
Abstract
Purpose
Altered movement complexity, indicative of system dysfunction, has been demonstrated with increased running velocity and neuromuscular fatigue. The critical velocity (CV) denotes a metabolic and neuromuscular fatigue threshold. It remains unclear whether changes to complexity during running are coupled with the exercise intensity domain in which it is performed. The purpose of this study was to examine whether movement variability and complexity differ exclusively above the CV intensity during running.
Methods
Ten endurance-trained participants ran at 95%, 100%, 105% and 115% CV for 20 min or to task failure, whichever occurred first. Movement at the hip, knee, and ankle were sampled throughout using 3D motion analysis. Complexity of kinematics in the first and last 30 s were quantified using sample entropy (SampEn) and detrended fluctuation analysis (DFA-α). Variability was determined using standard deviation (SD).
Results
SampEn decreased during all trials in knee flexion/extension and it increased in hip internal/external rotation, whilst DFA-α increased in knee internal/external rotation. SD of ankle plantar/dorsiflexion and inversion/eversion, knee internal/external rotation, and hip flexion/extension and abduction/adduction increased during trials. Hip flexion/extension SampEn values were lowest below CV. DFA-α was lower at higher velocities compared to velocities below CV in ankle plantar/dorsiflexion, hip flexion/extension, hip adduction/abduction, hip internal/external rotation. In hip flexion/extension SD was highest at 115% CV.
Conclusions
Changes to kinematic complexity over time are consistent between heavy and severe intensity domains. The findings suggest running above CV results in increased movement complexity and variability, particularly at the hip, during treadmill running.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Running is comprised of a series of repeated and rhythmic actions. The cyclic nature of running suggests that motion is regular, with low variability (Jordan et al. 2006). Previous studies examining the variability of movement during running have traditionally used linear measures such as standard deviation, coefficient of variation, and root mean square (Belli et al. 1995; Cher et al. 2017). Haken et al. (1985) proposed that increased variability in movement during locomotion is indicative of a loss of stability and diminished ability to respond to external perturbations. Linear measures merely quantify the magnitude of variability, whereas non-linear measures quantify dynamic and temporal aspects of time series and provide greater insight into the complexity of underlying motor control (Stergiou and Decker 2011). Complexity is considered to be temporal regularity or randomness of a time-series (Pincus et al. 1994) and can be quantified using measures of entropy and fractal scaling. For example, sample entropy (SampEn) quantifies the regularity of fluctuations in a time (Pincus 1991; Richman and Moorman 2000), and long-range correlations and statistical persistence can be quantified using fractal measures such as detrended fluctuation analysis exponent-α (DFA-α; Hausdorff et al. 1995).
Healthy and unfatigued systems are typically characterised by complex outputs which allow for adaptability to external perturbations, but a loss of complexity is evident in ageing or diseased states (Lipsitz and Goldberger 1992). Within the context of gait fractal dynamics, it has been shown that healthy young adults exhibit statistical persistence in stride intervals (Hausdorff et al. 1997, 1998). Conversely, stride interval time series from healthy older individuals and individuals with Huntingdon’s (Hausdorff et al. 1997) or Parkinson’s disease (Hausdorff et al. 1998) demonstrate anti-persistence. Further to changes in gait dynamics caused by ageing and disease, fatigue has been shown to alter temporal dynamics (Meardon et al. 2011; Schütte et al. 2015, 2018). During running tasks performed to task failure at 5 km race pace on a track, runners exhibited decreased DFA-α of stride time in the last lap compared to the first (Meardon et al. 2011). These findings were replicated by Schütte et al. (2018), demonstrating decreased DFA-α of stride time alongside increased complexity of stride length in the last lap compared to the first. Running-induced fatigue has also been shown to increase step complexity and complexity of trunk accelerations (Schütte et al. 2015). Importantly, both studies (Schütte et al. 2015, 2018) quantified fatigue using rating of perceived exertion scales, without reference to objective markers of fatigue.
In addition to fatigue, running velocity has been shown to affect complexity and variability of movement (Jordan et al. 2006; McGregor et al. 2009; Murray et al. 2017). A quasi U-shape in standard deviation and DFA-α was apparent with deviations from the preferred running velocity (Jordan et al. 2006; Mann et al. 2015). McGregor et al. (2009) further demonstrated decreased control entropy of accelerometry concomitant with increasing velocity during an incremental running test to exhaustion. When considering angular kinematics, Estep et al. (2018) recently demonstrated greater complexity of hip and knee movement during running when compared to walking. Importantly, Murray et al. (2017) showed SampEn and root mean square of shank and waist accelerations were positively correlated with blood [La] during a submaximal incremental test. Given the link between complexity and physiological responses such as increased blood [La] (Murray et al. 2017), and such responses are determined by physiological thresholds (Poole et al. 2016), changes in complexity during running may be defined by physiological thresholds. To date, the link between physiological boundaries and the complexity of movement during whole-body movement has not been investigated; it, therefore, remains unclear which mechanisms mediate complexity during locomotion.
Previous work has shown the fatigue-mediated decrease in complexity of torque outputs exclusively above critical torque (Pethick et al. 2016). The critical torque is analogous to critical velocity (CV) and demarks the boundary between the heavy and severe exercise-intensity domains (Poole et al. 2016). Exercise above CV is characterised by an inexorable increase in metabolic flux (e.g. inorganic phosphate, H+ ions, phosphocreatine) and systemic (e.g. pulmonary oxygen uptake) responses to exercise, whereas exercise below CV allows for the attainment of a steady state (Jones et al. 2007; Poole et al. 2016). Pethick et al. (2019) have recently demonstrated that muscle torque complexity depends, in part, on metabolic rate, with greater intensities invoking lower complexity. However, this phenomenon may not be evident during whole-body exercise, with greater movement complexity exhibited at greater intensities (Jordan et al. 2006; Mann et al. 2015; Murray et al. 2017). At present, no studies have examined changes to complexity of movement during whole-body exercise relative to physiological thresholds.
A recent review has eloquently highlighted the potential implementation of non-linear methods, including complexity, to forecast injury risk (Fonseca et al. 2020). However, without fundamental understanding and exploration of movement complexity during locomotion, the successful implementation of such methods in applied settings may be problematic and limited. The aim of this study, therefore, was to explore the variability and complexity of lower limb angular kinematics above and below CV. An additional aim was to examine whether there would be different temporal profiles of angular kinematic complexity and variability above and below the CV. Since changes to motor control have been shown to be dependent on metabolic rate, and previous literature demonstrating greater complexity at increased velocities, it was hypothesised that compared to trials below CV decreased complexity would only be evident above CV. It was expected that greater decreases in complexity over time would be evident in trials above CV when compared to trials below CV.
Methods
Participants
Ten recreationally trained males (age 29.3 ± 10.1 years; stature 1.76 ± 0.04 m; body mass 72.1 ± 9.6 kg; means ± SD) volunteered to participate in this study after giving written informed consent. The study was approved by the Health, Science, Engineering and Technology Ethics Committee of the University of Hertfordshire (protocol number: LMS/PGR/UH/03454) and adhered to the Declaration of Helsinki. All participants were male runners or multisport athletes, e.g. triathletes, familiar with treadmill running, aged between 18 and 50 years, with a \(\dot{V}{\text{O}}_{{2\max }}\) ≥ 45 ml min−1 kg−1. The level of the participants corresponded to performance level 2 in the classification of participants groups in sport science research (De Pauw et al. 2013). Exclusion criteria included vestibular or vision disorders, an observed \(\dot{V}{\text{O}}_{{2\max }}\) < 45 ml min−1 kg−1, pulmonary, neurological, or cardiovascular diseases, and current or recent (6 months prior to participation) musculoskeletal injuries to the lower extremity or back. Assessment of the exclusion criteria, with the exception of \(\dot{V}{\text{O}}_{{2\max }}\), was carried out by questionnaire during an initial screening on their first visit. Participants were instructed to arrive at the laboratory rested and were advised to avoid caffeine and food 3 h prior each test and to avoid strenuous exercise and refrain from alcohol in the 24 h before each test. All tests were performed at the same time of day (± 2 h) in laboratory conditions within a controlled environment (18–22 °C; 45–55% relative humidity).
Experimental design
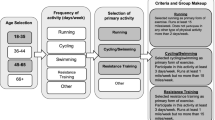
Participants were required to visit the laboratory on seven occasions within a 6-week period, with all tests separated by a minimum of 48 h (Fig. 1). All testing was performed on a motorised treadmill (Mercury, h/p/cosmos Sport and Medical, Traunstein, Germany). The first session was used to familiarise participants with the procedures and to conduct an incremental running test to determine velocity evoking gas exchange threshold (vGET), maximal aerobic velocity (MAV), and the maximum oxygen uptake (\(\dot{V}{\text{O}}_{{2\max }}\)). During the second and third visits, a series of constant work rate tests (CWR) at different intensities were performed to determine CV. On visits four to seven, participants performed in randomised order four experimental trails consisting of constant velocity test to task failure at velocities ranging from 95 to 115% of CV. During experimental trials lower limb kinematics were recorded throughout each trial.

Schematic of experimental design. CWR, constant work rate trials performed in a randomised order. Visits 2 and 3 were identical apart from the velocity at which the four CWR trials were performed (60% Δ, 70% Δ, 80% Δ and 100% MAV; where Δ refers to the velocity difference between vGET and the MAV). The numbers denote the order and not the velocity at which they were performed. Each of the visits 4–7 differed only in the velocity at which trials were performed (either 95%, 100%, 105%, or 115% CV in a randomised order)
Throughout all tests, pulmonary gas exchange was measured breath-by-breath using an online gas analyser (MetaLyzer 3B, Cortex Biophysik, Leipzig, Germany). The participants wore a face mask with low dead space (125 ml) and breathed through a low-resistance (< 0.1 kPa l−1 s−1 at 20 l s−1) impeller turbine, while O2 and CO2 were sampled at 50 Hz. The gas analyser was calibrated before each test with gases of known concentration and the turbine volume transducer was calibrated using a 3 l syringe (Hans Rudolph, Inc., Kansas City, MO). The analyser rise time and the transit delay for O2 and CO2 were < 100 ms and 800–1200 ms respectively, allowing breath-by-breath calculation. Therefore, \(\dot{V}{\text{O}}_{2}\), \(\dot{V}{\text{CO}}_{2}\), and \(\dot{V}_{{\text{E}}}\) data were recorded breath-by-breath and exported as a 10-s moving average for data analysis. Heart rate (HR) was recorded beat to beat using a heart rate monitor (Polar H7, Polar Electro, Kempele, Finland). Blood samples were collected from the fingertip into a capillary tube (10 μl) for analysis of blood [La] using an automated blood analyser (Biosen C-line, EKF Diagnostic, Barleben, Germany).
Measurements
Incremental exercise test
To determine vGET and MAV, an incremental exercise test to exhaustion was performed. The incline of the treadmill during this and all subsequent tests was set at 1% (Jones and Doust 1996). Following the completion of a standardised warm-up at a velocity of 1.67 m s−1 for 5 min, the test started at a velocity of 2.22 m s−1 and was increased by 0.14 m s−1 every minute until volitional exhaustion despite strong verbal encouragement.
Determination of critical velocity
A minimum of four CWR trials to task failure were performed at intensities that corresponded, approximately, to 60% Δ, 70% Δ, 80% Δ and 100% MAV; where Δ refers to the velocity difference between vGET and the MAV. This range of velocities was selected so that each participant could perform between 2–15 min before exhaustion (Muniz-Pumares et al. 2019). The CWR trials were performed in randomised order across two separate sessions, although in all testing sessions the lower intensity test always preceded the highest intensity test (Triska et al. 2017). On the second laboratory visit, two CWR trials were performed, with the final two CWR trials performed on the third laboratory visit. To avoid a possible priming effect in \(\dot{V}{\text{O}}_{2}\) and CV (Burnley et al. 2006; Karsten et al. 2018), a recovery period of 60-min was provided between CWR trials where participants were allowed to drink water ad libitum. Before the start of each CWR trial, all participants completed a standardised warm-up at a velocity of 1.67 m s−1 for 5 min, followed by a period of 3 min passive rest. The treadmill was then set to the criterion velocity where participants were required to stand with their feet astride the treadmill belt holding onto the handrails. The transitions from rest to running were performed by the participants using the handrails to suspend their body above the belt while they developed the velocity required with their legs. Timing for each trial began when the participant released the handrails and terminated when the participant grasped onto the handrails to signal task failure. Strong verbal encouragement was provided throughout, and participants were blinded to the velocity and elapsed time.
Experimental trials
During the final four visits runs were performed at velocities corresponding to 95%, 100%, 105% and 115% of the calculated CV (95% CV, 100% CV, 105% CV, and 115% CV). The velocities of experimental trials were calculated outside of the SEE for CV estimates, so that the trial below CV (95% CV) was 95% of CV minus 1 SEE, and trials above CV (105% CV and 115% CV) were the product of the percentage of CV plus 1 SEE. The order of these trials was randomised and completed in the same manner as the CWR trials, with the participant running until task failure despite strong verbal encouragement or for 20 min, whichever occurred first. Kinematic data from the right leg were used for analysis.
Motion analysis
Kinematic measures of the lower extremity were obtained using a 14-camera high speed motion capture system sampling at 200 Hz (10 Osprey cameras and 4 Raptor-E cameras; Motion Analysis Corp., Santa Rosa, CA). Prior to data collection the participants performed a static and dynamic calibration. The static calibration was performed using an L-frame with 4 retroreflective markers affixed placed on the corner of the treadmill. The dynamic calibration was performed by waving a wand with 3 retroreflective markers within the capture volume (approximately 5 × 2 × 3 m). A maximum standard deviation of 1.0 mm for the distance between markers was obtained. Data were inspected using Cortex software (Cortex-64 6.13.1751, Motion Analysis Corporation, Santa Rosa, CA) before importing into Visual 3D (Visual3D Version 5, C-motion, Germantown, MD).
A modified Helen Hayes marker set (Kadaba et al. 1990) was used to place 39 passive retroreflective markers (diameter 12 mm) on the skin bilaterally on the first metatarsals, between the second and third metatarsals, fifth metatarsals, calcaneus, lateral malleoli, medial malleoli, lateral femoral epicondyles, medial femoral epicondyles, iliac crests, anterior superior iliac spines and sacrum. Clusters of four markers were affixed bilaterally to the lateral aspect of the shank and thigh and were secured with rigid tape. To minimise interference effects and movement artifact during running, wands were not used during marker placement. Definitions for hip, knee, and ankle joint centres remained consistent with the Helen Hayes model (Kadaba et al. 1990), and additional markers were utilised to enable more consistent marker tracking. Previous pilot work demonstrated excellent intra- and inter-session reliability, evidenced by low coefficients of variation during dynamic movements using this marker set in sagittal (0.33–0.39%), frontal (1.22–1.41%), and transverse 2.11–3.12%) planes. From an initial static trial in the anatomical position, a kinematic model (pelvis, thigh, shank, and foot) was created for each participant. Ankle and knee joint centres were defined as the midpoint of the medial and lateral malleolus and the medial and lateral femoral epicondyle markers, respectively. The 3D coordinates of the hip joint centres were approximated using the coordinates of the reflective markers at the left and right anterior superior iliac spines and the marker at the sacrum (Bell et al. 1990). The foot, shank, and thigh were modelled as frustra of right cones, whereas the pelvis was modelled as a cylinder. Segmental anthropometric and geometrical properties were used based on the model by Hanavan (1964). Following the static trial, medial knee and medial ankle markers were removed for subsequent dynamic trials. Marker coordinates were smoothed using a 6 Hz fourth-order low-pass Butterworth filter. Joint rotations were calculated based on a right-hand convention using Euler angles in a X (flexion/extension), Y (adduction/abduction), Z (internal/external rotation) rotation sequence. Kinematic data were exported for the right hip, knee, and ankle joint rotations in the sagittal, frontal and transverse planes of motion.
Data analysis
Determination of MAV and vGET
MAV was calculated as the velocity of the last stage of the incremental exercise test fully completed. If the final stage was not completed in full, MAV was calculated using the following equation:
where VL represents the last completed stage (m s−1), t is the time of the incomplete stage performed, 60 s refers to the step duration, and 0.14 m s−1 denotes the delta velocity from the previous stage. This linear interpolation was based on the methodology used by Kuipers et al. (1985), where maximal workload was computed instead of MAV. In the current study, velocity of last completed stage and delta velocity from the previous stage were used in lieu of last workload completed and final load increment, respectively. \(\dot{V}{\text{O}}_{{2\max }}\) corresponded to the highest \(\dot{V}{\text{O}}_{{2}}\) average obtained over a 30-s rolling average. vGET was established as the velocity that elicited the following criteria: (1) the first disproportionate increase in \(\dot{V}{\text{CO}}_{{2}}\) from visual inspection of individual plots of \(\dot{V}{\text{CO}}_{{2}}\) versus \(\dot{V}{\text{O}}_{{2}}\); (2) an increase in \(\dot{V}_{{\text{E}}}\)/\(\dot{V}{\text{CO}}_{{2}}\) with no concomitant increase in \(\dot{V}_{{\text{E}}}\)/\(\dot{V}{\text{O}}_{{2}}\); and (3) the first increase in end-tidal O2 with no fall in end-tidal CO2 tension (Vanhatalo et al. 2016).
CV estimation
The CV was estimated using three 2-parameter models: (1) the hyperbolic v-Tlim model, where the velocity is plotted against time (Eq. 2); (2) the linear distance-time model, where the distance covered is plotted against time (Eq. 3), and (3) the linear inverse-of-time model, where the velocity is plotted against the inverse of time (Eq. 4):
where Tlim is time to task failure, D′ is the curvature constant, v is the velocity of the task, D is the distance performed, and CV is the asymptote termed critical velocity. The SEE associated with the CV obtained from the three models was calculated and expressed as coefficient of variation. A pre-determined threshold for SEE was set at 5% for estimates of CV and 10% for D′ (Muniz-Pumares et al. 2019). Where four constant velocity trials did not result in estimations of CV and D′ falling with the SEE thresholds, additional trials were performed until the SEE of the estimated CV was < 5%. To minimise error associated with modelling the velocity-duration relationship, the model (Eqs. 2, 3, or 4) with the smallest SEE for CV and D′ was used to give the ‘best individual fit’ estimate (Black et al. 2015, 2017).
Variability and complexity
Variability and complexity analysis were performed using MATLAB 2018b (Mathworks, Natick, MA). First, the initial and final 5 s of each trial were discarded (Terrier and Olivier 2011). Prior to linear and nonlinear analysis of the dependant variables time series were divided into 30 s epochs. Measures of complexity and variability were then performed on the steadiest 20 s of each epoch, identified as the consecutive 20 s with the lowest standard deviation (Pethick et al. 2016). The degree of complexity of dependant variables was quantified using SampEn (Eq. 5) in accordance with the algorithm detailed by Richman and Moorman (2000). SampEn (m, r, N) is the negative natural logarithm of the conditional probability that if two sequences of data of length m are both within the same distance r, then two sequences of data of length m + 1 are also within the same r (Richman and Moorman 2000). The parameters (m, r) were set (m = 2, r = 0.2) to allow for good conditional probability estimates whilst maintaining sufficient system information (Pincus et al. 1994), and in accordance with several studies examining gait (Arshi et al. 2015; Schütte et al. 2015; Murray et al. 2017; Vieira et al. 2017). SampEn quantifies a positive number typically between 0 and 2, with lower values towards 0 reflecting a high system regularity and low complexity and high values towards 2 representing a low system regularity and high complexity (Richman and Moorman 2000; Ramdani et al. 2009):
where r is the tolerance threshold, m is the template length, N is the length of the time series. Bi is the number of matches that remain similar, given the tolerance r, of the ith template of length m. Ai is then given as the number of matches that remain similar for the ith template of length m + 1. The quantity given as A/B is therefore the probability that two sequences within a tolerance of r for m points, remain within r of each other at the next point (m + 1). The fractal scaling of the time series was assessed using detrended fluctuation analysis (DFA; Eq. 6) as defined by Peng et al. (1994). Briefly, this method integrates the time series N, and then divides it into boxes of length n. A least-squares line is then fitted yn (k) in each box of length n, representing the trend in each box. The y coordinate of the straight line segments is denoted by yn (k). The integrated time series y (k) is detrended, by subtracting yn (k) from the local trend in each box. A root-mean-square calculation is then used to compute the magnitude of fluctuation, F (n), of y (k), from the least square trend in each box. For a box of length n, the size of fluctuation for the integrated and detrended time series is given as:
where F (n) is the average fluctuation, n is the box length, N is the total number of data points, k is the order of integration, y (k) is the integrated time series, and yn (k) is the local trend in its respective box. This process is then repeated across a range of box sizes (56 box sizes ranging from 4—N/4 data points) to provide a relationship between box size and F (n). The slope between log F (n) and log (n) represents the scaling exponent α, which corresponds to the correlational properties of the signal (Hu et al. 2001; Seely and Macklem 2004). Variability of the time series were quantified using standard deviation. Coefficient of variation was not used due to it being overly sensitive for mean values close to zero (Abdi 2010) which would be expected of transverse and frontal kinematics.
Statistical analysis
Kolmogorov–Smirnov tests for normality were conducted on the data. A two-way analysis of variance was performed on the SampEn and DFA values to test the effects of velocity (95% CV, 100% CV, 105% CV, and 115% CV) and time (Start and End) on the results. A one-way analysis of variance was performed to test the effects of velocity (95% CV, 100% CV, 105% CV, and 115% CV) on time to task failure (Tlim), end pulmonary \(\dot{V}{\text{O}}_{{2}}\), and blood [La] responses. Differences in \(\dot{V}{\text{O}}_{{2}}\) between CWR trials incremental exercise test, as well as experimental trials and incremental exercise test, were assessed using a one-way analysis of variance. Pairwise comparisons were conducted using Bonferroni adjustments where main effects and interactions were significant (P < 0.05). The assumption of sphericity was tested using Mauchly’s test, with Huynh–Feldt corrections made for violations (P < 0.05). All data are presented as means ± SD, and results were deemed statistically significant when P < 0.05. All statistical analyses were performed using SPSS (version 25.0; SPSS Inc, Chicago, IL).
Results
Preliminary measures and physiological responses
The mean vGET and MAV recorded during the first visit were 3.20 ± 0.44 m s−1 and 4.88 ± 0.41 m s−1, respectively. The mean \(\dot{V}{\text{O}}_{{2\max }}\) measured in the incremental exercise test was 3.77 ± 0.30 l min−1 (53 ± 5 ml min−1 kg−1) and was not significantly different from the mean \(\dot{V}{\text{O}}_{{2}}\) in CWR trials performed to estimate CV (3.62 ± 0.37 l min−1) measured at Tlim (P = 0.696). Estimates of CV derived from Eqs. (2–4) and “best individual fit” model are presented in Table 1. All participants were able to continue for 20 min without reaching task failure at 95% CV. Increased velocities resulted in significantly reduced Tlim above CV (Table 2). There was a significant effect on pulmonary \(\dot{V}{\text{O}}_{{2}}\) at Tlim (P = 0.022) with post-hoc analysis showing pulmonary \(\dot{V}{\text{O}}_{{2}}\) at Tlim was significantly greater in the trial at 105% CV (3.53 ± 0.39 l min−1) compared to trials performed at 100% CV (3.40 ± 0.35 l min−1) and 95% CV (3.27 ± 0.30 l min−1) (P < 0.05). Trials performed at 115% CV resulted in a \(\dot{V}{\text{O}}_{{2}}\) at Tlim of 3.37 ± 0.40 l min−1 which was not significantly different from other velocities. The \(\dot{V}{\text{O}}_{{2}}\) measured during the incremental exercise test differed from \(\dot{V}{\text{O}}_{{2}}\) at Tlim in trials performed at 95% CV (P < 0.001), 100% CV (P = 0.009), and 115% CV (P = 0.012), but not 105% CV (P = 0.847). Similarly, a significant effect was evident on HR at Tlim (P < 0.001; Table 2). Trials performed at or above CV resulted in significantly higher blood [La] when compared to the trial performed at 95% CV (P < 0.001; Table 2).
Linear analysis
The standard deviation of each running velocity for dependent variables in the first and last epoch is presented in Table 3. There were no significant velocity × time interactions (P > 0.05). There was a significant effect for time on standard deviation for ankle plantar/dorsiflexion (P = 0.032) and internal/external rotation (P = 0.006), knee internal/external rotation (P = 0.001), and hip flexion/extension (P = 0.001) and abduction/adduction (P = 0.002), with greater variability during the last 30-s epoch. There was a significant main effect for velocity on hip flexion/extension standard deviation with greater variability observed at higher velocities (P < 0.001, Fig. 2). There were significant main effects for velocity on knee flexion/extension SD (P = 0.015) and hip abduction/adduction standard deviation (P = 0.044) but no significant differences were observed using Bonferroni correction.

Changes to hip flexion/extension sample entropy (a), DFA-α (b), and standard deviation (c) over the course of trials performed at 95% CV (open circles), 100% CV (black circles), 105% CV (open squares), and 115% CV (black squares). For clarity error bars (± SD) have been omitted for all but the final data point. *Different from first epoch P < 0.05; aDifferent from 115% CV P < 0.05; bDifferent from 105% CV P < 0.05
Nonlinear analysis
The SampEn and DFA-α values for the first and last epoch for all conditions are presented in Tables 4 and 5, respectively. No significant velocity × time interactions were evident in SampEn (P > 0.05). There was a significant effect for time on SampEn in knee flexion/extension, with greater regularity in the last epoch compared to the first (P = 0.014). Conversely, hip internal/external rotation demonstrated more complex fluctuations in the last epoch when compared to the first during trials at or above CV (P = 0.001, Fig. 4). There was a significant effect for velocity on SampEn for hip flexion/extension (P = 0.001). There was also a significant effect for velocity on SampEn of hip internal/external rotation (P = 0.049), but subsequent pairwise comparisons showed no significant differences between velocities. There were significant velocity × time interactions of DFA-α evident in knee adduction/abduction (P = 0.049) and hip flexion/extension (P = 0.003, Fig. 2). DFA-α in knee adduction/abduction was lower in trials performed at 115% CV (P = 0.001). DFA-α was lower in ankle plantar/dorsiflexion during trials at 115% CV, indicating less statistical persistence, than at 105% CV and 100% CV (P = 0.003). Trials performed at higher velocities resulted in reduced statistical self-similarity at the hip, with lower DFA-α values in hip flexion/extension (P < 0.001, Fig. 2), hip adduction/abduction (P = 0.008, Fig. 3), and hip internal/external rotation (P = 0.001, Fig. 4). In trials at or below CV, DFA-α in knee internal/external rotation increased over time (P = 0.042).

Changes to hip adduction/abduction sample entropy (a), DFA-α (b), and standard deviation (c) over the course of trials performed at 95% CV (open circles), 100% CV (black circles), 105% CV (open squares), and 115% CV (black squares). For clarity error bars (± SD) have been omitted for all but the final data point. *Different from first epoch P < 0.05; aDifferent from 115% CV P < 0.05

Changes to hip internal/external rotation sample entropy (a), DFA-α (b), and standard deviation (c) over the course of trials performed at 95% CV (open circles), 100% CV (black circles), 105% CV (open squares), and 115% CV (black squares). For clarity error bars (± SD) have been omitted for all but the final data point. *Different from first epoch P < 0.05; aDifferent from 115% CV P < 0.05
Discussion
The purpose of the current study was to characterise changes to the pattern of variability and complexity of lower limb joint kinematics during running at different velocities relative to CV. The distinct physiological profile observed during the experimental trials (Table 2) suggests CV was approximated correctly (Ozyener et al. 2001). Data observed in the sagittal plane at the hip suggest that there was an increase in complexity and variability of proximal lower limb joint kinematics above the CV. Significant decreases in DFA-α observed at 115% CV in ankle plantar/dorsiflexion, knee abduction/adduction, hip abduction/adduction, and hip external/internal rotation indicated increased complexity above CV. The hypothesis that lower complexity would be evident above the CV when compared to trials at or below the CV is therefore refuted. Variability increased in a number of variables from the first epoch to last epoch. Demonstrable changes as a result of time were not evident across complexity of all variables and DFA-α and SampEn values behaved consistently between velocities below, at, and above CV. Changes in locomotor behaviour in some variables were evident only through the use of non-linear methods, suggesting these may be complimentary to non-linear methods. Ultimately, this may enable better understanding on running biomechanics in research and clinical practice. The current study has elucidated phenomena, herein discussed, which form the basis of further research in the application of non-linear analyses in running.
Effect of running velocity on variability and complexity
The findings of the current study suggest that greater complexity, as demonstrated by higher SampEn values and lower DFA-α values, and variability of angular kinematics, are evident at 115% CV compared to lower velocities. This was observed alongside similar metabolic conditions, as inferred by comparable blood [La] between 105% CV and 115% CV, which suggests that complexity and variability of movement during running may be more strongly mediated by velocity rather than metabolic rate per se. It has previously been suggested that increases to complexity and variability at greater velocities of locomotion may be a protective mechanism against injury, allowing for greater accommodation of external stressors (Estep et al. 2018). Indeed, running at greater velocities has been shown to increase the magnitude of potentially injurious variables including: ground reaction force (Keller et al. 1996), and accelerations acting on the body in the vertical, mediolateral, and anteroposterior planes (Sheerin et al. 2019). Risk of injury as a result of external perturbations may be increased at greater velocities due to increased forces and, if there is a resultant angular excursion, greater external joint moments. Furthermore, the time in which the system has to detect, identify, and adapt to external perturbations when moving at greater velocities is decreased (Biewener and Daley 2007). Indeed, runners with a history of medial tibial stress syndrome exhibited decreased complexity towards the end of a 3.2 km run (Schütte et al. 2018). Previous literature has expounded the relationship between runners with overuse injuries and diminished coordinative variability (Miller et al. 2008; Hamill et al. 2012; Schütte et al. 2018). It could, therefore, be argued that the decrease in complexity may predispose runners to injury due to a diminished ability to adapt to environmental threats. Future lines of inquiry may wish to examine the role of complexity in mitigating injury risk and overcoming external perturbations. Indeed, a recent review proposed a greater understanding of non-linear systems may lead to better injury forecasting in athletes (Fonseca et al. 2020).
It is unclear whether complexity and variability of angular kinematics change proportionately with increased velocity of running over a range of different intensity domains. Both Murray et al. (2017) and McGregor et al. (2009) have demonstrated proportional changes in complexity in relation to velocities ranging from moderate to severe intensities using accelerometers. There has been evidence to suggest that critical torque, and by inference CV, may be a phase transition rather than a sudden threshold, whereby some physiological responses associated with the severe intensity domain are apparent 2 standard errors below the estimate (Pethick et al. 2020). Although the current study used velocities outside the 95% confidence intervals associated with CV estimates (95% confidence limits 3.86 to 4.08 m s−1), the velocities used for 95% CV (3.71 ± 0.38 m s−1) and 105% CV (4.21 ± 0.42 m s−1) were close to CV. This may have resulted in less pronounced differences in motor control between heavy and severe domains. Further research should examine changes to variability and complexity of lower limb angular kinematics over a greater range of intensities.
Previous works have demonstrated increased complexity of movement, as quantified by accelerometers (McGregor et al. 2009; Murray et al. 2017) as well as through the use of stride-to-stride measurements (Jordan et al. 2006) with greater running velocities. When considering the regularity of angular kinematics, greater complexity has been demonstrated during running when compared to walking (Estep et al. 2018). The entropy values shown by Estep et al. (2018) during running at a self-selected velocity are lower than the current study. The authors used approximate entropy which should result in similar values when similar data lengths are inputted to SampEn (Pethick et al. 2015). During running, Estep et al. (2018) reported an average velocity of running (2.56 ± 0.27 m s−1) was much lower when compared velocities in the current study which may account for the discrepancy between studies. No previous investigators have examined changes to the complexity of angular kinematics at different velocities of running using non-linear analysis, limiting direct comparisons to existing literature.
Effect of time on variability and complexity
Alterations to the complexity of lower limb kinematics during exercise were only evident in few variables at the hip and knee as a result of time (Tables 4, 5). When changes to complexity and variability were apparent over time, these occurred irrespective of intensity. In line with previous studies examining variability of spatiotemporal gait parameters including stride intervals (Mo and Chow 2018; García-Pinillos et al. 2020), a greater number of changes were evident in variability, demonstrated by increases in standard deviation between the first epoch and last epoch (Table 3). To the best of our knowledge, changes to the complexity of lower limb angular kinematics over time have not previously been explored. In line with previous studies using accelerometers (Schütte et al. 2018), it was anticipated that complexity of movement would decrease with time. It was expected that greater decreases in complexity in trials above CV would be evident. Increased regularity was evident in internal/external rotation at the hip at velocities equal to or above the CV. Similarly, when running at or below CV, knee internal/external rotation exhibited greater self-similarity in the last epoch when compared to the first. Changes as a result of time in this study are likely to be attributed to two mechanisms: fatigue or habituation. Habituation in this case would be changes to variability and complexity in order to adapt the neuromuscular system to the running environment (e.g. surface) and running demands (e.g. velocity).
Fatigue has been implicated with the onset of maladaptive movement patterns at the hip and has been implicated with numerous lower limb injuries (Dierks et al. 2008; Powers 2010; Schütte et al. 2018). The increased complexity of hip movement in the transverse plane over time in this study may indicate a protective mechanism which allows for greater adaptability to external stressors during increased fatigue. The increase in complexity observed in the current study suggests that the ability of the system to explore solutions to perturbations affecting the transverse plane improves over time at velocities equal to or above CV. This may be a strategy which mitigates the increased risk of injury by rendering the system more able to stabilise joints and decrease loading on passive structures. Conversely, at the knee during velocities at or below CV, DFA-α values increase over time indicating greater self-similarity. A similar finding was found at 95% in knee flexion/extension, with SampEn values decreasing indicating greater regularity. These phenomena may be due to habituation and a lack of external stressors acting about the knee joint at low velocities allowing it to ‘switch off’. The roles of the knee during running are to act as an intermediary between hip and ankle as well as contributing to lower extremity stiffness to ensure efficiency of movement. Extraneous complexity at lower velocities may be inefficient and this may be a method of maintaining efficiency during running at lower velocities. A similar strategy may have not been necessitated at the hip due to the importance of hip musculature in maintaining lower limb stability (Powers 2010), and the ankle due to its ability to respond rapidly to proprioceptive feedback (Voloshina and Ferris 2015).
A common feature of performing sustained running is a reduction in the force generating capacity of musculature over time (Nicol et al. 1991; Boullosa et al. 2011; Girard et al. 2012). Previous research has consistently demonstrated increased variability concomitantly with a decrease in force production (Pethick et al. 2015). Briefly, this phenomenon has been attributed to alterations in muscle activation including increased motor unit synchronisation (Taylor et al. 2003), changes to the physiological organisation of motor units (Missenard et al. 2009), and possible changes to common drive (Farina and Negro 2015). Whether these central mechanisms are independent of, or are adjustments to, peripheral mechanisms remain unclear. Given that changes to standard deviation were observed above and below CV, our findings support the notion that changes to variability are controlled centrally (Missenard et al. 2009). Due to increased motor unit synchronisation associated with fatigue (Taylor et al. 2003), the observation of changes to variability alongside minimal changes to the temporal structure of kinematics was unexpected. This may be due to temporal constraints on movement placed upon the participants by the use of a motorised treadmill (Lindsay et al. 2014). When considering whole body movements the variability of ground reaction force and knee moments decreased and time-dependent measures of variability (SampEn) increased with fatigue during a side stepping task (Cortes et al. 2014). The contrary findings of the current study may be explained by differences in task. Cortes et al. (2014) measured variability of a side-stepping task which had greater degrees of freedom than running on a treadmill. It has previously been suggested that excessive variability of movement as a result of running fatigue may represent a lack of coordination, leading to an increased energy expenditure (Le Bris et al. 2006). The increased variability in this study may be either be viewed as a loss of system control (Stergiou and Decker 2011), or as a response to increase adaptability in a temporally constrained environment to mitigate increased injury risks associated with fatigue.
In the current study, fatigue was not measured directly and so changes to complexity or variability between the first and last epochs cannot be solely attributed to the effects of fatigue. However, it is likely that task failure observed in velocities above CV coincided with a marked decrease in the force generating capacity of the lower limb musculature (Boullosa et al. 2011). It is likely that due to the lack of distinctive changes of complexity between velocities above and below CV, changes to variability during running are mediated by both central and peripheral fatigue. Pethick et al. (2019) showed decreases in the complexity and variability of torque output was inextricably linked to the accumulation of metabolites in isolated movements. It could be that due to greater cognitive demands of whole-body movement that the complexity and variability of lower limb kinematics are not wholly determined by accumulation of metabolites. Indeed, previous research examining dual-task gait has demonstrated changes to variability in walking with the addition of cognitive tasks (Beauchet et al. 2005; Yogev-Seligmann et al. 2008). These results alongside the current findings suggest that executive function and finite attentional resources affect variability and complexity of locomotion. This may explain the lack of clear differences between changes to movement complexity and variability throughout trials between velocities above and below CV. Moreover, the mechanisms by which fatigue occurs may be different in single joint isometric exercise when compared to running. The decline of torque production during single joint isometric exercise is likely to be due to events occurring at the muscle (Place et al. 2009; Burnley et al. 2012). In addition to locomotor muscles, whole-body exercise is associated with greater demands on the pulmonary system (Amann 2012), and is usually terminated with the attainment of \(\dot{V}{\text{O}}_{{2\max }}\) (Burnley and Jones 2018). Further research may seek to expound on the relationship between central and peripheral fatigue and complexity during whole body movement.
Proximal changes to movement variability and complexity
Differences in the amount of variability and complexity as a result of manipulating velocity occurred more frequently at the hip joint when compared to the knee and ankle. This may be explained by the morphology and neurology of the lower limb musculature. Previous studies have examined the respective contribution of the hip, knee and ankle muscular function when running velocity is increased (Lemaire and Robertson 1989; Belli et al. 2002; Hanon et al. 2005). According to the findings of the previous authors, the relative contribution of the hip musculature increases concomitantly with increased running velocity. During running, the knee and ankle maintain high joint stiffness before and during the contact phase to allow for economical force production and elastic energy savings (Biewener and Roberts 2000). The largely unchanged complexity and variability observed at the knee and ankle may be a control strategy to preserve running efficiency at higher velocities (Schütte et al. 2017). Furthermore, it has been suggested that muscles that act around the ankle rely on higher gain proprioceptive feedback from ground contact, in contrast to the hip which is primarily feed-forward controlled (Daley and Biewener 2006). Increases in complexity as a result of higher velocities seen primarily at the hip may increase the adaptability to external stressors within proximal musculature, which is relatively insensitive to changes during stance (Daley et al. 2007). This could act to preserve stability of the centre of mass during running at greater velocities. An increase in complexity of ankle movement at greater velocities may not be necessary to accommodate external stressors, due to higher gain proprioceptive feedback regulation and enhanced capability to respond to perturbations (Voloshina and Ferris 2015). Given the movement about the knee is largely dependent on the force balance between hip and ankle (Daley et al. 2007), the velocity mediated alterations at proximal and distal joints may not be large enough to alter knee dynamics.
Limitations
A motorised treadmill was used to maintain a controlled environment between testing sessions and to enable the collection of large kinematic datasets using 3D motion analysis. The velocity of running is more variable overground when compared to treadmill running, even when pacing is controlled (Riley et al. 2008). Furthermore, when compared to overground running, treadmill running has been shown to result in greater regularity through greater constraint and increased voluntary control (Lindsay et al. 2014). Therefore, the dynamics of lower limb kinematics exhibited in this study may not be fully representative of lower limb kinematics of overground running. Moderately trained endurance runners participated in this study, so comparisons with other level groups may be limited since biomechanical differences have been reported between endurance runners of different performance levels (Ogueta-Alday et al. 2018).
Conclusion
The findings of this study demonstrate changes to kinematic complexity and variability over time are consistent between heavy and severe intensity domains during running. The findings suggest the CV does not demark a boundary above which there are changes to complexity or variability in kinematics during treadmill running over time. Decreases in DFA-α and increased SampEn in a number of kinematic variables at 115% CV suggest that running at a velocity substantially above CV results in increased complexity of movement. Changes over time to angular kinematics during running on a motorised treadmill may be limited to fluctuations in variability in lieu of changes to complexity due to temporal constraints. Furthermore, changes to movement strategies adopted may be more pronounced at the hip when compared to more distal joints.
Change history
20 April 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00421-021-04671-y
Abbreviations
- CV:
-
Critical velocity
- CWR:
-
Constant work rate
- D′:
-
Curvature constant of velocity relative to time
- DFA:
-
Detrended fluctuation analysis
- DFA-α :
-
Detrended fluctuation analysis α exponent
- MAV:
-
Maximal aerobic velocity
- SampEn:
-
Sample entropy
- SEE:
-
Standard error of the estimate
- T lim :
-
Time to task failure
- V:
-
Velocity
- vGET:
-
Velocity-evoking gas exchange threshold
- \(\dot{V}{\text{O}}_{2}\) :
-
Oxygen uptake
References
Abdi H (2010) Coefficient of variation. Sage, Thousand Oaks
Amann M (2012) Pulmonary system limitations to endurance exercise performance in humans. Exp Physiol 97:311–318. https://doi.org/10.1113/expphysiol.2011.058800
Arshi AR, Mehdizadeh S, Davids K (2015) Quantifying foot placement variability and dynamic stability of movement to assess control mechanisms during forward and lateral running. J Biomech 48:4020–4025. https://doi.org/10.1016/j.jbiomech.2015.09.046
Beauchet O, Dubost V, Herrmann F, Kressig R (2005) Stride-to-stride variability while backward counting among healthy young adults. J Neuroeng Rehabil 2:1–9. https://doi.org/10.1186/1743-Received
Bell AL, Pedersen DR, Brand RA (1990) A comparison of the accuracy of several hip center location prediction methods. J Biomech. https://doi.org/10.1016/0021-9290(90)90054-7
Belli A, Lacour JR, Komi PV et al (1995) Mechanical step variability during treadmill running. Eur J Appl Physiol Occup Physiol 70:510–517. https://doi.org/10.1007/BF00634380
Belli A, Kyröläinen H, Komi PV (2002) Moment and power of lower limb joints in running. Int J Sports Med 23:136–141. https://doi.org/10.1055/s-2002-20136
Biewener AA, Daley MA (2007) Unsteady locomotion: integrating muscle function with whole body dynamics and neuromuscular control. J Exp Biol 210:2949–2960. https://doi.org/10.1242/jeb.005801
Biewener AA, Roberts TJ (2000) Muscle and tendon contributions to force, work, and elastic energy savings: a comparative perspective. Exerc Sport Sci Rev 28:99–107
Black MI, Jones AM, Bailey SJ, Vanhatalo A (2015) Self-pacing increases critical power and improves performance during severe-intensity exercise. Appl Physiol Nutr Metab 40:662–670
Black MI, Jones AM, Blackwell JR et al (2017) Muscle metabolic and neuromuscular determinants of fatigue during cycling in different exercise intensity domains. J Appl Physiol 122:446–459. https://doi.org/10.1152/japplphysiol.00942.2016
Boullosa DA, Tuimil JL, Alegre LM et al (2011) Concurrent fatigue and potentiation in endurance athletes. Int J Sports Physiol Perform 6:82–93. https://doi.org/10.1123/ijspp.6.1.82
Burnley M, Jones AM (2018) Power-duration relationship: physiology, fatigue, and the limits of human performance. Eur J Sport Sci 18:1–12. https://doi.org/10.1080/17461391.2016.1249524
Burnley M, Doust JH, Jones AM, Time AMJ (2006) O2 kinetics time required for the restoration of normal heavy exercise V following prior heavy exercise. J Appl Physiol 101:1320–1327. https://doi.org/10.1152/japplphysiol.00475.2006
Burnley M, Vanhatalo A, Jones AM (2012) Distinct profiles of neuromuscular fatigue during muscle contractions below and above the critical torque in humans. J Appl Physiol 113:215–223. https://doi.org/10.1152/japplphysiol.00022.2012
Cher PH, Worringham CJ, Stewart IB (2017) Human runners exhibit a least variable gait speed. J Sports Sci 35:2211–2219. https://doi.org/10.1080/02640414.2016.1262053
Cortes N, Onate J, Morrison S (2014) Differential effects of fatigue on movement variability. Gait Posture 39:888–893. https://doi.org/10.1002/nbm.3066.Non-invasive
Daley MA, Biewener AA (2006) Running over rough terrain reveals limb control for intrinsic stability. Proc Natl Acad Sci USA 103:15681–15686. https://doi.org/10.1073/pnas.0601473103
Daley MA, Felix G, Biewener AA (2007) Running stability is enhanced by a proximo-distal gradient in joint neuromechanical control. J Exp Biol 210:383–394. https://doi.org/10.1038/jid.2014.371
De Pauw K, Roelands B, Cheung S et al (2013) Guidelines to classify female subject groups in sport-science research. Int J Sports Physiol Perform 2:111–122. https://doi.org/10.1123/ijspp.2015-0153
Dierks TA, Manal KT, Hamill J, Davis IS (2008) Proximal and distal influences on hip and knee kinematics in runners with patellofemoral pain during a prolonged run. J Orthop Sports Phys Ther. https://doi.org/10.2519/jospt.2008.2490
Estep A, Morrison S, Caswell S et al (2018) Differences in pattern of variability for lower extremity kinematics between walking and running. Gait Posture 60:111–115. https://doi.org/10.1016/j.gaitpost.2017.11.018
Farina D, Negro F (2015) Common synaptic input to motor neurons, motor unit synchronization, and force control. Exerc Sport Sci Rev 43:23–33. https://doi.org/10.1249/JES.0000000000000032
Fonseca ST, Souza TR, Verhagen E et al (2020) Sports injury forecasting and complexity: a synergetic approach. Sport Med 50:1757–1770. https://doi.org/10.1007/s40279-020-01326-4
García-Pinillos F, Cartón-Llorente A, Jaén-Carrillo D et al (2020) Does fatigue alter step characteristics and stiffness during running? Gait Posture 76:259–263. https://doi.org/10.1016/j.gaitpost.2019.12.018
Girard O, Millet GP, Micallef JP, Racinais S (2012) Alteration in neuromuscular function after a 5 km running time trial. Eur J Appl Physiol 112:2323–2330. https://doi.org/10.1007/s00421-011-2205-8
Haken H, Kelso JS, Bunz H (1985) A theoretical model of phase transitions.pdf. Biol Cybern 51:347–356
Hamill J, Palmer C, Van Emmerik REA (2012) Coordinative variability and overuse injury. Sport Med Arthrosc Rehabil Ther Technol 4:1–9. https://doi.org/10.1186/1758-2555-4-45
Hanavan E (1964) A mathematical model of the human body. Springer, New York
Hanon C, Thépaut-Mathieu C, Vandewalle H (2005) Determination of muscular fatigue in elite runners. Eur J Appl Physiol 94:118–125. https://doi.org/10.1007/s00421-004-1276-1
Hausdorff JM, Peng CK, Ladin Z et al (1995) Is walking a random walk? Evidence for long-range correlations in stride interval of human gait. J Appl Physiol 78:349–358. https://doi.org/10.1152/jappl.1995.78.1.349
Hausdorff JM, Mitchell SL, Firtion R et al (1997) Altered fractal dynamics of gait: reduced stride-interval correlations with aging and Huntington’s disease. J Appl Physiol 82:262–269. https://doi.org/10.1152/jappl.1997.82.1.262
Hausdorff JM, Cudkowicz ME, Firtion R et al (1998) Gait variability and basal ganglia disorders: stride-to-stride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov Disord 13:428–437. https://doi.org/10.1002/mds.870130310
Hu K, Ivanov PC, Chen Z et al (2001) Effect of trends on detrended fluctuation analysis. Phys Rev E 64:1–19. https://doi.org/10.1103/PhysRevE.64.011114
Jones AM, Doust JH (1996) A 1% treadmill grade most accurately reflects the energetic cost of outdoor running. J Sports Sci. https://doi.org/10.1080/02640419608727717
Jones AM, Wilkerson DP, DiMenna F et al (2007) Muscle metabolic responses to exercise above and below the “critical power” assessed using 31P-MRS. AJP Regul Integr Comp Physiol 294:R585–R593. https://doi.org/10.1152/ajpregu.00731.2007
Jordan K, Challis JH, Newell KM (2006) Long range correlations in the stride interval of running. Gait Posture 24:120–125. https://doi.org/10.1016/j.gaitpost.2005.08.003
Kadaba MP, Ramakrishnan HK, Wootten ME (1990) Measurement of lower extremity kinematics during level walking. J Orthop Res. https://doi.org/10.1002/jor.1100080310
Karsten B, Baker J, Naclerio F et al (2018) Time trials versus time-to-exhaustion tests: effects on critical power, W0, and oxygen-uptake kinetics. Int J Sports Physiol Perform 13:183–188. https://doi.org/10.1123/ijspp.2016-0761
Keller TS, Weisberger AM, Ray JL et al (1996) Relationship between vertical ground reaction force and speed during walking, slow jogging, and running. Clin Biomech. https://doi.org/10.1016/0268-0033(95)00068-2
Kuipers H, Verstappen FTJ, Keizer HA et al (1985) Variability of aerobic performance in the laboratory and its physiologic correlates. Int J Sports Med 1:197–201. https://doi.org/10.1055/s-2008-1025839
Le Bris R, Billat V, Auvinet B et al (2006) Effect of fatigue on stride pattern continuously measured by an accelerometric gait recorder in middle distance runners. J Sports Med Phys Fitn 46:227
Lemaire ED, Robertson DGE (1989) Power in sprinting. Track Field J 35:13–17
Lindsay TR, Noakes TD, Mcgregor SJ (2014) Effect of treadmill versus overground running on the structure of variability of stride timing. Percept Mot Skills 118:331–346. https://doi.org/10.2466/30.26.PMS.118k18w8
Lipsitz LA, Goldberger AL (1992) Loss of “complexity” and ageing. JAMA 267:1806–1809. https://doi.org/10.1001/jama.1992.03480130122036
Mann R, Malisoux L, Nührenbörger C et al (2015) Association of previous injury and speed with running style and stride-to-stride fluctuations. Scand J Med Sci Sport 25:e638–e645. https://doi.org/10.1111/sms.12397
McGregor SJ, Busa MA, Skufca J et al (2009) Control entropy identifies differential changes in complexity of walking and running gait patterns with increasing speed in highly trained runners. Chaos. https://doi.org/10.1063/1.3147423
Meardon SA, Hamill J, Derrick TR (2011) Running injury and stride time variability over a prolonged run. Gait Posture 33:36–40. https://doi.org/10.1016/j.gaitpost.2010.09.020
Miller RH, Meardon SA, Derrick TR, Gillette JC (2008) Continuous relative phase variability during an exhaustive run in runners with a history of iliotibial band syndrome. J Appl Biomech 24:262–270. https://doi.org/10.1123/jab.24.3.262
Missenard O, Mottet D, Perrey S (2009) Factors responsible for force steadiness impairment with fatigue. Muscle Nerve 40:1019–1032. https://doi.org/10.1002/mus.21331
Mo S, Chow DHK (2018) Stride-to-stride variability and complexity between novice and experienced runners during a prolonged run at anaerobic threshold speed. Gait Posture 64:7–11. https://doi.org/10.1016/j.gaitpost.2018.05.021
Muniz-Pumares D, Karsten B, Triska C, Glaister M (2019) Methodological approaches and related challenges associated with the determination of critical power and curvature constant. J Strength Cond Res 33:584–596
Murray AM, Ryu JH, Sproule J et al (2017) A pilot study using entropy as a non-invasive assessment of running. Int J Sports Physiol Perform 11:1–13. https://doi.org/10.1123/ijspp.2016-0205
Nicol C, Komi PV, Marconnet P (1991) Fatigue effects of marathon running on neuromuscular performance: II. Changes in force, integrated electromyographic activity and endurance capacity. Scand J Med Sci Sports 1:18–24. https://doi.org/10.1111/j.1600-0838.1991.tb00266.x
Ogueta-Alday A, Morante JC, Gómez-Molina J, García-López J (2018) Similarities and differences among half-marathon runners according to their performance level. PLoS ONE 13:1–11. https://doi.org/10.1371/journal.pone.0191688
Ozyener F, Rossiter HB, Ward S, Whipp BJ (2001) Influence of exercise intensity on the on- and off-transient kinetics of pulmonary oxygen uptake in humans. J Physiol 533:891–902. https://doi.org/10.1111/j.1469-7793.2001.t01-1-00891.x
Peng CK, Buldyrev SV, Havlin S et al (1994) Mosaic organization of DNA nucleotides. Phys Rev E 49:1685–1689. https://doi.org/10.1103/PhysRevE.49.1685
Pethick J, Winter SL, Burnley M (2015) Fatigue reduces the complexity of knee extensor torque fluctuations during maximal and submaximal intermittent isometric contractions in man. J Physiol 593:2085–2096. https://doi.org/10.1113/jphysiol.2015.284380
Pethick J, Winter SL, Burnley M (2016) Loss of knee extensor torque complexity during fatiguing isometric muscle contractions occurs exclusively above the critical torque. Am J Physiol Regul Integr Comp Physiol 310:R1144–R1153. https://doi.org/10.1152/ajpregu.00019.2016
Pethick J, Winter SL, Burnley M (2019) Relationship between muscle metabolic rate and muscle torque complexity during fatiguing intermittent isometric contractions in humans. Physiol Rep. https://doi.org/10.14814/phy2.14240
Pethick J, Winter SL, Burnley M (2020) Physiological evidence that the critical torque is a phase transition not a threshold. Med Sci Sport Exerc. https://doi.org/10.1249/mss.0000000000002389
Pincus SM (1991) Approximate entropy as a measure of system complexity. Mathematics 88:2297–2301. https://doi.org/10.1073/pnas.88.6.2297
Pincus SM, Goldberger AL, Investigator (1994) Physiological time-series analysis: what does regularity quantify? Am J Physiol 266:H1643–H1656
Place N, Bruton JD, Westerblad H (2009) Mechanisms of fatigue induced by isometric contractions in exercising humans and in mouse isolated single muscle fibres. Clin Exp Pharmacol Physiol 36:334–339. https://doi.org/10.1111/j.1440-1681.2008.05021.x
Poole DC, Burnley M, Vanhatalo A et al (2016) Critical power: an important fatigue threshold in exercise physiology. Med Sci Sports Exerc 48:2320–2334. https://doi.org/10.1249/MSS.0000000000000939
Powers CM (2010) The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther 40:42–51. https://doi.org/10.2519/jospt.2010.3337
Ramdani S, Seigle B, Lagarde J et al (2009) On the use of sample entropy to analyze human postural sway data. Med Eng Phys 31:1023–1031. https://doi.org/10.1016/j.medengphy.2009.06.004
Richman JS, Moorman RJ (2000) Physiological time-series analysis using approximate entropy and sample entropy. Am j Physiol Hear Circ Physiol 278:H2039–H2049. https://doi.org/10.1152/ajpheart.2000.278.6.H2039
Riley PO, Dicharry J, Franz J et al (2008) A kinematics and kinetic comparison of overground and treadmill running. Med Sci Sports Exerc 40:1093–1100. https://doi.org/10.1249/MSS.0b013e3181677530
Schütte KH, Maas EA, Exadaktylos V et al (2015) Wireless tri-axial trunk accelerometry detects deviations in dynamic center of mass motion due to running-induced fatigue. PLoS ONE 10:1–12. https://doi.org/10.1371/journal.pone.0141957
Schütte KH, Sackey S, Venter R, Vanwanseele B (2017) Energy cost of running instability evaluated with wearable trunk accelerometry. J Appl Physiol. https://doi.org/10.1152/japplphysiol.00429.2017
Schütte KH, Seerden S, Venter R, Vanwanseele B (2018) Influence of outdoor running fatigue and medial tibial stress syndrome on accelerometer-based loading and stability. Gait Posture 59:222–228. https://doi.org/10.1016/j.gaitpost.2017.10.021
Seely AJE, Macklem PT (2004) Complex systems and the technology of variability analysis. Crit Care 8:367–384. https://doi.org/10.1186/cc2948
Sheerin KR, Reid D, Besier TF (2019) The measurement of tibial acceleration in runners—a review of the factors that can affect tibial acceleration during running and evidence-based guidelines for its use. Gait Posture 67:12–24. https://doi.org/10.1016/j.gaitpost.2018.09.017
Stergiou N, Decker LM (2011) Human movement variability, nonlinear dynamics, and pathology: is there a connection? Hum Mov Sci 30:869–888. https://doi.org/10.1016/j.humov.2011.06.002
Taylor AM, Christou EA, Enoka RM (2003) Multiple features of motor-unit activity influence force fluctuations during isometric contractions. J Neurophysiol 90:1350–1361. https://doi.org/10.1152/jn.00056.2003
Terrier P, Olivier D (2011) Kinematic variability, fractal dynamics and local. J Neuroeng Rehabil 12:1–13. https://doi.org/10.1186/1743-0003-8-12
Triska C, Karsten B, Nimmerichter A, Tschan H (2017) Iso-duration determination of D′ and CS under laboratory and field conditions. Int J Sports Med 38:527–533. https://doi.org/10.1055/s-0043-102943
Vanhatalo A, Black MI, DiMenna FJ et al (2016) The mechanistic bases of the power–time relationship: muscle metabolic responses and relationships to muscle fibre type. J Physiol 594:4407–4423. https://doi.org/10.1113/JP271879
Vieira MF, Rodrigues FB, de Sá e Souza GS et al (2017) Linear and nonlinear gait features in older adults walking on inclined surfaces at different speeds. Ann Biomed Eng 45:1560–1571. https://doi.org/10.1007/s10439-017-1820-x
Voloshina AS, Ferris DP (2015) Biomechanics and energetics of running on uneven terrain. J Exp Biol 218:711–719. https://doi.org/10.1242/jeb.106518
Yogev-Seligmann G, Hausdorff JM, Giladi N (2008) The role of executive function and attention in gait. Mov Disord 23:329–342. https://doi.org/10.1002/mds.21720
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by BH. The first draft of the manuscript was written by BH and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
The study was approved by the Health, Science, Engineering and Technology Ethics Committee of the University of Hertfordshire (protocol number: LMS/PGR/UH/03454) and adhered to the Declaration of Helsinki.
Consent to participate
All participants gave their informed consent prior to their inclusion in the study.
Additional information
Communicated by Lori Ann Vallis.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hunter, B., Greenhalgh, A., Karsten, B. et al. A non-linear analysis of running in the heavy and severe intensity domains. Eur J Appl Physiol 121, 1297–1313 (2021). https://doi.org/10.1007/s00421-021-04615-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-021-04615-6