
Abstract
The maximal fat oxidation rate (MFO) assessed during a graded exercise test is a remarkable physiological indicator associated with metabolic flexibility, body weight loss and endurance performance. The present review considers existing biomarkers related to MFO, highlighting the validity of maximal oxygen uptake and free fatty acid availability for predicting MFO in athletes and healthy individuals. Moreover, we emphasize the role of different key enzymes and structural proteins that regulate adipose tissue lipolysis (i.e., triacylglycerol lipase, hormone sensitive lipase, perilipin 1), fatty acid trafficking (i.e., fatty acid translocase cluster of differentiation 36) and skeletal muscle oxidative capacity (i.e., citrate synthase and mitochondrial respiratory chain complexes II–V) on MFO variation. Likewise, we discuss the association of MFO with different polymorphism on the ACE, ADRB3, AR and CD36 genes, identifying prospective studies that will help to elucidate the mechanisms behind such associations. In addition, we highlight existing evidence that contradict the paradigm of a higher MFO in women due to ovarian hormones activity and highlight current gaps regarding endocrine function and MFO relationship.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Skeletal muscle comprises ~ 40% of total body mass and poses relevant implications for metabolic health and sports performance. A poor fat oxidation in skeletal muscle may lead to the accumulation of lipid intermediates such as diacylglycerols and ceramides which are considered “lipotoxic” and are related to insulin sensitivity (Goodpaster and Sparks 2017; Arad et al. 2020). On the other hand, increasing fat oxidation in skeletal muscle through exercise training will reduce glycogenolysis rate, delaying glycogen depletion which is related to muscle fatigue (Holloszy and Coyle 1984; Ørtenblad and Nielsen 2015; Hearris et al. 2018).
The maximal fat oxidation rate (MFO) observed at submaximal exercise intensity during an incremental-load exercise test represents the capacity of the skeletal muscle to use fatty acids as a fuel when energy demand raises by muscle contraction (Fig. 1). Since introduced by Jeukendrup and Achten (2001), many studies have analyzed the validity of this parameter as a marker of metabolic flexibility and a predictor of sports performance in endurance athletes, reporting that (1) MFO is directly related to insulin sensitivity (r = 0.33, p < 0.01) and 24-h fat oxidation (r = 0.65, p < 0.01) in healthy males (Robinson et al. 2015); (2) predicts total fat oxidation during steady-state exercise in men with obesity (R2 = 0.46, p < 0.01) (Chávez-Guevara et al. 2021) and is positively associated with exercise fat oxidation in the postprandial state in trained males (r = 0.83, p < 0.01) (Maunder et al. 2021); (3) is related with fat mass loss induced by exercise training performed at MFO intensity (FATmax) in subjects with obesity (r = 0.35, p < 0.01) (Drapier et al. 2018); (4) it explains 12 and 14% of endurance performance on Ironman (Frandsen et al. 2017) and ultra-trail male athletes, respectively (Martinez-Navarro et al. 2020). The aforementioned evidence highlights the relevance of investigating those biological and nutritional factors as well as the fitness components that determine MFO to understand the molecular and physiological mechanisms affecting metabolic health and athletic performance.

Biomarkers, health-related components of physical fitness and genetic polymorphism related to maximal fat oxidation (MFO). Those biomarkers and health-related components previously validated as MFO predictors are highlighted in green color while those biomarkers that have only been correlated with MFO are remarked in purple. The biomarkers that are not associated with MFO are colored in red those biomarkers whose relationship with MFO has not been analyzed (but could be associated) are highlighted in orange. ATGL triacylglycerol lipase, ACSL1 acyl-CoA synthetase, CS citrate synthase, CPT1 carnitine palmitoyl transferase 1, ERα estrogen receptor alpha, ECT electron transport chain, FATBP fatty acid binding protein, FATmax exercise intensity eliciting maximal fat oxidation, FFA free fatty acids, HAD β-hydroxy-acyl-CoA-dehydrogenase, HSL hormone sensitive lipase, MFO maximal fat oxidation, IMCL intramuscular lipids, MitoVD mitochondrial volume density, OXPHOS mitochondrial oxidative phosphorylation capacity, PLIN perilipin, VO2max maximal oxygen uptake. The fat oxidation and blood lactate kinetics showed in this figure correspond to Author’s experimental data collected from an incremental-load exercise test performed on a patient with obesity
Previous investigations reported that cardiorespiratory fitness (CRF), body fat, exercise intensity eliciting MFO (FATmax), and fasting duration before the exercise test accounted for 47% of MFO intra-individual variance in athletes (Randell et al. 2017). In a similar way, the CRF, self-reported physical activity level, fat mass, fat-free mass (FFM), biological sex, and macronutrient content of the diet determined 46% of MFO variance in healthy untrained individuals (Fletcher et al. 2017). The physiological mechanisms explaining the association of the variables mentioned above with MFO have been described by Purdom et al. (2018) while Maunder et al. (2018) and Amaro-Gahete et al. (2018) provided MFO and FATmax values for trained and untrained individuals with different nutritional status. Nevertheless, determinants of MFO in endurance athletes, people with chronic diseases and elderly adults require further analysis.
Several studies suggest that women have greater fat oxidation than men, when MFO is expressed as mg kg FFM−1 min−1 (Venables et al. 2005; Fletcher et al. 2017; Maunder et al. 2018). In these studies, females showed a lower FFM in comparison to males. Thus, when adjusting MFO relative to FFM this may result on females exhibiting a higher fat oxidation, because the regression of fat oxidation on FFM has a significant positive intercept. Nonetheless, Chrzanowski-Smith et al. (2021) reported that women exhibited a greater MFO relative to FFM in comparison to men even when both groups were matched by muscle mass. Moreover, a recent meta-analysis evidenced that sedentary women shows a higher reliance on fat oxidation during moderate intensity exercise in comparison to sedentary men (Cano et al. 2021). In this regard, several physiological mechanisms have been related with sex-based differences in fat oxidation, including (1) elevated lipolytic rate in adipose tissue; (2) elevated levels of estrogens; (3) increased proportion of type 1 muscle fibers; (4) elevated intramuscular lipids concentration. Therefore, is necessary to elucidate whether MFO is predicted by similar variables between sexes.
On the other hand, up to 50% of MFO variation remain unexplained and biomarkers representing adipose tissue metabolism and skeletal muscle oxidative capacity (i.e., lipolytic enzymes, circulating free fatty acids, mitochondrial content, hormones) could be involved in oxidative capacity processes affecting MFO (Muscella et al. 2020). In addition, Randell et al. (2017) pointed out that MFO could be also regulated by genetic and epigenetic factors, including several genetic polymorphisms associated with circulating fatty acid availability (Li et al. 2016), fat oxidation during physical exercise (Morita et al. 2009) and skeletal muscle fiber type composition (Ahmetov et al. 2012). Therefore, the present review considers several biomarkers and genetic polymorphism related to MFO, with particular emphasis on those biomarkers that have been validated as MFO predictor. Moreover, we describe the mechanisms behind such associations and discuss existing evidence regarding the effect of exercise training over all biomarkers and MFO. Furthermore, we identify prospective studies that will help to elucidate the molecular mechanism that may predispose to a low-fat oxidation phenotype leading to metabolic diseases and a poor physical performance.
Biomarkers associated with exercise-induced maximal fat oxidation rate
Several biomarkers regarding CRF, endocrine function, fatty acid metabolism and skeletal oxidative capacity have been related with MFO observing contrasting results depending on training status and biological sex (Table 1).
Cardiorespiratory fitness
Data from Venables et al. (2005) and Fletcher et al. (2017) showed that CRF is the main determinant of MFO variance in healthy individuals with low to moderate physical activity level (see standardized β coefficients reported in Table 1). In support of this, a positive and strong association between VO2max/peak and MFO has been reported in a combined group of trained/untrained individuals (R2 = 0.59, p < 0.01) (Nordby et al. 2006) and endurance trained males (R2 = 0.78, p < 0.01) (Amaro-Gahete et al. 2019a), with a modest association reported on female ironman athletes (R2 = 0.27, p < 0.01) (Vest et al. 2018), sedentary young adults with overweight (R2 = 0.26, p < 0.01) and obesity (R2 = 0.10, p < 0.05) (Amaro-Gahete et al. 2019b), and sedentary middle-aged adults (R2 = 0.13, p < 0.01) (Amaro-Gahete et al. 2021). In the same way, a positive and significant correlation between VO2max/peak and MFO has been reported in trained men (r: 0.52–0.65) (Robinson et al. 2016; Zurbuchen et al. 2020; Chrzanowski-Smith et al. 2021), combined groups of trained/untrained individuals (r: 0.72–0.84) (Dandanell et al. 2018; Shaw et al. 2020) as well as sedentary subjects with obesity (r = 0.59, p < 0.01) (Haufe et al. 2010), suggesting that improving CRF would lead to an increment on MFO.
Effect of exercise training over VO 2max and MFO
In this regard, a concomitant increment in MFO (∆: 0.03–0.07 g min−1) and VO2max was reported in adolescents and elderly adults with obesity after 8–10 weeks of exercise training at FATmax (Chávez-Guevara et al. 2020). Indeed, recent studies in young (20–40 years old) and middle-aged sedentary adults (40–65 years old) observed that changes in VO2max/peak induced by endurance training (3 days/week; 300 or 600 kcal day−1 above 70% VO2peak) (Rosenkilde et al. 2015) or high intensity interval training (HIIT) (40–65 min per week at an intensity of > 95% VO2max) (Amaro-Gahete et al. 2020) predicted MFO increments, demonstrating that enhancing CRF improves fat metabolism in untrained subjects. Up to date, the chronic effect of an exercise training intervention over MFO in athletic population remains unexplored. Nonetheless, Achten and Jeukendrup (2003a) reported that MFO was 16% higher in endurance trained men with high vs. low VO2max (71.9 ± 6.1 vs. 58.6 ± 5.2 mL kg−1 min−1). In the same way, a significant mean difference in MFO levels (~ 0.18 g min−1) was observed between long-distance male runners with high vs. low VO2max (68.4 ± 4.5 vs. 58.6 ± 5.4 mL kg−1 min−1) (Lima-Silva et al. 2010), suggesting that an increment on CRF induced by exercise training would augment MFO in endurance athletes, a hypothesis that needs to be supported by further studies.
Of note, all the above-mentioned studies evaluating the increment of MFO and VO2max induced by exercise training employed an intervention period ≤ 12 weeks. Further studies are needed to elucidate whether CRF and fat metabolism keep improving after 12 weeks of physical exercise. Otherwise, findings from previous randomized clinical trials suggest that MFO and VO2max increments depend of exercise training characteristics (i.e., intensity, volume). In young men with obesity, a large increment on MFO (∆: 0.08 g min−1; d = 1.49) and VO2max (∆: 2.8 mL kg−1 min−1; d = 0.82) was observed after 2 weeks of HIIT (8 exercise sessions speeded over 14 days; 10 × 60-s cycling intervals at workload eliciting ~ 90% HRmax interspersed with 60-s recovery at 50 W) while only a low increment on MFO (∆: 0.03 g min−1; d = 0.32) and VO2max (∆: 1.8 mL kg−1 min−1; d = 0.27) was observed after steady-state exercise training at FATmax (8 exercise sessions speeded over 14 days; 40–50 min day−1) (Lanzi et al. 2015). In addition, both MFO (∆16%, p < 0.05) and VO2max (∆14%, p < 0.05) increased significantly after 3 weeks of high intensity continuous training (5 days/week; 2 sessions day−1; 70% VO2max) in adolescents with obesity but remain unchanged in patients who trained at FATmax (5 days/week; 2 sessions day−1) (Lazzer et al. 2011). Thus, in the short-term, training at high intensity seems to be more effective at improving MFO in comparison to exercising at FATmax. On the other hand, high-volume endurance training (3 days/week; 600 kcal day−1 above 70% VO2peak) resulted on a larger increment on MFO in comparison to low-volume endurance training (3 days/week; 600 kcal day−1 above 70% VO2peak) in sedentary men with overweight (∆0.14 vs. 0.09 g min−1) (Rosenkilde et al. 2015). Moreover, in healthy men, the MFO and FATmax are higher during treadmill running in comparison to stationary cycling (Achten et al. 2003), elliptical and rowing exercises (Filipovic et al. 2021). Thus, the effect of exercise training on MFO may depend on exercise intensity, type and volume. Further clinical trials are need to stablish the optimal training characteristics for improving MFO in athletes, sedentary lean individuals and patients with chronic diseases.
Despite a clear relationship is observed between VO2max and MFO, the mechanisms behind such association are not fully understood. The VO2max represents the capacity of an organism for transport O2 from the environment to the body tissues for energy production in the mitochondrion through oxygen-dependent pathways, including fat oxidation. (Bassett and Howley 2000; Levine 2008). In this regard, the VO2max is determined by lungs capacity and volume, cardiovascular function, microcirculation, and skeletal muscle oxidative capacity (Wagner 1996; Levine 2008). Therefore, all the aforementioned factors might be implicated on the association between MFO and VO2max.
Biomarkers of skeletal muscle oxidative capacity associated with MFO
The VO2max is positively associated with several biomarkers of skeletal muscle oxidative capacity, including mitochondrial volume density (MitoVD) and oxidative phosphorylation capacity (OXPHOS) (Lundby and Jacobs 2016), capillary density (Hendrickse and Degens 2019) and type 1 muscle fibers abundance (Foster et al. 1978). Recent studies have evaluated the association of MFO with all the above-mentioned biomarkers providing valuable insights about the mechanism that regulate fat oxidation capacity.
Mitochondrial volume density and oxidative phosphorylation capacity
Dandanell et al. (2018) investigated the relationship of MitoVD and OXPHOS with MFO, observing a moderate correlation between these variables (r = 0.56 and r = 0.52 for MitoVD and OXPHOS respectively) when combining data from endurance trained and untrained men. In the same study, mitochondrial fatty acid oxidation measured in vitro turned to be positively related with MFO (r = 0.59) suggesting that exercise training improves skeletal muscle fat oxidation capacity by enhancing mitochondrial quantity and OXPHOS.
The enzymatic activity of citrate synthase (CS) and the protein content of the mitochondrial respiratory chain complexes are considered reliable biomarkers of MitoVD and OXPHOS in skeletal muscle (Larsen et al. 2012) and its relationship with MFO has been analyzed in combined cohorts of trained/untrained individuals (Nordby et al. 2006; Stisen et al. 2006; Dandanell et al. 2018; Shaw et al. 2020). These studies noted a higher CS activity in trained vs. untrained subjects (35–44% higher) but only Dandanell et al. (2018) found a strong and significant relationship between CS and MFO (r = 0.67, p < 0.01) which may be explained due to a larger difference on VO2max and CS activity among trained and untrained groups (see Table 1). In support of these data, the study by Maunder et al. (2021) observed that CS activity was more determinant than VO2max for predicting MFO in young trained men (see standardized beta coefficients reported in Table 1). Moreover, Shaw et al. (2020) found a significant relationship between MFO and mitochondrial respiratory chain complexes II, III, IV and V when combining the data from trained and untrained individuals (Table 1), supporting the hypothesis that increasing skeletal muscle oxidative capacity would lead to a higher MFO.
The augment of MFO was positively correlated with the increment of muscle CS activity (r = 0.63, p < 0.05) and OXPHOS (r = 0.78, p < 0.01) after 10 weeks of exercise training at FATmax in subjects with type 2 diabetes (Bordenave et al. 2008). Moreover, Rosenkilde et al. (2015) showed that changes in CS activity and mitochondrial complexes chain complexes II, III, IV, and V induced by 12 weeks of endurance exercise training were related with MFO augment in young sedentary overweight men. Up to date, there is no evidence of a concomitant increment on MitoVD and MFO in athletic population.
Skeletal muscle contraction promotes mitochondrial biogenesis through activation of the transcriptional coactivator peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC1-α) that recruits and co-regulates several transcription factors (i.e., nuclear respiratory factors 1 and 2, peroxisome proliferator-activated receptors, estrogen related receptor α) controlling the expression of mitochondrial proteins, including mitofusin 1 and 2 which regulate mitochondrial fusion and fission, respectively (Egan and Zierath 2013). In the same way, activation of PGC1-α upregulates the expression of several genes encoding CS and other proteins that regulate fatty acid trafficking and oxidation (see below) (Egan and Zierath 2013). Thus, future investigations should analyze the association between PGC1-α and MFO to elucidate molecular mechanisms implicated on metabolic health and sports performance. Interestingly, exercise intensity is positively related to exercise-induced increment of PGC1-α mRNA levels (r = 0.38) (Granata et al. 2018a) whilst training volume is directly related to MitoVD changes induced by physical exercise (Granata et al. 2018b). Therefore, future studies are needed to stablish training recommendations for optimizing skeletal muscle oxidative capacity and enhancing MFO.
In muscle fibers, the mitochondria are mainly distributed on intermyofibrillar cell compartment (Lundby and Jacobs 2016). Nonetheless, the relative increment of subsarcolemmal MitoVD is larger than in intermyofibrillar mitochondria after 6 weeks of high intensity endurance training (~ 72% VO2max) (Suter et al. 1995). This may optimize oxygen and fatty acid diffusion to skeletal muscle mitochondria improving fat oxidation capacity. Indeed, subsarcolemmal MitoVD showed a larger correlation with MFO (r = 0.62, p < 0.01) in comparison to intermyofibrillar MitoVD (r = 0.37, p < 0.01) (Dandanell et al. 2018). Whether an increment on subsarcolemmal MitoVD influences muscle oxygenation kinetics and fatty acid uptake elevating MFO remains to be elucidated.
In addition, endurance training also improves intrinsic mitochondrial function by enhancing the surface of the mitochondrial inner membrane that in turn is positively related to VO2max in both sedentary and trained individuals (Nielsen et al. 2017). The increment of mitochondrial cristae might lead to the assembly of electron transport chain supercomplexes enhancing mitochondrial respiratory capacity and ATP synthesis (Greggio et al. 2017). As before mentioned, a significant relationship between MFO and mitochondrial respiratory chain complexes II, III, IV and V was observed in lean individuals (Shaw et al. 2020). Nevertheless, whether an increment on electron transport chain supercomplexes could elevate MFO requires further investigation.
Exercise training improves MitoVD, mitochondrial respiration and insulin sensitivity in patients with obesity and type 2 diabetes, suggesting a link between skeletal muscle oxidative capacity and metabolic health (Genders et al. 2020). The mechanism behind such association is not fully understood but it might be possible that a higher fat oxidation induced by enhanced MitoVD and OXPHOS could attenuate the accumulation of bioactive lipids like diacylglycerols and ceramides which are related to insulin resistance (Perreault et al. 2018). In this regard, alongside with increased MFO and CS activity, Rosenkilde et al. (2015) also reported a significant reduction on fasting insulin levels (− 30%) after 12 weeks of endurance training in sedentary men with overweight. On the contrary, 10 weeks of exercise training at FATmax did not reduce insulin or glucose circulating levels in patients with diabetes despite a significant augment in MFO and CS activity (Bordenave et al. 2008). In the two aforementioned studies, changes of intramuscular lipids induced by exercise training were not measured. Therefore, future investigations are needed to elucidate whether an increment on MFO is associated with changes in skeletal muscle oxidative capacity, intramuscular lipid intermediates and insulin sensitivity.
In addition to increased MitoVD and OXPHOS, the abundance and activity of some glycolytic enzymes (e.g., lactate dehydrogenase) are reduced with exercise training attenuating muscle glycogenolysis which might delay glycogen depletion improving endurance performance (Holloszy and Coyle 1984; Egan and Zierath 2013; Knuiman et al. 2015; Hearris et al. 2018). Further studies should analyze the modifications in MFO and glycogen utilization induced by exercise training in athletes.
Capillary density
The MFO was positively correlated with muscle capillary density (r: 0.53–0.61) in young men (Dandanell et al. 2018; Shaw et al. 2020). Capillaries are blood vessels that deliver oxygen and nutrients to skeletal muscle fibers, being the number of capillaries per muscle fiber increased with endurance training throughout a process named angiogenesis (Egan et al. 2013; Hendrickse and Degens 2019). Up to date, whether an increment on capillary density induced by exercise training leads to a higher oxygen and fatty acid delivery to skeletal muscle elevating MFO remains undefined.
Fiber type distribution
Recent studies performed on healthy men, reported a positive correlation between MFO and %type I muscle fibers (r: 0.51–0.81) (Dandanell et al. 2018; Shaw et al. 2020). This relationship could be explained due to a higher capillary density, larger MitoVD and a higher activity of CS and mitochondrial respiratory chain complexes on type 1 muscle fibers in comparison to type 2 fibers (Egan and Zierath 2013). In addition, the abundance of transport proteins involved on fatty acid trafficking [i.e., fatty acid binding protein and fatty acid translocase cluster of differentiation 36 (CD36)] and the enzymatic activity of 3-hydroxyacyl-CoA dehydrogenase that regulates oxidation of fatty acids into the mitochondrion is also higher in type 1 muscle fibers (Vistisen et al. 2004; Egan and Zierath 2013).
To the best of our knowledge, the concomitant changes on %type I muscle fibers and MFO have not been analyzed neither in sedentary or trained individuals. Nevertheless, it is widely reported that skeletal muscle undergoes a remodeling process depending on exercise training characteristics. Several studies have shown that sprint, power and plyometric training could elicit a transition of type I muscle fibers to type IIa (Plotkin et al. 2021). Otherwise, endurance training promotes the shift of muscle fibers type IIa/IIx towards type I muscle fibers (Plotkin et al. 2021). The increment of type 1 muscle fibers might be of particular interest for long-distance runners in whom %type 1 muscle fibers is directly related to endurance performance (Foster et al. 1978). Moreover, patients with metabolic syndrome might benefit from increasing %type 1 muscle fibers because a diminished proportion of these muscle fibers is observed in this population when compared to lean subjects (Stuart et al. 2013; Albers et al. 2015). Further research is needed to elucidate whether an increment on MFO and the proportion of type 1 fibers improves insulin sensitivity and endurance performance in patients with diabetes and athletes respectively.
Cardiovascular function
A recent study evaluating the relationship between fat oxidation and muscle deoxygenation kinetics—assessed by the variations in deoxygenated hemo- and myoglobin concentrations—reported that the breakpoint and slope of the muscle deoxygenation kinetics correlated with MFO (r = 0.66, p < 0.05; r = − 0.41, < 0.05, respectively) in a combined group of physically active individuals and well-trained cyclist (Zurbuchen et al. 2020). Therefore, the greater the capacity for maintaining a balance between oxygen delivery and extraction throughout a larger range of exercise intensities, the greater the reliance on aerobic metabolism and fat oxidation for ATP production.
The cardiovascular system is responsible for oxygen transport from the lungs to the different bodily tissues (Wagner 1996; Hoppeler and Weibel 2000; Levine 2008), thereby, cardiovascular function might be associated with exercise fat oxidation. In this regard, Skattebo et al. (2022) reported a higher MFO relative to muscle mass during one-leg cycling in comparison with two-leg cycling (+ 54%) being such differences associated with an elevated mass-specific oxygen delivery and a higher increment on cardiac output in response to one-leg cycling. These data suggest that enhancing oxygen delivery to skeletal muscle by increasing cardiac output may elevate MFO.
An increment of cardiac output occurs in response to exercise training due to a larger stroke volume, derived from an increment of left ventricle chamber dimension and also an increment in end-diastolic filling pressure (Hoppeler and Weibel 2000; Levine 2008). Recently, Vaccari et al. (2020) reported a concomitant increment of cardiac output, stroke volume, VO2max and fat oxidation rates at 60–80% VO2max after 3 months of HIIT in patients with obesity (34 exercise sessions; 3-min sprint intervals at ~ 100% VO2peak interspersed by 90 s of walking at ~ 50% VO2peak). Nonetheless, in the same study, MFO did not increase in response to exercise training. Noteworthy, despite a large increment on cardiac output was reported by the previous study, authors did not evaluate modifications of muscle oxygenation kinetics. Therefore, further studies are needed to investigate the association among MFO, oxygen delivery to skeletal muscle and biomarkers of cardiovascular function (Fig. 1).
Pulmonary function
Ventilatory threshold
A moderate association of the first and second ventilatory thresholds (VT) with MFO has been reported by several studies in trained men (R2: 0.46–0.55) (Amaro-Gahete et al. 2019a, b; Zurbuchen et al. 2020; Maunder et al. 2021). The VT are positively related with muscle oxygenation kinetics (Zurbuchen et al. 2020) and performance in long-distance runners. Moreover, the VT increase with exercise training in sedentary men and women, with a higher improvement when exercise training is performed above the VT intensity (Gaskill et al. 2001).
The second VT indicates an increment on pulmonary ventilation that results from accumulation of lactate in the blood and skeletal muscle (Binder et al. 2008). The accumulation of lactate in skeletal muscle sarcoplasm induces a reduction of muscle pH that decrease the activity of carnitine palmitoyl transferase 1 (CPT1), thus reducing the entry of long-chain fatty acids into the mitochondrial matrix (Starritt et al. 2000; Achten and Jeukendrup 2004). Indeed, blood lactate levels are inversely associated with fat oxidation rates during a graded exercise test (San-Millán and Brooks 2018). Exercise training improves lactate clearance in skeletal muscle fibers by increasing the density of monocarboxylate transporters (MCT1 and MCT4) in the sarcolemma (Thomas et al. 2012). This adaptation delays the reduction of sarcoplasmic pH and the inhibition of CPT1 allowing a higher fat oxidation. San-Millán and Brooks (2018) reported that lactate threshold and MFO occurred at a higher workload in endurance trained athletes in comparison with patients that suffer from metabolic syndrome. Nevertheless, whether a parallel increment on lactate threshold, VT and MFO in obtained after exercise training remains to be elucidated.
Lung capacities and volumes
Pulmonary function is a critical determinant of pulmonary ventilation, oxygen uptake and VO2max (Wagner 1996). Several biomarkers of lung volumes (e.g., tidal volume) are positively related to physical activity and seem to be increased with endurance training (Lutfi 2017). Moreover, Durmic et al. (2017) suggest that lungs capacities also increase with exercise training because vital capacity and forced expiratory volume were higher in endurance trained individuals vs. sedentary controls. The adaptations of lungs capacities might be related to exercise intensity, type and volume because vital capacity and maximal expiratory volume are notably higher in water polo athletes when compared against basketball, handball and soccer players (Durmic et al. 2015). Although the mechanism behind the increment of lung volumes and capacities are not fully understood, Durmic et al. (2017) proposed that endurance exercise may change airways resistance conduction, alveolar expansion and lung elasticity. In addition, exercise training increases the strength of respiratory muscles contributing to a higher pulmonary ventilation (Hackett 2020). Further studies need to evaluate whether lung capacities and volumes correlate with muscle oxygenation kinetics and MFO.
Fatty acid metabolism
The contribution of fatty acid delivered from adipose tissue and intramuscular triglycerides (IMTG) to energy expenditure is determined by exercise intensity, being the plasma free fatty acids (FFA) the main energy source during low to moderate exercise intensity while IMTG increases its contribution as workload progressively augment during a graded exercise test (Hargreaves and Spriet 2020). The FATmax is commonly observed between 45 and 65% VO2max (Purdom et al. 2018) which represent a moderate exercise intensity (Mann et al. 2013). Nevertheless, because the FATmax and the aerobic threshold occur at a similar intensity in both sedentary (Peric and Nikolovski 2020) and trained individuals (Nikolovski et al. 2021), MFO is located at a low exercise intensity (MacIntosh et al. 2021). Thus, FFA would be the main fuel used for ATP production and its concentration might be associated with MFO.
Adipose tissue lipolysis
In this sense, Robinson et al. (2016) reported a low correlation between FFA concentration at FATmax and MFO in trained men (r = 0.27, p < 0.05). Such correlation disappeared when plasma FFA at rest was included as a covariate. Indeed, the FFA increment from rest to FATmax was not correlated with the differences between fat oxidation at rest and MFO. To the best of our knowledge, only this study has analyzed the association between FFA concentration at FATmax and MFO, therefore, further research is necessary to stablish a robust conclusion. Interestingly, sedentary men with obesity exhibited higher FFA availability at FATmax and higher absolute MFO during an incremental-load exercise in comparison to lean subjects (Lanzi et al. 2014) which has been related with a larger fat mass in patients with obesity (Amaro-Gahete et al. 2019b). Moreover, women with low abdominal to lower body fat mass ratio exhibited a higher MFO and FATmax in comparison to women with high abdominal to lower body fat mass ratio despite no differences in FFM and total fat mass (Isacco et al. 2014). The last finding could be explained by lower insulin levels and higher FFA concentration during moderate intensity exercise in women with high abdominal to lower body fat mass ratio (Isacco et al. 2013). Thereby, the relationship between FFA and MFO could be influenced by nutritional status and fat mass distribution, a hypothesis that also require further research.
The data from Robinson et al. (2016) suggest that fatty acid availability prior exercise seems to be more determinant than lipolytic response to this stimulus. In this sense, Frandsen et al. (2017) showed that overnight fasting (9–13 h) plasma FFA at rest was independently associated with MFO explaining 6% of its variation in male ironman athletes, although such association was not observed in female ironman athletes (R2 = 0.07, ns) in whom VO2peak was the only biomarker associated with MFO (Vest et al. 2018). The discrepancy across these studies suggests that MFO is determined by different physiological mechanisms across male and female ironman athletes which require further analysis. On the other hand, Frandsen et al. (2021) showed that increasing FFA throughout prolonged fasting (> 22 h) and repeated exercise sessions resulted on a higher MFO in endurance athletes. In the same study, a linear regression analysis showed that an increase of 500 μmol L in plasma FFA would augment MFO by 4.5 mg kg lean body mass−1 min−1 in men and by 5.5 mg kg lean body mass−1 min−1 in women (R2 = 0.70, p < 0.01), highlighting the association between FFA availability and MFO. Future investigations are needed to corroborate whether a higher FFA availability led to higher fatty acid uptake and oxidation in skeletal muscle.
Triacylglycerol hydrolysis (lipolysis) is a sequential process involving (1) several enzymes called lipases and (2) different regulatory proteins located in the surface of lipid droplets named perilipins. The enzymes triacylglycerol lipase (ATGL) and hormone sensitive lipase (HSL) catalyze the hydrolysis of the first and second ester bonds producing diacylglycerol and monoacylglycerol, respectively, while perilipin 1 facilitates the access of lipases into the lipid droplet (Tsiloulis and Watt 2015). Both, HSL and perilipin phosphorylation increases in response to β-adrenergic stimulation which augment during physical exercise (Jordy and Kiens 2014; Tsiloulis and Watt 2015). A pilot study in healthy individuals showed that MFO was positively related with HSL (r = 0.38, p < 0.05) and perilipin 1 (r = 0.71, p < 0.01) abundance in adipose tissue (Chrzanowski-Smith et al. 2021). The higher expression of these proteins may elevate FFA availability inducing a higher MFO. Nevertheless, this study did not measure the activity or phosphorylation status of these proteins. Moreover, in the same study, ex vivo adipose tissue lipolysis rates and MFO were not associated (r = − 0.38, p > 0.05). Several studies have informed an increment on adipose tissue HSL, ATGL and perilipin abundance after endurance training in rodents (Tsiloulis and Watt 2015). Moreover, aerobic exercise training seems to improve beta-adrenergic induced lipolysis in the sub-cutaneous adipose tissue of patients with obesity by decreasing the anti-lipolytic activity of alpha-2 adrenergic receptors (Laurens et al. 2020). Nonetheless, several studies report that FFA concentration at rest and during exercise does not increase with exercise training (Horowitz 2003; Tsiloulis and Watt 2015). Indeed, MFO increment after exercise training at FATmax (Bordenave et al. 2008), moderate intensity exercise (Rosenkilde et al. 2015) and high intensity interval training (Lanzi et al. 2015) occurred without a concomitant augment of circulating FFA at rest. Hence, despite increasing FFA availability is associated with an increment on MFO (Frandsen et al. 2021) more research is guaranteed to identify novel strategies that promote adipose tissue lipolysis in patients with obesity and athletes, to reduce body fat and increase the reliance on fatty acids for ATP production.
Intramuscular triglycerides
As above mentioned, MFO is located at a low exercise intensity when IMTG shows a modest contribution to energy expenditure. Nevertheless, skeletal muscle HSL (r = 0.75, p < 0.01), ATGL (r: 0.54–0.76) and perilipin 5 (r = 0.67, p < 0.01) content were positively related to MFO in healthy individuals (Shaw et al. 2020; Chrzanowski-Smith et al. 2021), suggesting that elevating IMTG breakdown would increase MFO. Of note, intramuscular lipids content was not related to MFO in patients with obesity (Haufe et al. 2010) or trained subjects (Dandanell et al. 2018). Hence, the relevance of IMTG utilization on MFO remains to be elucidated.
Previous studies, reported that perilipin 2 and 5 expression is upregulated by resistance exercise and endurance training in sedentary men, resulting on increased IMTG hydrolysis during physical exercise (Shaw et al. 2012; Shepherd et al. 2013, 2014). In addition, lipid droplets proximity to mitochondria in skeletal muscle increases with exercise training due to mobilization of lipid droplets from subsarcolemal region to intramyofibrillar cell compartment as well as elevated MitoVD and OXPHOS in both athletes and patients with obesity (Gemmink et al. 2020). These changes led to increased IMTG utilization during exercise which is related to improvements on insulin sensitivity in patients with obesity (Sheperd et al. 2014; Gemmink et al. 2020) and exercise performance on athletes (Hearris et al. 2018). Therefore, future studies are needed to investigate whether a simultaneous increase on IMTG breakdown and oxidation is associated to MFO.
Fatty acid trafficking and oxidation in skeletal muscle
The abundance of different proteins regulating fatty acid trafficking [i.e., carnitine palmitoyltransferase 1 (CPT-1), fatty acid binding protein and fatty acid translocase cluster of differentiation 36 (CD36)] and oxidation (3-hydroxyacyl-CoA dehydrogenase) in skeletal muscle has been also associated with MFO variations in different cohorts of trained/untrained individuals (Stisen et al. 2006; Shaw et al. 2020), trained men (Maunder et al. 2021) and physically active men and women (Chrzanowski-Smith et al. 2021). From the aforementioned proteins, only CD36 has been validated as MFO predictor explaining 11% of MFO variation in trained men (Maunder et al. 2021). The CD36 mediates long-chain fatty acids transports across the sarcolemma and mitochondrial double membrane where it colocalizes with CPT1 (Smith et al. 2012). Thus, long-chain fatty acids mobilization across sarcolemma and mitochondria seems to be an important determinant of MFO, a finding that need to be corroborated in other populations. A previous study in untrained women, reported an increment on both skeletal muscle mitochondria CD36 content (+ 51%) and fat oxidation (+ 68%) during moderate intensity exercise (65% VO2peak) after 6 weeks of high intensity interval training (3 days/week; 4-min cycling bouts at 90% VO2peak) (Talanian et al. 2010). In the same way, colocalization of CD36 with CPT-1 in the mitochondria increased by 25% after an endurance training intervention (3 days/week; 35–45 min day−1 at 70–85% HRmax) in women with obesity which turned to be strongly associated with the increment of fat oxidation rate at rest (R2 = 0.85, p < 0.01) (Schenk and Horowitz 2006). Likewise, expression levels of CD36 and CPT1 in skeletal muscle increased after 12 weeks of endurance training (5 days/week; 60 min day−1 at 85%HRmax) in elderly adults (Mulya et al. 2017). In the last study, the increment of muscle CPT1 was positively correlated with a resting fat oxidation augment (r = 0.45, p = 0.05). The aforementioned evidence suggest that exercise training could enhance MFO by promoting fatty acid uptake across the sarcolemma and mitochondrial membranes. Nevertheless, future investigation is needed to corroborate such hypothesis. Otherwise, the CD36 also mediates fatty acid release from adipose tissue (Pepino et al. 2014). It would be interesting that future studies investigate whether CD36 abundance in adipose tissue and skeletal muscle is associated with FFA rate of appearance/disappearance affecting MFO.
The fat oxidation rate at rest is positively correlated with MFO in trained men (r = 0.47, p < 0.01) (Robinson et al. 2016) and is downregulated by high glucose and insulin concentrations (Melzer 2011). Insulin suppresses adipose tissue lipolysis by stimulating the activity of cellular phosphodiesterase-3 (Horowitz 2003) and reduces skeletal muscle long-chain fatty acids oxidation and long-chain acylcarnitine concentration showing a decrement on the functional activity of CPT1 (Rasmussen et al. 2002; Sidossis et al. 1996). A previous study by Achten and Jeukendrup (2003b) reported a decline on MFO (~ 28%) when 75 g of glucose was consumed 45 min prior exercise testing in moderately trained individuals. This evidence suggests that circulating glucose, insulin and lactate—a metabolite representing skeletal muscle glycolytic flux—may be associated with MFO. In this regard, Amaro-Gahete et al. (2021) did not found any relationship between MFO, plasma glucose and insulin concentration in sedentary young and middle-aged adults (Amaro-Gahete et al. 2021). Furthermore, plasma glucose and lactate were not associated with MFO in trained men (Robinson et al. 2016). On the contrary, plasma lactate levels at rest were negatively associated with MFO (R2 = 0.12, p < 0.01) in male ironman athletes (Frandsen et al. 2017), although similar lactate concentrations were noted in comparison to the participants from the study of Robinson et al. (2016) (0.8 ± 0.3 vs. 0.8 ± 0.2 mmol L−1, respectively). Thus, the influence of glycolytic flux at rest and MFO remains controversial and future investigations including individuals with obesity and type II diabetes mellitus who exhibit higher circulating levels of lactate, glucose and insulin will help to elucidate the aforementioned mechanism.
Endocrine function
Physical exercise induces lipolysis throughout the action of several hormones (i.e., adrenaline, atrial natriuretic peptide, cortisol, glucagon and growth hormone) that regulate adipose tissue and skeletal muscle HSL and ATGL activity (Muscella et al. 2020). Nonetheless, whether the activity, circulating concentration of these hormones and the level of expression of their respective cellular receptors are associated with MFO remain unclear. Furthermore, previous studies have demonstrated that thyroid hormones regulate fatty acid oxidation in the skeletal muscle through p43 thyroid receptor alpha isoform which increases AMP-activated protein kinase phosphorylation and mitochondrial associated protein activity (enzymes that regulate CD36 translocation to sarcolemma and mitochondrial fatty acid oxidation) (Sayre and Lechleiter 2012). Thus, future studies should determine whether there is a direct association between thyroid hormones and MFO (Fig. 1).
On the other hand, female ovarian hormones (i.e., estradiol and progesterone) have been associated with higher MFO in women vs. men (Venables et al. 2005; Purdom et al. 2018; Maunder et al. 2018). In particular, estrogens could promote fatty acid oxidation through binding the estrogen receptor alpha in the sarcoplasm that dimerizes and subsequently is translocated to the nucleus promoting the transcription of Peroxisome proliferator-activated receptor gamma coactivator 1-alpha, Nuclear Respiratory Factor and additional genes involved in mitochondrial biogenesis and long-chain fatty acids oxidation (Ventura-Clapier et al. 2019). Nonetheless, circulating estradiol concentration did not exhibit a correlation with MFO neither in recreationally active or ironman female athletes (Vest et al. 2018; Frandsen et al. 2020). Moreover, skeletal muscle estradiol receptor alpha, CPT1, HSL and ATGL content were not different between physically active men and women in spite the higher MFO reported in the female participants’ cohort (Chrzanowski-Smith et al. 2021). Whereby, a higher skeletal muscle lipolysis and oxidative capacity induced by female sexual hormones seems not to be the physiological mechanism explaining MFO differences between sexes and further mechanisms should be explored. Interestingly, a recent study by Ponce González et al. (2017) reported a positive relationship between free testosterone levels and MFO in young men (r = 0.45, p < 0.05), which might be explained by the anabolic effect of testosterone that favor a higher muscle mass and a subsequent upregulation of genes involved in mitochondrial biogenesis and fatty acid metabolism via androgen receptor activity (Usui et al. 2014; Kelly and Jones 2015). Therefore, current evidence indicates that male but not female sexual hormones are related to MFO.
Genetic polymorphisms
As before discussed, association of different biomarkers with MFO are inconsistent among studies investigating participants with a similar physical fitness, with most of these biomarkers explaining less than 40% of MFO variation (Table 1). This evidence points out that genetics may play an important role on determining an organism capacity for increasing fat oxidation in response to physical exercise. Indeed, recent studies have reported a significant association of ACE, ADRB3, AR and CD36 genotype with MFO (Table 2) providing valuable evidence that enhance the comprehension of the molecular pathways regulating exercise metabolism.
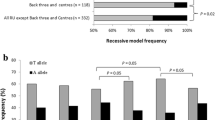
The ACE gene encodes the angiotensin-converting enzyme (ACE) which converts angiotensin I to angiotensin II increasing the vasoconstriction activity of this hormone that raise total peripheral resistance and blood pressure (Vasudeva et al. 2020). An intronic variant consisting of the deletion (D) of a 216 bp segment in intron 16 of the ACE gene has been associated with higher circulating levels of angiotensin II (Rigat et al. 1990), elevated blood pressure (Ma et al. 2018) and reduced CRF (Bueno et al. 2016). Thereby, the DD genotype is considered an independent cardiovascular risk factor (Yuan et al. 2017). A recent study by Montes-de-Oca-Garcia et al. (2021) reported that MFO was 29% higher in female carriers of the DD genotype in comparison to carriers of the reference allele (II). Interestingly, the opposite was found in male participants were MFO was superior in male carriers of the DD genotype (15% higher), demonstrating a sex–genotype interaction regarding MFO whose explanation require further analysis. The DD genotype has been associated with higher circulating levels of the angiotensin II hormone (Rigat et al. 1990) which stimulates vasoconstriction and may reduce fatty acid and oxygen uptake by skeletal muscle. In fact, male carriers of the DD genotype exhibit a reduced capillary density on skeletal muscle (Valdivieso et al. 2017) which may explain a low MFO. However, further studies evaluating the association of circulating ACE concentration with FFA rate of appearance/disappearance, skeletal muscle deoxygenation kinetics and MFO are needed for elucidating the mechanisms behind the association of ACE genotype with MFO.
On the other hand, a missense mutation in the ADRB3 gene—resulting on the interchange of a tryptophan (W) for an arginine (R) in the position 64 of the Beta-3 adrenergic receptor (β-AR3)—was associated with a lower energy expenditure at FATmax in healthy adolescents (~ 14% lower), being considered a consequence of lower fat oxidation rates (Correa de Jesus et al. 2018). The β-AR3 is a G-coupled protein located on adipocytes plasma membrane that regulate adipose tissue lipolysis by triggering HSL activation after binding of adrenaline (Tsiloulis and Watt 2015; Schena and Caplan 2019). The W > R substitution is located on a cytoplasmic topological domain that may negatively affect the receptor sensitivity reducing lipolysis and FFA availability during physical exercise which has been directly associated with MFO. Nonetheless, a previous study by Gómez-Gómez et al. (2014) did not observe a lower lipolytic rate in male carriers of the R allele during a steady-state exercise session at ~ 62% VO2max. Thus, evidence of a lower FFA availability and MFO in carriers of the W64R polymorphism is needed. Moreover, as both W64R polymorphism and MFO are associated with body mass index and obesity (Amaro-Gahete et al. 2019a, b; Schena and Caplan 2019; Chávez-Guevara et al. 2021) analyze the interaction of β-AR3 and MFO in this population would be especially relevant.
The AR gene encodes the androgen receptor protein (AR) that function as a steroid-hormone activated transcription factor that could upregulate lipolysis and fat oxidation in skeletal muscle (Kelly and Jones 2015). This gene contains 2 polymorphic trinucleotide repeat segments that encode polyglutamine (CAG) and polyglycine (GGN) tracts in the N-terminal transactivation domain of its protein that may affect AR sensitivity. Previous studies reported that MFO was ~ 35% higher in male carriers of the CAGL and GGNL genotypes in comparison with carriers of the CAGS and GGNS genotypes (see genotype classification described in Table 2) (Ponce-González et al. 2016; Ponce González et al. 2017). These results are interesting but controversial since the GAGL genotype was associated with a lower AR sensitivity (Chamberlain et al. 1994) that may lead to a reduced fat oxidation. Indeed, a recent study reported that AR inhibition attenuated skeletal muscle CPT1 and exercise fat oxidation increment on mice after 4 weeks of treadmill running (Kim et al. 2019). Therefore, it seems plausible that if a lower AR activity is associated with GAGL and GGNL genotypes, carriers of these genotypes should exhibit a lower MFO.
Interestingly, a single nucleotide polymorphism (T > C) in the upstream promoter region of the CD36 gene (intron 1B, − 3489 bp relative to the translation start site), was associated with higher levels of MFO in healthy individuals (Jayerwardene et al. 2014). This genetic variant has been also associated with a lower prevalence of type 2 diabetes in patients with obesity (Corpeleijn et al. 2006), supporting the association between MFO and insulin sensitivity (Robinson et al. 2016). Indeed, the T > C polymorphism may affect the transcription of CD36 gene (Corpeleijn et al. 2006). Because the CD36 abundance in skeletal muscle has been positively associated with MFO (Maunder et al. 2021), future studies performing skeletal muscle biopsies are required to determinate whether CT/CC genotypes exhibit a higher content of FAT/CD36 on skeletal muscle, and whether these hypothetical greater values are associated to elevated MFO. Moreover, the study by Jayewardene et al. (2014) showed a poor statistical power (n = 22; n ≤ 9 subjects per group) and they have to combine data from men and women together, matching participants by CRF. Thus, future investigations with a large statistical power and an appropriate control of those biological determinant of MFO are necessary to corroborate whether the CD36 genotypes partially explain MFO variance.
As noted, only a few number of studies have analyzed the association of genetic polymorphism with MFO, focusing on healthy subjects with low to moderate physical activity. Future studies investigating the interplay between the above-mentioned polymorphism, MFO and body fat reduction induced by exercise training in patients with obesity are needed. Besides, different polymorphism on the CD36 (rs2232169), SLC6A14 (rs2011162) and PCSK1 (rs6235) genes have been associated with a reduced fat oxidation at rest in European adults with obesity (Corpeleijn et al. 2010). Consequently, these may also be associated with MFO.
Conclusions and future directions
In conclusion, there are several biomarkers, health-related components of physical fitness and genetic polymorphism associated with MFO (Fig. 1). Up to date, only VO2max/peak has been validated as MFO predictor in athletes and sedentary individuals while plasma FFA, circulating lactate concentrations and the protein content of CS and CD36 in skeletal muscle show a modest association with MFO in trained subjects. Although numerous manuscripts have been recently published about the present topic, there is still a lot of “gaps” regarding the physiological mechanism that regulate exercise-induced fat oxidation. Noteworthy, the majority of the here discussed studies focuses on evaluating the relationship of novel biomarkers with MFO rather than analyzing their contribution to prediction models reported for athletes (Randell et al. 2017) and healthy individuals (Venables et al. 2005; Fletcher et al. 2017). Mainly, this occurs due to a low statistical power, the independent evaluation of men and women and the lack of physical activity level and dietary macronutrient content assessments. Besides, most of the studies focus on healthy young adults with a scarce information regarding elderly adults and people with chronic diseases. Nonetheless, this work set the basis for future large-scale metabolomics and genomics studies that will contribute to the progress of exercise metabolism field. Indeed, further research about the association of MFO with different transcription factors (e.g., Peroxisome proliferator-activated receptor alpha, Peroxisome proliferator-activated receptor gamma coactivator 1-alpha, Nuclear respiratory factor) regulating mitochondrial biogenesis and fatty acid metabolism (Egan and Zierath 2013) will provide a further understanding about the molecular mechanisms influencing metabolic health and athletic performance. Moreover, investigating different microRNAs related to CPT1 (i.e., miR-1) (Rodrigues et al. 2021), CD36 (i.e., miR-145, miR-20a-5p, miR-29a) (Ding et al. 2019; Lin et al. 2019; Wang et al. 2020) and ACE (i.e., miR-143) (Vasudeva et al. 2019) might help to identify epigenetic mechanisms controlling MFO. Recent studies reported that physical exercise could regulate the expression of the above-mentioned microRNAs (Fernández-Sanjurjo et al. 2018; Silva et al. 2020); therefore, these might be implicated on metabolic adaptations induced by exercise training.
Abbreviations
- ACE:
-
Angiotensin-converting enzyme
- AR:
-
Androgen receptor
- ATGL:
-
Adipose triacylglycerol lipase
- β-AR3 :
-
Beta-3 adrenergic receptor
- CD36:
-
Fatty acid translocase cluster of differentiation 36
- CPT1:
-
Carnitine palmitoyltransferase 1
- CRF:
-
Cardiorespiratory fitness
- CS:
-
Citrate synthase
- FATmax:
-
Exercise intensity corresponding to maximal fat oxidation
- FFA:
-
Free fatty acids
- FFM:
-
Fat-free mass
- HIIT:
-
High-intensity interval training
- HSL:
-
Hormone-sensitive lipase
- IMTG:
-
Intramuscular triglycerides
- MFO:
-
Maximal fat oxidation
- MitoVD :
-
Mitochondrial volume density
- OXPHOS:
-
Mitochondrial oxidative phosphorylation capacity
- VO2max :
-
Maximal oxygen uptake
- VO2peak :
-
Peak oxygen uptake
- VT:
-
Ventilatory threshold
References
Achten J, Jeukendrup AE (2003a) Maximal fat oxidation during exercise in trained men. Int J Sports Med 24(8):603–608. https://doi.org/10.1055/s-2003-43265
Achten J, Jeukendrup AE (2003b) The effect of pre-exercise carbohydrate feedings on the intensity that elicits maximal fat oxidation. J Sports Sci 21(12):1017–1024. https://doi.org/10.1080/02640410310001641403
Achten J, Jeukendrup AE (2004) Relation between plasma lactate concentration and fat oxidation rates over a wide range of exercise intensities. Int J Sports Med 25(1):32–37. https://doi.org/10.1055/s-2003-45231
Achten J, Venables MC, Jeukendrup AE (2003) Fat oxidation rates are higher during running compared with cycling over a wide range of intensities. Metabolism 52(6):747–752. https://doi.org/10.1016/s0026-0495(03)00068-4
Ahmetov II, Vinogradova OL, Williams AG (2012) Gene polymorphisms and fiber-type composition of human skeletal muscle. Int J Sport Nutr Exerc Metab 22(4):292–303. https://doi.org/10.1123/ijsnem.22.4.292
Albers PH, Pedersen AJ, Birk JB, Kristensen DE, Vind BF, Baba O, Nøhr J, Højlund K, Wojtaszewski JF (2015) Human muscle fiber type-specific insulin signaling: impact of obesity and type 2 diabetes. Diabetes 64(2):485–497. https://doi.org/10.2337/db14-0590 (Epub 2014 Sep 3, PMID: 25187364)
Amaro-Gahete FJ, Sanchez-Delgado G, Ruiz JR (2018) Commentary: Contextualising maximal fat oxidation during exercise: determinants and normative values. Front Physiol 9:1460. https://doi.org/10.3389/fphys.2018.01460
Amaro-Gahete FJ, Jurado-Fasoli L, Triviño AR, Sanchez-Delgado G, De-la-O A, Helge JW, Ruiz JR (2019a) Diurnal variation of maximal fat-oxidation rate in trained male athletes. Int J Sports Physiol Perform 14(8):1140–1146. https://doi.org/10.1123/ijspp.2018-0854
Amaro-Gahete FJ, Sanchez-Delgado G, Ara I, Ruiz R (2019b) Cardiorespiratory fitness may influence metabolic inflexibility during exercise in obese persons. J Clin Endocrinol Metab 104(12):5780–5790. https://doi.org/10.1210/jc.2019-01225
Amaro-Gahete FJ, De-la-O A, Jurado-Fasoli L, Sanchez-Delgado G, Ruiz JR, Castillo MJ (2020) Metabolic rate in sedentary adults, following different exercise training interventions: the FIT-AGEING randomized controlled trial. Clin Nutr 39(11):3230–3240. https://doi.org/10.1016/j.clnu.2020.02.001
Amaro-Gahete FJ, Sanchez-Delgado G, Jurado-Fasoli L, Ruiz JR (2021) Uncertain association between maximal fat oxidation during exercise and cardiometabolic risk factors in healthy sedentary adults. Eur J Sports Exerc Sci. https://doi.org/10.1080/17461391.2021.1895894 (advance online publication)
Arad AD, Basile AJ, Albu J, DiMenna FJ (2020) No influence of overweight/obesity on exercise lipid oxidation: a systematic review. Int J Mol Sci 21(5):1614. https://doi.org/10.3390/ijms21051614
Bassett DR, Howley ET (2000) Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exerc 32(1):70–84. https://doi.org/10.1097/00005768-200001000-00012
Binder RK, Wonisch M, Corra U, Cohen-Solal A, Vanhees L, Saner H, Schmid JP (2008) Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur J Cardiovasc Prev Rehabil 15(6):726–734. https://doi.org/10.1097/HJR.0b013e328304fed4
Bordenave S, Metz L, Flavier S, Lambert K, Ghanassia E, Dupuy AM, Michel F, Puech-Cathala AM, Raynaud E, Brun JF, Mercier J (2008) Training-induced improvement in lipid oxidation in type 2 diabetes mellitus is related to alterations in muscle mitochondrial activity. Effect of endurance training in type 2 diabetes. Diabetes Metab 34(2):162–168. https://doi.org/10.1016/j.diabet.2007.11.006
Bueno S, Pasqua LA, de Araújo G, Eduardo Lima-Silva A, Bertuzzi R (2016) The association of ACE genotypes on cardiorespiratory variables related to physical fitness in healthy men. PLoS ONE 11(11):e0165310. https://doi.org/10.1371/journal.pone.0165310
Cano A, Ventura L, Martinez G, Cugusi L, Caria M, Deriu F, Manca A (2021) Analysis of sex-based differences in energy substrate utilization during moderate-intensity aerobic exercise. Eur J Appl Physiol. https://doi.org/10.1007/s00421-021-04802-5 (advance online publication)
Chamberlain NL, Driver ED, Miesfeld RL (1994) The length and location of CAG trinucleotide repeats in the androgen receptor N-terminal domain affect transactivation function. Nucleic Acids Res 22(15):3181–3186. https://doi.org/10.1093/nar/22.15.3181
Chávez-Guevara IA, Urquidez-Romero R, Pérez-León JA, González-Rodríguez E, Moreno-Brito V, Ramos-Jiménez A (2020) Chronic effect of Fatmax training on body weight, fat mass, and cardiorespiratory fitness in obese subjects: a meta-analysis of randomized clinical trials. Int J Environ Res Public Health 17(21):7888. https://doi.org/10.3390/ijerph17217888
Chávez-Guevara IA, Hernández-Torres RP, Trejo-Trejo M, González-Rodríguez E, Moreno-Brito V, Wall-Medrano A, Pérez-León JA, Ramos-Jiménez A (2021) Exercise fat oxidation is positively associated with body fatness in men with obesity: defying the metabolic flexibility paradigm. Int J Environ Res Public Health 18(13):6945. https://doi.org/10.3390/ijerph18136945
Chrzanowski-Smith OJ, Edinburgh RM, Smith E, Thomas MP, Walhin JP, Koumanov F, Williams S, Betts JA, Gonzalez JT (2021) Resting skeletal muscle PNPLA2 (ATGL) and CPT1B are associated with peak fat oxidation rates in men and women but do not explain observed sex differences. Exp Physiol 106(5):1208–1223. https://doi.org/10.1113/EP089431
Corpeleijn E, van der Kallen CJ, Kruijshoop M, Magagnin MG, de Bruin TW, Feskens EJ, Saris WH, Blaak EE (2006) Direct association of a promoter polymorphism in the CD36/FAT fatty acid transporter gene with Type 2 diabetes mellitus and insulin resistance. Diabet Med 23(8):907–911. https://doi.org/10.1111/j.1464-5491.2006.01888.x
Corpeleijn E, Petersen L, Holst C, Saris WH, Astrup A, Langin D, MacDonald I, Martinez JA, Oppert JM, Polak J, Pedersen O, Froguel P, Arner P, Sørensen TI, Blaak EE (2010) Obesity-related polymorphisms and their associations with the ability to regulate fat oxidation in obese Europeans: the NUGENOB study. Obesity (silver Spring) 18(7):1369–1377. https://doi.org/10.1038/oby.2009.377
Dandanell S, Meinild-Lundby AK, Andersen AB, Lang PF, Oberholzer L, Keiser S, Robach P, Larsen S, Rønnestad BR, Lundby C (2018) Determinants of maximal whole-body fat oxidation in elite cross-country skiers: role of skeletal muscle mitochondria. Scand J Med Sci Sports 28(12):2494–2504. https://doi.org/10.1111/sms.13298
Ding D, Ye G, Lin Y, Lu Y, Zhang H, Zhang X, Hong Z, Huang Q, Chi Y, Chen J, Dong S (2019) MicroRNA-26a-CD36 signaling pathway: Pivotal role in lipid accumulation in hepatocytes induced by PM2.5 liposoluble extracts. Environmental Pollut 248:269–278. https://doi.org/10.1016/j.envpol.2019.01.112
Drapier E, Cherif A, Richou M et al (2018) Long term (3 years) weight loss after low intensity endurance training targeted at the level of maximal muscular lipid oxidation. Integr Obes Diabetes. https://doi.org/10.15761/iod.1000201
Durmic T, Lazovic B, Djelic M, Lazic JS, Zikic D, Zugic V, Dekleva M, Mazic S (2015) Sport-specific influences on respiratory patterns in elite athletes. J Bras Pneumol 41(6):516–522. https://doi.org/10.1590/S1806-37562015000000050
Durmic T, Lazovic Popovic B, Zlatkovic Svenda M, Djelic M, Zugic V, Gavrilovic T, Mihailovic Z, Zdravkovic M, Leischik R (2017) The training type influence on male elite athletes’ ventilatory function. BMJ Open Sport Exerc Med 3(1):e000240. https://doi.org/10.1136/bmjsem-2017-000240
Egan B, Zierath JR (2013) Exercise metabolism and the molecular regulation of skeletal muscle adaptation. Cell Metab 17(2):162–184. https://doi.org/10.1016/j.cmet.2012.12.012
Fernández-Sanjurjo M, de Gonzalo-Calvo D, Fernández-García B, Díez-Robles S, Martínez-Canal Á, Olmedillas H, Dávalos A, Iglesias-Gutiérrez E (2018) Circulating microRNA as emerging biomarkers of exercise. Exerc Sport Sci Rev 46(3):160–171. https://doi.org/10.1249/JES.0000000000000148
Filipovic M, Munten S, Herzig KH, Gagnon DD (2021) Maximal fat oxidation: comparison between treadmill, elliptical and rowing exercises. J Sport Sci Med 20(1):170–178. https://doi.org/10.52082/jssm.2021.170
Fletcher G, Eves FF, Glover EI, Robinson SL, Vernooij CA, Thompson JL, Wallis GA (2017) Dietary intake is independently associated with the maximal capacity for fat oxidation during exercise. Am J Clin Nutr 105(4):864–872. https://doi.org/10.3945/ajcn.116.133520
Foster C, Costill DL, Daniels JT, Fink WJ (1978) Skeletal muscle enzyme activity, fiber composition and VO2 max in relation to distance running performance. Eur J Appl Physiol Occup Physiol 39(2):73–80. https://doi.org/10.1007/BF00421711
Frandsen J, Vest SD, Larsen S, Dela F, Helge JW (2017) Maximal fat oxidation is related to performance in an ironman triathlon. Int J Sports Med 38(13):975–982. https://doi.org/10.1055/s-0043-117178
Frandsen J, Pistoljevic N, Quesada JP, Amaro-Gahete FJ, Ritz C, Larsen S, Dela F, Helge JW (2020) Menstrual cycle phase does not affect whole body peak fat oxidation rate during a graded exercise test. J Appl Physiol 128(3):681–687. https://doi.org/10.1152/japplphysiol.00774.2019
Frandsen J, Poggi AI, Ritz C, Larsen S, Dela F, Helge JW (2021) Peak fat oxidation rate is closely associated with plasma free fatty acid concentrations in women. Similar to Men Front Physiol 12:696261. https://doi.org/10.3389/fphys.2021.696261
Gaskill SE, Walker AJ, Serfass RA, Bouchard C, Gagnon J, Rao DC, Skinner JS, Wilmore JH, Leon AS (2001) Changes in ventilatory threshold with exercise training in a sedentary population: the HERITAGE Family Study. Int J Sports Med 22(8):586–592. https://doi.org/10.1055/s-2001-18522
Gemmink A, Schrauwen P, Hesselink M (2020) Exercising your fat (metabolism) into shape: a muscle-centred view. Diabetologia 63(8):1453–1463. https://doi.org/10.1007/s00125-020-05170-z
Genders AJ, Holloway GP, Bishop DJ (2020) Are alterations in skeletal muscle mitochondria a cause or consequence of insulin resistance? Int J Mol Sci 21(18):6948. https://doi.org/10.3390/ijms21186948
Gómez-Gómez E, Ríos-Martínez ME, Castro-Rodríguez EM, Del-Toro-Equíhua M, Ramírez-Flores M, Delgado-Enciso I, Pérez-Huitimea AL, Baltazar-Rodríguez LM, Velasco-Pineda G, Muñiz-Murguía J (2014) Carnitine palmitoyltransferase 1B 531K allele carriers sustain a higher respiratory quotient after aerobic exercise, but β3-adrenoceptor 64R allele does not affect lipolysis: a human model. PloS one 9(6):e96791. https://doi.org/10.1371/journal.pone.0096791
Goodpaster BH, Sparks LM (2017) Metabolic flexibility in health and disease. Cell Metab 25(5):1027–1036. https://doi.org/10.1016/j.cmet.2017.04.015
Granata C, Jamnick NA, Bishop DJ (2018a) Principles of exercise prescription, and how they influence exercise-induced changes of transcription factors and other regulators of mitochondrial biogenesis. Sports Med 48(7):1541–1559. https://doi.org/10.1007/s40279-018-0894-4
Granata C, Jamnick NA, Bishop DJ (2018b) Training-induced changes in mitochondrial content and respiratory function in human skeletal muscle. Sports Med 48(8):1809–1828. https://doi.org/10.1007/s40279-018-0936-y
Greggio C, Jha P, Kulkarni SS, Lagarrigue S, Broskey NT, Boutant M, Wang X, Conde Alonso S, Ofori E, Auwerx J, Cantó C, Amati F (2017) Enhanced respiratory chain supercomplex formation in response to exercise in human skeletal muscle. Cell Metab 25(2):301–311
Hackett DA (2020) Lung function and respiratory muscle adaptations of endurance- and strength-trained males. Sports 8(12):160. https://doi.org/10.3390/sports8120160
Hargreaves M, Spriet LL (2020) Skeletal muscle energy metabolism during exercise. Nat Metab 2(9):817–828. https://doi.org/10.1038/s42255-020-0251-4
Haufe S, Engeli S, Budziarek P, Utz W, Schulz-Menger J, Hermsdorf M, Wiesner S, Otto C, Fuhrmann JC, Luft FC, Boschmann M, Jordan J (2010) Determinants of exercise-induced fat oxidation in obese women and men. Horm Metab Res 42(3):215–221. https://doi.org/10.1055/s-0029-1242745
Hearris MA, Hammond KM, Fell JM, Morton JP (2018) Regulation of muscle glycogen metabolism during exercise: implications for endurance performance and training adaptations. Nutrients 10(3):298. https://doi.org/10.3390/nu10030298
Hendrickse P, Degens H (2019) The role of the microcirculation in muscle function and plasticity. J Muscle Res Cell Motil 40(2):127–140. https://doi.org/10.1007/s10974-019-09520-2
Holloszy JO, Coyle EF (1984) Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J Appl Physiol Respir Environ Exerc Physiol 56(4):831–838. https://doi.org/10.1152/jappl.1984.56.4.831
Hoppeler H, Weibel ER (2000) Structural and functional limits for oxygen supply to muscle. Acta Physiol Scand 168(4):445–456. https://doi.org/10.1046/j.1365-201x.2000.00696.x
Horowitz JF (2003) Fatty acid mobilization from adipose tissue during exercise. TEM 14(8):386–392. https://doi.org/10.1016/s1043-2760(03)00143-7
Isacco L, Duche P, Thivel D, Meddahi-Pelle A, Lemoine-Morel S, Duclos M, Boisseau N (2013) Fat mass localization alters fuel oxidation during exercise in normal weight women. Med Sci Sports Exerc 45(10):1887–1896. https://doi.org/10.1249/MSS.0b013e3182935fe3
Isacco L, Thivel D, Duclos M, Aucouturier J, Boisseau N (2014) Effects of adipose tissue distribution on maximum lipid oxidation rate during exercise in normal-weight women. Diabetes Metab 40(3):215–219. https://doi.org/10.1016/j.diabet.2014.02.006
Jayewardene AF, Gwinn T, Hancock DP, Mavros Y, Rooney KB (2014) The associations between polymorphisms in the CD36 gene, fat oxidation and cardiovascular disease risk factors in a young adult Australian population: a pilot study. Obes Res Clin Pract 8(6):e618–e621. https://doi.org/10.1016/j.orcp.2014.09.001
Jesus ÍC, Alle LF, Munhoz EC, Silva L, Lopes WA, Tureck LV, Purim K, Titski A, Leite N (2018) Trp64Arg polymorphism of the ADRB3 gene associated with maximal fat oxidation and LDL-C levels in non-obese adolescents. J Pediatr (ri J) 94(4):425–431. https://doi.org/10.1016/j.jped.2017.07.010
Jeukendrup A, Achten J (2001) Fatmax: a new concept to optimize fat oxidation during exercise? Eur J Sport Sci 1(5):1–5. https://doi.org/10.1080/17461390100071507
Jordy AB, Kiens B (2014) Regulation of exercise-induced lipid metabolism in skeletal muscle. Exp Physiol 99(12):1586–1592. https://doi.org/10.1113/expphysiol.2014.082404
Kelly DM, Jones TH (2015) Testosterone and obesity. Obes Rev 16(7):581–606. https://doi.org/10.1111/obr.12282
Kim J, Park J, Kim N, Park HY, Lim K (2019) Inhibition of androgen receptor can decrease fat metabolism by decreasing carnitine palmitoyltransferase I levels in skeletal muscles of trained mice. Nutr Metab 16:82. https://doi.org/10.1186/s12986-019-0406-z
Knuiman P, Hopman MT, Mensink M (2015) Glycogen availability and skeletal muscle adaptations with endurance and resistance exercise. Nutr Metab 12:59. https://doi.org/10.1186/s12986-015-0055-9
Lanzi S, Codecasa F, Cornacchia M, Maestrini S, Salvadori A, Brunani A, Malatesta D (2014) Fat oxidation, hormonal and plasma metabolite kinetics during a submaximal incremental test in lean and obese adults. PLoS ONE 9(2):e88707. https://doi.org/10.1371/journal.pone.0088707
Lanzi S, Codecasa F, Cornacchia M, Maestrini S, Capodaglio P, Brunani A, Fanari P, Salvadori A, Malatesta D (2015) Short-term HIIT and Fat max training increase aerobic and metabolic fitness in men with class II and III obesity. Obesity (silver Spring) 23(10):1987–1994. https://doi.org/10.1002/oby.21206
Larsen S, Nielsen J, Hansen CN, Nielsen LB, Wibrand F, Stride N, Schroder HD, Boushel R, Helge JW, Dela F, Hey-Mogensen M (2012) Biomarkers of mitochondrial content in skeletal muscle of healthy young human subjects. J Physiol 590(14):3349–3360. https://doi.org/10.1113/jphysiol.2012.230185
Laurens C, de Glisezinski I, Larrouy D, Harant I, Moro C (2020) Influence of acute and chronic exercise on abdominal fat lipolysis: an update. Front Physiol 11:575363. https://doi.org/10.3389/fphys.2020.575363
Lazzer S, Lafortuna C, Busti C, Galli R, Agosti F, Sartorio A (2011) Effects of low- and high-intensity exercise training on body composition and substrate metabolism in obese adolescents. J Endocrinol Invest 34(1):45–52. https://doi.org/10.1007/BF03346694
Levine BD (2008) VO2max: what do we know, and what do we still need to know?. J Physiol 586(1):25–34. https://doi.org/10.1113/jphysiol.2007.147629
Li SW, Wang J, Yang Y, Liu ZJ, Cheng L, Liu HY, Ma P, Luo W, Liu SM (2016) Polymorphisms in FADS1 and FADS2 alter plasma fatty acids and desaturase levels in type 2 diabetic patients with coronary artery disease. J Transl Med 14:79. https://doi.org/10.1186/s12967-016-0834-8
Lima-Silva AE, Bertuzzi RC, Pires FO, Gagliardi JF, Barros RV, Hammond J, Kiss MA (2010) Relationship between training status and maximal fat oxidation rate. J Sports Sci Med 9(1):31–35
Lin HY, Wang FS, Yang YL, Huang YH (2019) MicroRNA-29a suppresses CD36 to ameliorate high fat diet-induced steatohepatitis and liver fibrosis in mice. Cells 8(10):1298. https://doi.org/10.3390/cells8101298
Lundby C, Jacobs RA (2016) Adaptations of skeletal muscle mitochondria to exercise training. Exp Physiol 101(1):17–22. https://doi.org/10.1113/EP085319
Lutfi MF (2017) The physiological basis and clinical significance of lung volume measurements. Multidiscip Respir Med 12:3. https://doi.org/10.1186/s40248-017-0084-5
Ma Y, Tong X, Liu Y, Liu S, Xiong H, Fan H (2018) ACE gene polymorphism is associated with COPD and COPD with pulmonary hypertension: a meta-analysis. Int J Chron Obstruct Pulmon Dis 13:2435–2446. https://doi.org/10.2147/COPD.S168772
MacIntosh BR, Murias JM, Keir DA, Weir JM (2021) What is moderate to vigorous exercise intensity? Front Physiol 12:682233. https://doi.org/10.3389/fphys.2021.682233
Mann T, Lamberts RP, Lambert MI (2013) Methods of prescribing relative exercise intensity: physiological and practical considerations. Sports Med 43(7):613–625. https://doi.org/10.1007/s40279-013-0045-x
Martinez-Navarro I, Montoya-Vieco A, Collado E, Hernando B, Hernando C (2020) Ultra trail performance is differently predicted by endurance variables in men and women. Int J Sports Med. https://doi.org/10.1055/a-1255-3083(advance online publication)
Maunder E, Plews DJ, Kilding AE (2018) Contextualising maximal fat oxidation during exercise: determinants and normative values. Front Physiol 9:599. https://doi.org/10.3389/fphys.2018.00599
Maunder E, Plews DJ, Wallis GA, Brick MJ, Leigh WB, Chang WL, Stewart T, Watkins CM, Kilding AE (2021) Peak fat oxidation is positively associated with vastus lateralis CD36 content, fed-state exercise fat oxidation, and endurance performance in trained males. Eur J Appl Physiol. https://doi.org/10.1007/s00421-021-04820-3 (advance online publication)
Melzer K (2011) Carbohydrate and fat utilization during rest and physical activity. E Spen Eur E J Clin Nutr Metab 6(2):e45–e52. https://doi.org/10.1016/j.eclnm.2011.01.005
Montes-de-Oca-García A, Perez-Bey A, Velázquez-Díaz D, Corral-Pérez J, Opazo-Díaz E, Rebollo-Ramos M, Gómez-Gallego F, Cuenca-García M, Casals C, Ponce-González JG (2021) Influence of ACE gene I/D polymorphism on cardiometabolic risk, maximal fat oxidation, cardiorespiratory fitness, diet and physical activity in young adults. Int J Environ Res Public Health 18(7):3443. https://doi.org/10.3390/ijerph18073443
Morita E, Taniguchi H, Sakaue M (2009) Trp64Arg polymorphism in beta3-adrenergic receptor gene is associated with decreased fat oxidation both in resting and aerobic exercise in the Japanese male. Exp Diabetes Res 2009:605139. https://doi.org/10.1155/2009/605139
Mulya A, Haus JM, Solomon TP, Kelly KR, Malin SK, Rocco M, Barkoukis H, Kirwan JP (2017) Exercise training-induced improvement in skeletal muscle PGC-1α-mediated fat metabolism is independent of dietary glycemic index. Obesity (silver Spring) 25(4):721–729. https://doi.org/10.1002/oby.21799
Muscella A, Stefàno E, Lunetti P, Capobianco L, Marsigliante S (2020) The regulation of fat metabolism during aerobic exercise. Biomolecules 10(12):1699. https://doi.org/10.3390/biom10121699
Nielsen J, Gejl KD, Hey-Mogensen M, Holmberg HC, Suetta C, Krustrup P, Elemans C, Ørtenblad N (2017) Plasticity in mitochondrial cristae density allows metabolic capacity modulation in human skeletal muscle. J Physiol 595(9):2839–2847. https://doi.org/10.1113/JP273040
Nikolovski Z, Barbaresi S, Cable T, Peric R (2021) Evaluating the influence of differences in methodological approach on metabolic thresholds and fat oxidation points relationship. Eur J Sport Sci 21(1):61–68. https://doi.org/10.1080/17461391.2020.1717640
Nordby P, Saltin B, Helge JW (2006) Whole-body fat oxidation determined by graded exercise and indirect calorimetry: a role for muscle oxidative capacity? Scand J Med Sci Sports 16(3):209–214. https://doi.org/10.1111/j.1600-0838.2005.00480.x
Ørtenblad N, Nielsen J (2015) Muscle glycogen and cell function—location, location, location. Scand J Med Sci Sports 25(Suppl 4):34–40. https://doi.org/10.1111/sms.12599
Pepino MY, Kuda O, Samovski D, Abumrad NA (2014) Structure-function of CD36 and importance of fatty acid signal transduction in fat metabolism. Annu Rev Nut 34:281–303. https://doi.org/10.1146/annurev-nutr-071812-161220
Peric R, Nikolovski Z (2020) Can metabolic thresholds be used as exercise intensity markers in adult men with obesity—fat burn points used as an exercise marker. Comp Exerc Physiol 16(2):113–119. https://doi.org/10.3920/cep190035
Perreault L, Newsom SA, Strauss A, Kerege A, Kahn DE, Harrison KA, Snell-Bergeon JK, Nemkov T, D’Alessandro A, Jackman MR, MacLean PS, Bergman BC (2018) Intracellular localization of diacylglycerols and sphingolipids influences insulin sensitivity and mitochondrial function in human skeletal muscle. JCI Insight 3(3):e96805. https://doi.org/10.1172/jci.insight.96805
Plotkin DL, Roberts MD, Haun CT, Schoenfeld BJ (2021) Muscle fiber type transitions with exercise training: shifting perspectives. Sports 9(9):127. https://doi.org/10.3390/sports9090127
Ponce González JG, Guadalupe-Grau A, Rodríguez-González FG, Torres-Peralta R, Morales-Alamo D, Rodríguez-García L, Díaz-Chico BN, López Calbet JA, Dorado C (2017) Androgen receptor gene polymorphisms and maximal fat oxidation in healthy men. A longitudinal study. Polimorfismo del gen del receptor de andrógenos y oxidación máxima de grasa en hombres sanos/. Estudio longitudinal. Nutr Hosp 34(5):1089–1098. https://doi.org/10.2096/nh.885
Ponce-González JG, Rodríguez-Garcia L, Losa-Reyna J, Guadalupe-Grau A, Rodriguez-Gonzalez FG, Díaz-Chico BN, Dorado C, Serrano-Sanchez JA, Calbet JA (2016) Androgen receptor gene polymorphism influence fat accumulation: a longitudinal study from adolescence to adult age. Scand J Med Sci Sports 26(11):1313–1320. https://doi.org/10.1111/sms.12587
Purdom T, Kravitz L, Dokladny K, Mermier C (2018) Understanding the factors that effect maximal fat oxidation. J Int Soc Sports Nutr 15:3. https://doi.org/10.1186/s12970-018-0207-1
Randell RK, Rollo I, Roberts TJ, Dalrymple KJ, Jeukendrup AE, Carter JM (2017) Maximal fat oxidation rates in an athletic population. Med Sci Sports Exerc 49(1):133–140. https://doi.org/10.1249/MSS.0000000000001084
Rasmussen BB, Holmbäck UC, Volpi E, Morio-Liondore B, Paddon-Jones D, Wolfe RR (2002) Malonyl coenzyme A and the regulation of functional carnitine palmitoyltransferase-1 activity and fat oxidation in human skeletal muscle. J Clin Investig 110(11):1687–1693. https://doi.org/10.1172/JCI15715
Rigat B, Hubert C, Alhenc-Gelas F, Cambien F, Corvol P, Soubrier F (1990) An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Investig 86(4):1343–1346. https://doi.org/10.1172/JCI114844
Robinson SL, Hattersley J, Frost GS, Chambers ES, Wallis GA (2015) Maximal fat oxidation during exercise is positively associated with 24-hour fat oxidation and insulin sensitivity in young, healthy men. J Appl Physiol (1985) 118(11):1415–1422. https://doi.org/10.1152/japplphysiol.00058.2015
Robinson SL, Chambers ES, Fletcher G, Wallis GA (2016) Lipolytic markers, insulin and resting fat oxidation are associated with maximal fat oxidation. Int J Sports Med 37(8):607–613. https://doi.org/10.1055/s-0042-100291
Rodrigues AC, Spagnol AR, Frias FT, de Mendonça M, Araújo HN, Guimarães D, Silva WJ, Bolin AP, Murata GM, Silveira L (2021) Intramuscular injection of miR-1 reduces insulin resistance in obese mice. Front Physiol 12:676265. https://doi.org/10.3389/fphys.2021.676265
Rosenkilde M, Reichkendler MH, Auerbach P, Bonne TC, Sjödin A, Ploug T, Stallknecht BM (2015) Changes in peak fat oxidation in response to different doses of endurance training. Scand J Med Sci Sports 25(1):41–52. https://doi.org/10.1111/sms.12151
San-Millán I, Brooks GA (2018) Assessment of metabolic flexibility by means of measuring blood lactate, fat, and carbohydrate oxidation responses to exercise in professional endurance athletes and less-fit individuals. Sports Med 48(2):467–479. https://doi.org/10.1007/s40279-017-0751-x
Sayre NL, Lechleiter JD (2012) Fatty acid metabolism and thyroid hormones. Curr Trends Endocrinol 6:65–76
Schena G, Caplan MJ (2019) Everything you always wanted to know about β3-AR * (* but were afraid to ask). Cells 8(4):357. https://doi.org/10.3390/cells8040357
Schenk S, Horowitz JF (2006) Coimmunoprecipitation of FAT/CD36 and CPT I in skeletal muscle increases proportionally with fat oxidation after endurance exercise training. Am J Physiol Endocrinol Metab 291(2):E254–E260. https://doi.org/10.1152/ajpendo.00051.2006
Shaw CS, Shepherd SO, Wagenmakers AJ, Hansen D, Dendale P, van Loon LJ (2012) Prolonged exercise training increases intramuscular lipid content and perilipin 2 expression in type I muscle fibers of patients with type 2 diabetes. Am J Physiol Endocrinol Metab 303(9):E1158–E1165. https://doi.org/10.1152/ajpendo.00272.2012
Shaw CS, Swinton C, Morales-Scholz MG, McRae N, Erftemeyer T, Aldous A, Murphy RM, Howlett KF (2020) Impact of exercise training status on the fiber type-specific abundance of proteins regulating intramuscular lipid metabolism. J Appl Physiol (1985) 128(2):379–389. https://doi.org/10.1152/japplphysiol.00797.2019
Shepherd SO, Cocks M, Tipton KD, Ranasinghe AM, Barker TA, Burniston JG, Wagenmakers AJ, Shaw CS (2013) Sprint interval and traditional endurance training increase net intramuscular triglyceride breakdown and expression of perilipin 2 and 5. J Physiol 591(3):657–675. https://doi.org/10.1113/jphysiol.2012.240952
Shepherd SO, Cocks M, Tipton KD, Witard OC, Ranasinghe AM, Barker TA, Wagenmakers AJ, Shaw CS (2014) Resistance training increases skeletal muscle oxidative capacity and net intramuscular triglyceride breakdown in type I and II fibres of sedentary males. Exp Physiol 99(6):894–908. https://doi.org/10.1113/expphysiol.2014.078014
Sidossis LS, Stuart CA, Shulman GI, Lopaschuk GD, Wolfe RR (1996) Glucose plus insulin regulate fat oxidation by controlling the rate of fatty acid entry into the mitochondria. J Clin Investig 98(10):2244–2250. https://doi.org/10.1172/JCI119034
Silva F, Iop R, Andrade A, Costa VP, Gutierres Filho P, Silva RD (2020) Effects of physical exercise on the expression of microRNAs: a systematic review. J Strength Cond Res 34(1):270–280
Skattebo Ø, Peci D, Clauss M, Johansen EI, Jensen J (2022) Increased mass-specific maximal fat oxidation rate with small versus large muscle mass exercise. Med Sci Sports Exerc. https://doi.org/10.1249/MSS.0000000000002864
Smith BK, Bonen A, Holloway GP (2012) A dual mechanism of action for skeletal muscle FAT/CD36 during exercise. Exerc Sport Sci Rev 40(4):211–217. https://doi.org/10.1097/JES.0b013e31825eb263
Starritt EC, Howlett RA, Heigenhauser GJ, Spriet LL (2000) Sensitivity of CPT I to malonyl-CoA in trained and untrained human skeletal muscle. Am J Physiol Endocrinol Metab 278(3):E462–E468. https://doi.org/10.1152/ajpendo.2000.278.3.E462
Stisen AB, Stougaard O, Langfort J, Helge JW, Sahlin K, Madsen K (2006) Maximal fat oxidation rates in endurance trained and untrained women. Eur J Appl Physiol 98(5):497–506. https://doi.org/10.1007/s00421-006-0290-x
Suter E, Hoppeler H, Claassen H, Billeter R, Aebi U, Horber F, Jaeger P, Marti B (1995) Ultrastructural modification of human skeletal muscle tissue with 6-month moderate-intensity exercise training. Int J Sports Med 16(3):160–166. https://doi.org/10.1055/s-2007-972985
Talanian JL, Holloway GP, Snook LA, Heigenhauser GJ, Bonen A, Spriet LL (2010) Exercise training increases sarcolemmal and mitochondrial fatty acid transport proteins in human skeletal muscle. Am J Physiol Endocrinol Metab 299(2):E180–E188. https://doi.org/10.1152/ajpendo.00073.2010
Thomas C, Bishop DJ, Lambert K, Mercier J, Brooks GA (2012) Effects of acute and chronic exercise on sarcolemmal MCT1 and MCT4 contents in human skeletal muscles: current status. Am J Physiol Regul Integr Comp Physiol 302(1):R1–R14. https://doi.org/10.1152/ajpregu.00250.2011
Tsiloulis T, Watt MJ (2015) Exercise and the regulation of adipose tissue metabolism. Prog Mol Biol Transl Sci 135:175–201. https://doi.org/10.1016/bs.pmbts.2015.06.016
Usui T, Kajita K, Kajita T, Mori I, Hanamoto T, Ikeda T, Okada H, Taguchi K, Kitada Y, Morita H, Sasaki T, Kitamura T, Sato T, Kojima I, Ishizuka T (2014) Elevated mitochondrial biogenesis in skeletal muscle is associated with testosterone-induced body weight loss in male mice. FEBS Lett 588(10):1935–1941. https://doi.org/10.1016/j.febslet.2014.03.051
Vaccari F, Passaro A, D’Amuri A, Sanz JM, Di Vece F, Capatti E, Magnesa B, Comelli M, Mavelli I, Grassi B, Fiori F, Bravo G, Avancini A, Parpinel M, Lazzer S (2020) Effects of 3-month high-intensity interval training vs. moderate endurance training and 4-month follow-up on fat metabolism, cardiorespiratory function and mitochondrial respiration in obese adults. Eur J Appl Physiol 120(8):1787–1803. https://doi.org/10.1007/s00421-020-04409-2
Valdivieso P, Vaughan D, Laczko E, Brogioli M, Waldron S, Rittweger J, Flück M (2017) The metabolic response of skeletal muscle to endurance exercise is modified by the ACE-I/D gene polymorphism and training state. Front Physiol 8:993. https://doi.org/10.3389/fphys.2017.00993
Vasudeva K, Balyan R, Munshi A (2020) ACE-triggered hypertension incites stroke: genetic, molecular, and therapeutic aspects. Neuromolecular Med 22(2):194–209. https://doi.org/10.1007/s12017-019-08583-1
Venables MC, Achten J, Jeukendrup AE (2005) Determinants of fat oxidation during exercise in healthy men and women: a cross-sectional study. J Appl Physiol 98(1):160–167. https://doi.org/10.1152/japplphysiol.00662.2003
Ventura-Clapier R, Piquereau J, Veksler V, Garnier A (2019) Estrogens, estrogen receptors effects on cardiac and skeletal muscle mitochondria. Front Endocrinol 10:557. https://doi.org/10.3389/fendo.2019.00557
Vest SD, Frandsen J, Larsen S, Dela F, Helge JW (2018) Peak fat oxidation is not independently related to ironman performance in women. Int J Sports Med 39(12):916–923. https://doi.org/10.1055/a-0660-0031
Vistisen B, Roepstorff K, Roepstorff C, Bonen A, van Deurs B, Kiens B (2004) Sarcolemmal FAT/CD36 in human skeletal muscle colocalizes with caveolin-3 and is more abundant in type 1 than in type 2 fibers. J Lipid Res 45(4):603–609. https://doi.org/10.1194/jlr.M300424-JLR200
Wagner PD (1996) Determinants of maximal oxygen transport and utilization. Annu Rev Physiol 58:21–50. https://doi.org/10.1146/annurev.ph.58.030196.000321
Wang X, Ma Y, Yang LY, Zhao D (2020) MicroRNA-20a-5p ameliorates non-alcoholic fatty liver disease via inhibiting the expression of CD36. Front Cell Dev Biol 8:596329. https://doi.org/10.3389/fcell.2020.596329
Yuan Y, Meng L, Zhou Y, Lu N (2017) Genetic polymorphism of angiotensin-converting enzyme and hypertrophic cardiomyopathy risk: a systematic review and meta-analysis. Medicine 96(48):e8639. https://doi.org/10.1097/MD.0000000000008639
Zurbuchen A, Lanzi S, Voirol L, Trindade CB, Gojanovic B, Kayser B, Bourdillon N, Chenevière X, Malatesta D (2020) Fat oxidation kinetics is related to muscle deoxygenation kinetics during exercise. Front Physiol 11:571. https://doi.org/10.3389/fphys.2020.00571
Acknowledgements
The authors would like to thank Dr. Ed Maunder and Dr. Jacob Frandsen who kindly provided supplementary data regarding some of their studies and gave their consent for publication in this review. IACG was supported by a Ph.D scholarship (859438) from the Consejo Nacional de Ciencia y Tecnología (CONACyT). However, the institution did not participate in the manuscript preparation.
Author information
Authors and Affiliations
Contributions
IACG and FJAM conceived the main idea for the review. RPHT, ARJ and EGR participated in data extraction, analysis and interpretation. The first draft of the manuscript was written by IACG. All authors commented on previous versions of the manuscript, read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Additional information
Communicated by Michael Lindinger.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chávez-Guevara, I.A., Hernández-Torres, R.P., González-Rodríguez, E. et al. Biomarkers and genetic polymorphisms associated with maximal fat oxidation during physical exercise: implications for metabolic health and sports performance. Eur J Appl Physiol 122, 1773–1795 (2022). https://doi.org/10.1007/s00421-022-04936-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-022-04936-0