
Abstract
Purpose
To assess the effects of half-dose photodynamic therapy (PDT) combined with an intravitreous aflibercept (IVA) injection for pachychoroid neovasculopathy (PNV) and its predictive factors.
Methods
Clinical information of 43 patients (43 eyes) with PNV obtained before and 6 months after treatment with half-dose PDT combined with IVA was retrospectively analyzed. Patients were categorized into the sufficient (25 eyes, 58.1%) or insufficient (18 eyes, 41.9%) group based on resolution or persistence/recurrence of subretinal fluid (SRF), respectively, and clinical data were compared. Macular neovascularization (MNV) change was studied in 30 cases with available pre- and post-treatment optical coherence tomography angiography images.
Results
The sufficient group included younger patients with better baseline best-corrected visual acuity (BCVA), more treatment-naïve eyes, and smaller MNV lesions at baseline than the insufficient group (all, P < 0.047). Complete SRF resolution was 81.8% in treatment-naïve eyes and only 33.3% in previously treated eyes. MNV expanded after half-dose PDT was combined with IVA regardless of the treatment outcome (P = 0.003).
Conclusion
Half-dose PDT combined with IVA was effective for PNV treatment, especially for younger patients with good baseline BCVA, treatment-naïve eyes, and small MNV sizes at baseline. MNV expanded after treatment regardless of the treatment outcomes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.

Introduction
In recent years, pachychoroid disease has been proposed to be a spectrum of conditions caused by a pathologically thick choroid with dilated choroidal vessels and choroidal vascular hyperpermeability (CVH) [1, 2]. Several types of phenotypes exist in pachychoroid disease, including central serous chorioretinopathy (CSC), pachychoroid pigment epitheliopathy (PPE), pachychoroid neovasculopathy (PNV), and polypoidal choroidal vasculopathy. Occasionally, CSC or PPE persists for long periods and becomes chronic, leading to the development of type 1 macular neovascularization (MNV) referred to as “PNV” [3]. PNV pathogenesis may differ from conventional age-related macular degeneration (AMD), which is characterized by preceding drusen, while similarly developing MNV [2, 3]. PNV contributes to the pathogenesis of AMD, particularly among Asians, who have a higher prevalence of pachychoroid disease than Caucasians [2].
Anti-vascular endothelial growth factor (VEGF) therapy is the gold standard for treating AMD with MNV. Verteporfin photodynamic therapy (PDT) targeting CVH is widely used to treat chronic CSC. In particular, lower doses of verteporfin or reduced laser power (half-dose, half-fluence, and half-time PDT), which targets CVH, has been successfully applied previously [4,5,6,7,8]. Exudative changes in PNV may be caused by both MNV and CVH, and treatment options reportedly include vitreous injection of anti-VEGF drugs, several variations of PDT, or a combination of both [9,10,11,12,13,14,15], with no consensus. Combination therapy targeting both MNV and CVH may be effective, but it is also necessary to select appropriate therapy for individual case condition.
Thus, we investigated the effects of half-dose PDT combined with an intravitreous aflibercept (IVA) injection for PNV and its predictive factors.
Methods
Ethics statement
This retrospective observational case series two-center study was conducted according to the tenets of the Declaration of Helsinki and received the approval of the Institutional Review Board of the Nagoya University Graduate School of Medicine (2021–0339) and Kyorin University Graduate School of Medicine (1903). This study was registered with the University Hospital Medical Information Network (UMIN000046809). The Institutional Review Board granted a waiver of informed consent due to the retrospective nature of the study. We also published the present study on the Nagoya University network and Kyorin University network to allow patients to decline participation. All patient data were anonymized before analyses.
Participants
We collected data of consecutive eyes from patients diagnosed with PNV and treated with half-dose PDT combined with IVA at the Nagoya University Hospital and Kyorin University Hospital from June 2018 to August 2021, and followed up for at least six months.
The inclusion criteria were eyes diagnosed with PNV, regardless of whether they had been previously treated with anti-VEGF agents or PDT. The exclusion criteria were eyes with polypoidal choroidal vasculopathy diagnosed or suspected by optical coherence tomography (OCT), fluorescein angiography (FAG), and indocyanine green angiography (ICGA).
Patients included in the study underwent comprehensive ophthalmic examinations, including best-corrected visual acuity (BCVA), fundus photography, FAG and ICGA (Spectralis HRA + OCT, Heidelberg Engineering, Heidelberg, Germany), spectral domain OCT (Spectralis HRA + OCT, Heidelberg Engineering), and swept-source OCT angiography (OCTA) (Plex Elite 9000, Carl Zeiss Meditec Inc., Dublin, California, USA). Based on previous reports [12,13,14,15], we diagnosed PNV when all of the following clinical and morphological features of pachychoroid disease were observed in the same lesion. First, the outer choroidal dilation and inner choroidal attenuation were observed on OCT B-mode images following serous retinal detachment and flat irregular pigment epithelial detachment (PED). Second, CVH was observed on the corresponding ICGA images. Third and final, coinciding with the flat irregular PED observed in the OCT B-mode images, blood flow suggestive of MNV was detected on the OCTA image and leakage from it was detected on the FAG. Central choroidal thickness (CCT) was not included in the diagnostic criteria because of its high variability with age and clinical stage. Patients were retrospectively included in the study if the attending physician diagnosed PNV according to the above diagnostic criteria and half-dose PDT combined with IVA was performed. All cases were confirmed to meet the diagnostic criteria by two independent retinal specialists (JT and HO) before inclusion in the study.
Half-dose PDT Combined with IVA
All patients were treated with half-dose PDT combined with IVA. Half-dose PDT was performed within a week after IVA. For the half-dose PDT, half of the standard dose of verteporfin (3 mg/m2, Visudyne; Clinigen K.K., Tokyo, Japan) was infused over 8 min, followed by a delivery of 689 nm diode laser for 10 min following a previously reported protocol [4]. The CVH containing the lesion with MNV was identified using middle phase ICGA, and set as the PDT spot. The total light energy used was 50 J/cm2. After the treatment, patients were instructed to avoid sunlight for 5 days. Patients were followed up every month after combined treatment, and if subretinal fluid (SRF) recurred or persisted, or if subretinal pigment epithelium fluid accumulated significantly, additional treatment with IVA monotherapy or half-dose PDT combined with IVA was performed.
Clinical measurements
Patients were categorized into the sufficient or insufficient group based on resolution or persistence/recurrence of SRF within six months after half-dose PDT combined with IVA, respectively, and clinical data were compared. Treatment efficacy was evaluated by two independent retina specialists (JT and HO) who were masked to the clinical course and patient ID to ensure concordant results. Age, sex, treatment history with anti-VEGF agents or PDT, BCVA, and axial length at baseline were collected from medical records. The CCT and PED height at baseline were measured manually using the caliper function of the built-in software of the OCT device. CCT was defined as the distance between the Bruch membrane and the choroid-sclera boundary at the fovea. PED height was defined as the maximum distance between the retinal pigment epithelium and the Bruch’s membrane in the PED containing the MNV. Macular 3 × 3 mm cubes scan patterns on OCTA, including 300 A-scans per 3 mm, were obtained at baseline and 6–9 months after the combined treatment to assess MNV size. The en-face images containing MNV were generated by adjusting the segmentation from the lower edge of the outer nuclear layer to the Bruch’s membrane for each eye and removing projection artifacts using the built-in software of OCTA. Then the MNV area was measured by manually selecting the MNV on the en-face images, using ImageJ software (ver. 1.8.0; National Institutes of Health, Bethesda, MD, USA).
Statistical analyses
All statistical analyses were performed with the SPSS (ver. 28.0.0.0; IBM Corp., Armonk, NY, USA), and the Shapiro–Wilk test was performed to test data normality. For comparisons between the two groups, the Student’s t-test, the Mann–Whitney U test, and the Wilcoxon signed-rank test were used depending on correspondence and whether the distribution was normal or not. The Fisher’s exact test or χ-squared test was used to analyze the contingency table. A multiple logistic regression analysis was also performed. Data were presented by the mean ± standard deviation, and all P values < 0.05 were considered statistically significant.
Results
From the 47 eyes of 47 patients with PNV, data from 4 eyes were excluded due to the low-quality OCT image or less than 6 months of follow-up. Therefore, data from 43 consecutive eyes of 43 patients with PNV (30 males and 13 females) were included. Of the 43 eyes included in the study, 8 eyes were diagnosed with CSC or PPE at the initial visit and subsequently developed MNV and the other 35 eyes had MNV detected from the initial visit. There were no cases of subretinal hemorrhage during the follow-up period, either before or after treatment. The patient characteristics are summarized in Table 1. The mean age of the patients was 62.0 ± 10.4 (range, 41–84) years, the mean BCVA (logMAR) at baseline was 0.15 ± 0.17 (range, 20/63–20/20), and the mean axial length was 23.7 ± 1.0 (range, 21.5–25.9) mm. A total of 21 of the 43 eyes (48.9%) had a history of previous treatment, either an intravitreal injection of anti-VEGF agents or a half-dose PDT. All eyes were treated with half-dose PDT combined with IVA and followed up for at least six months. Of 43 eyes, 25 eyes (58.1%) that were categorized in the sufficient group, achieved complete SRF resolution, and did not require any additional treatment during the six-month follow-up period. Notably, 18 eyes (41.9%) were categorized in the insufficient group, showed persistent or recurrent SRF, and required additional IVA monotherapy or half-dose PDT combined with IVA during the 6-month follow-up period. Although there was no significant difference in sex and axial length between the sufficient and insufficient groups (P = 0.100, P = 0.892, respectively), the mean age in the sufficient group (58.4 ± 10.2 years) was significantly younger than that in the insufficient group (66.9 ± 8.9 years, P = 0.006). Additionally, the mean baseline BCVA (logMAR) was significantly better in the sufficient group than in the insufficient group (0.09 ± 0.14, 0.23 ± 0.17, respectively, P = 0.004). Seven eyes (28.0%) in the sufficient group and fourteen eyes (77.8%) in the insufficient group had a history of previous treatment, and the difference was statistically significant (P = 0.001). The 25 eyes that achieved complete SRF resolution did not need any additional treatment after half-dose PDT combined with IVA up to 6 months after treatment (Table 2). When classified according to the presence or absence of previous treatment history, the percentage of the complete SRF resolution was 81.8% in treatment-naïve eyes, and only 33.3% in previously treated eyes, which was a significant difference (P = 0.001).
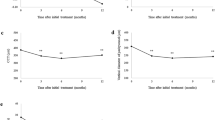
The OCT and OCTA findings at baseline were also analyzed and compared between the sufficient and insufficient groups (Fig. 1). There was no significant difference in the CCTs of the sufficient group and insufficient group (397.8 ± 152.7 μm, 361.9 ± 93.4 μm respectively, P = 0.346). Regarding the MNV morphology at baseline, the MNV sizes in the sufficient group were significantly smaller than those in the insufficient group (0.49 ± 0.55 mm2, 0.92 ± 0.88 mm2, respectively, P = 0.047). Although not significantly different, PED tended to be lower in the sufficient group than in the insufficient group (68.5 ± 63.2 μm, 74.2 ± 27.2 μm, respectively, P = 0.053).

Comparison of the central choroidal thickness (a), macular neovascularization (MNV) size at baseline (b), and pigment epithelial detachment (PED) height (c) between the sufficient group and insufficient group. * t-test, † Mann–Whitney U test
Logistic regression analysis was performed for four items that were significant in the univariate analysis: age, baseline BCVA, history of previous treatment, and baseline MNV size. The results showed that the outcome of half-dose PDT combined with IVA for PNV was significantly associated with age (OR = 1.09, 95% CI [1.004, 1.176], P = 0.040) and history of previous treatment (OR = 6.88, 95% CI [1.507, 31.400], P = 0.013). Baseline BCVA and baseline MNV size were not significantly associated with treatment outcome (P = 0.12, P = 0.51 respectively).
Of the total 43 eyes, OCTA was performed in 30 eyes, at baseline and 6–9 months after half-dose PDT combined with IVA. Thereafter, the changes in MNV size after half-dose PDT combined with IVA was evaluated. In total, 19 of the 30 eyes did not require additional treatment after the combined treatment, whereas 11 eyes required additional treatment with IVA monotherapy or half-dose PDT combined with IVA.
Figure 2 shows a representative case of the sufficient group, a 57-year-old woman with treatment-naïve PNV. Her baseline OCTA image showed MNV within a flat irregular PED just above the dilated outer choroidal vessels. The SRF disappeared within 1 month after half-dose PDT combined with IVA and did not recur during the 6-month follow-up. Nonetheless, 6 months after the treatment, the MNV size had enlarged by 27% compared to baseline.

Optical coherence tomography (OCT) and OCT angiography (OCTA) images of a representative case a 57-year-old female with treatment-naïve pachychoroid neovasculopathy in the sufficient group at baseline and six months post-treatment. En-face and B-scan OCTA images at baseline show macular neovasucularization (MNV) within a flat irregular pigment epithelial detachment (a, c). OCT image at baseline shows subretinal fluid (SRF) (b). Post-treatment en-face and B-scan OCTA images show enlarged MNV compared to baseline (d, f). Post-treatment OCT image showed no SRF (e) and no need for additional treatment
Figure 3 shows a representative case of the insufficient group, a 61-year-old man without any treatment history. His baseline OCTA images showed MNV with pachychoroid and the SRF recurred after combined treatment, requiring additional treatment with anti-VEGF agents. MNV maturation was not evident, but the MNV size significantly enlarged by 333.9% 6 months after treatment compared to baseline.

Optical coherence tomography (OCT) and OCT angiography (OCTA) images of a representative case of a 61-year-old male with treatment-naïve pachychoroid neovasculopathy in the insufficient group at baseline and six months post-treatment. En-face and B-scan OCTA images at baseline show small macular neovasucularization (MNV) size within flat irregular pigment epithelial detachment (a, c). OCT image at baseline showing subretinal fluid (SRF) (b). Post-treatment en-face and B-scan OCTA images showing enlarged MNV compared to baseline (d, f). Intravitreous aflibercept injection was added due to the residual SRF after combined treatment and OCT images six months after combined treatment showed no SRF (e)
Overall, the mean MNV size increased from 0.47 ± 0.45 mm2 at baseline to 0.69 ± 0.69 mm2 after half-dose PDT combined with IVA (46.8%, P = 0.003, Fig. 4a). However, there was no significant difference in the change in MNV size depending on whether additional treatment was required (P = 0.199, Fig. 4b).

Comparison of the macular neovascularization (MNV) size before and after treatment (a), and comparison of the change in MNV size with and without additional treatment (b). * Wilcoxon signed-rank test, † t-test
Discussion
In this study, complete SRF resolution was observed in 58.1% of the eyes with PNV treated with half-dose PDT combined with IVA at 6 months without additional treatment. Furthermore, this treatment response rate increased to 81.8% when restricted to treatment-naïve eyes.
Several variations of PDT combined with anti-VEGF therapy for treatment naïve PNV have been reported previously. Smretschnig et al. [16]. examined the treatment outcome of half-fluence PDT combined with an intravitreal injection of ranibizumab or bevacizumab for MNV in eyes with chronic CSC; 8 of 17 eyes (47%) did not require additional treatment during a 1-year follow-up. Kitajima et al. [11]. explored the efficacy of half-dose PDT combined with ranibizumab for PNV and reported that 6 of 11 eyes (55%) did not require additional treatment during a 1-year follow-up. Another study by Miki et al. [14]. found that when ranibizumab or aflibercept was combined with full-dose PDT for PNV eyes, most cases, 19 of 20 eyes (95%), required no additional therapy during the first year after treatment. Similar to the current study, Matsumoto et al. [13]. reported that the response rate at 1 year after half-dose PDT combined with IVA was 81% (17 of 21 eyes). These previously reported cases were in treatment-naïve eyes, and their outcome of PDT combined with anti-VEGF therapy was generally comparable to those of the treatment-naïve eyes in this study. PDT combined with anti-VEGF therapy is an effective treatment for treatment-naïve PNV. However, in this study, only one-third of the previously treated eyes with PNV did not require additional treatment for 6 months after half-dose PDT combined with IVA. Based on the above, previously treated PNV may be less effective and may have less benefit from half-dose PDT combined with IVA.
PNV is a condition in which chronic CSC or PPE is complicated by type 1 MNV, and it is speculated that ischemia of the choriocapillaris and dysfunction of the retinal pigment epithelium as a consequence of dilated outer choroidal vessels results in the formation of an abnormal vascular network [3, 17]. The pathogenesis of both chronic CSC and MNV leads to SRF accumulation. Since PNV is a chronic process, even with multimodal imaging such as OCT, OCTA, FAG and ICGA, it is difficult to clearly classify whether MNV or CVH is the cause of SRF in actual cases and it is likely that there is a mixture of both factors. Therefore, the concurrent use of anti-VEGF agents and PDT, which is effective in chronic CSC [4,5,6,7,8], may be a reasonable approach and effective treatment for PNV. Besides suppressing exudative changes from MNV, anti-VEGF drugs may also play a role in reducing inflammation that may be induced by PDT. In this study, the treatment response rate was significantly better for patients who were younger, had better baseline BCVA, no history of previous treatment with anti-VEGF agents or PDT, and small MNV size at baseline. Additionally, patients with lower PED height containing MNV tended to have higher treatment response rates. These results will help determine which cases should be considered for combination therapy. Progression proceeds from chronic CSC to PNV [18], and PNV has been shown to be in patients older in age and have poorer visual acuity than chronic CSC [19]. Additionally, MNV that develops in PNV is expected to expand over time, and the PED height may be related to MNV growth. Studies based on OCT findings indicate PNV has thinner CCT and lower choroidal vascularity index compared to CSC [20,21,22]. A comparison of cytokines in the aqueous humor showed that proinflammatory cytokines, interleukin-6 and interleukin-8 are decreased in PNV compared with chronic CSC, while angiogenic cytokines, VEGF-A and placental growth factor are increased in PNV [19]. These findings suggest that the pathophysiology of chronic CSC and PNV changes over time as MNV develops and gradually expands. Based on these findings, we consider the cases mostly included in the sufficient group in this study were those that still had strong characteristics of chronic CSC among the PNV. In the cases where MNV developed over time and the characteristics of chronic CSC weakened, it is possible that the main cause of SRD shifted from CVH to MNV, and that a single treatment of half-dose PDT with IVA was not sufficient to suppress the activity of MNV, thus additional treatment was necessary. This suggests that even when defining PNV as chronic CSC complicated by MNV, the treatment approach may need to be adjusted depending on the condition stage.
Previous studies have indicated that the use of conventional dose of verteporfin may induce MNV development in eyes with chronic CSC [23]. Decreased choroidal perfusion after PDT may increase the risk of MNV development by inducing choroidal ischemia [24, 25]. Thus, for safety reasons, PDT with the use of low doses of verteporfin or low laser power is widely used to treat chronic CSC. Chen et al. [26]. conducted a 3-year clinical course of 30 chronic CSC eyes with MNV (4 eyes were treated with anti-VEGF agents due to recurrent SRF but none received PDT). In those 30 eyes, the MNV area increase rate was approximately 1.4-folds. However, Hu et al. [27]. reported that MNV roughly doubled over 3 years after half-dose PDT in eyes with chronic CSC complicated by MNV. In this study, MNV also expanded six months after half-dose PDT combined with IVA regardless of treatment outcome, but the rate of expansion was only 1.47-folds. These results suggest that MNV may expand after conventional PDT and even after half-dose PDT, although the combination of anti-VEGF agents may reduce the rate of MNV expansion for at least six months after treatment. The MNV development with PNV is likely to be quiescent [20, 26], but the long-term course remains unclear, and continuous follow-up is necessary even when exudative change has subsided after treatment.
The study limitations include the short observation period, retrospective study design, lack of data on the natural history, and lack of comparison with other treatment methods, including half-dose/full-dose PDT combined with another anti-VEGF other than aflibercept, half-dose/full-dose PDT alone or anti-VEGF alone.
In conclusion, half-dose PDT combined with IVA was an effective treatment for PNV, especially for younger patients with good baseline BCVA, treatment-naïve eyes, and small baseline MNV size. MNV expanded after half-dose PDT combined with IVA regardless of treatment outcome, although the expansion rate may have been controlled. An extended study to search for an optimal treatment considering the clinical stages of PNV is warranted.
References
Cheung CMG, Lee WK, Koizumi H, Dansingani K, Lai TYY, Freund KB (2019) Pachychoroid disease. Eye (Lond) 33:14–33. https://doi.org/10.1038/s41433-018-0158-4
Yanagi Y (2020) Pachychoroid disease: a new perspective on exudative maculopathy. Jpn J Ophthalmol 64:323–337. https://doi.org/10.1007/s10384-020-00740-5
Pang CE, Freund KB (2015) Pachychoroid neovasculopathy. Retina 35:1–9. https://doi.org/10.1097/IAE.0000000000000331
Chan WM, Lai TYY, Lai RYK, Tang EWH, Liu DTL, Lam DSC (2008) Safety enhanced photodynamic therapy for chronic central serous chorioretinopathy: one-year results of a prospective study. Retina 28:85–93. https://doi.org/10.1097/IAE.0b013e318156777f
Fujita K, Imamura Y, Shinoda K, Matsumoto CS, Mizutani Y, Hashizume K, Mizota A, Yuzawa M (2015) One-year outcomes with half-dose verteporfin photodynamic therapy for chronic central serous chorioretinopathy. Ophthalmology 122:555–561. https://doi.org/10.1016/j.ophtha.2014.09.034
Haga F, Maruko R, Sato C, Kataoka K, Ito Y, Terasaki H (2017) Long-term prognostic factors of chronic central serous chorioretinopathy after half-dose photodynamic therapy: a 3-year follow-up study. PLOS One 12:e0181479. https://doi.org/10.1371/journal.pone.0181479
Lai TYY, Chan WM, Li H, Lai RKL, Liu DTL, Lam DSC (2006) Safety enhanced photodynamic therapy with half dose verteporfin for chronic central serous chorioretinopathy: a short term pilot study. Br J Ophthalmol 90:869–874. https://doi.org/10.1136/bjo.2006.090282
Oiwa K, Kataoka K, Maruko R, Ueno S, Ito Y, Terasaki H (2017) Half-dose photodynamic therapy for chronic central serous chorioretinopathy evaluated by focal macular electroretinograms. Jpn J Ophthalmol 61:260–266. https://doi.org/10.1007/s10384-017-0498-9
Guo J, Tang W, Xu S, Liu W, Xu G (2021) OCTA evaluation of treatment-naïve flat irregular PED (FIPED)-associated CNV in chronic central serous chorioretinopathy before and after half-dose PDT. Eye (Lond) 35:2871–2878. https://doi.org/10.1038/s41433-020-01345-5
Hikichi T, Kubo N, Yamauchi M (2021) One-year comparison of anti-vascular endothelial growth factor and half-dose photodynamic therapies for pachychoroid neovasculopathy. Eye (Lond) 35:3367–3375. https://doi.org/10.1038/s41433-021-01418-z
Kitajima Y, Maruyama-Inoue M, Ito A, Sato S, Inoue T, Yamane S, Kadonosono K (2020) One-year outcome of combination therapy with intravitreal anti-vascular endothelial growth factor and photodynamic therapy in patients with pachychoroid neovasculopathy. Graefes Arch Clin Exp Ophthalmol 258:1279–1285. https://doi.org/10.1007/s00417-020-04661-4
Matsumoto H, Hiroe T, Morimoto M, Mimura K, Ito A, Akiyama H (2018) Efficacy of treat-and-extend regimen with aflibercept for pachychoroid neovasculopathy and type 1 neovascular age-related macular degeneration. Jpn J Ophthalmol 62:144–150. https://doi.org/10.1007/s10384-018-0562-0
Matsumoto H, Mukai R, Kikuchi Y, Morimoto M, Akiyama H (2020) One-year outcomes of half-fluence photodynamic therapy combined with intravitreal injection of aflibercept for pachychoroid neovasculopathy without polypoidal lesions. Jpn J Ophthalmol 64:203–209. https://doi.org/10.1007/s10384-020-00722-7
Miki A, Kusuhara S, Otsuji T, Kawashima Y, Miki K, Imai H, Nakamura M, Tsujikawa A (2021) Photodynamic therapy combined with anti-vascular endothelial growth factor therapy for pachychoroid neovasculopathy. PloS One 16:e0248760. https://doi.org/10.1371/journal.pone.0248760
Tanaka K, Mori R, Wakatsuki Y, Onoe H, Kawamura A, Nakashizuka H (2021) Two-thirds dose photodynamic therapy for pachychoroid neovasculopathy. J Clin Med 10:2168. https://doi.org/10.3390/jcm10102168
Smretschnig E, Hagen S, Glittenberg C, Ristl R, Krebs I, Binder S, Ansari-Shahrezaei S (2016) Intravitreal anti-vascular endothelial growth factor combined with half-fluence photodynamic therapy for choroidal neovascularization in chronic central serous chorioretinopathy. Eye (Lond) 30:805–811
Dansingani KK, Balaratnasingam C, Klufas MA, Sarraf D, Freund KB (2015) Optical coherence tomography angiography of shallow irregular pigment epithelial detachments in pachychoroid spectrum disease. Am J Ophthalmol 160:1243-1254e.2. https://doi.org/10.1016/j.ajo.2015.08.028
Fung AT, Yannuzzi LA, Freund KB (2012) Type 1 (sub-retinal pigment epithelial) neovascularization in central serous chorioretinopathy masquerading as neovascular age-related macular degeneration. Retina 32:1829–1837. https://doi.org/10.1097/IAE.0b013e3182680a66
Terao N, Koizumi H, Kojima K et al (2018) Association of upregulated angiogenic cytokines with choroidal abnormalities in chronic central serous chorioretinopathy. Invest Ophthalmol Vis Sci 59:5924–5931. https://doi.org/10.1167/iovs.18-25517
Guo J, Tang W, Liu W, Chang Q, Xu G (2021) Clinical features of flat irregular pigment epithelial detachment associated with choroidal neovascularization in chronic central serous chorioretinopathy. Retina 41:199–207. https://doi.org/10.1097/IAE.0000000000002791
Demirel S, Yanık Ö, Özcan G, Batıoğlu F, Özmert E (2021) A comparative study on the choroidal vascularity index and the determination of cut-off values in the pachychoroid spectrum diseases. Jpn J Ophthalmol 65:482–491. https://doi.org/10.1007/s10384-021-00829-5
Wu JS, Chen SN (2019) Optical coherence tomography angiography for diagnosis of choroidal neovascularization in chronic central serous chorioretinopathy after photodynamic therapy. Sci Rep 9:9040. https://doi.org/10.1038/s41598-019-45080-8
Erikitola OC, Crosby-Nwaobi R, Lotery AJ, Sivaprasad S (2014) Photodynamic therapy for central serous chorioretinopathy. Eye (Lond) 28:944–957. https://doi.org/10.1038/eye.2014.134
Turkcuoglu P, Ilhan N, Kurt J, Aydemir O, Celiker U (2009) The protective role of Visudyne eyeglass against VEGF synthesis after photodynamic therapy with verteporfin. Acta Ophthalmol 87:871–874. https://doi.org/10.1111/j.1755-3768.2008.01368.x
Colucciello M (2006) Choroidal neovascularization complicating photodynamic therapy for central serous retinopathy. Retina 26:239–242
Chen YC, Chen SN (2020) Three-year follow-up of choroidal neovascularisation in eyes of chronic central serous chorioretinopathy. Br J Ophthalmol 104:1561–1566. https://doi.org/10.1136/bjophthalmol-2019-315302
Hu YC, Chen YL, Chen YC, Chen SN (2021) 3-year follow-up of half-dose verteporfin photodynamic therapy for central serous chorioretinopathy with OCT-angiography detected choroidal neovascularization. Sci Rep 11:13286. https://doi.org/10.1038/s41598-021-92693-z
Acknowledgements
This work was supported by the Japan Society for the Promotion of Science, KAKENHI, (grant number: JP 18K16953).
Funding
The authors did not receive financial support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Jun Takeuchi, Hikaru Ota, Yuyako Nakano, Etsuyo Horiguchi, Yosuke Taki and Keiko Kataoka. The first draft of the manuscript was written by Jun Takeuchi and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This retrospective study involving human participants was in accordance with the ethical standards of the institutional and national research committee, and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Institutional Review Board of the Nagoya University Graduate School of Medicine (2021–0339) and Kyorin University Graduate School of Medicine (1903 approved this study.
Conflicts of interest
Hiroko Terasaki received non-financial research support from Carl Zeiss related to OCT angiography. Jun Takeuchi received honoraria for lectures from Novartis, Santen, Bayer, Senju, and Chugai. Hikaru Ota received honoraria for lectures from Novartis. Yasuki Ito received honoraria for lectures from Aichi Ophthalmologists Association, Bayer, Canon, ZEISS, Kowa, Novartis, Okazaki City Medical Association, Pfizer, and Santen. Hiroko Terasaki received grants and honoraria for lectures from Otsuka, Kowa, Santen, Senju, Sanofi, Alcon, Novartis, ROHTO, Wakamoto. She received grants and consulting fees from Bayer and honoraria for lectures from HOYA and Johnson & Johnson. Koji M Nishiguchi received grants from Takara bio, Takeda pharmaceutical, JCR Pharma, Alcon, and Bayer, and honoraria for lectures from Novartis, Santen, Chugai Pharma, Kowa, Senju, Otsuka, and Wakamoto. He has a patent related to a single AAV vector. Keiko Kataoka received honoraria for lectures from Chugai, Novartis, Santen, Bayer, Senju, Boehringer Ingelheim, and Otsuka. The other authors have no conflicting interests to disclose.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Takeuchi, J., Ota, H., Nakano, Y. et al. Predictive factors for outcomes of half-dose photodynamic therapy combined with aflibercept for pachychoroid neovasculopathy. Graefes Arch Clin Exp Ophthalmol 261, 2235–2243 (2023). https://doi.org/10.1007/s00417-023-06030-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-023-06030-3