
Abstract
Purpose
This project aimed to quantify the effects of modifying computer work posture on neck/shoulder patterns during a prolonged typing task.
Method
Twenty healthy participants completed a 90-min typing task while sitting or walking on a treadmill. Electromyography (EMG) was recorded from eight upper body muscles and laser Doppler flowmetry (LDF) from two upper body sites. Effects of Time and Posture were assessed for EMG amplitude (RMS), variability (CoV), normalized mutual information (NMI), LDF and upper limb discomfort.
Results
Upper limb discomfort was higher during sitting and increased with time, from 0.86 ± 1.3 to 3.7 ± 3.1 out of 10. Interaction effects showed that EMG amplitude decreased over time for the lumbar erector spinae (LES) (from 6.3 ± 2.9 to 5.6 ± 3.2 % MIVC) and wrist extensor (from 12.4 ± 2.7 to 11.3 ± 3.5 % MIVC) during walking, but increased during sitting. Anterior Deltoid EMG amplitude was 64 % lower during walking while External Oblique EMG amplitude (43 %) and Lower Trapezius EMG variability (65 %) were higher during walking. Interaction effects showed higher LES CoV during walking compared to sitting (p = 0.019) in the beginning but not at the end of the task, and higher neck/shoulder NMI (p = 0.050) towards the end of the task during sitting compared to walking.
Conclusion
Results suggest that walking while performing computer work may be effective in inducing healthier muscular patterns, possibly explaining the lower level of discomfort compared to sitting.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Work-related musculoskeletal disorders (WRMSD) are chronic musculoskeletal symptoms which interfere with ones’ activities, can develop over time and can be partly or entirely related to a person’s main work (Stock et al. 2011). Larsson et al. (2007) identified neck/shoulder MSDs to typically develop from repetitive work, forceful exertions, high and/or prolonged static loads, and static or extreme postures. Previous literature has identified elements to support the presence of three injury pathways: a neuromuscular, a postural and a vascular one (Forde et al. 2002; Strom et al. 2009b).
Although the neck/shoulder load during computer work is quite low, with EMG values of associated muscles below 10 % of maximum contractions (Johansson et al. 1999; Roe and Knardahl 2002; Blangsted et al. 2004), increases in activity over time may still pose a risk for developing MSDs (Cooper and Straker 1998; Aaras et al. 1997; Kleine et al. 1999). However, previous studies do not show a clear association between trapezius muscle activity amplitude and neck symptoms during computer work (Strom et al. 2009a), such that other measures of muscle activity may be better predictors of symptoms. One such measure of muscle activity may be variability, which has been defined as the variation of behavioral outcomes over repetitions or time (Latash et al. 2002). Variability of the supraspinatus has been previously observed to increase with shoulder fatigue (Fedorowich et al. 2013), and greater variability of shoulder muscles has been seen in pain-free workers compared to those with pain (Madeleine et al. 2008b; Moseley and Hodges 2006). In addition, observing patterns of two muscles working together is another characteristic of muscle activity which has been studied lately. Mutual information (MI) is a statistical method which accounts for both linear and non-linear relationships as it quantifies shared activation patterns of two muscles’ electromyographic time series (Jeong et al. 2001; Kojadinovic 2005). Research has shown MI to increase with muscle fatigue and delayed onset muscle soreness (Madeleine et al. 2011) whereas another study found that initial low MI was a predictor of higher endurance (Fedorowich et al. 2013). Taken together, the recent literature suggests that high MI is not beneficial; however more experimental data need to be gathered to relate MI to better understood patterns associated with neck/shoulder work.
Blood flow plays an important role in supplying and regenerating muscles. Extended periods of computer work may compromise circulation, as flexed-neck or round shoulder postures could limit the thoracic circulatory area and blood flow to more distal structures (Keller et al. 1998). Physical activity has been proposed as a positive strategy in promoting blood flow, as cycling with relaxed shoulders has shown to increase blood flow to the shoulder and forearm (Andersen et al. 2010; Green et al. 2002; Tanaka et al. 2006). However, no studies have measured the effectiveness of methods to augment blood flow (e.g. through exercise) on the upper limb patterns during computer work.
Posture also appears to be a risk factor associated with MSD (Forde et al. 2002). Seated work may pose a risk as previous research has observed that neck pain was associated to prolonged sitting (odds ratio = 2.06) (Cagnie et al. 2007). A new trend in the workplace is Walk-and-Work workstations, with some documented benefits on physical activity as well as cardiovascular health (Thompson et al. 2008; Levine and Miller 2007). Nevertheless, one concern of this type of dual tasking is impairments in work performance which was seen by John et al. (2009) and Straker et al. (2009), although Funk et al. (2012) tested three walking speeds and found an optimal speed of 2.25 km/h where no effects were seen on typing performance. In one of the few studies on walk-and-work that accounted for acclimation to this novel task, a year-long study with treadmill workstations found all aspects of performance (quantity, quality, interaction quality) to exceed the initial performance measures (Ben-Ner et al. 2014). This may point to physical and psychological benefits of using a treadmill workstation, although the impacts on blood flow and musculoskeletal health, and the mechanisms underlying these potential benefits, remain unclear.
The objective of this study was to quantitatively assess the effects of Time and Posture on the muscular, vascular, discomfort and computer performance characteristics associated with a computer-typing task. To meet this objective, we recorded variables through time during the performance of a 90-min computer-typing task performed in the postures of sitting and walking on a treadmill. We hypothesized that there would be significant changes in our variables through Time and between Postures (but with no impact on computer performance measures), and that walking while working on the computer would alter the muscular, vascular and discomfort time responses.
Materials and methods
Participants
A convenience sample of 20 healthy young adults (10 males, 10 females; mean age = 27.65 ± 6.18 years; mean height = 169.72 ± 9.07 cm; mean mass = 69.31 ± 12.41 kg) was recruited by the researchers from the institutional social network. The inclusion criteria were the use of a computer for more than 40 h per 7 days, between the ages of 20 and 50, available for three experimental sessions, and free of neurological and musculoskeletal injuries, cardiovascular diagnoses and any other general health concern, as assessed by the Par-Q Health Questionnaire. A measure of perceived stress within the past month was assessed by a 14-question Perceived Stress Scale (PSS-14) (Cohen and Williamson 1988), which each participant completed prior to beginning the first experimental session. The study was performed at the Occupational Biomechanics and Ergonomics Lab (OBEL) of the Jewish Rehabilitation Hospital in Laval, Quebec. Informed, written consent was given by the participants prior to partaking, by signing forms approved by the Research Ethics Board of the Center for Interdisciplinary Research in Rehabilitation (CRIR) of Greater Montreal.
Session randomization
The three experimental sessions focused on recording data during the performance of a computer work task performed in the postures of sitting, standing or walking on a treadmill. In order to provide an opportunity for acclimation to the Walk-and-Work (WaW) task, that session could not be scheduled first. First a randomization process took place between the seated and standing sessions, then between the remaining session and the walking session. The WaW practice trial was performed at the end of the session preceding the WaW session. The sessions were separated by at least 48 h to avoid day-to-day fatigue or soreness effects. In this paper, we only report the analysis and results pertaining to the seated and WaW data.
Instrumentation
The participant was fitted with electromyographical (EMG) recording equipment (TeleMyo, Noraxon, USA, 10-350 Hz operating bandwidth). Eight muscle areas of the right arm, shoulder and trunk were prepared by being marked and shaved and then cleaned with rubbing alcohol to allow for better signal transmission. The Ag/AgCl surface electrodes (Ambu, Del) were then placed side by side in bipolar configuration, parallel to the muscle fibers. The 8 muscles were outfitted with electrodes in the same configuration each session. The placement over the cervical erector spinae (CES) was approximately 10 mm lateral to the C5 vertebra. For the upper trapezius (UT), the position was midpoint between C7 spinous process and acromion. Electrodes were also placed on the following sites—anterior deltoid (AD): between the lateral 1/3 of the clavicle and the deltoid tuberosity of the humerus; wrist extensor (Wext): over the muscle belly, approximately 2 finger widths distal to the elbow; middle trapezius (MT): midpoint between the thoracic spine and the medial border of the scapula; lower trapezius (LT): midpoint between the T8 spinous process and the inferior angle of the scapula; lumbar erector spinae (LES): midpoint between T12 and S1, along the lumbar spine over the transversus process; external oblique (EO): two finger widths below the last rib and three inches forward to the body’s midline (Basmajian and Blumenstein 1980). A reference electrode was placed over the right external epicondyle. Following this, the participant was outfitted with the cardiovascular equipment. Two laser Doppler flowmetry (FloLAB Monitor, Moor Instruments, Devon, England) electrodes were used: one positioned over the right UT, medial to the UT electrodes [shoulder LDF (SLDF)], and the second over the right Wext muscles, between the Wext electrodes and the external epicondyle [forearm LDF (FLDF)], to measure surface blood flow over the skin surface of these two areas.
Initial measures
After the electrodes and attached cables were placed and fixed with medical tape, the participant was instructed in completing maximum isometric voluntary contractions (MIVC), which were based on published standards (Basmajian and Blumenstein 1980; Madeleine et al. 2011). The UT was tested with the arm at the side; participants elevated their shoulder against external, static resistance applied on the shoulder. For the AD, the shoulder performed flexion with the arm flexed 45°, against resistance applied on the upper arm. The MT MIVC action consisted of scapula adduction with the shoulder at 90° flexion. The LT action was performed with the shoulder in an angle of 90° flexion and the scapula depressed against resistance applied under the upper arm. The Wext was tested by performing wrist extension from a neutral wrist angle, forearm pronated, with the arm resting on a table at 90° flexion in the elbow, against resistance applied on the dorsal part of the hand. To test the CES, subjects were lying prone, resistance was applied against the posterior aspect of the head, and the subject performed neck extension. The test for the LES involved the subject lying prone and performing lumbar extension with their arms at the side with stabilizing resistance applied on their hamstrings. To test the EO, the subject laid supine with knees flexed 90° and performed upper trunk flexion-rotation against resistance applied on the right pectoral, their trunk flexed 45°. A rigid frame structure was custom adapted to subject sizes to allow external resistance to be applied in the procedures for the first 4 muscles listed above, while resistance was applied manually for the last 4 muscles listed above. For each, two ramp-up, ramp-down, five-second MIVC trials were completed for each muscle with encouragement to push as hard as possible in the designated force direction. One minute of rest was given between each of the trials to ensure maximum effort was given in the next trial.
Next, subjects were positioned in the desired work posture (sitting or walking), which included adjusting the chair and computer desk. In the seated posture, an angle of 90° was created at the knee. In the walking session, the treadmill speed was programmed to 2.25 km/h as used in Funk et al. (2012). In all sessions, the work surface was adjusted to 5 cm below elbow height (Grandjean and Kroemer 1997) to maintain an approximate 90° elbow angle. After positioning the subject in the sessions’ computer work posture, the baseline cardiovascular measures were taken when the subject adopted a relaxed, static state. In order to see if stress affected the computer task, at this time the subject was asked to rate their pre-test level of stress on a scale of 0–10. The question posed was: “On a scale of 0-10 how stressed do you feel about participating in this session?” and the response was recorded.
Computer task
The typing task consisted of reproducing article text displayed on the computer using the Mavis Beacon Teaches Typing software, as used in Funk et al. (2012) and Straker et al. (2009). The subjects performed 10 blocks of 9 min each with EMG data collection taking place the last 30 s of each block. Immediately after each of these recordings, the participants were prompted to rest their arms at the sides of the computer. LDF was then collected for 30 s and during this time, participants were asked to refrain from shifting their body weight, in order to minimize movement artifacts in the LDF data. Following this, typing performance was recorded as average typing speed and errors during the previously finished block and discomfort was rated using a body map and discomfort scale (Messing et al. 2008; Antle et al. 2013). Subjects were prompted to indicate the body location(s) on the body map where they felt any discomfort, and for each identified region, they gave a number from 0 to 10 to indicate the intensity of this discomfort. At the end of the 90 min task, subjects again rated their stress level (on a scale of 0–10), and their response was recorded as post-test level of stress.
Data analysis
EMG data were filtered using a dual-pass fourth-order Butterworth band-pass of 20–500 Hz. The heartbeats were removed from the signals by first identifying a reference heartbeat in one trial and then cross-correlating it with the other signals to eliminate heartbeats from all 8 muscle signals. Following this, signals were full-wave rectified and then normalized to the EMG data collected during the MIVC, giving a percentage of the MIVC values for each muscle. Root-mean-square (RMS) values were calculated over 30 1-s non-overlapping windows for each collection period, and the 30 RMS values were averaged to obtain one representative mean amplitude value for each muscle from each collection block. Variability was calculated by computing coefficients of variation (CoV) for each muscle in each block by dividing the standard deviation of the 30 RMS values by the average RMS value.
Normalized mutual information (NMI) was calculated using EMG time series from each block. Calculations are detailed in Johansen et al. (2013). Briefly, NMI is based on the Entropy calculation, (average amount of information: H) of EMG time series where NMI is valued between 0, indicating no connectivity, and 1, indicating complete functional connectivity of the muscle pair. NMI was calculated for all the possible pairs in this study within two muscle groups: neck/shoulder group, CES, UT, AD, MT, LT, and trunk group, LES, EO. NMI of each muscle pair was calculated over 500-ms windows for each trial, and the median value was taken to represent the trial.
The data collected from LDF were integrated over non-overlapping 1 s windows for the 30 s time series. The 30, 1-s windows were averaged to obtain one representative value of blood flow following each work block. The initial LDF collection taken during the static state was considered the baseline blood flow measure, and the 10 following measures taken during the task were calculated as a percent change from this baseline. All analyses were done using Matlab software (Mathworks, Massachusetts, USA).
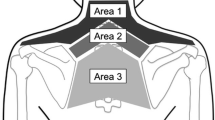
Since 79 % of subjects reported some discomfort in their neck/shoulder area (identified as the ensemble of the 6 regions shaded in yellow on the Fig. 1), we focused our discomfort analysis on this region, in analyzing the effects of Posture and Time on the highest discomfort score in that region. The highest score from the region, at each point in time, for each subject, was identified and kept for statistical analysis.

Body map used by subjects to indicate areas of discomfort. Region shaded in yellow indicates the six regions focused on for further analysis
Statistical analysis
Statistical analyses were performed to test the main effects of independent variables Time and Posture, as well as their interaction, on the muscular and vascular parameters. Time (blocks 1–10) × work posture (sit, walk) repeated measures ANOVA was run on the RMS, CoV, NMI and LDF variables. A Friedman ANOVA of work posture × time was run on discomfort measures reported for the neck/shoulder. A post hoc Wilcoxon paired analysis was run to establish where significant differences existed. Significance was set as p < 0.05. All analyses were run using SPSS software.
Results
Discomfort and performance
Upper limb (UL) reported discomfort was found to be significantly higher in the seated work posture (main Posture effect, Friedman ANOVA (19,19), 153.95, p < 0.0001) (see Fig. 2). Discomfort also significantly increased with time for each of the postures sit: Friedman ANOVA (19,9), 89.258, p < 0.0001 and walk: Friedman ANOVA (20,9), 53.831, p < 0.0001. Average performance measures after sitting for 9 min yielded errors: 105.2 ± 42.68 words; AWPM: 40.32 ± 11.85 words, and after 90 min, yielded errors: 113.6 ± 48.84 words; AWPM: 41.22 ± 11.12 words. The average performance measures after walking for 9 min were: errors: 96.85 ± 47.63 words; AWPM: 41.50 ± 9.54 words and after 90 min errors: 109.25 ± 50.68 words; AWPM: 42.25 ± 9.16 words. There were no significant effects found on any of the typing performance variables.

Discomfort ratings over time in the neck/shoulder area (group average values, SE). Significant posture effects were observed at each time period. Asterisks (*) denote a significant (p < 0.05) time-based difference with the data of time period 1 for the corresponding posture
Posture and time effects
Both the LES and Wext EMG RMS displayed decreases over time in the walking session but conversely increases with time were seen during sitting(significant Time × Posture interaction effects, LES [F(9,144) = 2.845, p = 0.004] (see Fig. 3a) and Wext [F(9,126) = 2.651, p = 0.008] (see Fig. 3b). The AD EMG RMS was found to be 64 % lower (as a % of MIVC) during walking compared to sitting, whereas the EO EMG RMS was found to be 43 % higher during walking compared to sitting (significant Posture main effects, AD [F(1,15) = 9.447, p = 0.008] and EO [F(1,15) = 19.001, p = 0.001]). LT average muscle activity displayed a significant 7 % increase from min 9 to min 90(main effect of time: [F(9,144) = 2.068, p = 0.036]). No other significant effects were found for average EMG RMS variables (see Table 1).

Normalized EMG RMS of the a LES muscle and b Wext muscle during sitting and walking (group average values, error bars indicate SEs). There were significant Time × Posture interaction effects (p < 0.05) for both muscles
The variability of LES was shown to somewhat decrease over time with walking, but to increase while sitting (Time × Posture interaction effect [F(9,144) = 2.306, p = 0.019] (see Fig. 4)). In addition, 65 % higher variability was displayed at the LT in the walking condition compared to sitting (Posture main effect [F(1,16) = 23.548, p = 0.000]). No other effects were found significant for any of the other variability parameters (see Table 2).

Variability (CoV) of the LES during sitting and walking. There was a significant Time × Posture interaction effect (p < 0.05)
There was an increase in CES-AD connectivity over time during sitting especially in the later blocks of the typing task, but an opposite pattern of decrease towards the end occurred during walking (significant Time × Posture interaction effect [F(9,135) = 1.951, p = 0.050])(see Fig. 5). CES-LT connectivity was found to increase over time, for the two postures (significant main effect of time, the [F(9,144) = 2.479, p = 0.012]). The walking condition displayed significantly greater LES-EO connectivity compared to sitting (main Posture effect [F(1,16) = 5.573, p = 0.031]). No other effects were found for any of the other muscle pairs. (See Table 3 for significant comparisons.)

Normalized mutual information for the muscle pair CES-AD. There was a significant Time × Posture interaction effect (p < 0.05)
LDF analyses looking at percent change from baseline found a trend toward increased blood flow with time at the shoulder [F(9,126) = 1.928, p = 0.054] and forearm [F(9,117) = 1.736, p = 0.088]. However, these results were found to not be statistically significant. There were no significant effects of Posture either (shoulder: [F(1,14) = 1.321, p = 0.270], forearm: [F(1,13) = 0.934, p = 0.351]).
The stress scale (0—indicating no stress up to 10—highly stressed) yielded a lack of change in response from pre- to post-test; therefore, these measures were chosen to be excluded from further analyses. During the sitting session, the average values were in the pre-test: M = 0.211, SD = 0.419; and post-test: M = 1.18, SD = 1.81 displaying little change in stress levels. Similarly during walking, average values were in the pre-test: M = 0.150, SD = 0.489; and post-test: M = 0.500, SD = 1.05 displaying a very small change from pre- to post-test.
Discussion
Discomfort and performance
UL discomfort was found to be significantly lower during walking compared to sitting. In addition, there was a later onset of discomfort while walking. Interestingly there were no effects of Time or Posture on any of the typing parameters. John et al. (2009) and Straker et al. (2009) both observed changes in computer performance while walking. However, those studies had not provided acclimation periods, and they used walking speeds of 1.6 and 3.2 km/h. In comparison, a 2.25 km/h walking speed (deemed to be an average, comfortable speed) was previously found to produce no decline in performance (Funk et al. 2012); therefore, we believed that using this speed would produce similarly stable performance measures. Thus, in order to obtain benefits from WaW without affecting performance, our results lead us to recommend an acclimation period, and regulation of the speed of walking while working.
Posture and time effects
Previous studies have suggested that increases in muscle activation over time may be associated with increased risk to develop musculoskeletal disorders (MSD) (Cooper and Straker 1998; Aaras et al. 1997; Kleine et al. 1999). Our results showed increases in EMG RMS values of the LES, Wext, AD, EO, and LT. These increases may be small especially when normalized to each muscle’s maximum voluntary activity level, but they were observed over only 90 min, suggesting that further increases could occur over a work day, which over time could represent a non-negligible accumulation of load during prolonged, long-term computer work. Moreover, both the LES and EO were more activated while walking, indicating that both may be working to stabilize the trunk and upper limbs against moving lower limbs, so that computer-typing movements can be adequately performed. Although higher activity may place these muscles at greater risk of developing injuries, the initially high activity of the LES during walking displayed a significant decrease over time and by the end of the 90-min task, reached nearly the same as the activity levels measured during sitting. One explanation is that motor learning takes place during the first few minutes of the walk-and-work task, with the body searching and finding upper trunk stabilizing strategies that at first depend on low back muscles, but that may eventually span more muscles. Conversely, the increases in activity seen while sitting may indicate a negative effect as this may place the LES more at risk of developing fatigue accumulation and injury in a prolonged sitting position. Previous studies have suggested that seated work may indeed place a higher strain on low back structures (Nachemson 1966; Wilke et al. 2001). However, little is known about the specific mechanisms that could underlie this higher low back load in the seated position (Mork and Westgaard 2009).
The Wext EMG RMS activity level was similar to levels reported previously during a seated computer task (Strom et al. 2009a). In our study, the significant interaction effect of the Wext muscle showed higher muscle activity during walking, although it increased over time only in sitting. This may reflect an attempt to stabilize the forearms when walking and typing, as walking creates more lateral body sway. The decreased Wext activity with time during walking can then be due to habituation to the WaW task, so over time the subjects may become better apt to type while walking.
The LES muscle displayed higher variability during walking compared to sitting. Higher motor variability has been hypothesized to prevent the development of symptoms and less variable movement patterns may be associated with a greater risk of injury (Mathiassen et al. 2003; Madeleine et al. 2008a). In the current study, the higher LES variability seen throughout the task during walking likely indicates a search to adapt to the novel task of typing while walking, although this also occurred during sitting. The fact that LES variability remains higher during walking compared to sitting, over the duration of the 90 min task, supports a protective effect of walking with regards to low back strain. Another postural muscle but this time for the shoulder girdle, the LT, which displayed higher variability while walking compared to sitting, may play a role in steadying the arms for typing. Therefore, greater variability in the LT may also indicate a healthy adaptive mechanism to performing a prolonged typing task in the standing position.
When looking at the analysis of between-muscle connectivity, three pairs of muscles exhibited significant effects. The increases over time seen in the CES-LT pair and the increase towards the end during sitting for the CES-AD pair seem in line with the findings from Madeleine et al. (2011) who found functional connectivity within the trapezius of males to increase with muscle fatigue. Although the computer task used in this project was not fashioned to induce muscle fatigue, the significant changes seen in EMG RMS muscle activation may support that some muscles experienced some fatigue. Therefore, the increased connectivity seen in these muscle pairs may suggest that over a prolonged time and during sitting, the CES may search for a muscle to partner with in order to share the load to continue the task, in line with the interpretation provided in Fedorowich et al. (2013). Conversely, during walking, the CES-AD pair showed a decrease in connectivity during the last few minutes of the task, which is in line with the decreases with time seen in NMI of the neck/shoulder area in the Fedorowich et al. (2013) study, although in that study, the task was performed to exhaustion. In that study, authors had interpreted the strategies of lowering NMI as efficient strategies of isolating muscle fatigue effects in order to prevent the spread of symptoms across more muscles. Furthermore, Svendsen et al. (2011) found lower NMI between muscle pairs in the forearm during a dynamic task compared to a static task which could indicate a beneficial muscular strategy during active work. Thus, our results of decreased CES-AD connectivity with time during walking could also seem to be a beneficial strategy.
Finally, the overall low level of muscle activity needed for the computer-typing task may be the reason for our fewer significant results compared to previous studies. Despite this, one last significant effect related to functional connectivity, the significantly higher mutual information between the trunk pair during walking, is easily explained by a need to coordinate the low trunk region during the highly stereotypical task of walking. However, it should be pointed out that it is possible that factors other than true differences in muscle activity firing may have impacted our findings especially for the walking condition. As such, the extra body movements produced during walking may have had an impact on the surface EMG signals; although we took care to stabilize the electrode cables against the moving limbs, it is possible that there was more movement of the electrodes relative to the muscles during the walking condition, inducing an additional source of error during those trials.
We initially hypothesized that walking would increase blood flow in the neck/shoulder, as exercise has previously been shown to augment blood flow in non-working limbs (Green et al. 2002; Tanaka et al. 2006) and more specifically, the neck/shoulder area (Anderson et al. 2010). However, this was not significant in our study. In previous studies, participants were not performing an upper limb task, and were instructed to relax their upper limbs, whereas in our study, the muscle activity required to stabilize the shoulders and forearms during computer work may have been sufficient to partly occlude blood flow to the upper limbs during walking. Lastly, our data may also be underpowered, although these studies referred to had on average 8 (Green, Tanaka, Anderson) and 28 (Strom) healthy participants, which is comparable to our sample size. Moreover, the observed power of some comparisons reached comparatively high values (AD EMG RMS Posture effect: 0.943; EO EMG RMS Posture effect: 0.982; LT EMG variability Posture effect: 0.995). Still, it is likely that some of the reported comparisons are affected by possible type II error. Further studies with larger sample sizes are necessary to confirm our findings.
In conclusion, the present study investigated the effects of modifying computer work posture on trunk and upper limb muscular and vascular patterns during a prolonged computer task. Walking displayed generally lower muscle activity and higher variability patterns whereas sitting was characterized by higher between-muscle functional connectivity and greater discomfort. This study contributes to the growing literature around walk-and-work computer workstations and may further help to identify mechanism-based interventions to reduce or even prevent neck/shoulder MSD.
Abbreviations
- AD:
-
Anterior deltoid
- ANOVA:
-
Analysis of variance
- AWPM:
-
Adjusted words per minute
- CES:
-
Cervical erector spinae
- CoV:
-
Coefficient of variation
- EMG:
-
Electromyography
- EO:
-
External oblique
- FLDF:
-
Forearm laser Doppler flowmetry
- LDF:
-
Laser Doppler flowmetry
- LES:
-
Lumbar erector spinae
- LT:
-
Lower trapezius
- MI:
-
Mutual information
- MIVC:
-
Maximum isometric voluntary contractions
- MSDs:
-
Musculoskeletal disorders
- MT:
-
Middle trapezius
- NMI:
-
Normalized mutual information
- PSS:
-
Perceived stress scale
- RMS:
-
Root-mean-square
- SLDF:
-
Shoulder laser Doppler flowmetry
- UL:
-
Upper limb
- UT:
-
Upper trapezius
- WaW:
-
Walk-and-work
- Wext:
-
Wrist extensor
- WRMSD:
-
Work-related musculoskeletal disorder
References
Aaras A, Fostervold KI, Ro O, Thoresen M, Larsen S (1997) Postural load during VDU work: a comparison between various work postures. Ergonomics 40:1255–1268. doi:10.1080/001401397187496
Andersen LL, Blangsted AK, Nielsen PK, Hansen L, Vedsted P, Sjogaard G, Sogaard K (2010) Effect of cycling on oxygenation of relaxed neck/shoulder muscles in women with and without chronic pain. Eur J Appl Physiol 110:389–394. doi:10.1007/s00421-010-1517-4
Antle DM, Cote JN (2013) Relationships between lower limb and trunk discomfort and vascular, muscular and kinetic outcomes during stationary standing work. Gait Posture 37:615–619. doi:10.1016/j.gaitpost.2012.10.004
Basmajian JV, Blumenstein R (1980) Electrode placement in EMG biofeedback. Williams & Wilkins, Baltimore
Ben-Ner A, Hamann DJ, Koepp G, Manohar CU, Levine J (2014) Treadmill workstations: the effects of walking while working on physical activity and work performance. PLoS ONE 9(2):e88620. doi:10.1371/journal.pone.0088620
Blangsted AK, Sogaard K, Christensen H, Sjogaard G (2004) The effect of physical and psychosocial loads on the trapezius muscle activity during computer keying tasks and rest periods. Eur J Appl Physiol 91:253–258. doi:10.1007/s00421-003-0979-z
Cagnie B, Danneels L, Van Tiggelen D, De Loose V, Cambier D (2007) Individual and work related risk factors for neck pain among office workers: a cross sectional study. Eur Spine J 16:679–686. doi:10.1007/s00586-006-0269-7
Cohen S, Williamson GM (1988) Perceived stress in a probability sample of the United-States. In: Spacapam S, Oskamp S (eds) The social psychology of health. Sage, Newbury Park
Cooper A, Straker L (1998) Mouse versus keyboard use: a comparison of shoulder muscle load. Int J Ind Ergonom 22:351–357. doi:10.1016/s0169-8141(97)00088-7
Fedorowich L, Emery K, Gervasi B, Cote JN (2013) Gender differences in neck/shoulder muscular patterns in response to repetitive motion induced fatigue. J Electromyogr Kinesiol 23:1183–1189. doi:10.1016/j.jelekin.2013.06.005
Forde MS, Punnett L, Wegman DH (2002) Pathomechanisms of work-related musculoskeletal disorders: conceptual issues. Ergonomics 45:619–630. doi:10.1080/00140130210153487
Funk RE, Taylor ML, Creekmur CC, Ohlinger CM, Cox RH, Berg WP (2012) Effect of walking speed on typing performance using an active workstation. Percept Motor Skill 115:309–318. doi:10.2466/06.23.26.pms.115.4.309-318
Grandjean E, Kroemer KHE (1997) Fitting the task to the human: A textbook of occupational ergonomics, 5th edn. Taylor & Francis, Philadelphia
Green D, Cheetham C, Mavaddat L, Watts K, Best M, Taylor R, O’Driscoll G (2002) Effect of lower limb exercise on forearm vascular function: contribution of nitric oxide. Am J Physiol-Heart C 283:H899–H907. doi:10.1152/ajpheart.00049.2002
Jeong J, Gore JC, Peterson BS (2001) Mutual information analysis of the EEG in patients with Alzheimer’s disease. Clin Neurophysiol 112:827–835
Johansen TI, Samani A, Antle DM, Cote JN, Madeleine P (2013) Gender effects on the coordination of subdivisions of the trapezius muscle during a repetitive box-folding task. Eur J Appl Physiol 113:175–182. doi:10.1007/s00421-012-2425-6
Johansson H, Sjolander P, Djupsjobacka M, Bergenheim M, Pedersen J (1999) Pathophysiological mechanisms behind work-related muscle pain syndromes. Am J Ind Med 36:104–106
John D, Bassett D, Thompson D, Fairbrother J, Baldwin D (2009) Effect of using a treadmill workstation on performance of simulated office work tasks. J Phys Act Hea 6:617–624
Keller K, Corbett J, Nichols D (1998) Repetitive strain injury in computer keyboard users: pathomechanics and treatment principles in individual and group intervention. J Hand Ther 11:9–26
Kleine BU, Schumann NP, Bradl I, Grieshaber R, Scholle HC (1999) Surface EMG of shoulder and back muscles and posture analysis in secretaries typing at visual display units. Int Arch Occ Environ Health 72:387–394. doi:10.1007/s004200050390
Kojadinovic I (2005) Relevance measures for subset variable selection in regression problems based on k-additive mutual information. Comput Stat Data Anal 49:1205–1227. doi:10.1016/j.csda.2004.07.026
Larsson B, Sogaard K, Rosendal L (2007) Work related neck-shoulder pain: a review on magnitude, risk factors, biochemical characteristics, clinical picture and preventive interventions. Best Pract Res Clin Rheumatol 21:447–463. doi:10.1016/j.berh.2007.02.015
Latash ML, Scholz JP, Schoner G (2002) Motor control strategies revealed in the structure of motor variability. Exerc Sport Sci Rev 30:26–31. doi:10.1097/00003677-200201000-00006
Levine JA, Miller JM (2007) The energy expenditure of using a “walk-and-work” desk for office workers with obesity. Br J Sports Med 41:558–561. doi:10.1136/bjsm.2006.032755
Madeleine P, Mathiassen SE, Arendt-Nielsen L (2008a) Changes in the degree of motor variability associated with experimental and chronic neck-shoulder pain during a standardised repetitive arm movement. Exp Brain Res 185:689–698. doi:10.1007/s00221-007-1199-2
Madeleine P, Voigt M, Mathiassen SE (2008b) The size of cycle-to-cycle variability in biomechanical exposure among butchers performing a standardised cutting task. Ergonomics 51:1078–1095. doi:10.1080/00140130801958659
Madeleine P, Samani A, Binderup AT, Stensdotter AK (2011) Changes in the spatio-temporal organization of the trapezius muscle activity in response to eccentric contractions. Scand J Med Sci Sports 21:277–286. doi:10.1111/j.1600-0838.2009.01037.x
Mathiassen SE, Moller T, Forsman M (2003) Variability in mechanical exposure within and between individuals performing a highly constrained industrial work task. Ergonomics 46:800–824. doi:10.1080/0014013031000090125
Messing KVN, Major M, Ouellet S, Tissot F, Couture V et al (2008) Body maps: an indicator of physical pain for worker-oriented ergonomic interventions. Pol Pract Health Safety 6:31–49
Mork PJ, Westgaard RH (2009) Back posture and low back muscle activity in female computer workers: a field study. Clin Biomech 24:169–175. doi:10.1016/j.clinbiomech.2008.11.001
Moseley GL, Hodges PW (2006) Reduced variability of postural strategy prevents normalization of motor changes induced by back pain: a risk factor for chronic trouble? Behav Neurosci 120:474–476. doi:10.1037/0735-7044.120.2.474
Nachemson A (1966) The load on lumbar disks in different positions of the body. Clin Orthop Relat Res 45:107–122
Roe C, Knardahl S (2002) Muscle activity and blood flux during standardised data-terminal work. Int J Ind Ergonom 30:251–264. doi:10.1016/s0169-8141(02)00129-4
Stock S, Funes A, DelisleA, St-Vincent M, Turcot A, Messing M (2011) Troubles musculo-squelettiques. In: Vézina M et al. Enquête québécoise sur des conditions de travail, d’emploi, et de santé et de sécurité du travail (EQCOTESST), Chapitre 7. Institut de recherche Robert-Sauvé en santé et sécurité du travail—Institut national de santé publique du Québec et Institut de la statistique du Québec
Straker L, Levine J, Campbell A (2009) the effects of walking and cycling computer workstations on keyboard and mouse performance. Hum Factors 51:831–844. doi:10.1177/0018720810362079
Strom V, Knardahl S, Stanghelle JK, Roe C (2009a) Pain induced by a single simulated office-work session: time course and association with muscle blood flux and muscle activity. Eur J Pain 13:843–852. doi:10.1016/j.ejpain.2008.11.003
Strom V, Roe C, Knardahl S (2009b) Work-induced pain, trapezius blood flux, and muscle activity in workers with chronic shoulder and neck pain. Pain 144:147–155. doi:10.1016/j.pain.2009.04.002
Svendsen JH, Samani A, Mayntzhusen K, Madeleine P (2011) Muscle coordination and force variability during static and dynamic tracking tasks. Hum Movement Sci 30:1039–1051. doi:10.1016/j.humov.2011.02.001
Tanaka H, Shimizu S, Ohmori F, Muraoka Y, Kumagai M, Yoshizawa M, Kagaya A (2006) Increases in blood flow and shear stress to nonworking limbs during incremental exercise. Med Sci Sport Exer 38:81–85. doi:10.1249/01.mss.0000191166.81789.de
Thompson WG, Foster RC, Eide DS, Levine JA (2008) Feasibility of a walking workstation to increase daily walking. Br J Sports Med 42:225–228. doi:10.1136/bjsm.2007.039479 (discussion 228)
Wilke HJ, Neef P, Hinz B, Seidel H, Claes L (2001) Intradiscal pressure together with anthropometric data - a data set for the validation of models. ClinBiomech 16:S111–S126. doi:10.1016/s0268-0033(00)00103-0
Acknowledgments
In addition to the participants in the study, the authors wish to thank David Antle, Amanda Farias and Zach Weber for their assistance in data collection and analyses. This research was supported by grant Grants from the Canadian Foundation for Innovation and the Institut de Recherche Robert-Sauvé en Santé etenSécurité du Travail (IRSST). Julie Côté holds a Gender, Work and HealthResearch Chair from the Canadian Institutes for HealthResearch and the IRSST.
Conflict of interest
No author has financial or personal conflicts of interest that could inappropriately influence their work.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Fausto Baldissera.
Rights and permissions
About this article

Cite this article
Fedorowich, L.M., Emery, K. & Côté, J.N. The effect of walking while typing on neck/shoulder patterns. Eur J Appl Physiol 115, 1813–1823 (2015). https://doi.org/10.1007/s00421-015-3163-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-015-3163-3