
Abstract
Purpose
To evaluate the improvement in targeted reaching movements toward targets of various contrasts in a patient implanted with a suprachoroidal–transretinal stimulation (STS) retinal prosthesis.
Methods
An STS retinal prosthesis was implanted in the right eye of a 42-year-old man with advanced Stargardt disease (visual acuity: right eye, light perception; left eye, hand motion). In localization tests during the 1-year follow-up period, the patient attempted to touch the center of a white square target (visual angle, 10°; contrast, 96, 85, or 74%) displayed at a random position on a monitor. The distance between the touched point and the center of the target (the absolute deviation) was averaged over 20 trials with the STS system on or off.
Results
With the left eye occluded, the absolute deviation was not consistently lower with the system on than off for high-contrast (96%) targets, but was consistently lower with the system on for low-contrast (74%) targets. With both eyes open, the absolute deviation was consistently lower with the system on than off for 85%-contrast targets. With the system on and 96%-contrast targets, we detected a shorter response time while covering the right eye, which was being implanted with the STS, compared to covering the left eye (2.41 ± 2.52 vs 8.45 ± 3.78 s, p < 0.01).
Conclusions
Performance of a reaching movement improved in a patient with an STS retinal prosthesis implanted in an eye with residual natural vision. Patients with a retinal prosthesis may be able to improve their visual performance by using both artificial vision and their residual natural vision.
Clinical trial registration
Beginning date of the trial: Feb. 20, 2014
Date of registration: Jan. 4, 2014
Trial registration number: UMIN000012754
Registration site: UMIN Clinical Trials Registry (UMIN-CTR)
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The vision of patients with hereditary retinal dystrophies such as retinitis pigmentosa slowly degrades, possibly leading to total blindness. Since there is no established therapy for these diseases, several preclinical and clinical trials have been undertaken with the aim of recovering vision [1].
Artificial vision is one of the most promising methods for the recovery of vision; this involves implanting a device in the visual pathway at some point between the retina and visual cortex and stimulating neurons electrically. Among these devices, retinal prostheses that stimulate the retina electrically have been the most actively investigated. There are three types of retinal prosthesis, classified according to the position where the electrodes are inserted: epiretinal prostheses [2, 3], subretinal prostheses [4,5,6], and suprachoroidal prostheses [7,8,9]. These prostheses have been shown to recover the vision of blind patients, although to a visual acuity which does not greatly exceed counting fingers generally regarding retinitis pigmentosa [10].
To further improve retinal prostheses, being able to appropriately evaluate the visual function of patients with ultra-low vision is important. However, this is difficult to judge on the basis of visual acuity alone [11,12,13]; functional vision tests are therefore needed to evaluate the residual vision in these patients [14]. The “square localization” test is a test of functional vision developed by the Argus II group to evaluate their retinal prosthesis [15]. In this test, the subject is instructed to point to a displayed target and the distance is measured between the center of the target and the position to which the subject is pointing. The test evaluates not only the ability to detect the position of localized light, but also eye–hand coordination. The use of an Argus II retinal prosthesis was shown to reduce the deviation in square localization [16]. We used a localization test based on square localization to examine targeted reaching movements in subjects with simulated ultra-low vision, but found no significant correlation between the amount of deviation and visual acuity [17]. This result suggests that a functional vision test such as square localization may also reflect visual ability other than visual acuity. This visual ability is probably affected by many factors such as visual contrast sensitivity, size of the visual field, age, duration of the vision reduction, and so on.
The inclusion criteria for patients in the trial of Argus II retinal prostheses included vision at bare light perception or less, in which localized light cannot be identified. In contrast, patients eligible for suprachoroidal–transretinal stimulation (STS) retinal prostheses include those with “hand motion” vision, in which their residual natural vision may allow the perception of high-contrast targets. Expanding the eligibility criterion from bare light perception to hand motion increases the number of patients who benefit from retinal prostheses. Residual retinal ganglion cells (RGCs) are necessary for artificial vision, and animal experiments using Royal College of Surgeons rats have shown that residual RGCs decrease with time after the degeneration of photoreceptor cells [18]. Patients with hand motion vision may have more RGCs and thus may have a greater chance of increasing their visual ability after the implantation of a retinal prosthesis compared with those with bare light perception.
Patients suffering from retinitis pigmentosa with residual vision show visual acuity to high-contrast targets but exhibit poor low-contrast sensitivity [19]. In this study, we evaluated the improvement in reaching movements to targets of various levels of contrast in a retinitis pigmentosa patient implanted with an STS retinal prosthesis, whose visual acuity in one eye was hand motion. We used the localization test with low-contrast targets, examining the effect of artificial vision in a condition where there was residual natural vision. In the field of cochlear implants, devices are implanted in patients with residual auditory function, helping them with speech recognition in complex listening environments [20].
Patient and methods
Patient
The patient was a 42-year-old man with advanced Stargardt disease (Fig. 1). His visual acuity before surgery was “light perception” in the right eye and hand motion in the left eye. He suffered subjective blindness at elementary school age. A mutation of ABCA4 gene was confirmed by genetic testing. Two and a half years before undergoing STS retinal prosthesis implantation [9], Goldmann perimetry showed residual partial sensitivity in the periphery in both eyes (Fig. 2). He underwent STS retinal prosthesis implantation surgery in his right eye and was then examined periodically using the localization test during a 1-year follow-up period.

Fundus photo. Advanced retinal degeneration was observed in the macula and peripheral retina in both eyes

Goldmann perimetry. Residual visual field (V/4 isopter) was observed in the periphery of both eyes
The procedures used in this study adhered to the principles of the Declaration of Helsinki and were approved by the Ethics Committee of Osaka University Hospital. A full explanation of the purpose of this study and the procedures to be used was presented to the patient, and he signed an informed consent form. It was made clear to the patient that he was free to withdraw at any time. The project was posted on the University Hospital Medical Information Network (UMIN), registration number UMIN 000012754 (2014.1.4).
Localization test
The localization test used a custom-built computer system (Nidek, Gamagohri, Japan) with a laptop computer (ThinkPad W520®, Lenovo, Beijing, China) and a 19-inch Elo 1929LM Medical Healthcare Touchmonitor® touch-sensitive screen (Elo Touch Solutions, Inc., Milpitas, CA, USA). The patient viewed the screen at a distance of 40 cm, with the center of the screen directly in front of the midpoint of the right and left eye. The visual angle of the screen was 53.6° × 42.8°. The illuminance of the room was 192 lx (LM331®, AS ONE, Osaka, Japan).
The test involved 20 trials. During each trial, a white square target (visual angle 10° × 10°, 7 cm × 7 cm) was displayed at one of 16 positions on the screen (4 × 4, uniform distribution), determined randomly by the computer program. The Michelson contrast value of the target, as measured by a luminance meter (BM-8®, Topcon, Itabashi, Japan), was set at one of three values: 96% (target brightness, 252.0 cd/m2; background brightness, 5.3 cd/m2), 85% (target brightness, 252.0 cd/m2; background brightness, 20.7 cd/m2), or 74% (target brightness, 252.0 cd/m2; background brightness, 37.2 cd/m2). The patient was instructed to touch the center of the target with his right index finger. He was permitted to move his head and eyes during the task unless he moved his head closer to the screen. The point on the screen the patient touched was automatically recorded, and the distance from the center of the target to the point touched was calculated. These differences were averaged over all 20 trials; this distance, referred to as the absolute deviation, indicated the accuracy of the patient’s reaching movement.
The localization test was conducted every month during the 1-year follow-up period. At each test session, the absolute deviation was measured under conditions with the STS system on or off and with one eye (right and left), both eyes occluded, or no occlusion, respectively. The order of the tests was randomly selected.
In addition, at 5 months after surgery, we examined the patient’s response time between when a 96%-contrast target was displayed and when the patient touched the screen. This was measured in a condition with the left eye occluded and the right eye occluded and compared afterwards.
Statistical analyses
Paired t tests were used to evaluate differences in the absolute deviation between the system on and off conditions. A p value of 0.05 or less was considered significant. SigmaPlot 12.2® (Systat Software Inc., San Jose, CA, USA) was used for the analyses.
Results
With the left eye occluded, absolute deviation with the high-contrast (96%) targets was generally lower under the STS system on condition than under the system off condition (Fig. 3a, b), but this difference was not statistically significant at 1, 3, and 9 months after the implantation surgery. With both eyes occluded, the absolute deviation with the high-contrast targets was always significantly lower under the system on condition than under the system off condition (Fig. 4).

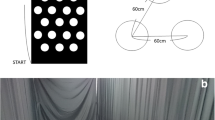
Results of the localization test (contrast of target, 96%; left eye occlusion). a Deviation from the center of the targets with or without retinal prosthesis at 5 months after the implantation surgery. The points represent the positions touched by the patient when the origin is set at the center of the target. The blue and red points represent the touched points with the suprachoroidal–transretinal stimulation (STS) system off and on, respectively. The central square represents the area of the white target (visual angle 10° × 10°, 7 cm × 7 cm). b Time course of the absolute deviation. The blue and red lines represent the mean deviations with the STS system off and on, respectively (visual angle 10° equals 7 cm). The vertical bars represent the standard deviation. M denotes months after surgery. *p < 0.05, **p < 0.01

Time course of the absolute deviation with target contrast 96% and both eyes occluded. The blue and red lines represent the mean deviations with the suprachoroidal–transretinal stimulation system off and on, respectively (visual angle 10° equals 7 cm). *p < 0.05, **p < 0.01
With the left eye occluded and the contrast of the targets reduced to 74%, the absolute deviation was always significantly smaller under the system on condition than under the system off condition (Fig. 5). When the contrast of the targets was 85% and both eyes were open, the absolute deviation was significantly smaller under the system on condition than under the system off condition (Fig. 6). In contrast, no significant difference was observed between the system on and system off conditions with high-contrast targets (96%) and both eyes open (data not shown).

Time course of the absolute deviation with target contrast 74% and the left eye occluded. The blue and red lines represent the mean deviations with the suprachoroidal–transretinal stimulation system off and on, respectively (visual angle 10° equals 7 cm). *p < 0.05, **p < 0.01

Time course of the absolute deviation with target contrast 85% and both eyes open. The blue and red lines represent the mean deviations with the suprachoroidal–transretinal stimulation system off and on, respectively (visual angle 10° equals 7 cm). *p < 0.05, **p < 0.01
The patient’s response time (the time between the target being displayed and the patient touching the screen), measured at 5 months, showed no significant difference in absolute deviation under the system on condition between left eye occlusion and right eye occlusion (absolute deviation: left eye occluded, 9.7° ± 3.4°; right eye occluded, 9.4° ± 6.8°; p = 0.84, paired t test), but the response time was significantly shorter with right eye occlusion (response time: left eye occluded, 8.5 ± 3.8 s; right eye occluded, 2.4 ± 2.5 s; p < 0.01, paired t test).
In addition, the absolute deviation was significantly smaller under the system on condition than under the system off condition with right eye occlusion (right eye occlusion and system off, 19.6° ± 12.0°; right eye occlusion and system on, 9.4° ± 6.8°; p < 0.01, paired t test).
Discussion
We used the accuracy of targeted reaching movements to evaluate the visual function of a patient with severe outer-retinal dystrophy but with residual natural vision, who was implanted with an STS retinal prosthesis. With high-contrast targets and the patient using both artificial vision and his residual natural vision in the right eye, the absolute deviation was significantly lower with the STS system on than when it was off for most of the test sessions during the follow-up period. However, no significant difference was observed on several occasions (Fig. 3b). On the test days when no significant difference was observed, the patient reported that he could see better with his residual natural vision. These results suggest that residual natural vision fluctuates and that the patient was able to see the high-contrast targets when his visual condition was good.
With both eyes occluded and the STS system off, the patient touched the display randomly; the absolute deviation was always lower with the system on (Fig. 4). This suggests that the patient’s visual performance achieved by artificial vision alone evaluated with both eyes occluded showed consistent results.
When the contrast of the targets was reduced to 74% and the patient used both artificial vision and residual natural vision in the right eye, the absolute deviation was always smaller when the STS system was on than when it was off (Fig. 5). This result indicates that the patient was able to identify low-contrast targets by artificial vision.
With both eyes open and a target contrast of 85%, the absolute deviation was significantly lower when the STS system was on than when it was off (Fig. 6). This contrasts with the result for high-contrast targets (96%), where there was no significant difference with when both eyes were open. These results suggest that residual natural vision can identify high-contrast targets but not lower-contrast targets and that artificial vision helped with discriminating low-contrast targets even under natural viewing conditions.
The patient’s mean response time to touch the display was significantly shorter with right artificial vision and left residual vision (right eye occlusion) than with right artificial vision and right residual vision (left eye occlusion) when the STS system was on. His residual vision may be more dominant in the left eye compared with the right eye. Therefore, when the STS system was off, the patient recognized targets with his left peripheral visual field by turning his eyes to the left (Fig. 7a). When the system was on, he used two gaze positions: a left gaze position using the peripheral visual field in the left eye and a forward gaze position using the central artificial visual field in the right eye (Fig. 7b). The patient reported that he recognized the rough position of a target by right artificial visual field and then confirmed the position by his left peripheral visual field. The reduction in reaction time with a combination of right artificial vision and left residual vision may have been due to the additive effect of artificial and residual vision.

Eye position. a Eye position under the system off condition. The patient watched the target with his left peripheral visual field by turning his eyes to the left. b Eye position under the system on condition. The patient fixated the target with the suprachoroidal–transretinal stimulator having a straight gaze with his right eye
In daily life, it is uncommon to come across high-contrast objects (such as the Landolt C), and people generally need to be able to distinguish low-contrast objects [21]. For patients with STS retinal prostheses, manipulating the threshold brightness of the CCD camera stimulating the electrode array can allow the patient to identify low-contrast targets. Improvements to image processing software may allow patients to highlight important objects [22, 23].
A limitation of this study was that we analyzed the interaction between artificial and natural vision in only one patient with residual peripheral visual field. Further study involving more patients with advanced outer-retinal dystrophy is needed to investigate whether artificial vision is really useful for patients with a residual visual field.
In conclusion, with an appropriate target contrast, the performance of a targeted reaching movement consistently improved in a patient implanted with an STS retinal prosthesis in an eye with residual natural vision. It is possible that patients with retinal prosthesis can improve their visual performance by using both the artificial vision and their residual natural vision.
Change history
25 May 2018
The original publication of this paper contain an error because of an incorrect captured corresponding author.
References
Guadagni V, Novelli E, Piano I, Gargini C, Strettoi E (2015) Pharmacological approaches to retinitis pigmentosa: a laboratory perspective. Prog Retin Eye Res 48:62–81. https://doi.org/10.1016/j.preteyeres.2015.06.005
Humayun MS, Weiland JD, Fujii GY, Greenberg R, Williamson R, Little J, Mech B, Cimmarusti V, Van Boemel G, Dagnelie G, de Juan E (2003) Visual perception in a blind subject with a chronic microelectronic retinal prosthesis. Vis Res 43:2573–2581
Rizzo JF 3rd, Wyatt J, Loewenstein J, Kelly S, Shire D (2003) Perceptual efficacy of electrical stimulation of human retina with a microelectrode array during short-term surgical trials. Invest Ophthalmol Vis Sci 44:5362–5369
Zrenner E (2002) Will retinal implants restore vision? Science (New York, NY) 295:1022–1025. https://doi.org/10.1126/science.1067996
Chow AY, Chow VY, Packo KH, Pollack JS, Peyman GA, Schuchard R (2004) The artificial silicon retina microchip for the treatment of vision loss from retinitis pigmentosa. Arch Ophthalmol (Chicago, Ill: 1960) 122:460–469. https://doi.org/10.1001/archopht.122.4.460
Lorach H, Goetz G, Mandel Y, Lei X, Galambos L, Kamins TI, Mathieson K, Huie P, Dalal R, Harris JS, Palanker D (2015) Performance of photovoltaic arrays in-vivo and characteristics of prosthetic vision in animals with retinal degeneration. Vis Res 111:142–148. https://doi.org/10.1016/j.visres.2014.09.007
Wong YT, Chen SC, Seo JM, Morley JW, Lovell NH, Suaning GJ (2009) Focal activation of the feline retina via a suprachoroidal electrode array. Vis Res 49:825–833. https://doi.org/10.1016/j.visres.2009.02.018
Shivdasani MN, Luu CD, Cicione R, Fallon JB, Allen PJ, Leuenberger J, Suaning GJ, Lovell NH, Shepherd RK, Williams CE (2010) Evaluation of stimulus parameters and electrode geometry for an effective suprachoroidal retinal prosthesis. J Neural Eng 7:036008. https://doi.org/10.1088/1741-2560/7/3/036008
Fujikado T, Kamei M, Sakaguchi H, Kanda H, Endo T, Hirota M, Morimoto T, Nishida K, Kishima H, Terasawa Y, Oosawa K, Ozawa M, Nishida K (2016) One-year outcome of 49-channel suprachoroidal-transretinal stimulation prosthesis in patients with advanced retinitis pigmentosa. Invest Ophthalmol Vis Sci 57:6147–6157. https://doi.org/10.1167/iovs.16-20367
Geruschat DR, Flax M, Tanna N, Bianchi M, Fisher A, Goldschmidt M, Fisher L, Dagnelie G, Deremeik J, Smith A, Anaflous F, Dorn J (2015) FLORA: phase I development of a functional vision assessment for prosthetic vision users. Clin Exp Optom 98:342–347. https://doi.org/10.1111/cxo.12242
Klein BE, Klein R, Lee KE, Cruickshanks KJ (1999) Associations of performance-based and self-reported measures of visual function. The Beaver Dam Eye Study. Ophthalmic Epidemiol 6:49–60
Rubin GS, Bandeen-Roche K, Huang GH, Munoz B, Schein OD, Fried LP, West SK (2001) The association of multiple visual impairments with self-reported visual disability: SEE project. Invest Ophthalmol Vis Sci 42:64–72
West SK, Rubin GS, Broman AT, Munoz B, Bandeen-Roche K, Turano K (2002) How does visual impairment affect performance on tasks of everyday life? The SEE Project. Salisbury Eye Evaluation. Arch Ophthalmol (Chicago, Ill: 1960) 120:774–780
Subramanian A, Dickinson C (2006) Spatial localization in visual impairment. Invest Ophthalmol Vis Sci 47:78–85. https://doi.org/10.1167/iovs.05-0137
Ahuja AK, Behrend MR (2013) The Argus II retinal prosthesis: factors affecting patient selection for implantation. Prog Retin Eye Res 36:1–23. https://doi.org/10.1016/j.preteyeres.2013.01.002
Rizzo S, Belting C, Cinelli L, Allegrini L, Genovesi-Ebert F, Barca F, di Bartolo E (2014) The Argus II Retinal Prosthesis: 12-month outcomes from a single-study center. Am J Ophthalmol 157:1282–1290. https://doi.org/10.1016/j.ajo.2014.02.039
Endo T, Kanda H, Hirota M, Morimoto T, Nishida K, Fujikado T (2016) False reaching movements in localization test and effect of auditory feedback in simulated ultra-low vision subjects and patients with retinitis pigmentosa. Graefe’s Arch Clin Exp Ophthalmol Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie 254:947–956. https://doi.org/10.1007/s00417-015-3253-2
Isago H, Sugano E, Wang Z, Murayama N, Koyanagi E, Tamai M, Tomita H (2012) Age-dependent differences in recovered visual responses in Royal College of Surgeons rats transduced with the Channelrhodopsin-2 gene. J Mol Neurosc 46:393–400. https://doi.org/10.1007/s12031-011-9599-y
Hirota M, Morimoto T, Kanda H, Lohmann TK, Miyagawa S, Endo T, Miyoshi T, Fujikado T (2017) Relationships between spatial contrast sensitivity and parafoveal cone density in normal subjects and patients with retinal degeneration. Ophthalmic Surg Lasers Imaging Retina 48:106–113. https://doi.org/10.3928/23258160-20170130-03
Gifford RH, Dorman MF, Skarzynski H, Lorens A, Polak M, Driscoll CL, Roland P, Buchman CA (2013) Cochlear implantation with hearing preservation yields significant benefit for speech recognition in complex listening environments. Ear Hear 34:413–425. https://doi.org/10.1097/AUD.0b013e31827e8163
Owsley C, Sloane ME (1987) Contrast sensitivity, acuity, and the perception of ‘real-world’ targets. Br J Ophthalmol 71:791–796
Parikh N, Itti L, Weiland J (2010) Saliency-based image processing for retinal prostheses. J Neural Eng 7:16006. https://doi.org/10.1088/1741-2560/7/1/016006
Barnes N, Scott AF, Lieby P, Petoe MA, McCarthy C, Stacey A, Ayton LN, Sinclair NC, Shivdasani MN, Lovell NH, McDermott HJ, Walker JG (2016) Vision function testing for a suprachoroidal retinal prosthesis: effects of image filtering. J Neural Eng 13:036013. https://doi.org/10.1088/1741-2560/13/3/036013
Funding
This study was partly supported by the Strategic Research Program for Brain Sciences by the Ministry of Education, Culture, Sports, Science and Technology of Japan. The sponsor had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of Osaka University Hospital and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Endo, T., Fujikado, T., Hirota, M. et al. Light localization with low-contrast targets in a patient implanted with a suprachoroidal–transretinal stimulation retinal prosthesis. Graefes Arch Clin Exp Ophthalmol 256, 1723–1729 (2018). https://doi.org/10.1007/s00417-018-3982-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-018-3982-0