile 2014; Laryionava et al. 2015; Walling et al. 2008). In order to develop a better tool, we evaluated patients’ willingness to undergo medical treatment given the risks of experiencing various treatment-related adverse events that may arise as a consequence of chemotherapy or biological therapy for their metastatic CRC. This is the first step in our research agenda to improve the understanding patients have of the risks and benefit tradeoffs of the metastatic CRC treatment.
Materials and methods
Eligible patients
Patients diagnosed with advanced CRC [tumor–node–metastasis (TNM) system stage III or IV] (Edge SB et al. 2010) who were receiving or had completed at least one chemotherapy regimen were eligible for this study. Patients were recruited at the Ruesch Center for the Cure of GI Cancers from Georgetown University Lombardi Comprehensive Cancer Center (LCCC). Potential participants were identified by LCCC’s Non-Therapeutic Subject Registry (NTSR), which provides centralized patient recruitment services for non-therapeutic clinical treatment studies. NTSR implements a universal protocol and patient consent that includes collection of sociodemographic information. Interested patients who completed the NTSR protocol, and who met the study’s eligibility criteria, were then contacted, consented, and enrolled by study research staff. Enrolled participants completed a study-specific electronic survey. This study was approved by the MedStar Health Research Institute-Georgetown University Oncology Institutional Review Board #2013-0026.
Survey overview
Survey development began with formative work involving qualitative interviews with patients and medical oncologists, team input, and finally cognitive testing with additional patients. Cognitive testing was used to refine the hypothetical health scenarios within the survey. The final, web-based survey was conducted by trained research staff either in person using a tablet device when patients were visiting the clinic, or via phone for patients with computer and internet access to the survey. The survey was designed to measure patient preferences for 15 treatment-related adverse events that may arise as a consequence of chemotherapy or biological therapy for metastatic CRC.
Survey design
The survey consisted of two parts, with the second part determined by responses on the first. In the first part, patients were asked to rate the importance (on a 4-level Likert scale: not important, somewhat important, very important, or extremely important) of 15 treatment-related adverse events in their medical treatment decision-making, and to indicate whether or not they have ever experienced each. The list of 15 specific medical treatment-related adverse events included cardiovascular-related events (stroke, heart attack), GI perforation, and other adverse events related to common GI chemotherapy and biological therapy including depression, fatigue, hypertension, neuropathy, blood clot in lung or legs, bleeding (coughing up blood, stomach or nose bleeds), nausea/vomiting, diarrhea, pain, fatigue, hair loss, rash and skin change, and sexual function issues. These adverse events were described by trained interviewers (in person or by phone) who employed key words and short phrases to convey information concerning specific areas of morbidity (Ness et al. 1999; Ness et al. 1998).
In the second part of the survey, the web-based program selected only those treatment-related adverse events that were rated “somewhat important” to “extremely important” by the respondent, who was then asked to identify the top five most important events from this sub-list in their medical treatment decision-making. Then, using a series of hypothetical vignettes for these top five adverse events, patients responded to individual standard gamble items. The standard gamble technique we employed was based on formative data and participant feedback during the cognitive interviews, following prior studies (Torrance 1987; Ross et al. 2003). In this technique, patients were asked to compare a described adverse event to a gamble in which there is a probability “p” of living in full health or probability “1 − p” of immediate death. The value of “p” at which a patient is indifferent between the two options (gamble vs. living in the described outcome state) becomes the preference assigned to that treatment-related adverse event. Preference scores elicited from standard gamble range between 0 (representing death) and 1 (representing full health).
In the survey, participants reported socioeconomic and demographic characteristics including age, sex, race/ethnicity, marital status, level of education, employment status, health insurance, and household income level. Clinical variables extracted from patient medical records included date of cancer diagnosis, cancer stage, prior treatment (surgery, radiation), and currently receiving chemotherapy (yes/no).
Statistical analysis
For each of the treatment-related adverse events, we compared preference scores between patients diagnosed with CRC stages III and IV to identify differences. Ordinary least square (OLS) regressions were used to evaluate the effects of demographic and clinical variables on patient preference scores for all medical treatment-related adverse events, controlling for other characteristics in the regression model. We conducted subgroup analyses stratifying by age group (30–64 and 65–84 years) and stage (III, IV) to identify the variability in preferences across these strata. Result differences with p value <0.05 were considered statistically significant.
Results
A total of 107 participants completed the survey. Patient demographic characteristics are shown in Table 1. The mean (±SD) age was 57 (±12.5), and half of the sample was female. Three-quarters had college degrees or higher, and more than half had an annual household income of $100,000 or higher. Only two patients reported no health insurance. Approximately half of the sample was currently receiving chemotherapy.
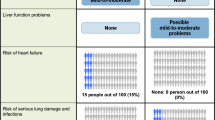
Patients identified more clinically serious adverse events as important factors in their medical treatment decision-making (Fig. 1). Specifically, between 78–80 % of participants rated stroke, heart attack, GI perforation, and blood clot in lungs or legs as “very important” or “extremely important” in deciding a medical treatment regimen for metastatic CRC. Other treatment-related adverse events were rated either “very important” or “extremely important” by at least a quarter of patients, ranging from 62 % [bleeding (coughing up blood, stomach or nose bleeds)] to 26 % (hair loss).

Percent of advanced colorectal cancer patients who rated various medical treatment-related adverse events as either very or extremely important to their treatment decision-making
The top five treatment-related adverse events chosen by patients followed closely to the most frequently endorsed “important” adverse events (Table 2). Rankings were relatively similar among patients diagnosed with stage III and IV. Fewer patients reported ever experiencing clinically serious adverse events (e.g., stroke, heart attack, GI perforation) than other adverse events that are not as clinically serious (e.g., nausea, diarrhea, fatigue). The most often experienced treatment-related adverse events were neuropathy (79 %), fatigue (79 %), and diarrhea (72 %).
Table 3 lists average patient preference scores on treatment-related adverse events for all patients and by stage at diagnosis. Lower preference scores represent less willingness to tolerate such an adverse event and thus lower preferences for medical treatment that may cause this event. Overall, patients were less willing to tolerate non-acute, less clinically serious adverse events that are likely more symptom-related and more related to long-term functional ability and overall quality-of-life such as depression (0.68), fatigue (0.71), and pain (0.66) (all ranges between 0 and 1). Among them, stage III patients reported lower, but not statistically significantly different willingness to tolerate these adverse events compared to patients with stage IV disease (depression 0.50 vs. 0.75; fatigue 0.52 vs. 0.81; pain 0.48 vs. 0.78). Preference scores of previously experienced adverse events, on average, were not statistically different from those that were not experienced (0.76 vs. 0.80).
Our multivariable analysis of willingness to tolerate any treatment-related adverse events is shown in Table 4. We found that older age (−0.03 per 10 years, p < 0.01) and prior radiotherapy (−0.10, p < 0.0001) were associated with patients’ being less willing to tolerate adverse events due to medical treatment after adjusting for other demographic and clinical variables. Greater willingness to tolerate treatment-related adverse events was associated with higher education (0.08 for college degree or higher compared to lower than college degree, p < 0.01), higher household income (0.05 for $100 K or more compared to <$100 K, p < 0.05), and stage IV disease (relative to stage III disease 0.06, p < 0.05).
Subgroup analysis (data not shown) identified similar effects on lower education, prior radiotherapy, and stage III disease among patients <65 years old (significantly associated with less willingness to tolerate treatment-related adverse events), while only prior radiotherapy remained significant among patients ≥65 years old. Among patients with stage III disease, older age and prior radiotherapy remained significantly associated with less willingness to tolerate treatment-related adverse events, whereas lower education, lower income, and prior radiotherapy remained significant among those with stage IV disease.
Discussion
Our study found that patients with advanced CRC prioritize clinically severe, less likely medical treatment-related adverse events, but report being less willing to tolerate more common, symptom-related adverse events when making medical treatment decisions on their metastatic CRC. Patients may have more satisfaction and less regret if they had a better understanding of the potential treatment-related adverse events and survival benefits of their treatment (Stryker et al. 2006; Sanda et al. 2008). As the personalized oncology care movement has gained in momentum in the twenty-first century through advances in genomic sciences, our study suggests that tailored treatment decision-making recognizing individual patient’s preferences and values could provide significant additional value to patient care (Ganz 2015). Our study is among the first to evaluate patients’ preferences and attitudes regarding multiple potential medical treatment-related adverse events in treating metastatic CRC (Craig et al. 2014).
Different patient characteristics appeared to variably influence patients’ willingness to tolerate adverse events from chemotherapy or biological therapy to treat metastatic CRC. Overall, we found that individuals who had prior radiotherapy were less willing to tolerate risks of any medical treatment-related adverse events. Radiotherapy and medical therapy for CRC share common treatment-related adverse events such as nausea and vomiting, diarrhea, stomach bleeding, and sexual problems. This finding indicates that past patient experiences play an important role in current patient treatment preference.
Notably, we found that different patient characteristics are predictive of their willingness to tolerate risks of medical treatment-related adverse events by age and stage. This finding reflects the clinical and demographic variation of patient preferences. This finding is supported by research examining patient–physician communication among those diagnosed with advanced cancer. Recent findings show that when treatment goals are discussed during patient visits, patients are more likely to receive less aggressive treatment and earlier referrals to hospice (Wright et al. 2008; Laryionava et al. 2015). Although recent research has described decision support tools for chemotherapy decisions among patients with advanced CRC (Leighl et al. 2011), the present results highlight the importance of additional dialogue about possible treatment-related adverse events and patients’ willingness to tolerate certain events relative to other events, or not to tolerate any adverse events at all (Goelz et al. 2011; Back 2010).
Finally, we identified not only that patients were averse to multiple acute and serious adverse events such as stroke and heart attack, but also that they were less willing to tolerate less clinically serious, but more common symptom-related adverse events (e.g., depression, pain, and fatigue). These findings reflect the high value that patients place on symptom severity or functional impact that are less likely to be managed in routine clinical visits (Ganz 2015). These results also suggest that better personalizing oncology treatments to the individual may benefit from more carefully monitoring these domains before and after a treatment decision and during follow-up care to improve the quality of cancer care (Institute of Medicine 2013).
A strength of the present study is our use of standard gamble to elicit patient preferences for the first time in patients with advanced CRC for their treatment-related adverse events. While several methods are available that directly elicit preference, standard gamble is associated with the highest test–retest reliability within the cancer population (Ross et al. 2003; Kattan et al. 1997), and has theoretical advantages (Kattan et al. 1997; Kattan 2003). Because standard gamble involves uncertainty, it is the only preference measure that captures patients’ risk attitudes: risk-averse, risk-neutral, or risk-seeking (Torrance 1987; Fischer et al. 1986). Additionally, using a patient-specific measure is preferable for our study to using group-level measures such as EQ-5D or Health Utility Index, which reflects societal preferences rather than individual preferences and values (Cowen et al. 1998). A criticism of standard gamble is that it may be difficult for subjects to complete, especially for patients with low literacy. However, low literacy is not an independent predictor of preference values that are elicited via standard gamble in cancer patients (Hahn et al. 2007). Importantly, our cognitive testing of the survey prior to implementation demonstrated patients’ ability to complete standard gamble items.
Another strength of the study was our use of an adaptive survey design. Although study participants initially responded to 15 medical treatment-related adverse events, our tailored computer assessment allows the patient to prioritize these adverse events. The subsets of adverse events were chosen by individual patients and were therefore tailored to each participant who then completed standard gamble vignettes on those tailored events. The benefit of this design is decreased patient burden. Our survey design allowed us to focus on outcomes important for personalized medical treatment decision-making.
Our study is subject to several limitations. First, due to the limited number of eligible patients with concurrent metastatic CRC, we included patients with either stage III or IV CRC. We also evaluated potential differences between stages. Second, since patients do not experience all the adverse events of interest, we employed hypothetical treatment vignettes. To address this, we adjusted for experience of the adverse events in the analysis. Third, the statistically significant differences we identified are larger than 0.03, which has been used as a threshold for minimum important difference (MID) (Sullivan et al. 2005). While there is no consensus on what constitutes a MID for a preference score, other research has suggested higher MIDs up to 0.07 (Sullivan et al. 2005; Fu and Kattan 2006). Fourth, the survey was conducted at a single clinic within the Washington DC metropolitan area, which may limit generalizability of our findings. Likewise, generalizability is limited by the homogeneity of our patient sample, as most of the participants were insured with relatively high education and income compared with national averages. Fifth, due to limited sample size we were unable to assess each adverse event individually. Finally, our analysis may be subject to confounding from unmeasured factors, such as unmeasured comorbid conditions and health behaviors.
Ultimately, the goal of this study is to establish patient preferences regarding a wide range of possible treatment-related outcomes as a foundation to improve cancer therapeutic decisions. Ideally, these considerations would include not only the status of an individual’s cancer and risk of progression, but also the likelihood of treatment-related adverse events and treatment-related declines in functional status or quality-of-life. Increased patient awareness of these risks and benefits could help avoid unnecessary toxicities and treatment.
Fundamentally, this work provides a resource allowing patients to seek a treatment choice best suited to them, ranging from one that will maximize their quality-of-life to options that focus on prolonging survival. For patients with late stage cancer, this may lead to specific decision points such as choosing when to stop taking additional medical agents, enter hospice, or alternatively maintain a focus on aggressive treatment options. A great deal of future research is necessary to determine the optimal use and validation of this methodology in metastatic CRC and with respect to subsequent patient health outcomes and expectations. Next steps of research include evaluating methods to collect and disseminate individual patient preferences in a format that is usable for busy medical oncologists for CRC. This includes developing a decision-analytic tool that integrates the type of preferences individual patient has and make tailored treatment decisions. This patient-centered care will reflect better quality in cancer care.
References
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti AE (eds) (2010) AJCC cancer staging manual, 7th edn. Springer, Berlin
Arora NK, Hesse BW, Rimer BK, Viswanath K, Clayman ML, Croyle RT (2008) Frustrated and confused: the American public rates its cancer-related information-seeking experiences. J Gen Intern Med 23:223–228
Audrey S, Abel J, Blazeby JM, Falk S, Campbell R (2008) What oncologists tell patients about survival benefits of palliative chemotherapy and implications for informed consent: qualitative study. BMJ 337:a752
Back A, Arnold RM, Baile WF, Tulsky JA, Fryer-Edwards K (2010) Improving oncologists’ communication skills. http://depts.washington.edu/oncotalk. Accessed 20 Dec 2013
Choueiri TK, Mayer EL, Je Y et al (2011) Congestive heart failure risk in patients with breast cancer treated with bevacizumab. J Clin Oncol 29:632–638
CMS (2014) Clinical quality measures. http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/ClinicalQualityMeasures.html
Cowen ME, Miles BJ, Cahill DF, Giesler RB, Beck JR, Kattan MW (1998) The danger of applying group-level utilities in decision analyses of the treatment of localized prostate cancer in individual patients. Med Decis Making 18:376–380
Craig BM, Reeve BB, Cella D, Hays RD, Pickard AS, Revicki DA (2014) Demographic differences in health preferences in the United States. Med Care 52:307–313
Epner DE, Baile WF (2014) Difficult conversations: teaching medical oncology trainees communication skills one hour at a time. Acad Med 89:578–584
Fischer G, Kamlet MS, Fienberg S, Schkade D (1986) Risk preference for gains and losses in multiple objective decision making. Manag Sci 31:1065–1086
Fu AZ, Kattan MW (2006) Racial and ethnic differences in preference-based health status measure. Curr Med Res Opin 22:2439–2448
Galfrascoli E, Piva S, Cinquini M et al (2011) Risk/benefit profile of bevacizumab in metastatic colon cancer: a systematic review and meta-analysis. Dig Liver Dis 43:286–294
Ganz P (2015) Quality of cancer care, plenary address. Washington, DC, world congress of psycho-oncology, from national to global: implementing the standard of psychosocial care in oncology
Gattellari M, Butow PN, Tattersall MH (2001) Sharing decisions in cancer care. Soc Sci Med 52:1865–1878
Goelz T, Wuensch A, Stubenrauch S et al (2011) Specific training program improves oncologists’ palliative care communication skills in a randomized controlled trial. J Clin Oncol 29:3402–3407
Grothey A, Van CE, Sobrero A et al (2013) Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 381:303–312
Hahn EA, Cella D, Dobrez DG et al (2007) The impact of literacy on health-related quality of life measurement and outcomes in cancer outpatients. Qual Life Res 16:495–507
Harris KA (1998) The informational needs of patients with cancer and their families. Cancer Pract 6:39–46
Hurwitz H, Fehrenbacher L, Novotny W et al (2004) Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 350:2335–2342
Institute of Medicine (2013) Delivering high-quality cancer care: charting a new course for a system in crisis. National Academies Press, Washington, DC
Kaldjian LC, Curtis AE, Shinkunas LA, Cannon KT (2008) Goals of care toward the end of life: a structured literature review. Am J Hosp Palliat Care 25:501–511
Kattan MW (2003) Comparing treatment outcomes using utility assessment for health-related quality of life. Oncology (Williston Park) 17:1687–1693
Kattan MW, Cowen ME, Miles BJ (1997) A decision analysis for treatment of clinically localized prostate cancer. J Gen Intern Med 12:299–305
Laryionava K, Heussner P, Hiddemann W, Winkler EC (2015) Framework for timing of the discussion about forgoing cancer-specific treatment based on a qualitative study with oncologists. Support Care Cancer 23:715–721
Leighl NB, Butow PN, Tattersall MH (2004) Treatment decision aids in advanced cancer: when the goal is not cure and the answer is not clear. J Clin Oncol 22:1759–1762
Leighl NB, Shepherd HL, Butow PN et al (2011) Supporting treatment decision making in advanced cancer: a randomized trial of a decision aid for patients with advanced colorectal cancer considering chemotherapy. J Clin Oncol 29:2077–2084
Ness RM, Holmes A, Klein R, Greene J, Dittus R (1998) Outcome states of colorectal cancer: identification and description using patient focus groups. Am J Gastroenterol 93:1491–1497
Ness RM, Holmes AM, Klein R, Dittus R (1999) Utility valuations for outcome states of colorectal cancer. Am J Gastroenterol 94:1650–1657
O’Connor AM, Rostom A, Fiset V et al (1999) Decision aids for patients facing health treatment or screening decisions: systematic review. BMJ 319:731–734
Prigerson HG, Bao Y, Shah MA et al (2015) Chemotherapy use, performance status, and quality of life at the end of life. JAMA Oncol 1:778–784
Ramlau R, Gorbunova V, Ciuleanu TE et al (2012) Aflibercept and Docetaxel versus Docetaxel alone after platinum failure in patients with advanced or metastatic non-small-cell lung cancer: a randomized, controlled phase III trial. J Clin Oncol 30:3640–3647
Ross PL, Littenberg B, Fearn P, Scardino PT, Karakiewicz PI, Kattan MW (2003) Paper standard gamble: a paper-based measure of standard gamble utility for current health. Int J Technol Assess Health Care 19:135–147
Sanda MG, Dunn RL, Michalski J et al (2008) Quality of life and satisfaction with outcome among prostate-cancer survivors. N Engl J Med 358:1250–1261
Semenza GL (2008) A new weapon for attacking tumor blood vessels. N Engl J Med 358:2066–2067
Street RL Jr, Voigt B (1997) Patient participation in deciding breast cancer treatment and subsequent quality of life. Med Decis Making 17:298–306
Stryker JE, Wray RJ, Emmons KM, Winer E, Demetri G (2006) Understanding the decisions of cancer clinical trial participants to enter research studies: factors associated with informed consent, patient satisfaction, and decisional regret. Patient Educ Couns 63:104–109
Sullivan PW, Lawrence WF, Ghushchyan V (2005) A national catalog of preference-based scores for chronic conditions in the United States. Med Care 43:736–749
Torrance GW (1987) Utility approach to measuring health-related quality of life. J Chronic Dis 40:593–603
Walling A, Lorenz KA, Dy SM et al (2008) Evidence-based recommendations for information and care planning in cancer care. J Clin Oncol 26:3896–3902
Weeks JC, Catalano PJ, Cronin A et al (2012) Patients’ expectations about effects of chemotherapy for advanced cancer. N Engl J Med 367:1616–1625
Wright AA, Zhang B, Ray A et al (2008) Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 300:1665–1673
Zafar SY, Malin JL, Grambow SC et al (2013) Chemotherapy use and patient treatment preferences in advanced colorectal cancer: a prospective cohort study. Cancer 119:854–862
Acknowledgments
This study was supported by the Ruesch Center for the Cure of Gastrointestinal Cancers at Georgetown University, and Grant P30CA051008 from the National Cancer Institute. Dr Jensen was supported in part by Grant Number KL2TR000102 from the National Center for Research Resources (NCRR) and the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health (NIH), through the Clinical and Translational Science Awards Program (CTSA).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. L. M. has received a speaker honorarium from Genentech, Bayer, Amgen, and Celgene. Other authors declared no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Fu, A.Z., Graves, K.D., Jensen, R.E. et al. Patient preference and decision-making for initiating metastatic colorectal cancer medical treatment. J Cancer Res Clin Oncol 142, 699–706 (2016). https://doi.org/10.1007/s00432-015-2073-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-015-2073-4