
Abstract
Purpose
To explore the relationship between the bleb vasculature and surgical outcome after trabeculectomy (TRAB) using optical coherence tomography angiography (OCT-A).
Methods
A prospective study was conducted, which included 26 eyes of 26 primary glaucoma patients in the final analysis. Thereinto, six patients underwent TRAB combined 5-FU and 12 patients received subconjunctival 5-FU injection postoperation. The bleb vessel was evaluated using OCT-A 1 week, 2 weeks, 1 month, 3 months, and 6 months after TRAB. Intraocular pressure (IOP), filtering bleb height, and bleb wall thickness were recorded at the same time. Pearson’s correlation analysis and linear regression analysis were performed to determine the correlation of the vessel area data with other parameters.
Results
Compared with vessel area 1 week after surgery, there was significant increase of the vessel area (△vessel area) 2 weeks (11.13 ± 11.91%, p < 0.05) and 1 month (16.91 ± 14.85%, p < 0.0001) after surgery in all patients. The △vessel area was significantly greater in acute angle closure (AAC) and primary angle closure glaucoma (PACG) 1-month post-TRAB as compared with that 1 week (p < 0.05). The results indicated that the △vessel area 1-month post-TRAB was positive correlated with IOP 6-month post-TRAB (β = 3.88, p = 0.042).
Conclusions
Filtering bleb vascularization evaluation using OCT-A could potentially predict IOP 6-month post-TRAB. Surgery effect predicted by filtering bleb vascularization detection is conducive to the select specific postoperative intervention to improve the success rate of TRAB.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Scarring in the surgical area is a common cause of failure of trabeculectomy (TRAB) [1]. An advanced treatment modality is required that can minimize fibrosis and result in better outcomes than TRAB.
Angiogenesis accompanies scar formation [2, 3] and vessels within scars are thought to play a crucial role in surgical incision healing. A previous study demonstrated that the response of vessels to trauma was a key factor in scar development [4]. Research also showed that scar stability did not occur until at least 6 months after surgery [5].
The Indiana Bleb Appearance Grading Scale (IBAGS) and Moorfields Bleb Grading System (MBGS) have long been used to analyze the vascularity of filtering blebs in glaucoma patients [6, 7]. However, these assessment methods are partly subjective. A new technology, optical coherence tomography angiography (OCT-A), can detect blood flow of ocular tissue rapidly and non-invasively [8,9,10]. Evidence is emerging that OCT-A provide a means of detecting the vessel area of the ocular anterior segment.
The aim of the present study was to examine the correlation of the vessel area in the operative region with surgical outcomes post-TRAB using OCT-A.
Methods
Study design
This was a prospective study of 49 eyes of 46 consecutive subjects with primary glaucoma who visited The First Affiliated Hospital of Soochow University from June 2017 to Feb 2018, and 26 eyes of 26 patients who had undergone TRAB were included finally. This study was approved by the ethics review board of The First Affiliated Hospital of Soochow University and abided by the tenets of the Declaration of Helsinki. All subjects were encouraged to sign informed consent forms.
Subjects
In all patients enrolled in this study, best corrected visual acuity (BCVA) in LogMAR, IOP, and center corneal thickness (CCT) was measured. In addition, data were obtained on the patients’ medical histories, systematic disease histories, premedication duration/kinds, TRAB combined 5-fluorouracil (5-FU), and postoperative 5-FU subconjunctival injection (Table 1). The inclusion criteria and exclusion criteria were as follows: Inclusion criteria: (1) Patients with primary glaucoma; (2) IOP was not adequately controlled with maximal tolerated medical therapy; (3) With advanced glaucomatous visual field defects and the presence of an advanced glaucomatous optic disc cupping; (4) No prior history of conjunctival injury or surgery; (5) No prior history of TRAB in the past 6 months; (6) No other ocular disease or surgery. Exclusion criteria: (1) With postoperative bleb massage or bleb needlings; (2) With usage of ocular hypotensive agents after surgery; (3) With postoperative conjunctival hemorrhage; (4) With severe surgery complications such as hyphema, malignant glaucoma, entophthalmia, and so on.
Surgical technique
The same glaucoma specialist (QC) performed all the fornix-based bleb TRAB surgery. A 3 × 4-mm square scleral flap was made which was dissected into the two thirds scleral depth. Then the 5-FU (25 mg/mL, SunRise, Shang Hai, China) was applied for 3 min in a soaked cotton fleece and irrigated with 100 mL of balanced salt solution (it was not conducted in the older patients with thin conjunctival tissue). The excision of a block of trabecular meshwork tissue was performed followed by peripheral iridectomy. The scleral flap was sewed up with four 10–0 nylon sutures. The conjunctiva was closed with 8–0 Vicryl sutures and secured at the limbus by interrupted sutures.
After the surgery, the TRAB patients were prescribed Tobradex (Alcon, USA) every 2 h in daytime, 2.5 g of Pranopulin (Senju Pharmaceutical Co., Fukusaki, Japan) Qid, and 25 mg of atropine sulfate ophthalmic gel solution (Xing Qi, Shen Yang, China) every night. The Tobradex dosage was tapered to Qid 3 days after surgery. Three-month post-surgery, all drugs were ceased.
In this study, all patients had undergone laser suture lysis for only one suture on the angle of scleral flap around 2 weeks after surgery. If laser suture lysis did not work successfully (IOP < 14 mmHg), 5-FU subconjunctival injection was conducted merely, and the patients who underwent bleb massage or 5-FU subconjunctival injection combined needle revision were not included in the final analysis.
OCT data acquisition and processing
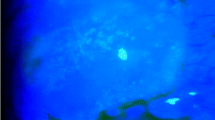
The masked doctor (XY and RS) examined bleb vessel and morphology parameters (bleb height and bleb wall thickness) in all patients with 1-week, 2-week, 1-month, 3-month, and 6-month post-TRAB. OCT-A (Optovue, Fremont, CA, USA) scanning (6 × 6-mm HD Angio Retina protocol) was performed to detect the vessel density of the filtering bleb region 1-week, 2-week, 1-month, 3-month, and 6-month post-TRAB (Fig. 1d). The investigation depth of OCT-A was 2.0 mm. The vessel data from scanning laser ophthalmoscope (SLO) pattern OCT-A images were edited using Image ProPlus, version 6.0 (Media Cybernetics, USA) by Doctor XY. The vessels were drawn for three times, and the mean value average was obtained by calculating the results of three measurements. The vessel area 1-week post-TRAB was set as the baseline for each subject. The scanned site was focused according to the initial detection (Fig. 1a, b). Bleb morphology was determined by anterior-segment OCT (AS-OCT), using the corneal cross-line protocol. The filtering bleb height and bleb wall thickness were measured, as shown in Fig. 1c. To avoid the effects of IOP fluctuation, all measurements were obtained from 9:00 to 11:00 AM. In this study, the measurement was performed for three times, and the tonometer was calibrated before use.

Ocular anterior-segment image of a 66-year-old female AAC patient 2 weeks after TRAB. a Slit-lamp anterior-segment photography of a filtering bleb. The black dotted line indicates the location imaged by OCT-A. b Bleb morphology was scanned using the corneal cross-line protocol. The crossing focused on the center of the scleral flap. c Representative vertical cross-sectional image, showing bleb height (H), bleb wall thickness (T), and sclera lake (*). d OCT-A scan (6 × 6-mm HD Angio Retina protocol) of a filtering bleb (left superior image). The right superior image was taken automatically by OCT-A. The inferior image is the corresponding horizontal sectional image. e Time-dependent kinetic changes of bleb vessels in 26 eyes of 26 patients, as detected by OCT-A. The change rate of the vessel area in all eyes significantly increased 2 weeks and 1 month after TRAB (one-way ANOVA, *p < 0.05, ***p < 0.0001). W, week; M, month. The data are presented as the mean ± SD
Statistical analysis
The statistical package SPSS 17.0 (SPSS, CA, USA) was used to analyze the data. Differences between groups were analyzed using an unpaired t test or a one-way analysis of variance (ANOVA). For comparisons of the △vessel area data and parameters of the patients, Pearson’s correlation analysis and univariate and multivariate linear regression analyses were performed. A p value < 0.05 was considered statistically significant.
Results
Forty-eight eyes of 46 patients undergone trabeculectomy in this study, and 26 patients with glaucoma were followed up for 6 months after TRAB without violation of inclusion criteria. The subjects comprised 12 males and 14 females aged 56.04 ± 15.67 years. There were 11 eyes with acute angle closure (AAC), 11 eyes with primary angle closure glaucoma (PACG) and 4 eyes with primary open angle glaucoma (POAG). IOP was measured using Goldman tonometry. The mean pre-operative IOP was 29.99 ± 14.66 mmHg. The postoperative IOP was 12.69 ± 4.067 mmHg after 1 week, 12.92 ± 3.687 mmHg after 2 weeks, 14.08 ± 2.841 mmHg after 1 month, 13.54 ± 2.453 mmHg after 3 months, and 13.73 ± 2.92 mmHg after 6 months. The mean CCT was 537.5 ± 18.25 μm, and the mean BCVA in LogMAR 1 day before surgery was 0.5788 ± 0.6132.
Figure 1 shows the results of OCT-A 6 × 6-mm HD retinal scanning of the filtering bleb and surrounding zone. After selecting the maximum overlap area of five time-point images, we analyzed the difference between the reset new images. The vessel area 1-week post-TRAB was designated as zero. In all 26 eyes, 2 weeks, 1 month, 3 months, and 6 months after surgery, the △vessel area was 11.13 ± 11.91, 16.91 ± 14.85, 4.722 ± 14.2, and − 4.701 ± 17.8%, respectively. The △vessel area was significantly increased 2-week and 1-month post-TRAB (p < 0.0001) (Fig. 1e). In AAC group (Fig. 2a–f), 2-week, 1-month, 3-month, and 6-month post-surgery, the △vessel area was 11.82 ± 7.885, 12.88 ± 14.34, 6.543 ± 9.427, and 1.777 ± 15.73%, respectively. The △vessel area was significantly increased after 1 month (p = 0.0318). In PACG group (Fig. 2g–l), the △vessel area was 10.44 ± 11.72, 24.02 ± 15.03, 9.499 ± 10.81, and − 4.002 ± 14.15% at the 2-week, 1-month, 3-month, and 6-month follow-ups, respectively. The △vessel area was significantly increased at the 1-month follow-up (p < 0.0001). Comparison of ocular-related parameters in the glaucoma groups 1-month and 6-month post-surgery revealed that the △vessel area was greater in POAG group than in the AAC and PACG groups 6 months after surgery (p = 0.0374). There were no significant differences between the groups in gender, age, pre-operative medications kinds, pre-operative medications duration, pre-operative prostaglandin (PG), systemic disease, pre-operative BCVA, pre-operative IOP, TRAB combined 5-FU, and subconjunctival 5-FU injection postoperative (Table 1).

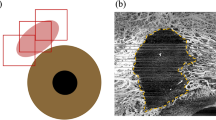
Time kinetic bleb vessel detected by OCT-A of AAC and PACG. a–e An example case of an AAC patient. Five images scanned by OCT-A 1 week, 2 weeks, 1 month, 3 months, and 6 months after TRAB, respectively. f The change rate in the vessel area increased significantly 1-month post-TRAB, as analyzed by a one-way ANOVA (*p < 0.05). g–k An example case of a PACG patient. Five images scanned by OCT-A in 1 week, 2 weeks, 1 month, 3 months, and 6 months after TRAB, respectively. l The change rate of vessel area increased significantly 1-month post-TRAB, as analyzed by a one-way ANOVA (***p < 0.0001). The data are presented as the mean ± SD
The results of the linear regression analysis revealed a significant association between the △vessel area 1-month post-TRAB and IOP 6 months after TRAB (β = 3.88, p = 0.042, Table 2). Pearson’s correlation analysis confirmed the correlation (r2 = 0.3558, p = 0.0013, Fig. 3). There was no correlation between the △vessel area and other factors such as gender, age, pre-operative medications kinds, pre-operative medications duration, pre-operative PG, systemic disease, central corneal thickness (CCT), pre-operative BCVA, pre-operative IOP, surgery frequency, TRAB combined 5-FU, and subconjunctival 5-FU injection postoperative (Table 2).

Scatter plots illustrating the linear correlation between postoperative IOP and △vessel area (%) 1 month after TRAB. a, b There was no correlation between the △vessel area 1-month postoperatively and IOP 1 and 3-month postoperatively. c △Vessel area 1-month postoperatively correlated to the 6-month postoperative IOP (y = 0.1173x + 11.748, r2 = 0.3558, p = 0.0013)
Discussion
OCT-A is widely applied to scan blood vessels and determine the choroidal neovascularization area in age-related macular degeneration patients. In the clinic, IBAGS and MBGS are employed to determine the vascularity of filtering blebs in glaucoma patients, with surface vessel visibility assessed in a slit-lamp examination [6, 7]. The advantages of OCT-A are that it can detect blood flow of orbital tissue simply, rapidly, reproducibly, and non-invasively. In addition, OCT-A can detect blood flow not visible with a slit lamp. Furthermore, OCT-A has an investigation depth of 2.0 mm. OCT-A is also a noncontact method, unlike ultrasound biomicroscopy. Therefore, it does not come into direct contact with the filtering bleb. The use of OCT-A in the detection of blood flow in various areas, such as the optical disc, iris, and burn scar tissue, is supported by the literature [11,12,13]. The findings of the present study suggest that OCT-A can provide a quantitative assessment method of the blood flow of a filtering bleb after TRAB. A quantitative measurement may aid assessments of vessels of filtering blebs.
IOP is the most frequently used evaluation index of the effect of antiglaucoma surgery [1, 14, 15]. More significantly, for the first time, this study revealed that an association between the vessel area 1-month post-TRAB and IOP after 6 months. Previous research demonstrated the applicability of OCT studies to detect bleb morphology and IOP. Narita and Kawana reported that a tall bleb, with a thick hypo-reflective wall seemed to be a feature of a well-functioning bleb [16, 17]. In the current study, we assumed that bleb height and bleb wall thickness do not directly related to the △vessel area. A previous study suggested that avascular and white tissue represented scar formation following skin burns [18]. On the contrary, the ophthalmic literature suggests that flatter, more diffuse, and avascular blebs can successfully lower the postoperative IOP [19, 20].
To the best of our knowledge, TRAB is considered the gold standard for antiglaucoma surgeries. Scar formation in the operative region, especially between the Tenon capsules and sclera flap is the leading cause of failure in TRAB [21]. The literature provides considerable evidence for a close relationship between vascularization and scar formation [22]. Inflammation is an important factor in promoting vascularization, thus caused further scar formation. Nadella et al. showed that macrophages migrated into wounds and that new vessels formed in the early phases of healing [23]. The same study demonstrated that inflammation was the initial factor underlying the development of vascularization, which was significant in established scars. In contrast, Meziani et al. found no significant difference in vascularization between functioning blebs and nonfunctioning blebs [24]. They performed en-face AS-OCT 1.25 to 108 months after filtration surgery. In contrast, we used OCT-A to detect time-dependent changes in kinetics of vessels from 1 week to 6 months after surgery. In the present study, the △vessel area 1-month post-TRAB exhibited the greatest increase in density. The △vessel area was correlated with IOP 6-month post-surgery but not with IOP 1-month or 3-month post-surgery. We hypothesized that the △vessel area peak was associated with subsequent scar formation in the operative area. Our finding is consistent with that of previous studies, which demonstrated an absence of vascularization in the filtration surgery area by in vivo confocal microscopy and showed that this was correlated with a good functioning bleb [25]. Our data suggest that the rate of change in the vessel density in and around the filtering bleb 1 month after surgery, at least partly, is a strong prognostic indicator of the effect of TRAB surgery.
Some researchers also speculated that TRAB combined with 5-FU helped to reduce blood vessel density and lower the IOP [26]. But we found no difference in the blood vessel density of patients treated with 5-FU intra- or post-surgery. We hypothesized that the increase in blood vessels was less pronounced for the use of 5-FU. But for ethical reasons, we cannot abandon treating the postoperative high IOP patients in clinic. To eliminate drug interference in the outcome, patients with post-TRAB ocular hypotensive agents were excluded finally. We cannot get the data in failure group for the moment. In addition, the possibility that the small sample size gave rise to the significant difference cannot be ruled out, and the reliability of the finding should be confirmed in a larger sample.
Our results demonstrate that vascularization of a filtering bleb detected by OCT-A could be used for predicting surgery effect to some extent. By predicting filtering bleb functioning using OCT-A, specific treatments, such as subconjunctival 5-FU injection, could be developed to enhance success rates of TRAB.
References
Landers J, Martin K, Sarkies N et al (2012) A twenty-year follow-up study of trabeculectomy: risk factors and outcomes. Ophthalmology 119:694–702
Beer TW, Baldwin HC, Goddard JR et al (1998) Angiogenesis in pathological and surgical scars. Hum Pathol 29:1273–1278
Shaunak S, Thomas S, Gianasi E et al (2004) Polyvalent dendrimer glucosamine conjugates prevent scar tissue formation. Nat Biotechnol 22(8):977–984
Brown NJ, Smyth EA, Cross SS (2002) Angiogenesis induction and regression in human surgical wounds. Wound Repair Regen 10:245–251
Zhang Z, Nie F, Chen X et al (2015) Upregulated periostin promotes angiogenesis in keloids through activation of the ERK 1/2 and focal adhesion kinase pathways, as well as the upregulated expression of VEGF and angiopoietin-1. Mol Med Rep 11:857–864
Cantor LB, Mantravadi A, WuDunn D et al (2003) Morphologic classification of filtering blebs after glaucoma filtration surgery: the Indiana bleb appearance grading scale. J Glaucoma 12:266–271
Wells AP, Crowston JG, Marks J et al (2004) A pilot study of a system for grading of drainage blebs after glaucoma surgery. J Glaucoma 13:454–460
Shields MV, Welch RJ, Say EAT (2017) Cilioretinal artery imaged with optical coherence tomography angiography. Ophthalmology 124:1448
Richter GM (2017) The promise of optical coherence tomography angiography in glaucoma. Ophthalmology 124:1577–1578
Lommatzsch C, Rothaus K, Koch JM et al (2018) OCTA vessel density changes in the macular zone in glaucomatous eyes. Graefes Arch Clin Exp Ophthalmol 256(8):1499–1508
Skalet AH, Li Y, Lu CD et al (2017) Optical coherence tomography angiography characteristics of Iris melanocytic tumors. Ophthalmology 124:197–204
Kang AS, Welch RJ, Sioufi K et al (2017) Optical coherence tomography angiography of iris microhemangiomatosis. Am J Ophthalmol Case Rep 6:24–26
Gong P, Es'haghian S, Harms KA et al (2016) In vivo label-free lymphangiography of cutaneous lymphatic vessels in human burn scars using optical coherence tomography. Biomed Opt Express 7:4886–4898
Romero P, Hirunpatravong P, Alizadeh R et al (2018) Trabeculectomy with mitomycin-C: outcomes and risk factors for failure in primary angle-closure glaucoma. J Glaucoma 27:101–107
Jampel HD, Solus JF, Tracey PA et al (2012) Outcomes and bleb-related complications of trabeculectomy. Ophthalmology 119:712–722
Narita A, Morizane Y, Miyake T et al (2017) Characteristics of early filtering blebs that predict successful trabeculectomy identified via three-dimensional anterior segment optical coherence tomography. Br J Ophthalmol. https://doi.org/10.1136/bjophthalmol-2017-310707
Kawana K, Kiuchi T, Yasuno Y, Oshika T (2009) Evaluation of trabeculectomy blebs using 3-dimensional cornea and anterior segment optical coherence tomography. Ophthalmology 116(5):848–855
Huggenberger R, Detmar M (2011) The cutaneous vascular system in chronic skin inflammation. J Investig Dermatol Symp Proc 15(1):24–32
Khaw PT, Chang L, Wong TT et al (2001) Modulation of wound healing after glaucoma surgery. Curr Opin Ophthalmol 12:143–148
Kasaragod D, Fukuda S, Ueno Y et al (2016) Objective evaluation of functionality of filtering bleb based on polarization-sensitive optical coherence tomography. Invest Ophthalmol Vis Sci 57:2305–2310
Palanca-Capistrano AM, Hall J, Cantor LB et al (2009) Long-term outcomes of intraoperative 5-fluorouracil versus intraoperative mitomycin C in primary trabeculectomy surgery. Ophthalmology 116:185–190
Amadeu T, Braune A, Mandarim-de-Lacerda C et al (2003) Vascularization pattern in hypertrophic scars and keloids: a stereological analysis. Pathol Res Pract 199:469–473
Nadella V, Mohanty A, Sharma L et al (2018) Inhibitors of apoptosis protein antagonists (Smac mimetic compounds) control polarization of macrophages during microbial challenge and sterile inflammatory responses. Front Immunol 8:1792. https://doi.org/10.3389/fimmu
Meziani L, Tahiri Joutei Hassani R, El Sanharawi M et al (2016) Evaluation of blebs after filtering surgery with En-face anterior-segment optical coherence tomography: a pilot study. J Glaucoma 25:e550–e558
Caglar C, Karpuzoglu N, Batur M, Yasar T (2016) In vivo microscopy and biomicroscopy of filtering blebs after trabeculectomy. J Glaucoma 25:e377–e383
Broadway DC, Bloom PA, Bunce C et al (2004) Needle revision of failing and failed trabeculectomy blebs with adjunctive 5-fluorouracil: survival analysis. Ophthalmology 111:665–673
Funding
This research was supported by Jiangsu Provincial Medical Innovation Team (No. CXTDA2017039) and the Soochow Scholar Project of Soochow University (No. R5122001) to P Lu.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
This study was approved by the ethics review board of The First Affiliated Hospital of Soochow University and abided by the tenets of the Declaration of Helsinki (clinical trial registration number: ChiCTR1800014446).
Informed consent
All subjects were encouraged to sign informed consent forms.
Rights and permissions
About this article

Cite this article
Yin, X., Cai, Q., Song, R. et al. Relationship between filtering bleb vascularization and surgical outcomes after trabeculectomy: an optical coherence tomography angiography study. Graefes Arch Clin Exp Ophthalmol 256, 2399–2405 (2018). https://doi.org/10.1007/s00417-018-4136-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-018-4136-0