
Abstract
Sox10 is a transcription factor regulating the development of several cell lineages and is involved in tumor development. However, the clinicopathological relevance of Sox10 expression in ovarian cancer has not been examined. We assessed expression of Sox10 in ovarian epithelial tumors by immunohistochemistry and assessed its prognostic value by analyzing the correlation between its expression and clinicopathological factors. We used tissue microarrays including 244 ovarian epithelial tumors. Sox10 staining was found in the cytoplasm or nucleus of tumor cells. Malignant serous, mucinous, and endometrioid tumors were significantly more likely to express Sox10 than benign and borderline tumors. Expression patterns in adenocarcinomas were different for histologic subtypes: nuclear Sox10 staining was common in clear-cell adenocarcinomas and serous adenocarcinomas, whereas all cases of mucinous and endometrioid tumors were negative for nuclear staining. Nuclear Sox10 staining was also associated with chemoresistance and shorter overall survival in ovarian adenocarcinomas, notably in high-grade serous adenocarcinoma. Sox10 is expressed in many ovarian carcinomas, suggesting that it might be involved in oncogenesis of ovarian carcinoma. Expression pattern of Sox10 differs between histological subtypes. Nuclear Sox10 expression is an independent indicator of poor prognosis in ovarian adenocarcinomas, notably in high-grade serous adenocarcinomas.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ovarian epithelial tumors stand out as a result of an increasing incidence and high mortality, due to the late diagnosis and frequent recurrence. Despite numerous studies searching for prognostic markers which predict the risk of recurrence, no useful marker is yet available. For early diagnosis, accurate determination of prognosis and the development of tailored therapy, which might improve outcome for these patients, new markers are needed.
Sox10 is a transcription factor of the sex determining region Y (SRY)-related high motility group (HMG)-box gene family. It plays an important role in the maintenance and migration of neural crest stem cells [1–4], and in their differentiation into neural crest-derived melanocytes and glia [5, 6]. Loss-of-function mutations in Sox10 gene impair the development of neural cells and melanocytes, resulting in neurocristopathies such as Waardenburg syndrome, characterized by sensorineural hearing loss and hypopigmentation [5, 7, 8]. Sox10 also contributes to the maintenance of stem cell properties in the neural crest [9].
Sox10 is expressed in melanocytes and Schwann cells, and in the corresponding tumors [10]. Therefore, it can be used as a marker of peripheral neural tumors, melanocytic tumors [10, 11], and neural crest-derived tumors [12]. Sox10 is considered to be a more sensitive marker than S-100 for these tumors [11]. In addition, Sox10 has also been found in some human solid tumors. For example, in neuroendocrine tumors of the lung, it is expressed by sustentacular cells, the presence of which is inversely correlated with neuroendocrine tumor grade [13]. Sox10 expression has been reported in basal-like, triple-negative and metaplastic carcinoma of breast [14], acinic cell carcinoma, adenoid cystic carcinoma, myoepithelial carcinoma, pleomorphic adenoma of salivary gland [15, 16], and hepatocellular carcinoma [17]. Sox10 reportedly functions as an oncogene by cell cycle dysregulation in melanomagenesis [18], and by activating the Wnt/β-catenin cascade in hepatocellular carcinoma [17]. In contrast, Sox10 is silenced or downregulated in prostatic carcinoma [19] and in gastrointestinal cancer [20], suggesting that in these tumors, it might function as a tumor suppressor.
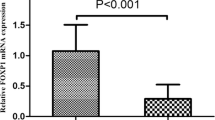
In ovarian carcinomas, the expression pattern and the role of Sox10 are controversial. In two previous studies that used tissue microarrays and immunohistochemistry to detect Sox10 expression in tumor tissue, all 26 samples of ovarian carcinoma were negative for Sox10 [11, 21]. However, we previously showed that Sox10 mRNA expression is upregulated in chemoresistant ovarian serous carcinomas compared to chemosensitive carcinomas and normal control tissues [22].
To clarify whether or not Sox10 is expressed in ovarian carcinomas, we examined Sox10 protein expression in 244 ovarian epithelial tumors by immunohistochemical staining on a tissue microarray. We also determined if Sox10 expression might constitute a valuable marker for differential diagnosis or prognosis and compared its expression with clinicopathological parameters and patient survival.
Materials and methods
Tissue samples and pathologic examination
We studied formalin-fixed, paraffin-embedded ovarian epithelial tumor tissue samples from 244 women who had been treated at the CHA Bundang Medical Center between 1998 and 2013. Treatment consisted of radical surgery followed by a first-line chemotherapy regimen, consisting of paclitaxel and cisplatin or carboplatin. Chemoresistance was defined as persistent or recurrent carcinoma within 6 months after initiation of first-line Taxol-platinum chemotherapy, according to the National Comprehensive Cancer Network (NCCN) guidelines.
Clinicopathological data were obtained from clinical databases of the hospital. The histological subtype of each ovarian tumor had been determined according to the World Health Organization classification. Clinical stage had been evaluated according to the criteria of the International Federation of Gynecology and Obstetrics (FIGO). Histopathologic grading of serous adenocarcinoma was assessed according to a two-tiered system of high grade (HG) and low grade (LG).
Tissue microarray
Tissue samples were retrieved from the tumor bank of the CHA Bundang Medical Center, School of Medicine, CHA University. Hematoxylin and eosin (H&E)-stained sections of the selected cases were reviewed, and representative areas were marked on the H&E-stained sections and corresponding paraffin blocks. For each case, three tissue cores with a diameter of 2 or 3 mm were punched out from the marked tissue areas of each donor tissue block. They were then arranged into recipient paraffin blocks using a manual microarray device (UNITMA, Quick-RAY, UNITech Science, Seoul, Korea).
Immunohistochemical analysis
Tissue microarrays were deparaffinized in xylene for 30 min and rehydrated in a graded series of alcohol. Endogenous peroxidase activity was blocked via 30 min of treatment with 3 % hydrogen peroxide in methanol. For antigen retrieval, the sections were heated in 0.1 mol/l citrate buffer (pH 6.0) for 15 min in a microwave oven. Slides were incubated for 60 min at room temperature with mouse monoclonal anti-human Sox10 antibody (ab122977; 1:150 dilution; Abcam, Cambridge, UK) in 0.3 % bovine serum albumin (BSA) in Tris-buffered saline (pH 7.4). They were then incubated for 30 min with a secondary antibody using a HRP Polymer Ultravision LP Detection System (Thermo Scientific, Waltham, MA, USA) at room temperature. The sections were then developed with diaminobenzidine and counterstained with hematoxylin. Immunohistochemical staining was interpreted by two independent pathologists. Expression of Sox10 was considered positive when >25 % of tumor cells in the three cores of a sample were stained. As control, we used neurogenic tumors, such as schwannoma, which were diffusely positive for Sox10.
Statistical analyses
Statistical analysis was conducted using the SPSS statistics software package (IBM SPSS Statistics version 20). Associations between Sox10 expression and clinicopathological factors were evaluated using χ 2 analysis. For survival analysis, the Kaplan-Meier method, log-rank test, and Cox proportion hazard model were used. All tests were two-sided, and p < 0.05 was considered significant.
Results
Clinicopathological characteristics
We enrolled 244 women in the study, with an age range from 19 to 86 years (mean 47.9 years); 94 patients (38.5 %) were ≥50 years. Histological types included 131 serous tumors, 73 mucinous tumors, 32 endometrioid tumors, and 8 clear-cell carcinomas. Of the 123 patients with a malignant tumor, including all tumor types, 41 % had nodal metastases and 25 % had distant metastases (Table 1). FIGO stages in these 123 cases were stage I, 28 %; stage II, 10 %; stage III, 46 %; and stage IV, 16 %.
Of the 80 patients with HG serous adenocarcinoma, 53 % had nodal metastases and 34 % had distant metastases. FIGO stages in these cases was stage I, 6 (8 %); stage II, 10 (13 %); stage III, 45 (56 %); and stage IV, 19 (24 %). Chemoresistance was recorded in 39 % of these cases.
Sox10 expression in ovarian epithelial tumors
In all 244 cases, focal or diffuse Sox10 staining was observed in the cytoplasm or nucleus of ovarian epithelial tumor cells (Fig. 1). The results of staining for each histological tumor type are presented in Table 2. Cytoplasmic staining was seen in 86 % of HG serous adenocarcinomas, 75 % of endometrioid adenocarcinomas, 50 % of mucinous adenocarcinomas, and in <50 % of cases for the other tumor types. Nuclear staining was seen in 63 % of clear-cell carcinomas, 23 % of HG serous adenocarcinomas, 22 % of LG serous adenocarcinomas, and 4 % of serous borderline tumors, while it was negative in all other tumor types.

Immunohistochemical staining of Sox10 in ovarian epithelial tumors. (a, b) Negative staining in serous cystadenoma (a) and serous borderline tumor (b); c positive nuclear Sox10 staining in serous adenocarcinoma; d, e no reactivity in mucinous cystadenoma (d) and mucinous borderline tumor (e); f positive cytoplasmic staining in mucinous adenocarcinoma; g no reactivity in endometriotic cyst; h endometrioid adenocarcinoma showing cytoplasmic Sox10 staining; i positive nuclear Sox10 staining in clear-cell carcinoma
The immunohistochemical staining pattern of Sox10 was compared between the various ovarian tumor types (Fig. 2). For cytoplasmic staining (Fig. 2a), a significant association was found with malignancy in serous (p < 0.001), mucinous (p < 0.001), and endometrioid tumors (p = 0.0046). For nuclear staining, a significant association was found with malignancy in serous tumors (Fig. 2b), with lower number of positive cases in benign and borderline tumors (p = 0.022 for LG serous adenocarcinoma, and p = 0.004 for HG serous adenocarcinoma.)

a High-grade serous, mucinous, and endometrioid adenocarcinomas have significantly higher expression of cytoplasmic Sox10 than benign or borderline tumors (p < 0.001, p < 0.001, and p = 0.0046, respectively, χ 2 test). b In serous adenocarcinomas, nuclear Sox10 expression is significantly higher than in serous benign or borderline tumors (p = 0.022 for low-grade serous adenocarcinoma and p = 0.004 for high-grade serous adenocarcinoma, χ 2 test). c Serous and endometrioid adenocarcinomas were significantly more likely to have cytoplasmic Sox10 expression than clear-cell carcinoma (p < 0.001 and p = 0.004, respectively). Cytoplasmic Sox10 expression in serous adenocarcinoma was more frequent than in mucinous adenocarcinoma (p = 0.005). Nuclear Sox10 expression in clear-cell carcinoma was significantly more frequent than in high-grade serous, mucinous, or endometrioid adenocarcinomas (p = 0.014, p = 0.003, and p < 0.001, respectively, χ 2 test)
Cytoplasmic Sox10 staining of HG serous, endometrioid, and mucinous adenocarcinomas was more frequent than that of clear-cell carcinomas (Fig. 2c), but the difference was statistically significant only for HG serous and endometrioid adenocarcinomas (p < 0.001 and p = 0.004, respectively). Nuclear staining was more frequent in clear-cell carcinomas than in HG serous (p = 0.014), mucinous (p = 0.003), and endometrioid (p < 0.001) while a nonsignificant trend was found for LG serous adenocarcinomas (p = 0.092).
Correlation between Sox10 staining and clinicopathologic parameters in serous adenocarcinomas
We analyzed associations between Sox10 staining and clinicopathological parameters in 80 cases of HG serous adenocarcinomas, the most frequent and lethal type of ovarian carcinoma. Cytoplasmic Sox10 staining was not significantly associated with any clinicopathological factor. Nuclear Sox10 staining was positively associated only with chemoresistance (Table 3, p = 0.006). Nuclear staining was found in 39 % of chemoresistant but in only 12 % of cases of chemosensitive serous adenocarcinomas. Patient age, FIGO stage, and the presence of nodal or distant metastases were not associated with nuclear Sox10 staining.
Association of Sox10 immunoreactivity with overall survival
Survival analyses were separately performed for the 123 adenocarcinomas and separately for the 80 HG serous adenocarcinomas (Fig. 3). Median follow-up was 51.1 months (range, 0.6–141.1 months). During the follow-up period, 30 of the 123 patients (24 %) died of disease, including 21 patients with HG serous adenocarcinoma. Kaplan-Meier analysis revealed that nuclear Sox10 staining (n = 25) was associated with shorter overall survival (81 % (79/98) vs. 56 % (14/25)) in patients with ovarian adenocarcinoma (Fig. 3a, p = 0.013). As shown in Fig. 3b, nuclear Sox10 staining in HG serous adenocarcinoma was also associated with poorer overall survival. For the group with nuclear Sox10 staining overall survival was significantly lower (8/18, 44 %) than for the nuclear Sox10 negative group (51/62, 82 %) (p < 0.001).

Kaplan-Meier survival curves for nuclear Sox10 immunoreactivity. a In the 123 patients with ovarian adenocarcinoma, nuclear Sox10 expression correlated with poorer overall survival rate (p = 0.013, log-rank). b Among the 80 patients with high-grade serous adenocarcinoma, nuclear Sox10 positivity also associated with poor overall survival (p < 0.001, log-rank)
We also performed multivariate Cox regression (Table 4). In the 123 adenocarcinomas, nuclear Sox10 positivity (HR = 3.408, p < 0.002) and higher stage (HR = 13.806, p < 0.001) were independent predictors of poor survival. Similarly, in the 80 HG serous adenocarcinomas, nuclear Sox10 positivity (HR = 6.613, p < 0.001), and higher stage (HR = 8.015, p = 0.046) were significantly associated with poor overall survival, suggesting that nuclear Sox10 positivity is an independent indicator of poor prognosis.
Discussion
Ovarian carcinoma accounts for the largest proportion of tumor-related mortality of all gynecological malignancies [23], due to late detection and frequent recurrence [24, 25]. There have been many efforts to develop biomarkers for early detection of the disease and for accurate prognosis but as yet without conclusive or reproducible results. One of the reasons for this is that ovarian carcinomas are heterogeneous in view of the existence of serous, endometrioid, clear cell, and mucinous subtypes, each of these subtypes being associated with different molecular pathogenetic events and a different response to therapy [26–28]. Development of biomarkers for early diagnosis and prognosis of the different subtypes is necessary.
In a previous study on genes related to chemoresistance in ovarian cancer, we found that Sox10 mRNA expression is significantly upregulated in HG serous adenocarcinomas compared to normal controls and in chemoresistant carcinomas compared to chemosensitive ones [22]. We therefore studied expression characteristics of Sox10 protein, to determine if Sox10 can be used as a marker for differential diagnosis or to predict outcome in various types of ovarian carcinoma.
Sox genes belong to the high mobility group superfamily and encode transcription factors. They regulate various developmental processes, and their encoded proteins are involved in different tumors as tumor promoter or suppressor. Sox10 is overexpressed in peripheral neural and melanocytic tumors [11] and in solid tumors such as neuroendocrine tumor of the lung [13], basal-like, triple-negative and metaplastic carcinoma of breast [14], and hepatocellular carcinoma [17]. Sox10 knockdown in human melanoma cells induces senescence and suppresses melanomagenesis [18]. Sox10 was reported to be significantly upregulated in hepatocellular carcinoma, and it induced proliferation of hepatocellular carcinoma cells and elevation of β-catenin levels [17], which formed a Sox10/TCF4/β-catenin complex to transactivate downstream target genes. Therefore, Sox10 is considered as an oncogene in melanoma and hepatocellular carcinoma. In contrast, Sox10 functions as a tumor suppressor in some other tumors. Sox10 inhibits the Wnt/β-catenin signaling pathway in digestive carcinomas by interacting with β-catenin [20]. Interaction of Sox10 with β-catenin inhibits tumor cell survival, metastasis, and epithelial-mesenchymal transition and suppresses stem cell properties [20]. Similarly, Sox10 was found downregulated in prostate carcinoma tissue compared to benign prostate tissue. In prostate carcinoma, low immunoreactivity of Sox10 was associated with high PSA level and advanced pathological stage [19]. Clearly, the role of Sox10 in oncogenesis of epithelial tumors needs to be further elucidated.
We found that in ovarian carcinomas, Sox10 expression is associated with oncogenic properties. Sox10 expression was significantly more common in ovarian adenocarcinomas, including serous, mucinous, and endometrioid types than in their benign and borderline counterparts. This result is in contrast with those of a previous study, reporting that Sox10 is not expressed in ovarian carcinomas (21 serous and 2 clear-cell carcinomas) [21]. The number of cases in this study, however, was small, smaller tissue cores were used as well as a different primary antibody, a goat polyclonal antibody raised against a peptide mapping at the N-terminus of Sox10, whereas we used a mouse monoclonal antibody raised against recombinant human Sox10. The different sources of antibody and different epitope specificity might be responsible for these differences in immunohistochemical staining.
The adenocarcinomas in our study showed distinct Sox10 expression patterns according to histological type. Serous and clear cell types showed both nuclear and cytoplasmic staining, whereas mucinous and endometrioid types showed only cytoplasmic staining, suggesting that the pathobiology of ovarian adenocarcinoma subtypes is different, particularly between mucinous and serous types. Of note, nuclear Sox10 expression was more common in clear-cell adenocarcinoma (63 %) than in other types (0–23 %), which suggests that it might be a useful differential marker for clear-cell carcinoma.
We found nuclear expression of Sox10 to be positively associated with chemoresistance, in agreement with our previous report with higher expression of Sox10 mRNA in chemoresistant HG serous adenocarcinomas [22]. We hypothesize that this is associated with the stem cell supporting properties of Sox10 in normal tissues and cancer [29, 30]. Nuclear Sox10 staining was also significantly associated with shorter overall survival, and an independent marker of poor prognosis in both serous adenocarcinomas and all ovarian adenocarcinomas. Considering that Sox10 is a transcription factor, increased nuclear expression of Sox10 may be related to aggressiveness of a malignant tumor. In hepatocellular carcinoma cells, Sox10 promotes proliferation and facilitates TCF4 binding to β-catenin, the stable Sox10/TCF4/β-catenin complex activating downstream target genes [17].
We found cytoplasmic Sox10 staining in serous adenocarcinomas and in a small proportion of clear-cell carcinomas but not in association with aggressiveness. The function of cytoplasmic Sox10 is not clear. Rehberg et al. [31], however, demonstrated Sox10 nucleo-cytoplasmic shuttling in HeLa and C6 cells. The active leucine-rich nuclear export signal of Sox10 appeared to be a key determinant this nucleo-cytoplasmic shuttling and inhibition of nuclear export of Sox10 by an export-defective mutation decreased transactivation of endogenous target genes. These data suggest that Sox10 nucleo-cytoplasmic shuttling may be important in its DNA-binding activity. Cytoplasmic Sox10 expression has also been reported in prostatic adenocarcinoma, but not in association with poor survival [19]. In a study on adenoid cystic carcinomas, nuclear Sox10 staining was intense and cytoplasmic staining was detectable in a majority of tumor cells [15]. Further studies on molecular mechanisms associated with cytoplasmic expression of Sox10 are clearly needed.
In conclusion, we found that Sox10 is expressed in most types of ovarian carcinoma and with different expression patterns in different histological types. We also found nuclear Sox10 expression to be an independent indicator of poor survival in ovarian carcinomas. Further studies on the molecular mechanisms involved and eventual therapeutic importance of Sox10 in ovarian carcinomas are warranted.
References
Drerup CM, Wiora HM, Topczewski J, Morris JA (2009) Disc1 regulates foxd3 and sox10 expression, affecting neural crest migration and differentiation. Development (Cambridge, England) 136(15):2623–2632. doi:10.1242/dev.030577
Kuhlbrodt K, Herbarth B, Sock E, Hermans-Borgmeyer I, Wegner M (1998) Sox10, a novel transcriptional modulator in glial cells. J Neurosci off J Soc Neurosci 18(1):237–250
McKeown SJ, Lee VM, Bronner-Fraser M, Newgreen DF, Farlie PG (2005) Sox10 overexpression induces neural crest-like cells from all dorsoventral levels of the neural tube but inhibits differentiation. Dev Dynamics:Off Pub Am Assoc Anatomists 233(2):430–444. doi:10.1002/dvdy.20341
Miyahara K, Kato Y, Koga H, Dizon R, Lane GJ, Suzuki R, Akazawa C, Yamataka A (2011) Visualization of enteric neural crest cell migration in SOX10 transgenic mouse gut using time-lapse fluorescence imaging. J Pediatr Surg 46(12):2305–2308. doi:10.1016/j.jpedsurg.2011.09.020
Kelsh RN (2006) Sorting out Sox10 functions in neural crest development. BioEssays: News and Rev Mol, Cell Dev Biol 28(8):788–798. doi:10.1002/bies.20445
Mollaaghababa R, Pavan WJ (2003) The importance of having your SOX on: role of SOX10 in the development of neural crest-derived melanocytes and glia. Oncogene 22(20):3024–3034. doi:10.1038/sj.onc.1206442
Lee KE, Nam S, Cho EA, Seong I, Limb JK, Lee S, Kim J (2008) Identification of direct regulatory targets of the transcription factor Sox10 based on function and conservation. BMC Genomics 9:408. doi:10.1186/1471-2164-9-408
Pingault V, Bondurand N, Kuhlbrodt K, Goerich DE, Prehu MO, Puliti A, Herbarth B, Hermans-Borgmeyer I, Legius E, Matthijs G, Amiel J, Lyonnet S, Ceccherini I, Romeo G, Smith JC, Read AP, Wegner M, Goossens M (1998) SOX10 mutations in patients with Waardenburg-Hirschsprung disease. Nat Genet 18(2):171–173. doi:10.1038/ng0298-171
Kim J, Lo L, Dormand E, Anderson DJ (2003) SOX10 maintains multipotency and inhibits neuronal differentiation of neural crest stem cells. Neuron 38(1):17–31
Chan JK (2013) Newly available antibodies with practical applications in surgical pathology. Int J Surg Pathol 21(6):553–572. doi:10.1177/1066896913507601
Nonaka D, Chiriboga L, Rubin BP (2008) Sox10: a pan-schwannian and melanocytic marker. Am J Surg Pathol 32(9):1291–1298. doi:10.1097/PAS.0b013e3181658c14
Karamchandani JR, Nielsen TO, van de Rijn M, West RB (2012) Sox10 and S100 in the diagnosis of soft-tissue neoplasms. Appl Immunohistochem Mol Morphol 20(5):445–450. doi:10.1097/PAI.0b013e318244ff4b
Tsuta K, Raso MG, Kalhor N, Liu DC, Wistuba II, Moran CA (2011) Sox10-positive sustentacular cells in neuroendocrine carcinoma of the lung. Histopathology 58(2):276–285. doi:10.1111/j.1365-2559.2011.03747.x
Cimino-Mathews A, Subhawong AP, Elwood H, Warzecha HN, Sharma R, Park BH, Taube JM, Illei PB, Argani P (2013) Neural crest transcription factor Sox10 is preferentially expressed in triple-negative and metaplastic breast carcinomas. Hum Pathol 44(6):959–965. doi:10.1016/j.humpath.2012.09.005
Ivanov SV, Panaccione A, Nonaka D, Prasad ML, Boyd KL, Brown B, Guo Y, Sewell A, Yarbrough WG (2013) Diagnostic SOX10 gene signatures in salivary adenoid cystic and breast basal-like carcinomas. Br J Cancer 109(2):444–451. doi:10.1038/bjc.2013.326
Ohtomo R, Mori T, Shibata S, Tsuta K, Maeshima AM, Akazawa C, Watabe Y, Honda K, Yamada T, Yoshimoto S, Asai M, Okano H, Kanai Y, Tsuda H (2013) SOX10 is a novel marker of acinus and intercalated duct differentiation in salivary gland tumors: a clue to the histogenesis for tumor diagnosis. Mod Pathol 26(8):1041–1050. doi:10.1038/modpathol.2013.54
Zhou D, Bai F, Zhang X, Hu M, Zhao G, Zhao Z, Liu R (2014) SOX10 is a novel oncogene in hepatocellular carcinoma through Wnt/beta-catenin/TCF4 cascade. Tumour Biol 35(10):9935–9940. doi:10.1007/s13277-014-1893-1
Cronin JC, Watkins-Chow DE, Incao A, Hasskamp JH, Schonewolf N, Aoude LG, Hayward NK, Bastian BC, Dummer R, Loftus SK, Pavan WJ (2013) SOX10 ablation arrests cell cycle, induces senescence, and suppresses melanomagenesis. Cancer Res 73(18):5709–5718. doi:10.1158/0008-5472.can-12-4620
Zhong WD, Qin GQ, Dai QS, Han ZD, Chen SM, Ling XH, Fu X, Cai C, Chen JH, Chen XB, Lin ZY, Deng YH, Wu SL, He HC, Wu CL (2012) SOXs in human prostate cancer: implication as progression and prognosis factors. BMC Cancer 12:248. doi:10.1186/1471-2407-12-248
Tong X, Li L, Li X, Heng L, Zhong L, Su X, Rong R, Hu S, Liu W, Jia B, Liu X, Kou G, Han J, Guo S, Hu Y, Li C, Tao Q, Guo Y (2014) SOX10, a novel HMG-box-containing tumor suppressor, inhibits growth and metastasis of digestive cancers by suppressing the Wnt/beta-catenin pathway. Oncotarget 5(21):10571–10583
Mohamed A, Gonzalez RS, Lawson D, Wang J, Cohen C (2013) SOX10 expression in malignant melanoma, carcinoma, and normal tissues. Appl Immunohistochem Mol Morphol 21(6):506–510. doi:10.1097/PAI.0b013e318279bc0a
Kang KW, Lee MJ, Song JA, Jeong JY, Kim YK, Lee C, Kim TH, Kwak KB, Kim OJ, An HJ (2014) Overexpression of goosecoid homeobox is associated with chemoresistance and poor prognosis in ovarian carcinoma. Oncol Rep 32(1):189–198. doi:10.3892/or.2014.3203
Siegel R, Ma J, Zou Z, Jemal A (2014) Cancer statistics, 2014. CA Cancer J Clin 64(1):9–29. doi:10.3322/caac.21208
Davidson B, Trope CG (2014) Ovarian cancer: diagnostic, biological and prognostic aspects. Women’s Health (Lond Engl) 10(5):519–533. doi:10.2217/whe.14.37
du Bois A, Luck HJ, Meier W, Adams HP, Mobus V, Costa S, Bauknecht T, Richter B, Warm M, Schroder W, Olbricht S, Nitz U, Jackisch C, Emons G, Wagner U, Kuhn W, Pfisterer J (2003) A randomized clinical trial of cisplatin/paclitaxel versus carboplatin/paclitaxel as first-line treatment of ovarian cancer. J Natl Cancer Inst 95(17):1320–1329
Kurman RJ, Shih Ie M (2010) The origin and pathogenesis of epithelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol 34(3):433–443. doi:10.1097/PAS.0b013e3181cf3d79
Nezhat FR, Apostol R, Nezhat C, Pejovic T (2015) New insights in the pathophysiology of ovarian cancer and implications for screening and prevention. Am J Obstet Gynecol 213(3):262–267. doi:10.1016/j.ajog.2015.03.044
Kurman RJ (2013) Origin and molecular pathogenesis of ovarian high-grade serous carcinoma. Annals of Oncology: Official Journal of the European Society For Medical Oncology/ESMO 24(Suppl 10):x16–x21. doi:10.1093/annonc/mdt463
Wong CE, Paratore C, Dours-Zimmermann MT, Rochat A, Pietri T, Suter U, Zimmermann DR, Dufour S, Thiery JP, Meijer D, Beermann F, Barrandon Y, Sommer L (2006) Neural crest-derived cells with stem cell features can be traced back to multiple lineages in the adult skin. J Cell Biol 175(6):1005–1015. doi:10.1083/jcb.200606062
Civenni G, Walter A, Kobert N, Mihic-Probst D, Zipser M, Belloni B, Seifert B, Moch H, Dummer R, van den Broek M, Sommer L (2011) Human CD271-positive melanoma stem cells associated with metastasis establish tumor heterogeneity and long-term growth. Cancer Res 71(8):3098–3109. doi:10.1158/0008-5472.CAN-10-3997
Rehberg S, Lischka P, Glaser G, Stamminger T, Wegner M, Rosorius O (2002) Sox10 is an active nucleocytoplasmic shuttle protein, and shuttling is crucial for Sox10-mediated transactivation. Mol Cell Biol 22(16):5826–5834. doi:10.1128/MCB.22.16.5826-5834.2002
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by the Ethics Committee of the CHA Bundang Medical Center, and informed consent was obtained from all patients.
Conflict of interest
The authors declare that they have no conflicts of interest.
Funding
This research was supported by the Basic Science Research Program funded by the Korean Government (grants NRF-2015-R1A2A2A01005197 and KHIDI-A111804).
Rights and permissions
About this article

Cite this article
Kwon, AY., Heo, I., Lee, H.J. et al. Sox10 expression in ovarian epithelial tumors is associated with poor overall survival. Virchows Arch 468, 597–605 (2016). https://doi.org/10.1007/s00428-016-1918-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-016-1918-9