
Abstract
Background
A noticeable change of the male-to-female sex ratio (SR) has been observed in Amyotrophic Lateral Sclerosis (ALS) leading to an apparent regression of SR with time (SR close to 1:1).
Objective
To provide a global SR estimate and investigate its relation with respect to population age.
Methods
A systematic review and meta-analysis was conducted including only population-based studies with a high-quality methodology in European ancestral origin population. Male-to-female SR was estimated by three different measures: SR number, SR crude incidence and SR standardized incidence. Standard and dose–response meta-analyses were performed to assess the pooled SR measures (irrespective of population age) and the evolution of the SR measures with respect to population age, respectively. Potential sources of heterogeneity were investigated via meta-regression.
Results
Overall, 3254 articles were retrieved in the literature search. Thirty-nine studies stratified by time periods were included. The overall pooled male-to-female ratio was 1.28 (95% CI 1.23–1.32) for SR number, 1.33 (95% CI 1.29–1.38) for SR crude incidence and 1.35 (95% CI 1.31–1.40) for SR standardized incidence. The SR number with respect to population age reveals a progressive reduction of SR at increasing age, while the SR crude incidence in relation to age displays a U-shaped curve.
Conclusions
The number and the incidence of ALS cases were consistently higher in males than females. Dose–response meta-analysis showed that SR measures change with respect to population age. Further original research is needed to clarify if our findings are reproducible in other populations.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Background
Amyotrophic Lateral Sclerosis (ALS) is a rare neurodegenerative disorder, whose male-to-female sex ratio (SR) is a controversial issue. There has been a noticeable change in the SR over time. Studies published before 1990, mostly non population-based, reported SR of 2:1 while more recent European or US population-based studies described a SR that is now approaching 1:1 [1,2,3]. Chio et al. based on the 20-year period of the PARALS register, showed that the adjusted male-to-female rate ratio decreased from 1.27:1 (1995–2004) to 1.17:1 (2005–2014) [4].
The regression of SR with time could be related to the design of the studies that were examined: (1) non-population-based studies in oldest time-periods (vs population-based in recent investigations), (2) type of design (prospective vs retrospective), (3) diagnostic criteria. A better ascertainment of female ALS cases in more recent times cannot be excluded [1,2,3]. Nevertheless, such evolution (if confirmed) could also be explained by a real increase of ALS incidence for female as compared to male. This latter might be related to a progressive change in the sex prevalence of exposure to some risk factors (e.g., smoking habits, occupation). The effect of the ageing of the populations and longer life expectancy in female could be also implicated.
The evolution of SR with age in a given population is another unclear matter in ALS. Some reports indicated a progressive increase of SR with age, but to date this issue was overlooked.
A systematic approach focusing on population-based studies is mandatory to get closer to the real pattern (a reliable illustration of observable characteristics of a group) of SR in ALS. Such an approach would need to rely on: (1) reports from homogeneous populations in terms of ancestral origin, to control any variability of SR related to ethnicity [5], (2) reports with high and homogeneous standards for case ascertainment (hence including only population-based studies). In this context, we performed a systematic review and meta-analysis of ALS sex ratio in European ancestral origin population. The aim was to provide a global SR estimate and investigate the evolution of SR with respect to population age along with the exploration of possible sources of heterogeneity (such as the time period).
Methods
This meta-analysis is undertaken within the framework of a global epidemiological investigation of ALS. Additional methodological details have been described elsewhere [5,6,7]. We followed the recommendations of the guideline for Meta-analysis Of Observational Studies in Epidemiology (MOOSE) [8] and The Role of Systematic Reviews and Meta-Analyses of Incidence and Prevalence Studies in Neuroepidemiology [9].
Definitions
Motor neuron disease (MND) was investigated which includes ALS and ALS subtypes: Progressive Bulbar Palsy (PBP), Progressive Muscular Atrophy (PMA), and Primary Lateral Sclerosis (PLS) [10]. Population-based studies with high-quality design were determined by the use of multiple sources of case ascertainment within defined geographical and time boundaries of well-defined populations [11]. Ancestral origin was defined as a group of individuals, who are more or less isolated geographically or culturally, who share a common genetic pool, whose allele frequencies at some loci differ from those of the other populations [12]. Subcontinent was used as a proxy for ancestral origin. Subcontinent classification was based on the United Nations Statistics Division [13].
Search strategy
We searched in Medline and Embase (until June 2016) without language limitations. Key-words are described in Table e-1. Hand searching was also performed. All references identified were imported into Endnote X7 and duplicates were deleted.
Inclusion criteria
We included population-based studies of newly diagnosed ALS cases with a neurological confirmation using multiple sources to ensure the highest level of completeness for case ascertainment. Given that ancestral origin could play a role in ALS variability, we only included studies of European population using subcontinent as a proxy (Sub-continents: Europe, Northern America, Australia and New Zealand) to control any variability of SR related to ancestral origin. Therefore, studies of non-European populations were excluded from the analysis.
The starting date of our investigation was 1969. As a result, for the only study that started before this date (with a long follow-up, 1925–1998) [14], we considered only the period 1969–1998. For studies with a follow-up period longer than 15 years, authors or their collaborators were contacted to obtain ALS patients distribution by age and sex for intermediate periods lasting around 10 years as a maximum. For studies presenting two different periods in the same geographic area, we considered both periods. This has enabled us to assess time-trend evolution of SR in given areas.
Data extraction
A checklist was used to assess the basic principles of descriptive epidemiology of the included articles. We recorded the following data: authors, year of publication, period, location, design, sources of case ascertainment, diagnostic criteria, number of patients (male, female), study population (male, female, age structure), number of cases and the number of person years at follow-up (PYFU) within each age group and sex. For each enrolled ALS case, the individual follow-up was defined (within each age group and sex) as the time between the entry in the age interval and one of the following events (whichever occurred first): ALS diagnosis, end of the age-interval, censoring (e.g., loss to follow-up). Authors or their collaborators were contacted to obtain updated data and/or additional information, if necessary. When more than one publication was available for the same geographic area at different periods, data was gathered separately. Life expectancies at 50 years for male and female were retrieved from the demographic yearbook published by the United Nations at the mid-point of the study period for each geographical area [15].
Statistical analysis
Male-to-female SR was estimated with three different measures:
-
i.
SR number: the ratio of the number of male cases by number of female cases, which is the most common way to report sex ratio in the ALS literature.
-
ii.
SR crude incidence: the ratio of the ALS crude incidence rate in males by the ALS crude incidence rate in females. Incidence rates were defined as the number of ALS cases divided by the number of PYFU.
-
iii.
SR standardized incidence: the ratio of the standardized incidence rate in males by the standardized incidence rate in females. Standardized incidence rates were defined as the number of ALS cases divided by the number of PYFU, weighted by the population age structure under-surveillance. Direct standardization was performed using the 2010 US population.
The assessment of pooled SR measures (irrespective of population age) and the assessment of the evolution of the SR measures with respect to population age were performed by standard and dose–response meta-analyses, separately. These two analyses are detailed in the following subsections.
Meta-analysis of the SR measures
To determine the overall and subcontinent-specific pooled estimates of each SR measure, a standard meta-analysis was performed following a two-step process.
First step: for each included study, a Poisson regression model was fitted to investigate the study-specific association between the number of cases (or incidence rates accordingly) and sex. The natural logarithm of males-to-females SR was straightforwardly assessed by looking at the estimated regression coefficient for sex. Second step: all the SRs (estimated in all studies) were pooled in a standard meta-analysis.
The presence of between-study heterogeneity was assessed by the Cochran’s Q-test (as well as the corresponding I2 measure) and was declared if its p value was lower than 0.10 and, at the same time, I2 was greater than 25% [16]. A fixed-effect or a random-effect model was performed according to the absence or the presence of significant heterogeneity, respectively [17]. The analysis was repeated for each SR measure, overall and within each subcontinent (strata variable), separately. Forest plots of the study-specific SR estimates (converted in their original scale), as well as the pooled SR estimates, were shown.
Meta-regression was also performed, in presence of significant heterogeneity, to investigate potential sources of heterogeneity with respect to a number of key study characteristics (i.e., study-level covariates), using random effect models. As recommended by the Cochrane guidelines [18], meta-regression was performed for all included studies and within subcontinents, which included at least ten studies.
Assessment of the evolution of pooled SR measures with respect to population age
To determine the overall and subcontinent-specific evolution of each SR measure with respect to the population age, a dose–response meta-analysis was performed following a similar two-step process. The term “dose–response” has become increasingly common in recent years and was merely used herein for describing the change, defined as a mathematical function, of any endpoint (e.g., SR measures) with respect to a quantitative independent variable (i.e., a “dose”), which was represented by the population age.
First step: For each included study, a Poisson regression model was fitted to investigate the study-specific relationship between the number of cases (or incidence rates accordingly) and the population age (defined as a continuous variable), in males and females, respectively. At this time, each model included: age, sex and age-by-sex interaction term as covariates so that the evolution of the SR measures can be straightforwardly assessed by looking at the estimated regression coefficients for those covariates, which represent changes in the natural logarithm of SR for each yearly increase of population age, sex and for the differential slope of the yearly increase between sex, respectively. Second step: all the regression estimates were pooled in a multivariate meta-analysis.
The presence of between-study heterogeneity of the coefficient estimates was assessed by the multivariate Cochran’s Q-test (along with I2) and a fixed-effect or a random-effect model was performed for each SR measure as appropriate. Moreover, the estimated pooled relationship between SR measures with respect to different population age was graphically depicted with a plot of the “meta-analyzed” curve along with its gray band denoting a 95% confidence interval. Also, in this case, a meta-regression was eventually performed in presence of significant heterogeneity using random effect models. Further details about statistical methods can be found in the supplemental material (Appendix e-1).
Two-sided p values < 0.05 were considered statistically significant. Analyses were performed using SAS®, version 9.4 (SAS Institute, Cary, NC) and the computing environment R (R Development Core Team 2008, version 3.6.3, package: metafor).
Results
Included studies
Overall, 3254 articles were retrieved in the literature search. After removing all duplicates, the title and abstract were considered of 291 full-text articles. A comprehensive examination of the full texts was performed to identify 44 population-based studies of ALS incidence using multiple sources of case ascertainment. We excluded ten studies because they were conducted outside the geographic area of interest and another two studies due to a lack of available sex-stratified data (from Lancashire and Nova Scotia). Authors provided supplementary and updated information on ALS incidence from South East—England, Emilia Romagna—Italy, and Countryside—Ireland (replacing data for one study). Data were stratified in seven studies, which were carried out in the same area at different time periods (South East—England, Countryside—Faroe Island, Countryside—Ireland, Swabia—Germany, Emilia Romagna—Italy, Olmsted county—US and Canterbury—New Zealand). One period was excluded due to poor data quality (Faroe Island, 1998—2009) and another because case ascertainment was only conducted in a geographic segment of the original area (South East England, 2007–2013). The PRISMA flowchart is shown in Figure e-1. A total of 39 population-based investigations stratified by time periods were included in the analysis [consisting of 32 published articles, 3 investigations from personal data and 4 stratified time periods (3 published studies and 1 personal data)]. Characteristics of the included studies are described in Table e-2.
Geographical coverage
Of the 39 population-based studies on populations of European origin, 27 were in Europe (12 in Northern Europe, 5 in Western Europe, 10 in Southern Europe), 10 in Northern America (Canada and the USA), and 2 in New Zealand.
Meta-analysis of the male-to-female SR measures
Forest plots with study-specific and pooled SR estimates from meta-analyses were performed for all studies and within each subcontinent, as shown in Fig. 1. The number and the incidence of ALS cases were consistently higher in males than females, both in the study population and within the subcontinents (Northern Europe, Western Europe, Southern Europe, Northern America, Australia and New Zealand). The overall pooled male-to-female SR number was 1.28 (95% CI 1.23–1.32) (Fig. 1a). When we took into account the time at which the ALS occurred (i.e., PYFU) for each sex, the overall pooled SR crude incidence was 1.33 (95% CI 1.29–1.38) (Fig. 1b) while, when we considered the PYFU for each sex and controlled the age distribution of the population, the overall pooled SR standardized incidence was 1.35 (95% CI 1.31–1.40) (Fig. 1c).


Forest plots and pooled estimates of: a SR number (SRn), b SR crude incidence (SRci), c SR standardized incidence (SRsi)
No significant heterogeneity was detected for all studies and within each subcontinent for SR number (Table 1a). As shown in Table 1b and c, no significant heterogeneity was detected for all studies in SR crude incidence and SR standardized incidence, while there was statistically significant heterogeneity in Northern Europe for both SR crude incidence (Cochran’s Q, p = 0.076 and I2 = 39.8%, Table 1b) and SR standardized incidence (Cochran’s Q, p = 0.031 and I2 = 48.3%, Table 1c). Meta-regression was conducted to explore the sources of heterogeneity. We found that the overall between-study heterogeneity in Northern Europe was explained in part (i.e., reduced) by GPS coordinates (R2 = 43.6%) for SR crude incidence (Table e-3a), while it was almost totally explained by the time period of the study (R2 = 92.7%) for SR standardized incidence (Table e-3b).
Evolution of pooled male-to-female SR measures with respect to population age
Dose–response meta-analyses were performed to assess the relationship of ALS incidence between SR measures at different population ages. The observed number of cases and the crude incidence rates per 100 000 PYFU in males and females related to population age values were reported, for each original study, along with the estimated curves by subcontinents: (a) Northern Europe, (b) Southern Europe, (c) Western Europe, (d) Northern America, and (e) New Zealand, in Figure e-2 and Figure e-3, respectively. The goodness of fit measures (R2) calculated from Poisson models are shown in Table e-4.
As shown in Tables 2a and b, significant heterogeneity was detected in New Zealand for both SR number (multivariate Cochran’s Q, p = 0.014 and I2 = 71.7%) and SR crude incidence (multivariate Cochran’s Q, p = 0.065 and I2 = 58.5%), respectively. However, heterogeneity could not be explored due to the very small number of included studies (N = 2) for that subcontinent.
Sex ratio related to population age
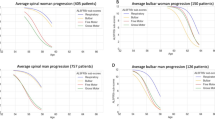
A closer look at the estimated “meta-analyzed” curves of pooled male-to-female SR number with respect to population age reveals a progressive reduction of SR number at increasing age. As shown in Fig. 2, the overall pattern was characterized by a higher SR number for younger ages followed by a progressive slow steady decrease which continued in the oldest old (resulting in an SR number inversion). At the peak age (60 s or 70 s), the SR number ranged from 1.20 to 1.36. A similar pattern was found within each subcontinent, although the SR number inversion in the oldest age was not found in Western Europe and Northern America. Unlike the SR number, the male-to-female crude incidence rate ratio in relation to age displayed a U-shaped curve (Fig. 3). The pattern exhibited a higher SR crude incidence for younger ages with a steady decrease until the peak age of incidence (60–70 s, SR crude incidence = 1.44) followed by a subsequent progressive increase in older age. Therefore, a high SR crude incidence for both the youngest and the oldest ages with an inflexion at the peak age of incidence was found. A similar pattern was observed within each subcontinent (Fig. 3).

Dose–response meta-analysis of male-to-female SR number with respect to population age, overall (with and without the inclusion of New Zealand) and by subcontinent

Dose–response meta-analysis of male-to-female SR crude incidence with respect to population age, overall (with and without the inclusion of New Zealand) and by subcontinent
These findings were consistent after performing all statistical analyses having excluded the two studies from New Zealand. Table e-5 shows the pooled estimates of SR number and SR crude incidence by age categories along with their 95% CI in all studies and within subcontinents.
Discussion
This meta-analysis provides a global assessment of ALS male-to-female SR measures and their relationship with different ages in European ancestral origin populations. A higher number and incidence of male cases compared to female cases was consistently described in SR estimates. Dose–response meta-analyses show the specific relationship between SR measures and population age. All results were consistent within the subcontinents (Northern Europe, Western Europe, Southern Europe, Northern America, Australia and New Zealand).
Male-to-female SR is a subject that has drawn attention in recent years [19, 20] due to an apparent increase of incident female cases which led to a regression of SR over time (SR close to 1). It was suggested that this is related, at least in part, to lifestyle or exposure changes in the last decades. Methodological issues, improvement of case ascertainment in females and changes in the age structure of the population along with longer life expectancy were also proposed. Here, we conducted several meta-analyses including original studies with a high-standard methodology to perform a statistical synthesis of SR estimates. Statistical synthesis of findings allows the degree of conflict to be formally assessed, and reasons for different results to be explored and quantified [21]. For instance, we have found that the between-study heterogeneity was explained by the time period for SR standardized incidence in Northern Europe.
The higher number and incidence of male cases than female cases was consistent in all SR measures (SR number, SR crude incidence and SR standardized incidence). The relationship of male-to-female SR with respect to the population age highlights the importance of taking into account the population at risk. The SR number showed a progressive increase in female cases at increasing age (Fig. 2). This was in contrast with SR crude incidence where SR remains higher in younger age and older age (Fig. 3). This difference might be due to the far higher PYFU in the oldest old females than the oldest old males. Therefore, the adjusted data for the underlying population structure allowed us to control for the relative increase in the proportion of females in the elderly population.
The findings from the SR crude incidence could be considered a more reliable description of the male-to-female SR because incidence rates include follow-up times and implicitly account for the fact that females achieve higher survival than males. The SR crude incidence clearly shows that accounting for individual PYFU, the male to female ratios was characterized by a U-shape.
The relationship between male-to-female SR number and population age might explain the change of SR over time: several decades ago, the age at diagnosis was around 60 s (corresponding a SR around 1.4) while nowadays mean age is closer to 70 s (corresponding a SR closer to 1). In that respect, we cannot exclude the possibility that a change in age at diagnosis could be explained by a change in life expectancy in the corresponding time. If the relationship between SR number and population age is similar across populations, it could also explain (at least in part) the differences in SR reported in other parts of the world. Population-based studies have reported a SR number around 2 in Northern Africa [22] and South Asia [23], where age at diagnosis was around 50 s. However, it is difficult to draw conclusions given the limited quality data in several subcontinents and the potential role of ancestral origin and environmental exposure in ALS heterogeneity. Methodological issues cannot be excluded. It remains to be determined whether these differences in sex distribution are genuine in other populations or they could be explained by differences in terms of population structure, accessibility to the health system, or reduced case ascertainment in females. Further original studies with high standard methodology are needed in areas poorly represented in the literature to clarify this important issue.
Studies have suggested there may be differences in male-to-female SR among ALS subtypes. For instance, male-to-female SR was 1:2 for PLS [24], 2:1 for PMA, 4:1 for flail-arm-syndrome and 1:1 for flail-leg-syndrome [25]. However, these studies were conducted in referral centres that are known to drive a selection bias [26] and there was a limited number of cases included. Only one population-based study reported a male predominance of PLS cases (male-to-female SR = 1.45) [27]. Therefore, it very difficult to draw conclusions on SR in ALS subtypes given the limited quality data. Further studies are needed, mainly population-based studies.
It remains to explore the influence of genetics and environmental factors in the predominance of incident male cases and the relationship between SR and population age. Sex differences in ALS might be linked to unequal exposures or different responses to risk factors [28]. For instance, case–control studies have shown that the risk of developing ALS appeared to be greater in female smokers than in male smokers [29, 30]. Although this association remains controversial, this suggests that males and females could experience different effects from the same exposure [28]. The relation between age, sex, and genetic susceptibility is another interesting subject to investigate. The role of ancestral origin also needs to be considered. A recent population-based study described the association of clinical characteristics and phenotypes with age and sex. The authors suggested a possible link between the pathologic process and a differential susceptibility determined by age, sex, and genetics [31]. These relations could have important implications to improve our understanding of ALS.
The strengths of this work rely on several points. First, we included only population-based studies using multiple sources for case ascertainment (high-quality methodology). Second, we obtained updated and verified data by contacting the authors or their collaborators when necessary. Third, the dose–response meta-analysis was performed following a strong analytical approach which let to assess the nonlinear relationship between ALS measures and population age within each study (first step) and then to meta-analyze findings among studies in a multivariate fashion (second step). Last, we investigated the sources of heterogeneity using several study-level covariates including time period. Some limitations need to be discussed. First, we used a geographical approach as a proxy of ancestral origin. We recognize that it is difficult to argue about the homogeneity of populations within a given subcontinent. However, it is a useful initial approach to address ethnicity given the lack of stratified data by ancestral origin populations in the literature. Second, we included only studies of European ancestral origin populations in an effort to control variability related to ethnicity. In that respect, our findings cannot be generalized to other populations. Last, although we investigated potential sources of heterogeneity, meta-regression does not allow us to speculate about the presence of any cause-effect relationship.
Conclusion
This meta-analysis found that the number and the incidence of ALS cases were consistently higher in males than females in the European ancestral origin population. Dose–response meta-analysis showed that SR measures change with respect to population age. All the elements combined allow us to improve our understanding of SR measures. It is necessary to explore the influence of other factors (e.g., ancestral origin, environmental factors) on age and sex. Further original research is needed to clarify if our findings are similar in other populations.
Data availability
The data for the analyses described in this paper are available by request from the authors.
References
Beghi E, Logroscino G, Chiò A et al (2006) The epidemiology of ALS and the role of population-based registries. Biochim Biophys Acta 1762:1150–1157. https://doi.org/10.1016/j.bbadis.2006.09.008
Logroscino G, Traynor BJ, Hardiman O et al (2008) Descriptive epidemiology of amyotrophic lateral sclerosis: new evidence and unsolved issues. J Neurol Neurosurg Psychiatry 79:6–11. https://doi.org/10.1136/jnnp.2006.104828
Luna J, Logroscino G, Couratier P, Marin B (2017) Current issues in ALS epidemiology: variation of ALS occurrence between populations and physical activity as a risk factor. Rev Neurol (Paris) 173:244–253. https://doi.org/10.1016/j.neurol.2017.03.035
Chiò A, Mora G, Moglia C et al (2017) Secular trends of amyotrophic lateral sclerosis: the piemonte and valle d’Aosta register. JAMA Neurol 74:1097–1104. https://doi.org/10.1001/jamaneurol.2017.1387
Marin B, Boumédiene F, Logroscino G et al (2017) Variation in worldwide incidence of amyotrophic lateral sclerosis: a meta-analysis. Int J Epidemiol 46:57–74. https://doi.org/10.1093/ije/dyw061
Marin B, Logroscino G, Boumédiene F et al (2016) Clinical and demographic factors and outcome of amyotrophic lateral sclerosis in relation to population ancestral origin. Eur J Epidemiol 31:229–245. https://doi.org/10.1007/s10654-015-0090-x
Marin B, Fontana A, Arcuti S et al (2018) Age-specific ALS incidence: a dose-response meta-analysis. Eur J Epidemiol 33:621–634. https://doi.org/10.1007/s10654-018-0392-x
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283:2008–2012. https://doi.org/10.1001/jama.283.15.2008
Fiest KM, Pringsheim T, Patten SB et al (2014) The role of systematic reviews and meta-analyses of incidence and prevalence studies in neuroepidemiology. Neuroepidemiology 42:16–24. https://doi.org/10.1159/000355533
Mitsumoto H, Chad DA, Pioro EP (1998) Amyotrophic lateral sclerosis. Oxford University Press, Oxford
Szklo M (1998) Population-based cohort studies. Epidemiol Rev 20:81–90. https://doi.org/10.1093/oxfordjournals.epirev.a017974
(2000) Census, race and science. Nat Genet 24:97–98. https://doi.org/10.1038/72884
United Nations Statistics Division Composition of macro geographical (continental) regions, geographical sub-regions, and selected economic and other groupings. https://unstats.un.org/unsd/methodology/m49/
Sorenson EJ, Stalker AP, Kurland LT, Windebank AJ (2002) Amyotrophic lateral sclerosis in Olmsted County, Minnesota, 1925 to 1998. Neurology 59:280–282. https://doi.org/10.1212/wnl.59.2.280
United Nations Demographic yearbook. DYB annual issues. https://unstats.un.org/unsd/demographic-social/products/dyb/index.cshtml
Greenland S (1987) Quantitative methods in the review of epidemiologic literature. Epidemiol Rev 9:1–30. https://doi.org/10.1093/oxfordjournals.epirev.a036298
van Houwelingen HC, Arends LR, Stijnen T (2002) Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 21:589–624. https://doi.org/10.1002/sim.1040
Higgins J, Thomas J (2011) Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration
Manjaly ZR, Scott KM, Abhinav K et al (2010) The sex ratio in amyotrophic lateral sclerosis: a population based study. Amyotroph Lateral Scler Off Publ World Fed Neurol Res Group Mot Neuron Dis 11:439–442. https://doi.org/10.3109/17482961003610853
Trojsi F, D’Alvano G, Bonavita S, Tedeschi G (2020) Genetics and sex in the pathogenesis of amyotrophic lateral sclerosis (ALS): is there a link? Int J Mol Sci. https://doi.org/10.3390/ijms21103647
Deeks JJ, Higgins JP, Douglas DG, on behalf of the Cochrane Statistical Methods Group (2019) Chapter 10: analysing data and undertaking meta-analyses. In: Cochrane Handbook for Systematic Reviews of Interventions, 2nd Edition. John Wiley & Sons, Chichester (UK)
Radhakrishnan K, Ashok PP, Sridharan R, Mousa ME (1986) Descriptive epidemiology of motor neuron disease in Benghazi, Libya. Neuroepidemiology 5:47–54. https://doi.org/10.1159/000110812
Sajjadi M, Etemadifar M, Nemati A et al (2010) Epidemiology of amyotrophic lateral sclerosis in Isfahan. Iran Eur J Neurol 17:984–989. https://doi.org/10.1111/j.1468-1331.2010.02972.x
Ramanathan RS, Rana S (2018) Demographics and clinical characteristics of primary lateral sclerosis: case series and a review of literature. Neurodegener Dis Manag 8:17–23. https://doi.org/10.2217/nmt-2017-0051
Wijesekera LC, Mathers S, Talman P et al (2009) Natural history and clinical features of the flail arm and flail leg ALS variants. Neurology 72:1087–1094. https://doi.org/10.1212/01.wnl.0000345041.83406.a2
Logroscino G, Marin B, Piccininni M et al (2018) Referral bias in ALS epidemiological studies. PLoS ONE 13:e0195821. https://doi.org/10.1371/journal.pone.0195821
Finegan E, Chipika RH, Li Hi Shing S et al (2019) The clinical and radiological profile of primary lateral sclerosis: a population-based study. J Neurol 266:2718–2733. https://doi.org/10.1007/s00415-019-09473-z
McCombe PA, Henderson RD (2010) Effects of gender in amyotrophic lateral sclerosis. Gend Med 7:557–570. https://doi.org/10.1016/j.genm.2010.11.010
Alonso A, Logroscino G, Jick SS, Hernán MA (2010) Association of smoking with amyotrophic lateral sclerosis risk and survival in men and women: a prospective study. BMC Neurol 10:6. https://doi.org/10.1186/1471-2377-10-6
Weisskopf MG, McCullough ML, Calle EE et al (2004) Prospective study of cigarette smoking and amyotrophic lateral sclerosis. Am J Epidemiol 160:26–33. https://doi.org/10.1093/aje/kwh179
Chiò A, Moglia C, Canosa A et al (2020) ALS phenotype is influenced by age, sex, and genetics: a population-based study. Neurology 94:e802–e810. https://doi.org/10.1212/WNL.0000000000008869
Acknowledgements
We thank the following main authors or co-authors of population-based articles who answered our solicitation and for the useful material that they were able to provide: Kari Murros, Poul Joensen, Raeburn Forbes, Robert Swingler (the Scottish MND Register is funded by MND Scotland and supported by the Anne Rowling Regenerative Neurology Clinic), Ibrahim Imam, James Rooney, Albert Ludolph, Gabriele Nagel, Marwa Elamin, Ammar Al-Chalabi, Orla Hardiman, Mark Heverin, Mark Huisman, Joachim Wolf, Adriano Chio, Federica Pisa, Jessica Mandrioli, Monica Bandettini, Stefano Zocollela, Maura Pugliatti, Leslie Parish, Paolo Ragonese, Valerie Mc Guire, Will Longstreth, Eric J. Sorenson, Farrah Mateen, James D. Bonaparte, Cristina Vazquez, Carlos Ketzoian, Kurupath Radhakrishnan, Chien-Hsu Lai, Chung Yan G Fong, Hitoshi Okumura, Tameko Kihira, Bruce Taylor and A Lannuzel. We thank Paul Mehta, Heather Jordan and Jhaqueline Valle for providing data to calculate US incidence. The data came from surveillance projects funded by the Agency for Toxic Substances and Disease Registry’s (ATSDR) National ALS Registry [www.cdc.gov/als] (Contract #200-2009- 32577 and Contract #200-2010-F-36614). We also thank Walter Rocca and Brandon R. Grossardt for the detailed data on Olmsted county population with which they provided us, and Hidenao Sasaki, Robert Miller and Eric Denys as contact persons. We thank Vanna Pistotti for her advice during the literature search, as well as Mineko Terao, Lorenzo Moja and Claudio Pelucchi. We thank Limoges teaching hospital for its grant initiative for mobility.
Funding
This research received no specific Grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed significantly to this paper. Conceptualization: AF, BM, MC; data curation: AF, BM; statistical analysis: AF, BM; interpretation; AF, BM, JL; writing-original draft: AF, BM, JL; all authors reviewed the first draft. All authors contributed to the final manuscript in terms of intellectual content.
Corresponding author
Ethics declarations
Conflicts of interest
Andrea Fontana, Benoit Marin, Jaime Luna, Giancarlo Logroscino, Farid Boumédiene, Pierre-Marie Preux, Philippe Couratier and Massimilano Copetti declare no disclosures relevant to the manuscript. Ettore Beghi declares to collaborate with the Italian Ministry of Health, SOBI, Arvelle Therapeutics and the American ALS Association.
Ethical approval
As this review of the literature/meta-analysis does not involve ALS patients but makes use of publications concerning ALS, informed consent of patients is not applicable. Not even approval of an ethics committee is applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Fontana, A., Marin, B., Luna, J. et al. Time-trend evolution and determinants of sex ratio in Amyotrophic Lateral Sclerosis: a dose–response meta-analysis. J Neurol 268, 2973–2984 (2021). https://doi.org/10.1007/s00415-021-10464-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-021-10464-2