
Abstract
Purpose
Adolescence is a period of growing independence and maturity, within the period of legal minority. As parents or guardians are socially and legally responsible for adolescents’ medical decisions, shared decision-making in adolescent healthcare could be ethically challenging.
This review aims to identify and map the ethical tensions in shared decision-making in adolescent healthcare.
Methods
We systematically searched the literature following the PRISMA guidelines to identify relevant articles, which were analyzed using the review of reasons methodology Strech and Sofaer (J Med Ethics 38(2):121-6, 2012).
Results
We included 38 articles which involved adolescents, healthcare professionals and parents as being the main stakeholders. Shared decision-making was influenced not only by individual stakeholders’ characteristics, but by tensions between stakeholder dyads. Most studies supported the involvement of the adolescent in decision-making, depending on their life experience, decision-making capacity and clinical condition.
Conclusions
Shared decision-making in adolescent health is receiving increasing attention. However, questions remain on what this concept entails, the roles and involvement of stakeholders and its practical implementation.
What is known: • Although adolescents wish to be involved in health decisions, shared decision-making in adolescents is underexplored • Adolescent shared decision-making is different from pediatric and adult shared decision-making, and is ethically complex due to the adolescent’s growing autonomy | |
What is new: • Adolescent SDM involves three-way interactions between the adolescent, healthcare professional and parents • In adolescent shared decision-making, involving or excluding a stakeholder and sharing or withholding information are ethically value-laden steps • Research is needed to further understand the roles of adolescents’ personal value systems, extended or reconstituted families and decision aids in shared decision-making |
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Traditional medical decision making models such as paternalism (where the physician makes decisions) or the more recent autonomy model (where patients are central) are being replaced by shared-decision making (SDM). SDM is defined as an approach where Healthcare Professionals (HCPs) and patients together agree on an evidence-based treatment plan consistent with the patient’s values and preferences [2, 3]. Grounded on the ethical principles of both self-determination and relational autonomy, SDM encourages the involvement of family members in decision-making [4]. As SDM extends beyond the physician–patient dyad, it should be suited for decision making in adolescents, defined as persons aged between 10 and 19 years by the World Health Organization [5,6,7]. As adolescence is a period of growing independence within the period of legal minority, decision-making in adolescent healthcare is often complex and ethically challenging.
While SDM in adults is based on the principles of respect for autonomy and beneficence, pediatric decision-making is based primarily on preventing harm (non-maleficence) [8]. Adolescence falls developmentally and chronologically on the border between childhood and adulthood. Legally, adolescents are minors unless they are considered emancipated or mature minors; this means that, as in pediatric SDM, they are dependent on their parents or guardians to executes their preference. Therefore, SDM in adolescents is unique, and the tensions may not be captured within the frameworks of pediatric or adult SDM. While studies show that adolescents desire active involvement in healthcare decisions, this may not always happen in practice [6]. While studies show that adolescents desire active involvement in healthcare decisions, this may not always happen in practice. Currently, in clinical practice, adolescents are often marginalized decision makers, in spite of evidence suggesting that involving adolescents could improve well-being, knowledge, satisfaction and treatment adherence [9].
On the contrary, SDM is an established concept in medical research involving adolescents [10]. For instance, the MacCAT-CR (MacArthur Competence Assessment Tool for Clinical Research), a clinical tool to assess research participants’ decision-making capacity, has been adapted for use in children [11]. In a study involving genetic research on biobank-stored tissues, adolescents were permitted to give informed consent [12]. These developments show the feasibility of involving adolescents in SDM, albeit in a different context.
Although there are ongoing discussions regarding the ethical and legal framework of adult and pediatric SDM in healthcare, the ethical tensions of SDM in adolescents remain inadequately explored [13]. In this study we conducted a review of literature on the ethical aspects of SDM in adolescents. The research question is as follows; “what are the normative considerations around shared decision-making in adolescent healthcare”? Through it we aim to identify the normative arguments, describe notable trends and identify gaps for future research.
Methods
A detailed description on the search strategy, article selection, data extraction and analysis is provided in the supplementary materials (Supplements 1 and 2). 38 publications were selected out of the initial 18,622 and the Nvivo software package [14] was used to code and identify themes on this topic.
Results
Included articles and overview
38 articles fulfilled the inclusion criteria. These were published between 1993 and 2022, with the majority (81%) being published after 2010. Authors from various disciplines contributed to this literature: medicine(47%), bioethics (21%), psychology (10%) nursing (8%), philosophy (5%), physiotherapy (3%), law (3%), and dentistry (3%). The articles and their features are listed below in Supplement 3. Most of the articles are in favor of SDM, with two articles neutral in position and one against SDM.
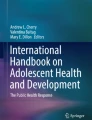
To organize the information from our review, we created a conceptual map shown in Fig. 1. The results are structured accordingly- firstly, we describe the three main stakeholders and their characteristics, and secondly, we describe the stakeholder interactions and possible ethical tensions.

Conceptual map of the three main stakeholders, ethically relevant stakeholder characteristics (shown in blue text) and ethical tensions in their interactions (shown in grey text)
Stakeholders and their characteristics
The adolescent
Most studies (28/38) find that adolescents’ decision-making capacity influences their participation in SDM. Decision-making capacity (DMC) refers to the ability to comprehend information, understand the consequences of decisions, weigh benefits and risks and make a voluntary and informed choice [15,16,17,18]. Unlike maturity, which was conceptualized either in terms of cognitive development [15, 18]or neuropsychological development [19,20,21]. DMC is a combination of intellectual and functional characteristics. Most articles therefore considered DMC, rather than maturity, as being important for SDM.
DMC can vary widely between adolescents depending on their age, [19, 22,23,24,25,26,27], or on physical or psychological co-morbidities [15, 28,29,30]. Further, DMC is not a static or uniform requirement, but depends also on the decision [18, 30,31,32]. For instance, refusing a lifesaving treatment requires more DMC than consenting to it [17, 31]. Decisions about fertility preservation while transitioning could also be beyond the decisional capacity of adolescents [30, 31], as it requires them to “…. consider desires for biological parenthood during a period in which thinking about family formation is developmentally non-normative” [31].
Although DMC is considered important, there is lack of consensus on its exact conceptualization. Some studies cite empirical literature on adolescents’ cognition, neurophysiological development and psychosocial characteristics to argue that adolescents’ DMC is either similar or dissimilar to those of adults [15, 16, 20, 23, 24, 26, 28, 33,34,35]. Some, however, argue for a more normative and theoretical conceptualization of DMC, as neurophysiological characteristics alone cannot determine whether an adolescent should make a decision [28, 36]. Rather, it depends also on the relational context of the adolescent, and is shaped by their place in society as a whole [21, 36].
Four studies argue that adolescents’ lived experience should influence the extent of their involvement in SDM [16, 24, 26, 34]. Irrespective of their age, children with chronic or recurring illness can possess deeper understanding of their condition, about the consequences of medical decisions, and about their conceptions of the good [16, 24, 26, 34]. In such cases, more weight could be given to their views.
Not all medical decisions require the same decisional capacity [16, 32]. Minor decisions, for instance whether a wound can be sutured, might lie within the capabilities of an adolescent, whereas major decisions, such as undergoing heart surgery, might not [16]. For potentially lifesaving interventions, adolescents are often permitted to consent to, but seldom allowed to refuse, the treatment [18, 28, 32, 37, 38]. Tucker [38] calls this “asymmetric paternalism”, and argues that it is justifiable based on safeguarding adolescents’ welfare, while allowing them to exercise their decision-making to a certain extent.
“Major” treatment decisions include not only those that are potentially life-saving, but also very personal choices involving sensitive information, such as decisions on reproductive or mental health [16]. Decisions on fertility preservation in transgender adolescents could also be considered highly personal, as individuals may hold diverse beliefs about concepts such as genetic relatedness [30, 31].
The healthcare professional
Healthcare professional are ideally placed to encourage SDM, depending on their knowledge, beliefs and experience. Professionals who receive guidance on SDM are likelier to encourage SDM; however, considering the paucity of guidelines on SDM, this may not often be the case [16, 21, 26, 39]. Knowledge about adolescents’ conditions and prior clinical experience could play a role [16, 28, 40]. Especially in emerging fields such as gender affirming surgery, SDM could be encouraged or hindered by the clinician’s personal views [33]. Often, medical decision-making takes place in constrained and chaotic situation, where the lack of time and opportunity to establish trustful relationships can hinder SDM [16, 22]. Additionally, the institutional culture and attitudes around clinical decision-making could also influence SDM [28, 40].
The parents
SDM depends on parents' and adolescents' unique family dynamics. Whereas the family is often considered one relational unit [29], this may not be the case when individuals are separated geographically, emotionally or legally, all of which could influence the extent of parental involvement and responsibility [20, 23, 29]. Further, parenting styles could vary widely among families, from being authoritative to permissive, which could affect children’s involvement in decisions [16, 18, 25, 31, 35]. Additionally, practical considerations such as finances could also affect the decision, especially in expensive and complex treatments [18, 30, 39]
SDM can be influenced by the cultural, social and religious context of the family [16, 40,41,42]. For instance, parents in Western contexts could be likelier to support their adolescent child’s developing autonomy, whereas those in (or influenced by) totalitarian regimes could be more paternalistic [16]. Parents from vulnerable communities or minority groups could also be less likely to entrust their child’s medical care to professionals [41].
Stakeholder interactions and ethical tensions
The adolescent-healthcare professional relationship
Especially when adolescents suffer a life-threatening illness or when the prognosis is bleak, HCPs may hesitate to share this information with them to prevent emotional pain and hopelessness [20, 22, 24, 43, 44]. However, such efforts to protect the adolescent, could do more harm than disclosure itself. Cohen, et al. [20] argues that even for untreatable illnesses, adolescents can grasp and handle the information. When information is withheld, the adolescent might obtain it from other sources or guess based on others’ responses [24], which can lead to fear and isolation and a lack of trust in the physician [22, 24]. [44].
As HCPs provide medical expertise, adolescents contribute expertise in their identities as they have the clearest picture of their goals [31, 33, 40].
However, depending on the risk–benefit ratio, there could be limits to which adolescents’ views can be incorporated. The onus remains on HCPs to determine whether adolescents’ requests will promote their overall good [33, 40, 45].
In some instances, upholding adolescents ‘ autonomous decision could involve harm to their best interests or their welfare [16, 18, 22, 24, 28, 30, 31, 37, 38, 43, 46]. This could be especially morally distressing for HCPs if the adolescent refuses treatment for a life-threatening condition[18, 20, 28, 32, 37, 38, 46].
Although HCPs may not be obliged to accept treatment refusal from adolescents, they could benefit from exploring the reasons behind treatment refusal [18, 22, 28, 31, 33, 37]. For instance, an adolescent refusing chemotherapy because they do not wish to lose their hair could be overlooking other life-saving benefits [24].
Some studies question whether, in allowing adolescents to consent to but not refuse lifesaving treatment, their growing autonomy is being supported [26, 32, 37, 38, 46]. Most, however, agree that welfare should be the main ethical consideration.
The parent-healthcare professional relationship
HCPs and parents could disagree on whether and how much information should be given to adolescents. Parents sometimes act as gatekeepers and disallow HCPs from sharing information with the adolescent patient, especially when the prognosis is poor [20, 24, 29]. In this context, disclosing against parents’ wishes harms trust[24, 29]. Rather than taking these actions, HCPs could engage in dialogue with parents to encourage disclosure [24, 29].
In most societies, adult patients have a right to confidentiality of medical records and data; HCPs cannot divulge information except under exceptional circumstances [47, 48]. Whether adolescents are legally entitled to the same level of confidentiality is determined by the social and legal context [47, 48]. In many Western contexts, adolescents’ confidentiality is respected if they show a high level of DMC[25, 35, 48]. This could be especially true for the domain of sexual health [25, 35, 48]. Some, however, argue against protecting adolescent confidentiality as the standard of care, as supportive parents could guide adolescents in their decision-making [17, 25, 35].
Parents are considered default decision-makers for their minor children, through the moral authority conferred on them by society [19, 37, 39, 42, 43, 45]. However, their right to decide on children’s behalf is not absolute, but subject to the “best interest” standard [19, 37, 42, 43, 45]. As the adolescents are not only members of their family but also of broader society, decisions that contradict their best interests could be rejected by HCPs and overruled by the court [19, 37, 42, 43, 45].
The adolescent-parent relationship
When faced with the choice to share medical information with their adolescent children, parents may hesitate as they feel obliged to protect their child from emotional burden. Studies discuss different reasons for and against disclosure by parents [16, 20, 24, 29, 41, 44, 49].
On the one hand, arguments for disclosure are based on research showing that disclosure caused no harm, and consequently led adolescents to active, knowledgeable participation in SDM [20, 24, 29]. In addition, one author[29] states that such disclosure should be the norm and should only be avoided if there is clear evidence of imminent harm to the patient. Although parents may feel that they are shielding children from the emotional burden of their medical diagnosis, this could paradoxically lead to stress and anxiety in adolescents [15, 35].
On the other hand, proponents for withholding information base their arguments on preventing psychological harm to adolescents, such as feelings of fear, stress, confusion, or stigmatization [16, 20, 24, 36, 41, 44]. Moreover, parents may not divulge medical information to adolescents based on religious and cultural reasons, especially when life-threatening illnesses such as cancer are diagnosed [41, 44].
Situations can arise where parents’ and adolescents’ interests conflict. Parents’ deeply held values and beliefs may differ from those of their children, or adolescents may hold different visions for their future lives than their parents, which could affect the medical decision [17, 28, 42, 49]. Parents’ vision of future quality of life may also occasionally exceed those of their child [15, 41]. In more extreme cases, parents may lack the capacity to make the best decision for their child as they could be habitually negligent of their children [17, 47].
Parents’ emotions could also play a role in SDM [29, 34, 36, 43, 50]. The “emotional proximity” of parents to their child's situation could prevent them from grasping their best interests [29]. Emotional distress caused by seeing their child suffer could also prevent parents from considering their child’s wishes [25, 29, 34, 35]. Despite the possible differences, the fact remains that adolescents are in a position of dependence and therefore require the approval of their guardian, unless they seek emancipation or are considered mature minors [25, 29, 34, 35, 43, 47, 50]. Moreover, studies have shown that where complex decisions are involved, adolescents prefer to be guided by a trusted adult [25, 44].
Parents and other family members should ideally be “supportive co-pilots” in SDM; however, the possible consequences of the decision could play a role in this process [15, 16, 22, 27, 28, 40, 50]. Situations involving high stakes, [18, 28, 30] or adolescents’ chronic illness or disability could cause parents to be almost exclusive decision-makers, [28, 41, 43]. SDM could also become strained if they object to treatment processes considered novel or unconventional, such as gender affirming therapy, based on fear of the unknown and irreversible consequences for the adolescent, who could blame their parents in future [33].
In some instances, parents could prioritize the best interests of the family unit, rather than those of the adolescent [15, 17, 20, 21, 28, 29, 34, 49]. This could be especially true in societies where familial autonomy is valued over individual autonomy [16, 42]. The interests of siblings, parents and other family members, especially in decisions that causes long-term impacts on the family, could play a part in SDM [16, 21, 41]. Financial considerations may also shape parents’ interests, such as whether surgical interventions will be reimbursed [39].
A few studies discuss how family composition and structure have an impact on SDM, especially when decisional authority is not shared equally among parents; this could lead to ethical challenges from decisional conflicts [17, 23, 30].
Conceptualizing SDM
Nineteen of the thirty-eight included articles did not use the term “shared decision-making”; however, they discussed adolescents’, parents’ and HCPs’ involvement in making medical decisions. The remaining nineteen articles explicitly used the term SDM, of which fourteen defined or described the concept. Most of these define SDM as a collaborative process involving the three main stakeholders, with varying levels of emphasis on involving adolescents [19, 27, 28, 30, 33, 40, 43,44,45, 48]. Others define SDM as a family-centered decision process, where the entire family’s values and preferences can be integrated with HCPs’ expertise, with special attention to adolescents’ views [8, 17, 34].
Furthermore, multiple approaches to SDM have been described. For instance, Birchley [43] outlines three models of SDM: the shared rational deliberative joint decision model (SJDM), the professionally driven best interests compromise model (PBCM) and moral SDM. Whereas all stakeholders are considered equals in order to reach a consensus in SJDM, PBCM allows the HCP to strategically control the negotiation to advance adolescents’ best interests [43]. Moral SDM, on the other hand, requires the stakeholders to compromise some of their individual interests to reach a shared decision [43]. Lang and Paquette [28] touch upon an “arbitrative model” of SDM, where the HCP acts as a mediator between parents and adolescents in case of disagreements. Although there could be some common elements in pediatric SDM such as providing information, deciding stakeholders’ roles, understanding each stakeholder’s values and deciding on a treatment option together, SDM in practice could vary widely among providers [28].
Discussion
Our results map the ethical considerations of this process. Overall, the results highlight the importance of adolescent SDM, and of involving the adolescent to an extent appropriate to the situation. This is also reflected in empirical research among healthcare professionals [51,52,53,54,55] and among adolescents [5, 52, 56,57,58,59,60]. Empirical research among parents show more divergent interests [52, 61, 62]; this could pose a challenge as in most cases, parents have the moral and legal responsibility to decide on children’s behalf.
Defining adolescent SDM
In this review, some studies defined SDM as a collaborative process involving the three main stakeholders; however, a few emphasized the inclusion of the family as a whole, and integrating their values. Although these definitions are not mutually exclusive, they focus on different aspects. The varying definitions of pediatric SDM is also acknowledged in literature [63,64,65]. The American Academy of Pediatrics (AAP), for instance, identifies four attributes of pediatric SDM: involvement of at least two parties, bidirectional exchange of knowledge, understanding treatment options, and equal consideration of all parties’ values [63, 66]. Park and Cho [64] identified four characteristics: involvement of the three stakeholders, collaborative partnership, making compromises and the child’s welfare as the ultimate goal. Others define SDM as an evidence-based process that fosters collaboration between the three parties in medical decision-making [67]. The differing definitions could in part be due to diverse clinical settings, ranging from the outpatient department to the ICU, and the wide developmental range and ages of pediatric patients [63,64,65].
Although adolescence involves a narrower age range, we encountered various definitions: 10 to 19 according to the World Health Organization (WHO) and the European Academy of Pediatrics (EAP); 11 to 21 as per the AAP; 13 to 18 as per Medline’s indexing system (MeSH) and 11 to 19 according to Embase’s thesaurus [7, 68,69,70]. From our experience, we find that this could pose a challenge to researchers while searching and reviewing literature. The lack of a generally accepted definition of both concepts (i.e. adolescence and SDM) could potentially impact research on adolescent SDM, as well as its implementation, practice and assessment.
Stakeholders’ involvement and characteristics
In this review, the three main stakeholders identified were adolescents, HCPs and parents. Although this triadic involvement seems self-evident (except when one party is severely incapacitated), it may not always be part of SDM practice. In their systematic review of pediatric SDM interventions, Wyatt, et al. [6] report that out of 54 interventions, only three targeted the patient-HCP-parent triad. A majority of the interventions (34) targeted the parents alone, 14 targeted a dyad, six targeted the HCP and three the patient [6]. As the focus is on pediatric patients rather than adolescents, some interventions excluded patients due to their age. However, this was not the case in most interventions, and the authors consider patients’ exclusion their most remarkable finding [6].
In contrast, parents could sometimes be excluded by design from SDM. Discussing SDM in adolescents’ contraceptive use, Gonzalez, et al. [71] include adolescents and HCPs as stakeholders with seemingly little discussion on involving parents. In their pilot study on SDM for smoking cessation in adolescents, Chen, et al. [72] target adolescents exclusively. Although excluding parents could be justifiable, for instance, based on preserving adolescents’ confidentiality, neither article appears to explicitly motivate this exclusion, implying that the tripartite model of adolescent SDM cannot be considered a default.
Ethical tensions could also arise from stakeholder characteristics,. Similar to Boland, et al. [67]’s systematic review, we found that HCPs’ knowledge and beliefs, the clinical environment and lack of time, adolescents’ age, capacity and clinical condition could all impact SDM. Additional insights from this review include the influence of family members besides parents and the socio-cultural context, in line with Alden et al. [73]. Additionally, very little research addresses the dynamics within reconstituted families and how this impacts SDM. As more and more adolescents are living in reconstituted families in Western societies, SDM in this context needs to be studied further [74].
Concerning cultural or religious beliefs, the consensus appears to be that they can be incorporated in SDM when they do not compromise adolescents’ welfare, or when evidence-based practices cannot unequivocally promote adolescents’ best interests. This may, however, be challenging in practice. As adolescent patients could consider religious beliefs important, and as not much guidance exists on how to incorporate them, it could present an important theme for future research [75].
Guidance and tools on SDM
Although some studies included in this review outline approaches [28, 43] or steps [8, 40, 48] for SDM, they mostly do not focus on its procedural aspects. A growing phenomenon in the procedural aspect is the development of decisional aids and tools to promote SDM in clinical practice. These tools could assume various formats such as documents, interactive websites or mobile phone apps, and could target one or more stakeholders. This has already been explored for transgender care [76]cand inflammatory bowel disease [77].
Strengths and limitations
Our study employed a comprehensive search of relevant sources. Nonetheless, none of the included articles included the context of low and lower-middle income countries, where nearly 90% of the adolescent worldwide reside [78]. This lack of representation could be due to the language criteria used, or the scarcity of literature from these regions. Consequently, the tensions highlighted may not be globally representative. Finally, as highlighted in the results, only thirteen of the analyzed articles defined SDM, and the definitions of both adolescence and SDM varied considerably. The resulting challenges to searching and retrieving literature on adolescent SDM may also be reflected in this paper.
Conclusion and future research directions
This review shows that adolescent SDM is made complex by the interactions and ethical tensions among stakeholders. As our results show, involving or excluding a stakeholder, or sharing information, could be value-laden steps, depending on the clinical and familial context. However, the body of evidence on adolescent SDM appears to be growing, which is an encouraging sign. As it is an inherently ethically laden field, care should be taken to incorporate its ethical aspects in future research and practice.
Based on the findings of this study, the following areas could benefit from future research:
-
The concept of adolescent SDM and its essential attributes, as opposed to pediatric and adult SDM
-
The involvement of stakeholders and under what conditions exclusion can be justified
-
The dynamics of adolescent SDM in reconstituted families
-
Incorporating adolescents’ or families’ cultural or religious beliefs within SDM
-
The role of decisional aids and tools in SDM
As the position of the adolescent in society evolves, their roles in health and healthcare may also change. Much empirical research highlights their willingness to play active roles in health decisions. Learning to strike the balance between sidelining adolescents on the one hand versus burdening them on the other will prove crucial to promoting SDM.
Data Availability
The articles included in this review are publicly available. The coding scheme and coded data are available from the authors upon reasonable request.
Abbreviations
- DMC:
-
Decision-making capacity
- HCP:
-
Healthcare Professional
- SDM:
-
Shared Decision-making
References
Strech D, Sofaer N (2012) How to write a systematic review of reasons. J Med Ethics 38(2):121–6. https://doi.org/10.1136/medethics-2011-100096
Elwyn Dominick G, Frosch R, Thomson N, Joseph-Williams A, Lloyd P, Kinnersley E, Cording D, Tomson C, Dodd S, Rollnick A, Edwards M, Barry (2012) Shared decision making: a model for clinical practice. J Gen Intern Med 27(10):1361–1367. https://doi.org/10.1007/s11606-012-2077-6
Elwyn G, Laitner S, Coulter A, Walker E, Watson P, Thomson R (2010) Implementing shared decision making in the NHS. BMJ 341:c5146–c5146. https://doi.org/10.1136/bmj.c5146
Barry MJ, Edgman-Levitan S (2012) Shared decision making–pinnacle of patient-centered care (in eng). N Engl J Med 366(9):780–781. https://doi.org/10.1056/NEJMp1109283
Lipstein EA, Muething KA, Dodds CM, Britto MT (2013) “I’m the One Taking It”: adolescent participation in chronic disease treatment decisions. J Adolesc Health 53(2):253–259. https://doi.org/10.1016/j.jadohealth.2013.02.004
Wyatt KD et al (2015) Shared decision making in pediatrics: a systematic review and meta-analysis. Acad Pediatr 15(6):573–583. https://doi.org/10.1016/j.acap.2015.03.011
World Health Organization. "Adolescent Health." https://www.who.int/health-topics/adolescent-health#tab=tab_1 (accessed 11th August, 2023).
Sawyer K, Rosenberg AR (2020) How should adolescent health decision-making authority be shared? AMA J Ethics 22(5):E372-379. https://doi.org/10.1001/amajethics.2020.372. (in eng)
Wijngaarde RO, Hein I, Daams J, Van Goudoever JB, Ubbink DT (2021) Chronically ill children’s participation and health outcomes in shared decision-making: a scoping review. Eur J Pediatr 180(8):2345–2357. https://doi.org/10.1007/s00431-021-04055-6
Field MJ, Behrman RE, Institute of Medicine (US) Committee on Clinical Research Involving Children (2004) Understanding and Agreeing to Children’s Participation in Clinical Research. National Academies Press (US), In Ethical Conduct of Clinical Research Involving Children (in en)
Hein IM et al (2014) Accuracy of the macarthur competence assessment tool for clinical research (MacCAT-CR) for measuring children’s competence to consent to clinical research. JAMA Pediatr 168(12):1147–1153. https://doi.org/10.1001/jamapediatrics.2014.1694
Hens K, Cassiman J-J, Nys H, Dierickx K (2011) Children, biobanks and the scope of parental consent. Eur J Hum Genet 19(7):735–739. https://doi.org/10.1038/ejhg.2011.29
de Winter JP, Toelen J, Milani P (2024) Empowering young voices: navigating the complexities of minors in healthcare decisions. Eur J Pediatr 183(6):2515–2516. https://doi.org/10.1007/s00431-024-05524-4
NVivo (2022) NVivo Software 1.6.1 (v1137). ed
Hopkins KA, Ott MA, Salih Z, Bosslet GT, Lantos J (2019) When adolescent and parents disagree on medical plan, who gets to decide? Pediatrics 144(2). (in eng). https://doi.org/10.1542/peds.2019-0291
Jeremic V, Sénécal K, Borry P, Chokoshvili D, Vears DF (2016) Participation of children in medical decision-making: challenges and potential solutions. J Bioeth Inq 13(4):525–534. https://doi.org/10.1007/s11673-016-9747-8. (in eng)
Mutcherson KM (2005) Whose body is it anyway? An updated model of healthcare decision-making rights for adolescents. Cornell J Law Public Policy 14(2):251–325
Sinclair SJ (2009) Involvement of adolescents in decision making for heart transplants. MCN Am J Matern Child Nurs 34(5):276–81. https://doi.org/10.1097/01.Nmc.0000360417.39659.49. (in eng, quiz 282-3)
Behbahani M, McGuire LS, Burokas L, Obringer E, Nikas D (2021) Challenges in shared decision-making in pediatric neuro-oncology: two illustrative cases of the pursuit of postoperative alternative medicine. Clin Ethics 16(1):49–52. https://doi.org/10.1177/1477750920928899. (in English)
Cohen LL, Stolerman M, Walsh C, Wasserman D, Dolan SM (2012) Challenges of genetic testing in adolescents with cardiac arrhythmia syndromes. J Med Ethics 38(3):163–167. https://doi.org/10.1136/medethics-2011-100087
Salter EK (2017) Conflating capacity & authority: why we’re asking the wrong question in the adolescent decision-making debate. Hastings Center Rep 47(1):32–41. https://doi.org/10.1002/hast.666. (in English)
Berkowitz I, Burgart A, Truog RD, Mancuso TJ, Char D, Lantos JD (2020) Parents demand and teenager refuses epidural anesthesia. Pediatrics 145(6). in eng. https://doi.org/10.1542/peds.2019-3295
Ciliberti R, Alfano L, Baldelli I, de Stefano F, Bonsignore A (2018) Self-determination, healthcare treatment and minors in Italian clinical practice: ethical, psychological, juridical and medical-legal profiles. Acta Bio-Med: Atenei Parmensis 89(1):34–40. https://doi.org/10.23750/abm.v89i1.6368
Leikin S (1993) The role of adolescents in decisions concerning their cancer therapy. Cancer 71(10 Suppl):3342–6. https://doi.org/10.1002/1097-0142(19930515)71:10+%3c3342::aid-cncr2820711734%3e3.0.co;2-i. (in eng)
Partridge B (2014) Adolescent pediatric decision-making: a critical reconsideration in the light of the data. HEC Forum 26(4):299–308. https://doi.org/10.1007/s10730-014-9250-8. (in eng)
Piker A (2011) Balancing liberation and protection: a moderate approach to adolescent health care decision-making. Bioethics 25(4):202–208. https://doi.org/10.1111/j.1467-8519.2009.01754.x. (in eng)
Williams JC, Atack NE, Dhaliwal RDK (2015) Who wears the braces? A practical application of adolescent consent. Br Dent J 218(11):623–627. https://doi.org/10.1038/sj.bdj.2015.497
Lang A, Paquette ET (2018) Involving minors in medical decision making: understanding ethical issues in assent and refusal of care by minors. Semin Neurol 38(5):533–538. https://doi.org/10.1055/s-0038-1668078. (in eng)
Salter EK (2013) Should we tell Annie? Preparing for death at the intersection of parental authority and adolescent autonomy. Narrat Inq Bioeth 3(1):81–8. https://doi.org/10.1353/nib.2013.0006. (in eng)
Warton C, McDougall RJ (2022) Fertility preservation for transgender children and young people in paediatric healthcare: a systematic review of ethical considerations. J Med Ethics. https://doi.org/10.1136/medethics-2021-107702
Chen D, Simons L (2018) Ethical considerations in fertility preservation for transgender youth: a case illustration. Clin Pract Pediatr Psychol 6(1):93–100. https://doi.org/10.1037/cpp0000230. (in eng)
Kuther TL (2003) Medical decision-making and minors: issues of consent and assent. Adolescence 38(150):343–58 (in eng)
Grimstad F, Boskey E (2020) How should decision-sharing roles be considered in adolescent gender surgeries? AMA J Ethics 22(5):452–457
Harrison C, Kenny NP, Sidarous M, Rowell M (1997) Bioethics for clinicians: 9. Involving children in medical decisions. Cmaj 156(6):825–8 (in eng)
Partridge BC (2010) Adolescent psychological development, parenting styles, and pediatric decision making. J Med Philos 35(5):518–525. https://doi.org/10.1093/jmp/jhq044. (in eng)
Ruhe KM, Wangmo T, Badarau DO, Elger BS, Niggli F (2015) Decision-making capacity of children and adolescents—suggestions for advancing the concept’s implementation in pediatric healthcare. Eur J Pediatr 174(6):775–782. [Online]. Available: https://springerlink.bibliotecabuap.elogim.com/content/pdf/10.1007/s00431-014-2462-8.pdf. Accessed 20 April 2023
Ross LF (2009A) Against the tide: arguments against respecting a minor’s refusal of efficacious life-saving treatment. Camb Q Healthc Ethics 18(3):302–15. https://doi.org/10.1017/s0963180109090471. (in eng, discussion 315-22)
Tucker F (2016) Developing autonomy and transitional paternalism. Bioethics 30(9):759–766. https://doi.org/10.1111/bioe.12280. (in eng)
Ardern CL, Grindem H, Ekås GR, Seil R, McNamee M (2018) Applying ethical standards to guide shared decision-making with youth athletes. Br J Sports Med 52(20):1289–1290. https://doi.org/10.1136/bjsports-2018-099183. (in eng)
Langer DA, Jensen-Doss A (2018) Shared decision-making in youth mental health care: using the evidence to plan treatments collaboratively. J Clin Child Adolesc Psychol 47(5):821–831
Lanocha N, Tate T, Salter E, Elster N, Antommaria AHM (2021) Can parents restrict access to their adolescent's voice?: deciding about a tracheostomy. Pediatrics 147(4). in eng.https://doi.org/10.1542/peds.2021-050358
Parsapoor A, Parsapoor MB, Rezaei N, Asghari F (2014) Autonomy of children and adolescents in consent to treatment: ethical, jurisprudential and legal considerations. Iran J Pediatr 24(3):241–248. in English. [Online]. Available: https://www.embase.com/search/results?subaction=viewrecord&id=L373187681&from=exporthttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC4276576/pdf/IJPD-24-241.pdf. Accessed 8 May 2023
Birchley G (2014) Deciding together? Best interests and shared decision-making in paediatric intensive care. Health Care Anal 22(3):203–222. https://doi.org/10.1007/s10728-013-0267-y. (in eng)
Gibson F, Coyne I (2017) Addressing the ethical challenges for young adults, from a rights-based perspective. In: Bleyer A, Barr R, Ries L, Whelan J, Ferrari A (eds) Cancer in adolescents and young adults, 2nd edn. Springer International Publishing, Cham, pp 765–778 (Pediatric Oncology)
Alessandri AJ (2011) Parents know best: or do they? Treatment refusals in paediatric oncology. J Paediatr Child Health 47(9):628–631. https://doi.org/10.1111/j.1440-1754.2011.02170.x
Ross LF (2009) Arguments against respecting a minor’s refusal of efficacious life-saving treatment redux, part II. Camb Q Healthc Ethics 18(4):432–40. https://doi.org/10.1017/s096318010909063x. (in eng, discussion 440-2)
Almeida RAD, Lins L, Rocha ML (2015) Ethical and bioethical dilemmas in adolescent health care. Rev Bioética 23:320–330
Michaud PA (2016) Assessing adolescent capacity for decision making in clinical care: the practical application of bioethics and human rights principles. In International Handbook on Adolescent Health and Development: The Public Health Response: Springer International Publishing, Cham, pp. 359–372.
Zhong YJ, Cavolo A, Labarque V, Gastmans C (2022) Physician decision-making process about withholding/withdrawing life-sustaining treatments in paediatric patients: a systematic review of qualitative evidence. Bmc Palliative Care 21(1):Art no. 113. https://doi.org/10.1186/s12904-022-01003-5
Azotam AN (2012) Pediatric consent: case study analysis using a principles approach. Nurs Ethics 19(4):581–585. https://doi.org/10.1177/0969733012448348. (in English)
Bjønness S, Viksveen P, Johannessen JO, Storm M (2020) User participation and shared decision-making in adolescent mental healthcare: a qualitative study of healthcare professionals’ perspectives. Child Adolesc Psychiatry Mental Health 14(1):2. https://doi.org/10.1186/s13034-020-0310-3
Coyne I, Amory A, Kiernan G, Gibson F (2014) Children’s participation in shared decision-making: children, adolescents, parents and healthcare professionals’ perspectives and experiences. Eur J Oncol Nurs 18(3):273–280. https://doi.org/10.1016/j.ejon.2014.01.006
Day E, Jones L, Langner R, Stirling LC, Hough R, Bluebond-Langner M (2018) “We just follow the patients’ lead”: Healthcare professional perspectives on the involvement of teenagers with cancer in decision making. Pediatr Blood Cancer 65(3):e26898. https://doi.org/10.1002/pbc.26898
Needle JS, Peden-McAlpine C, Liaschenko J (2019) Physicians’ Perspectives on adolescent and young adult advance care planning: the fallacy of informed decision making. J Clin Ethics 30(2):131–142. https://doi.org/10.1086/jce2019302131
Schalkers I, Parsons CS, Bunders JF, Dedding C (2016) Health professionals’ perspectives on children’s and young people’s participation in health care: a qualitative multihospital study. J Clin Nurs 25(7–8):1035–1044. https://doi.org/10.1111/jocn.13152
Bjønness S, Grønnestad T, Storm M (2020) "I’m not a diagnosis: Adolescents’ perspectives on user participation and shared decision-making in mental healthcare. Scand J Child Adolesc Psychiatr Psychol 8:139–148. https://doi.org/10.21307/sjcapp-2020-014
Cousino MK et al (2023) Medical and end-of-life decision-making preferences in adolescents and young adults with advanced heart disease and their parents. JAMA Netw Open 6(5):e2311957–e2311957. https://doi.org/10.1001/jamanetworkopen.2023.11957
Jordan A, Joseph-Williams N, Edwards A, Holland-Hart D, Wood F (2019) I’d like to have more of a say because it’s my body: adolescents’ perceptions around barriers and facilitators to shared decision-making. J Adolesc Health 65(5):633–642. https://doi.org/10.1016/j.jadohealth.2019.05.024. (in eng)
Viksveen P et al (2022) User involvement in adolescents’ mental healthcare: a systematic review. Eur Child Adolesc Psychiatr 31(11):1765–1788. https://doi.org/10.1007/s00787-021-01818-2
Weaver MS, Baker JN, Gattuso JS, Gibson DV, Sykes AD, Hinds PS (2015) Adolescents’ preferences for treatment decisional involvement during their cancer. Cancer 121(24):4416–4424. https://doi.org/10.1002/cncr.29663
Bjønness S, Grønnestad T, Johannessen JO, Storm M (2022) Parents’ perspectives on user participation and shared decision-making in adolescents’ inpatient mental healthcare. Health Expect 25(3):994–1003. https://doi.org/10.1111/hex.13443. (in eng)
Vanwymelbeke J et al (2023) Clinical adolescent decision-making: Parental perspectives on confidentiality and consent in Belgium and The Netherlands. Ethics Behav 33:371–386. https://doi.org/10.1080/10508422.2022.2086873
Kon AA, Morrison W (2018) Shared decision-making in pediatric practice: a broad view. Pediatrics 142(Supplement 3):S129–S132. https://doi.org/10.1542/peds.2018-0516B
Park ES, Cho IY (2018) Shared decision-making in the paediatric field: a literature review and concept analysis. Scand J Caring Sci 32(2):478–489. https://doi.org/10.1111/scs.12496
Taub S, Lanocha N (2023) Shared decision-making in pediatrics: toward a more participatory model. Pediatr Rev 44(1):50–52. https://doi.org/10.1542/pir.2021-004984
Adams RC, Levy SE, (2017) Shared decision-making and children with disabilities: pathways to consensus. Pediatrics 139(6). https://doi.org/10.1542/peds.2017-0956
Boland L et al (2019) Barriers and facilitators of pediatric shared decision-making: a systematic review. Implement Sci 14(1):7. https://doi.org/10.1186/s13012-018-0851-5
EAP. About Adolescent Health Strategic Advisory Group. Accessed 20 Jun 2023
Elsevier. "Emtree - Embase." https://www.embase.com/emtree?id=5556&term=adolescence. Accessed 20 Jun 2023
NLM. "Adolescent - MeSH - NCBI." https://www.ncbi.nlm.nih.gov/pubmed/. Accessed 20 June 2023
Gonzalez SC, Preiss RM, Allende-Richter S (2019) Contraceptive shared decision-making: an innovative approach in adolescent and young adults contraceptive counseling. Clin Pediatr 58(4):466–469. https://doi.org/10.1177/0009922818821884
Chen K-L et al (2021) Shared Decision-Making Model for Adolescent Smoking Cessation: Pilot Cohort Study," International Journal of Environmental Research and Public Health, vol. 18, no. 20, p. 10970. [Online]. Available: https://www.mdpi.com/1660-4601/18/20/10970https://mdpi-res.com/d_attachment/ijerph/ijerph-18-10970/article_deploy/ijerph-18-10970-v2.pdf?version=1634718765. Accessed 8 May 2023
Alden DL et al (2018) Who decides: me or we? Family involvement in medical decision making in Eastern and Western Countries. Med Decis Making 38(1):14–25. https://doi.org/10.1177/0272989x17715628
Willekens M et al (2023) Is blood thicker than water? Perceptions on the role of stepparents in medical decisions among minors. J Child Health Care 13674935231211217. https://doi.org/10.1177/13674935231211217
Ragsdale JR, Hegner MA, Mueller M, Davies S (2014) Identifying religious and/or spiritual perspectives of adolescents and young adults receiving blood and marrow transplants: a prospective qualitative study. Biol Blood Marrow Transplant 20(8):1242–1247. https://doi.org/10.1016/j.bbmt.2014.04.013
de Snoo-Trimp J, de Vries A, Molewijk B, Hein I (2022) How to deal with moral challenges around the decision-making competence in transgender adolescent care? Development of an ethics support tool. BMC Med Ethics 23(1):96. https://doi.org/10.1186/s12910-022-00837-1. (in eng)
Matula KA, Minar P, Daraiseh NM, Lin L, Recker M, Lipstein EA (2022) Pilot trial of iBDecide: evaluating an online tool to facilitate shared decision making for adolescents and young adults with ulcerative colitis. Health Expect 25(6):3105–3113. https://doi.org/10.1111/hex.13618
Nagata JM, Hathi S, Ferguson BJ, Hindin MJ, Yoshida S, Ross DA (2018) Research priorities for adolescent health in low- and middle-income countries: a mixed-methods synthesis of two separate exercises. J Glob Health 8(1):010501. https://doi.org/10.7189/jogh.08.010501
Acknowledgements
The authors wish to thank Thomas Vandendriessche, Anouk D’Hont, Norin Hamouda, Krizia Tuand and Chayenne Van Meel, the reference librarians of KU Leuven Libraries – 2Bergen (Leuven, Belgium), for their help in conducting the systematic literature search.
Funding
The authors received no funding for this work.
Author information
Authors and Affiliations
Contributions
OS, RJ, JT and KD made substantial contributions to the study's conception and design. OS and RJ executed database searches and article screening, performed data extraction, analysis and synthesis, and actively engaged in manuscript drafting and revision. KD, JT provided intellectual input, supervision, performed data analysis and synthesis, reviewed methodological quality and contributed to manuscript review and revision. All authors carefully reviewed and granted approval of the final manuscript.
Corresponding author
Ethics declarations
Competing interests
Author 3 serves as Editorial Advisor for the European Journal of Pediatrics. The authors have no other competing interests to declare.
Additional information
Communicated by Peter de Winter
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Oluwaseun Rebecca Sobode and Roshni Jegan are both first authors.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sobode, O.R., Jegan, R., Toelen, J. et al. Shared decision-making in adolescent healthcare: a literature review of ethical considerations. Eur J Pediatr 183, 4195–4203 (2024). https://doi.org/10.1007/s00431-024-05687-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-024-05687-0