
Abstract
Background
Patients with idiopathic cervical dystonia (CD) experience involuntary neck muscle contractions, abnormal head position and pain accompanied by dysfunctions in somatosensory processes such as postural control, cervical sensorimotor and perception of visual verticality. First-line treatment is injection with botulinum toxin (BoNT). It remains unclear whether this affects sensorimotor processes.
Aim
To investigate the effect of first-line care on deficiencies in somatosensory processes.
Methods
In this observational study, 24 adult patients with idiopathic CD were assessed three times over a treatment period of 12 weeks following a single treatment with BoNT. Disease severity was assessed by a disease-specific questionnaire, rating scale and the visual analogue scale. Seated postural control was assessed with posturography, cervical sensorimotor control was assessed by the joint repositioning error with an eight-camera infrared motion analysis system during a head repositioning accuracy test and perception of visual verticality was assessed with the subjective visual vertical test.
Results
Disease symptoms significantly improved following BoNT injections and deteriorated again at 12 weeks. This improvement was not accompanied by improved postural control, cervical sensorimotor control and perception of visual verticality. A trend toward improvement was seen; however, it did not reach the level of the control population.
Conclusion
The peripheral and central treatment effects of BoNT have little to no effect on postural and cervical sensorimotor control in CD. Further research may explore whether sensory training or specialized exercise therapy improves somatosensory integration and everyday functioning in patients with CD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cervical dystonia (CD) is a focal form of dystonia characterized by dystonic contractions of the neck muscles. “Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive movements, postures, or both. Dystonic movements are typically patterned, twisting, and may be tremulous. Dystonia is often initiated or worsened by voluntary action and associated with overflow muscle activation” [1]. Initially, CD was regarded as a motor disorder in which deficient motor output causes involuntary neck muscle contractions, repetitive movements, abnormal head postures or both in which one or more nodes of the sensorimotor network (e.g., cortex, basal ganglia, cerebellum and brainstem) are involved [2, 3]. However, the concept is shifting towards the idea that defaulted (somato)sensory processing also plays an important role in the symptomatology of CD because dysfunctions in sensory processing affect motor control and internal feedback mechanisms [4,5,6,7]. Somatosensory processes of postural control and cervical sensorimotor control are impaired in CD [8,9,10] and may affect everyday activities in patients with CD as they provide postural stability and functional stability of the head and neck.
The first-line recommended treatment for CD is injection with botulinum toxin (BoNT) in the dystonic muscles [11]. Additionally, physical therapy is sometimes applied [12, 13]. The impact of first-line treatment, e.g., BoNT injections in the dystonic muscle(s), could provide relevant information for the selection of future physiotherapy modalities in the treatment of CD targeting somatosensory integration.
The neurotoxin BoNT-A targets the neuromuscular junction, blocks neuromuscular signal transmission at the motor endplate and causes alterations in peripheral sensory input [14]. Not only fewer muscle contractions are observed, afferent output from extra- and intrafusal fibers of the muscle spindles is inhibited [15, 16]. Consequently, decreased somatosensory afference from neck muscle spindles may influence central somatosensory processing of postural control, cervical sensorimotor control and perception of visual verticality since the somatosensory afference is used to construct posture and spatial orientation [17, 18]. Therefore, we would expect postural control and cervical sensorimotor control to improve after a BoNT injection and decrease when the effect of the intervention is no longer present.
This is the first study to investigate the effect of a BoNT treatment on the somatosensory processes of cervical sensorimotor control, seated postural control and perception of visual verticality. The aim of the present study was to explore whether alterations in cervical afference due to BoNT-A treatment alter somatosensory integration to normalize postural control, cervical sensorimotor control and perception of visual verticality in patients with idiopathic CD.
Methods
Participants and setting
A total of 24 consecutive patients with the diagnosis of idiopathic isolated late-onset cervical dystonia according to the current criteria [19] were recruited in a tertiary center of neurology at the Antwerp University Hospital. All patients received regular treatments of botulinum toxin injections and no additional exercise treatment targeting somatosensory integration. Patients were assessed at least 3 months after the last injection, immediately prior to a new injection of botulinum toxin when the clinical effect of the injection was no longer present. The group was followed during one treatment cycle and assessed on three occasions (see supplementary material). Patients were excluded in case of clinical features suggestive for segmental distribution of dystonia, other neurological disorders, vestibular dysfunction, or previous surgery of the cervical spine and alcohol intake in the past 24 h. For the control group of asymptomatic individuals, additional exclusion criteria were set: rheumatoid arthritis, no bothersome neck or back pain in the past 6 months and no neck or head trauma in the past 5 years.
Data of the patient group for postural control were compared to a control group of 36 asymptomatic controls. Data of subjective perception of visual verticality of the patient group were compared to a control group of 30 asymptomatic controls. For cervical sensorimotor control, data of the patient group were compared to a normative data base of 70 asymptomatic controls. The control groups were recruited through personal contacts and in hospital and university settings.
The protocol was approved by the Ethics Committee of the Antwerp University Hospital (reference 14/8/74) and the study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants provided informed consent before particpating. Recruitment took place from August 2014 to November 2015 and assessment was performed in the Multidisciplinary Motor Centre Antwerp (M2OCEAN).
Intervention and follow-up
Patients received their regular BoNT injection under electro-myographic (EMG) guidance with abobotulinumtoxinA (Dysport®, Ipsen, Biopharm SAS, Boulogne-Billancourt, France) or onabotulinumtoxinA (BOTOX®, Allergan, Inc., Irvine, CA, USA). BoNT-A dose and injected muscles were registered. The dosage of the two types of BoNT-A in Dysport® and BOTOX® is expressed in units. Muscles to treat were selected based on clinical evaluation and electro-myographic (EMG) assessment.
Baseline measurement (test 1) took place immediately prior to the BoNT treatment at least 3 months after the last injection when the effect should no longer be present [14, 20]. Test 2 took place 4 weeks after treatment when the highest treatment effect is expected [20]. The last assessment (test 3) took place 12 weeks after the treatment when the effect should no longer be present [14, 20].
Outcome measures
Disease severity
Disease-specific characteristics were obtained through one questionnaire: the Cervical Dystonia Impact Profile (CDIP-58), and one rating scale filled out by the therapist: the Toronto Western Spasmodic Rating Scale (TWSTRS). Head tremor was assessed through the subscale of the Tsui scale. The rating scales and questionnaire are all validated and recommended in the assessment of patients with CD [21]. A higher score indicates greater impairment.
The visual analogue scale (VAS) was used to evaluate pain at the time of assessment. Patients were asked to mark the level of their pain on a 100-mm, non-hatched line of which one end represents ‘no pain’ and the other ‘the worst possible pain at this moment’. The VAS is a pain assessment tool with good clinimetric properties [22] and with a minimal clinical relevant change of 10 mm [23].
Somatosensory processing or integration
Three types of somatosensory processing were assessed, e.g., cervical sensorimotor control, seated postural control and perception of visual verticality. Maintaining postural balance in stance relies predominantly on somatosensory input from the lower limbs and ankle strategy [24]. To minimize somatosensory input from the lower limbs, we assessed postural control in a seated position. To reduce the interference of fatigue, the order of testing was randomized by computer prior to testing. All assessments were conducted by the same researcher (J.D.P) in the Multidisciplinary Motor Centre Antwerp M2OCEAN.
Cervical sensorimotor control was assessed by the head repositioning accuracy (HRA) test. Measurements in 3D were obtained through an eight-camera infrared motion analysis system recording at 100 Hz (VICON® T10, Oxford Metrics, Oxford). The outcome measure for cervical sensorimotor control is the joint repositioning error (JPE) which is expressed in degrees (°) [25]. This test is proven to be valid and reliable [26]. Rigid plates with reflective markers were placed on the head and sternum. No alleviating effect was reported of the pressure of the head band in the patient group. The measurement error of the VICON® T10 system in Multidisciplinary Motor Centre Antwerp M2OCEAN is < 1° [27]. A more detailed description of marker placements and data analysis was published previously [9].
In the HRA test, blindfolded participants are instructed to relocate their head as accurately as possible to a self-determined neutral head position after performing an active movement in the two cardinal planes (flexion–extension and left–right rotation of the neck) [28]. The neutral head position for patients was equal to the dystonic head position. They were asked to perform the neck movements without using sensory tricks and within comfortable limits to avoid supplementary nociceptive input. This test was verbally explained, followed by a demonstration and performed ten times in each plane of movement. The JPE was calculated quantitatively by the absolute error (AE) and qualitatively by the constant error (CE) [25, 29]. The absolute error (AE) is the mean of the total deviation from the neutral head position over the trials [29], whereas the constant error (CE) is a measure of both direction and deviation from the neutral head position. It is calculated as the mean of the repositioning error over the trials incorporating the positive and negative values in each trial in the cardinal plane [25].
Seated postural control was assessed during quiet sitting with two embedded force plates (AMTI®, Advanced Mechanical Technology Inc., Watertown, MA). Center of pressure (CoP) displacement was measured with a sampling frequency of 1000 Hz and filtered through a fourth-order zero-phase Butterworth low-pass filter with a cut-off frequency of 10 Hz [30]. Participants were seated on a chair without back or arm rests on one force plate. Both feet were placed next to each other with the hands resting on the thighs on the adjacent force plate. The signals were processed with Vicon® software (version 1.8.5). A custom-made Matlab model (version 2016b) was written to calculate CoP parameters in which total CoP was calculated as the weighted average of the CoP displacements on the two force plates.
The following CoP parameters were calculated, as previously described by Prieto et al. [31]: range of the antero-posterior and medio-lateral displacements (mm) (range ML, range AP), sway path as distance covered by the successive positions of the moving COP (mm), the sway area (mm2) is an ellipse which encompassed 95% of the CoP distribution, the mean velocity of CoP displacements in the antero-posterior and medio-lateral direction (mm/s) (mVel ML and mVel AP). Smaller sway parameters represent better postural stability.
Three samples of 30 s were recorded with eyes closed and eyes open [32] with a 30-s rest between trials. The first 10 s of each trial were discarded to avoid non-stationarity in the start of the measurement [33].
Perception of visual verticality was obtained through the subjective visual vertical (SVV) test [34, 35], measured with the Difra vertitest type DI072010 (Difra, Belgium) with an accuracy of 0.1°. The vertitest is positioned behind the participant and projects a laser bar of approximately 1 m on an opposing white wall. Participants sat on a chair without backrest in a completely darkened room. Head position was not corrected in patients with CD, control subjects kept the head in a neutral position.
The laser bar was made invisible to the participant when the researcher set the bar in the starting roll position. The participant then rotated the laser bar to a vertical position using a remote control. The deviation in degrees (°) was noted where a clockwise (CW) deviation of the bar results in a positive SVV score and a counterclockwise (CCW) in a negative score. The fixed order of the seven starting roll positions of the laser bar in relation to the earth’s vertical was 20° CCW, 10° CW, 5° CCW, 0° (earth’s vertical), 5° CW, 10° CCW and finally 20° CW. The average of the seven trials was calculated.
Participants performed one practice trial and did not receive any feedback about their performance during the assessment. No time limits were set for the adjustments.
A head on body tilt of < 60° leads to a contralateral overestimation of the tilt in asymptomatic subjects. They compensate by setting the laser bar to a contralateral tilt of the visual vertical. This is referred to as the “E-effect” [36]. If patients with CD show an E-effect, we expect a CW deviation and positive values in patients with left laterocollis. Patients with a right laterocollis would have a negative SVV score because of the CCW deviation. When calculating a mean SVV score of patients with right or left laterocollis, this would lead to a value close to 0. Therefore, the raw SVV score of patients with left laterocollis was multiplied with − 1 to allow between-subject comparison.
Statistical analysis
Data were analyzed using SPSS® vs. 22. Shapiro–Wilks test was calculated to assess normality of data distribution. Level of significance was set at 0.05 for all analysis and corrected with a Bonferroni correction in case of multiple outcome parameters.
Non-normally distributed data were analyzed using the Friedman test to detect differences over time in the patient group. In case of significant differences on the Friedman test, a Wilcoxon test was performed to detect differences between specific time intervals. Next, to explore whether treatment effect influenced somatosensory processes over time the patient group was subdivided into responders and non-responders to BoNT treatment. Patients with an improvement of ≥ 20% on the total TWSTRS score were categorized as responders to the BoNT treatment [37]. Again, a Friedman test was used to calculate differences over time in the responder and non-responder groups.
To explore between-group differences between the group responders and non-responders, a Mann–Whitney U test was used to calculate differences in age, disease severity and disease duration. A chi-square test was used to explore differences in gender and presence of dystonic head tremor.
Changes in sensorimotor parameters following BoNT treatment were correlated to mean differences in disease characteristics, differences in cervical sensorimotor control and postural control by means of Spearman rho correlation coefficients.
Additionally, a Mann–Whitney U test was used to calculate differences between the control groups and the patient group in test 3 (12 weeks follow-up).
Results
Demographic characteristics
Baseline subject demographics of patients with CD are presented in Table 1. The age of the 20 females and 4 males ranged between 30 and 86 years with a mean of 59.2 years (± 13.9 SD). Disease severity ranged from 21.75 to 61.75/85 on the TWSTRS with a mean score of 36.07 (± 9.74 SD). The score on the CDIP-58 ranged from 25.86 to 75.86/100 with a mean score of 47.69 (± 13.79 SD). Visible dystonic head tremor was present in ten patients (41.7%). No participants were lost to follow-up.
A group of 36 asymptomatic subjects (16 men and 20 women) with a mean age of 58.9 years (± 16.6 SD) participated as the control group for postural control. For perception of visual verticality, a control group of 30 asymptomatic subjects (12 males and 18 females) participated with a mean age of 59.4 years (± 17.4 SD). The normative database for cervical sensorimotor control consisted of 70 asymptomatic controls with at least ten participants per decade (30–90 years), except for the decade + 80 years (n = 4). The age of the patient group did not differ from the control groups.
Treatment characteristics
Of the 24 patients, 18 received botulinum injection of BOTOX® and 6 received injections of Dysport® (75% and 25% of the participants, respectively). BoNT-A was injected in 2–7 different muscles with a mean of 3.8 muscles injected during one treatment session (See Table 1).
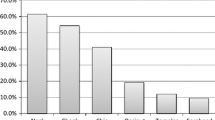
The splenius capitis muscle(s) was injected in 100% of the treatment sessions, the sternocleidomastoideus in 62.5%, the semispinalis capitis in 58.3%, the levator scapulae in 58.3%, the trapezius in 29.3% and the scalene with 4.2%.
After treatment, 14 patients were categorized as ‘responders’ and 10 as ‘non-responders’. No differences were found between the responders and non-responders for age, disease severity, disease duration and gender. The proportion of patients with dystonic head tremor was significantly higher in the non-responder group compared to the responders (χ2(1) = 8.03, p = 0.011). In the non-responder group, 72% of the patients showed a dystonic head tremor.
Disease characteristics over time
Disease severity, reflected by the mean score on the TWSTRS and CDIP-58, significantly decreased with 21.3% and 21.9%, respectively, after BoNT-A treatment (see Fig. 1) and increased from test 2 to test 3. The pain at time of assessment, measured by the VAS, significantly changed over time (p = 0.031). With a significant decrease in pain intensity in test 2 compared to baseline (p = 0.015) and a significant increase in pain from test 2 to test 3 (p = 0.017).

Evolution of disease characteristics over time. Mean score and standard deviation are presented, *significant difference between tests 1 and 2 for the mean score on the Toronto Western Spasmodic Rating Scale (TWSTRS) and Cervical Dystonia Impact Profile (CDIP-58)
Somatosensory processing over time
Cervical sensorimotor control
Patients showed impaired cervical sensorimotor control at baseline compared to the control population for all parameters except for the absolute error on return from extension.
During follow-up, the head repositioning error, calculated as the absolute and constant error, did not change over time except for the movement direction “return from flexion” in the patient group (AE ext p = 0.023, AE fl p = 0.011, AE rot left p = 0.582, AE rot right p = 0.513) (see Fig. 2 top and Table in supplementary material). The head repositioning error calculated as the constant error did not change over time (CE ext p = 0.093, CE fl p = 0.034, CE rot left p = 0.959, CE rot right p = 0.846) (see Fig. 2 bottom and Table in supplementary material). The joint position error as calculated by the absolute error and the constant error tended to decrease over time for repositioning after extension, although not significantly after Bonferroni correction.

Evolution over time of the absolute and constant joint position error. AE absoluter error (top), CE constant error (bottom), ext extension of the cervical spine, fl flexion of the cervical spine, rot rotation. Median and interquartile range are presented. The graphs depict changes in head repositioning accuracy from baseline (test 1) to 4 weeks follow-up (test 2) to 12 weeks follow-up (test 3). The CE was sig. larger in the patient group in tests 1, 2 and 3 compared to controls and in the opposite direction. Patients overshoot (e.g., surpass the neutral head position) whereas asymptomatic controls undershoot (e.g., stop before reaching the neutral head position). *Significant difference after Bonferroni correction
Both the responder and non-responder groups showed no significant changes in joint position error over time.
In test 2, the head repositioning error of patients was significantly larger in patients compared to controls for the constant error in return from every movement direction (CE ext p < 0.0001, CE fl p < 0.0001, CE rot left p = 0.002, CE rot right p < 0.0001), for the absolute error in return from left and right rotation (AE ext p = 0.046, AE fl p = 0.365, AE rot left p = 0.006, AE rot right p = 0.003).
In test 3, the head repositioning error of patients was significantly larger compared to asymptomatic controls for the constant error in return from every movement direction (CE ext p = 0.001, CE fl p < 0.0001, CE rot left p = 0.001, CE rot right p < 0.0001), and for the absolute error in return from left rotation (AE ext p = 0.729, AE fl p = 0.500, AE rot left p = 0.007, AE rot right p = 0.050).
Postural control over time
All postural control parameters in patients with CD were significantly larger at baseline compared to the control group for the patients with head tremor. In the patient group without head tremor, all postural control parameters were significantly larger at baseline compared to the control group except for the mean velocity in the medio-lateral direction.
One parameter of postural control changed over time in the patient group without head tremor: the range of the CoP displacement in the antero-posterior direction (p = 0.006). The Wilcoxon test post hoc showed that the CoP displacement in the antero-posterior direction was significantly smaller at week 12 compared to baseline in the condition eyes open (p = 0.045). No other parameter changed over time in the patient group with and without head tremor from baseline to follow-up at 4 and 12 weeks (See Fig. 3 and Table in supplementary material).

Center of pressure (CoP) displacements over time. Changes in CoP displacements in patients without head tremor (a top figure) and in patients with head tremor (b bottom figure). The graphs depict changes in CoP displacements in the eyes closed condition from baseline (test 1) to 4 weeks follow-up (test 2) to 12 weeks follow-up (test 3). Range ML range of the CoP displacement in medio-lateral direction, range AP range of the CoP displacement in antero-posterior direction, mVel ML mean velocity of the CoP displacement in medio-lateral direction, mVel AP mean velocity of the CoP displacement in antero-posterior direction, Area sway area of an ellipse that encompassed 95% of the CoP distribution, Path sway path represents distance covered by the successive positions of the moving COP. *Significant difference after Bonferroni correction
The group responders and non-responders showed no significant changes in postural sway parameters over time.
In test 3, all postural sway parameters of patients were significantly larger in patients compared to controls in the eyes open and eyes closed condition (p ranged from < 0.0001 to 0.014).
Perception of visual verticality over time
Perception of visual verticality was not different from the asymptomatic control group (p = 0.43) at baseline. This remained so through follow-up.
Discussion
In this observational study, impaired postural and cervical sensorimotor control was found in patients with idiopathic cervical dystonia at baseline. A single treatment of BoNT-A injection in patients with idiopathic cervical dystonia showed a significant beneficial effect on disease symptoms but showed little to no effect on cervical sensorimotor control, postural control or the perception of the visual vertical. Contrary to the hypothesis, the decrease in disease symptoms and pain did not result in increased postural control and cervical sensorimotor control as no correlations were found in the group of patients who showed a good treatment effect. The perception of visual verticality was well within normal ranges and remained so through the follow-up period.
The impaired postural control (e.g., increased postural sway parameters) and cervical sensorimotor control (e.g., impaired head repositioning accuracy) in CD might be attributed to dysfunctions in sensory afference from the neck as well as dysfunctions in the sensorimotor network at the level of the central nervous system. Since peripheral vestibular function seems intact as measured by the subjective visual vertical test, and previously reported by Rosengren et al. [38], the results of decreased postural stability and sensorimotor control may support the hypothesis for the involvement of the cerebellum in the pathophysiology of CD [39,40,41].
In standard care, BoNT is injected into the dystonic muscles causing local chemodenervation at the neuromuscular junction. This leads to fewer muscle contractions and a reduction in afferent sensory information [14, 15, 42, 43]. Next to the peripheral effect of BoNT, secondary central neurological changes have been observed following BoNT injection. It appears that BoNT modulates basal ganglia activity [44], decreases the loss of intracortical inhibition [45], and modulates the somatosensory cortex [46, 47] in the sensorimotor network. These mechanisms of action could affect somatosensory processes such as cervical sensorimotor control and postural control.
Our results showed a reduction of pain and other disease characteristics such as improved mobility, disability and head position following treatment with BoNT. The reduction of ≥ 20% of the total TWTRS score in our patient population was expected as a clinically relevant improvement and is comparable to other research [37, 48]. Then symptoms increased again towards baseline level at week 12 as expected due to the temporary effect of BoNT [11, 14]. The improvement in disease symptoms at week 4 is not accompanied by an increased cervical sensorimotor control or postural stability. None of the parameters from postural and cervical sensorimotor control follow the curve of the treatment effect as seen in the improvement of pain and disease severity scores on the TWSTRS and CDIP-58. Although some parameters (e.g., HRA extension and sway area) tend to gradually improve over time, they did not reach the level of the control population. Several hypotheses should be considered.
First, the presence of neck pain might affect the results since the pain matrix and the sensorimotor network show overlapping brain areas [3, 49]. In patients with aspecific chronic neck pain [50,51,52,53], impaired cervical sensorimotor control and postural control have been observed as cervical somatosensory afference contributes to postural control and sensorimotor control [17, 54,55,56]. Our results showed that pain severity decreased following BoNT treatment to increase to baseline level after 12 weeks. The reduction in neck pain did not correlate to differences in postural or cervical sensorimotor control. Therefore, we believe that pain might contribute to the sensorimotor dysfunctions but is not the sole cause.
Second, the density of muscle spindles in the injected muscles with BoNT-A is not the highest density found in neck muscles. The highest density of muscle spindles is found in suboccipital muscles and the longus colli muscle [57, 58]. These muscles are located close to the spine and were not treated in our patient group with CD. The proportion of decreased somatosensory input from the injected neck muscles could, therefore, be insufficient in normalizing cervical sensorimotor control and postural control.
Third, sensory reweighting might influence the sensorimotor processes of cervical sensorimotor control and postural control. Previous research reported that patients with CD seemingly ignore proprioceptive input from muscle spindles generated by neck muscle vibrations [8, 59]. This could explain the non-linear response of cervical sensorimotor control in patients with CD to the altered sensory afference from the neck muscle spindles following BoNT treatment. It would imply that patients downregulate the impact of proprioceptive afference in sensorimotor processes [60, 61]. The mean disease duration of our study population was 8 years; the participants could, therefore, increasingly rely on vestibular cues as proprioceptive information from the neck might be discarded as not reliable. Additionally, secondary adaptations in the sensorimotor network following BoNT treatment have been observed with functional magnetic resonance imaging such as reduced basal ganglia activation and cortical activation [3, 47]. The peripheral and secondary central effects of BoNT are apparently not sufficient to normalize cervical sensorimotor control or postural control. Moreover, the group with dystonia regularly received BoNT treatment. Therefore, it is plausible that cortical [45] or subcortical plasticity [62] would be present following the injections. This would decrease treatment effects detectable after one single BoNT injection. A botulinum toxin-naïve group of patients would provide more insight into this matter.
Fourth, a learning effect should be considered. Although a learning effect seems unlikely since the time interval between assessments was 4 and 8 weeks, in neck pain populations, a significant improvement in joint position sense was obtained after a 4–6-week interval of regular exercises two times a day [63, 64]. It is unlikely that the three assessments in this study would result in a learning effect. Nonetheless, habituation to the laboratory setting may influence the assessment as mental stress deteriorates the symptoms of dystonia [65].
Finally, the outcome measures might not be sensitive enough to detect changes. The clinimetric properties regarding the validity and reliability of the head repositioning accuracy test, as outcome for cervical sensorimotor control, have been reviewed multiple times in several patient populations where a joint repositioning error is 0.58°–1.66° larger in patient populations, depending on the measurement device used [26, 66]. The responsiveness to change, however, is not well documented [63, 67]. Posturography as outcome for postural stability in stance is widely used and is responsive to changes in time following exercise interventions [68]. However, this has not been established for posturography in a seated condition to our knowledge.
There are some limitations to this study. As no patient control group was included, this report is an observational study. We did not include a patient control group because it is ethically not preferable to deny first-line recommended treatment to patients with CD. With a year incidence of 8–12 cases per million [69], it is difficult to recruit BoNT-naive patients for a cross-over design. Future research is therefore needed to confirm the results of this study. Nevertheless, the data provide valuable baseline measurements in patients regularly treated with BoNT, not receiving additional physiotherapy targeted at postural and cervical sensorimotor control.
The results are biased by the small number of patients and high percentage of non-responder patients (40%). A cut-off of 20% improvement on the TWSTRS scale was used to allocate patients in the responder group. Some considerations can be made concerning the rather high percentage of non-responder patients. First, in the group of non-responders, 72% of the patients showed a dystonic head tremor. The measure to assess improvement, the TWSTRS, does not include tremor assessment. Therefore, the TWSTRS score cannot reflect the improvement in head tremor. These findings also reflect the difficulty of treating dystonic head tremor [70] and the limited effect of BoNT in the treatment of head tremor [71, 72]. Second, disease severity of the participants in this trial was mild to moderate. Some clinical trials preset a disease severity of 30 points on the total TWSTRS score [73] although a minimal score of 20 is also applied [74]. In our sample, 8 of the 24 patients had a TWSTRS score < 30 points. This implies little margin for improvement after treatment. Finally, two patients showed an improvement of 19% and were, therefore, included in the non-responder group although the improvement was clinically relevant. Assigning the two patients to the responder group would lower the percentage of non-responders to 33%.
In conclusion, our study found a beneficial effect of BoNT on disease severity and pain. One single BoNT intervention, however, has little to no effect on head repositioning accuracy, seated postural control or perception of visual verticality in patients with idiopathic CD. As a peripheral intervention does lead to a normalization of somatosensory integration, the results of this study confirm the impairments in different nodes of the sensorimotor network. In addition to the peripheral intervention with BoNT, a specialized exercise treatment targeting somatosensory integration might be beneficial in the standard care of patients with CD.
References
Jinnah HA, Albanese A (2014) The new classification system for the dystonias: why was it needed and how was it developed? Mov Disord Clin Pract 1:280–284. https://doi.org/10.1002/mdc3.12100
Neychev VK, Gross RE, Lehéricy S et al (2011) The functional neuroanatomy of dystonia. Neurobiol Dis 42:185–201. https://doi.org/10.1016/j.nbd.2011.01.026
Opavský R, Hluštík P, Otruba P, Kaňovský P (2011) Sensorimotor network in cervical dystonia and the effect of botulinum toxin treatment: a functional MRI study. J Neurol Sci 306:71–75. https://doi.org/10.1016/j.jns.2011.03.040
Tinazzi M, Rosso T, Fiaschi A (2003) Role of the somatosensory system in primary dystonia. Mov Disord 18:605–622. https://doi.org/10.1002/mds.10398
Tinazzi M, Fiorio M, Fiaschi A et al (2009) Sensory functions in dystonia: insights from behavioral studies. Mov Disord 24:1427–1436. https://doi.org/10.1002/mds.22490
Konczak J, Abbruzzese G (2013) Focal dystonia in musicians: linking motor symptoms to somatosensory dysfunction. Front Hum Neurosci 7:297. https://doi.org/10.3389/fnhum.2013.00297
Patel N, Jankovic J, Hallett M (2014) Sensory aspects of movement disorders. Lancet Neurol 13:583–592. https://doi.org/10.1016/S1474-4422(13)70213-8
Bove M, Brichetto G, Abbruzzese G et al (2007) Postural responses to continuous unilateral neck muscle vibration in standing patients with cervical dystonia. Mov Disord 22:498–503. https://doi.org/10.1002/mds.21357
De Pauw J, Mercelis R, Hallemans A et al (2017) Cervical sensorimotor control in idiopathic cervical dystonia: a cross-sectional study. Brain Behav. https://doi.org/10.1002/brb3.735
de Pauw J, Mercelis R, Hallemans A et al (2018) Postural control and the relation with cervical sensorimotor control in patients with idiopathic adult-onset cervical dystonia. Exp Brain Res. https://doi.org/10.1007/s00221-018-5174-x
Albanese A, Asmus F, Bhatia KP et al (2011) EFNS guidelines on diagnosis and treatment of primary dystonias. Eur J Neurol 18:5–18. https://doi.org/10.1111/j.1468-1331.2010.03042.x
De Pauw J, Van der Velden K, Meirte J et al (2014) The effectiveness of physiotherapy for cervical dystonia: a systematic literature review. J Neurol 1857–1865. https://doi.org/10.1007/s00415-013-7220-8
Prudente CN, Zetterberg L, Bring A et al (2018) Systematic review of rehabilitation in focal dystonias: classification and recommendations. Mov Disord Clin Pract 0:1–9. https://doi.org/10.1002/mdc3.12574
Jankovic J (2017) Botulinum toxin: state of the art. Mov Disord 32:1131–1138. https://doi.org/10.1002/mds.27072
Rosales RL, Dressler D (2010) On muscle spindles, dystonia and botulinum toxin. Eur J Neurol 17(Suppl 1):71–80. https://doi.org/10.1111/j.1468-1331.2010.03056.x
Trompetto C, Currà A, Buccolieri A et al (2006) Botulinum toxin changes intrafusal feedback in dystonia: a study with the tonic vibration reflex. Mov Disord 21:777–782. https://doi.org/10.1002/mds.20801
Kristjansson E, Treleaven J (2009) Sensorimotor function and dizziness in neck pain: implications for assessment and management. J Orthop Sports Phys Ther 39:364–377. https://doi.org/10.2519/jospt.2009.2834
Clemens IAH, De Vrijer M, Selen LPJ et al (2011) Multisensory processing in spatial orientation: an inverse probabilistic approach. J Neurosci 31:5365–5377. https://doi.org/10.1523/JNEUROSCI.6472-10.2011
Albanese A, Bhatia K, Bressman SB et al (2013) Phenomenology and classification of dystonia: a consensus update. Mov Disord 28:863–873. https://doi.org/10.1002/mds.25475
Odergren T, Hjaltason H, Kaakkola S et al (1998) A double blind, randomised, parallel group study to investigate the dose equivalence of Dysport and Botox in the treatment of cervical dystonia. J Neurol Neurosurg Psychiatry 64:6–12. https://doi.org/10.1136/jnnp.64.1.6
Albanese A, Del Sorbo F, Comella C et al (2013) Dystonia rating scales: critique and recommendations. Mov Disord 28:874–883. https://doi.org/10.1002/mds.25579
Hawker GA, Mian S, Kendzerska T, French M (2011) Measures of adult pain: visual analog scale for pain (VAS pain), numeric rating scale for pain (NRS pain), McGill pain questionnaire (MPQ), short-form McGill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form-36 bodily pain scale (SF). Arthritis Care Res 63:240–252. https://doi.org/10.1002/acr.20543
Kelly AM (2001) The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emerg Med J 18:205–207
Gatev P, Thomas S, Kepple T, Hallett M (1999) Feedforward ankle strategy of balance during quiet stance in adults. J Physiol 514:915–928. https://doi.org/10.1111/j.1469-7793.1999.915ad.x
Hill R, Jensen P, Baardsen T et al (2009) Head repositioning accuracy to neutral: a comparative study of error calculation. Man Ther 14:110–114. https://doi.org/10.1016/j.math.2008.02.008
Michiels S, De Hertogh W, Truijen S et al (2013) The assessment of cervical sensory motor control: a systematic review focusing on measuring methods and their clinimetric characteristics. Gait Posture 38:1–7. https://doi.org/10.1016/j.gaitpost.2012.10.007
Sanders K, Vereeck LHA (2012) Reliability of VICON measurements. Antwerp Univ. https://doi.org/10.1017/CBO9781107415324.004
Revel M, Andre-Deshays C, Minguet M (1991) Cervicocephalic kinesthetic sensibility in patients with cervical pain. Arch Phys Med Rehabil 72:288–291
Treleaven J, Jull G, Sterling M (2003) Dizziness and unsteadiness following whiplash injury: characteristic features and relationship with cervical joint position error. J Rehabil Med 35:36–43
Latash ML, Ferreira SS, Wieczorek SA, Duarte M (2003) Movement sway: changes in postural sway during voluntary shifts of the center of pressure. Exp Brain Res 150:314–324. https://doi.org/10.1007/s00221-003-1419-3
Prieto TE, Myklebust JB, Hoffmann RG et al (1996) Measures of postural steadiness: differences between healthy young and elderly adults. IEEE Trans Biomed Eng 43:956–966. https://doi.org/10.1109/10.532130
Duarte M, Freitas SM (2010) Revision of posturography based on force plate for balance evaluation. Rev Bras Fisioter 14:183–192
Carpenter MG, Frank JS, Winter D, Peysar GW (2001) Sampling duration effects on centre of pressure summary measures. Gait Posture 13:35–40
Saeys W, Vereeck L, Bedeer A et al (2010) Suppression of the E-effect during the subjective visual and postural vertical test in healthy subjects. Eur J Appl Physiol 109:297–305. https://doi.org/10.1007/s00421-010-1355-4
Saeys W, Vereeck L, Truijen S et al (2012) Influence of sensory loss on the perception of verticality in stroke patients. Disabil Rehabil 34:1965–1970. https://doi.org/10.3109/09638288.2012.671883
Müller G (1916) Über das Aubertsche phänomen. Z Sinnesphysiol 49:109–246
Zoons E, Dijkgraaf MGW, Dijk JM et al (2012) Botulinum toxin as treatment for focal dystonia: a systematic review of the pharmaco-therapeutic and pharmaco-economic value. J Neurol 259:2519–2526. https://doi.org/10.1007/s00415-012-6510-x
Rosengren SM, Colebatch JG (2010) Vestibular evoked myogenic potentials are intact in cervical dystonia. Mov Disord 25:2845–2853. https://doi.org/10.1002/mds.23422
Malone A, Manto M, Hass C (2014) Dissecting the links between cerebellum and dystonia. Cerebellum 13:666–668. https://doi.org/10.1007/s12311-014-0601-4
Filip P, Lungu OV, Bareš M (2013) Dystonia and the cerebellum: a new field of interest in movement disorders? Clin Neurophysiol 124:1269–1276. https://doi.org/10.1016/j.clinph.2013.01.003
Prudente CN, Hess EJ, Jinnah HA (2014) Dystonia as a network disorder: what is the role of the cerebellum? Neuroscience 260:23–35. https://doi.org/10.1016/j.neuroscience.2013.11.062
Kaňovský P, Rosales RL (2011) Debunking the pathophysiological puzzle of dystonia–with special reference to botulinum toxin therapy. Parkinsonism Relat Disord 17(Suppl 1):S11–S14. https://doi.org/10.1016/j.parkreldis.2011.06.018
Jankovic J (2004) Botulinum toxin in clinical practice. J Neurol Neurosurg Psychiatry 75:951–957. https://doi.org/10.1136/jnnp.2003.034702
Dresel C, Bayer F, Castrop F et al (2011) Botulinum toxin modulates basal ganglia but not deficient somatosensory activation in orofacial dystonia. Mov Disord 26:1496–1502. https://doi.org/10.1002/mds.23497
Gilio F, Curra A, Lorenzano C et al (2000) Effects of botulinum toxin type A on intracortical inhibition in patients with dystonia. Ann Neurol 48:20–26
Kafiovskf P, Streitovb H, Dufek J et al (1998) Change in lateralization of the P22/N30 cortical component of median nerve somatosensory evoked potentials in patients with cervical dystonia after successful treatment with botulinum toxin A. 108–117
Delnooz CCS, Pasman JW, Beckmann CF, van de Warrenburg BPC (2013) Task-free functional MRI in cervical dystonia reveals multi-network changes that partially normalize with botulinum toxin. PLoS One 8:e62877. https://doi.org/10.1371/journal.pone.0062877
Duarte GS, Castelão M, Rodrigues FB et al (2016) Botulinum toxin type A versus botulinum toxin type B for cervical dystonia. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD004314.pub3
Iannetti GD, Mouraux A (2010) From the neuromatrix to the pain matrix (and back). Exp Brain Res 205:1–12. https://doi.org/10.1007/s00221-010-2340-1
Treleaven J (2008) Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man Ther 13:2–11. https://doi.org/10.1016/j.math.2007.06.003
Palmgren PJ, Andreasson D, Eriksson M, Hägglund A (2009) Cervicocephalic kinesthetic sensibility and postural balance in patients with nontraumatic chronic neck pain–a pilot study. Chiropr Osteopat 17:6. https://doi.org/10.1186/1746-1340-17-6
Vuillerme N, Pinsault N (2009) Experimental neck muscle pain impairs standing balance in humans. Exp Brain Res 192:723–729. https://doi.org/10.1007/s00221-008-1639-7
Stanton TR, Leake HB, Chalmers KJ et al (2016) Evidence of impaired proprioception in chronic, idiopathic neck pain: systematic review and meta-analysis. Phys Ther 96:876–887. https://doi.org/10.2522/ptj.20150241
Bove M, Fenoggio C, Tacchino a et al (2009) Interaction between vision and neck proprioception in the control of stance. Neuroscience 164:1601–1608. https://doi.org/10.1016/j.neuroscience.2009.09.053
Röijezon U, Clark NC, Treleaven J (2015) Proprioception in musculoskeletal rehabilitation. Part 1: basic science and principles of assessment and clinical interventions. Man Ther 20:368–377. https://doi.org/10.1016/j.math.2015.01.008
Falla D, Farina D (2008) Neuromuscular adaptation in experimental and clinical neck pain. J Electromyogr Kinesiol 18:255–261. https://doi.org/10.1016/j.jelekin.2006.11.001
Kulkarni V, Chandy MJ, Baby KS (2001) Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurol India 49:355
Boyd-Clark LC, Briggs C, Galea MP (2002) Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine (Phila Pa 1976) 27:694–701. https://doi.org/10.1097/00007632-200204010-00005
Wöber E, Schnider P, Steinhoff N et al (1999) Posturographic findings in patients with idiopathic cervical dystonia before and after local injections with botulinum toxin. Eur Neurol 41:194–200
Peterka RJ, Loughlin PJ (2004) Dynamic regulation of sensorimotor integration in human postural control. J Neurophysiol 91:410–423. https://doi.org/10.1152/jn.00516.2003
Peterka RJ (2002) Sensorimotor integration in human postural control. J Neurophysiol 88:1097–1118. https://doi.org/10.1152/jn.00605.2001
Blood AJ, Tuch DS, Makris N et al (2006) White matter abnormalities in dystonia normalize after botulinum toxin treatment. Neuroreport 17:1251–1255. https://doi.org/10.1097/01.wnr.0000230500.03330.01.White
Jull G, Falla D, Treleaven J et al (2007) Retraining cervical joint position sense: the effect of two exercise regimes. J Orthop Res 404–412. https://doi.org/10.1002/jor
Humphreys BK, Irgens PM (2002) The effect of a rehabilitation exercise program on head repositioning accuracy and reported levels of pain in chronic neck pain subjects. J Whiplash Relat Disord 1:99–112. https://doi.org/10.3109/J180v01n01_09
Jahanshahi M (2000) Factors that ameliorate or aggravate spasmodic torticollis. J Neurol Neurosurg Psychiatry 68:227–229
de Vries J, Ischebeck BK, Voogt LP et al (2015) Joint position sense error in people with neck pain: a systematic review. Man Ther 20:736–744. https://doi.org/10.1016/j.math.2015.04.015
Humphreys BK (2008) Cervical outcome measures: testing for postural stability and balance. J Manipulative Physiol Ther 31:540–546. https://doi.org/10.1016/j.jmpt.2008.08.007
Low DC, Walsh GS, Arkesteijn M (2017) Effectiveness of exercise interventions to improve postural control in older adults: a systematic review and meta-analyses of centre of pressure measurements. Sport Med 47:101–112. https://doi.org/10.1007/s40279-016-0559-0
Defazio G, Jankovic J, Giel JL, Papapetropoulos S (2013) Descriptive epidemiology of cervical dystonia. Tremor Other Hyperkinet Mov (N Y). doi: tre-03-193-4374-2 [pii]
Jost WH, Tatu L (2015) Selection of muscles for botulinum toxin injections in cervical dystonia. Mov Disord Clin Pract 2:224–226. https://doi.org/10.1002/mdc3.12172
Hallett M, Albanese A, Dressler D et al (2013) Evidence-based review and assessment of botulinum neurotoxin for the treatment of movement disorders. Toxicon 67:94–114. https://doi.org/10.1016/j.toxicon.2012.12.004
Simpson DM, Blitzer A, Brashear A et al (2008) Assessment: Botulinum neurotoxin for the treatment of movement disorders (an evidence-based review): report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 70:1699–1706. https://doi.org/10.1007/s00394-015-0841-1.A
Mordin M, Masaquel C, Abbott C, Copley-Merriman C (2014) Factors affecting the health-related quality of life of patients with cervical dystonia and impact of treatment with abobotulinumtoxinA (Dysport): results from a randomised, double-blind, placebo-controlled study. BMJ Open 4:e005150. https://doi.org/10.1136/bmjopen-2014-005150
Comella CL, Jankovic J, Truong DD et al (2011) Efficacy and safety of incobotulinumtoxinA (NT 201, XEOMIN®, botulinum neurotoxin type A, without accessory proteins) in patients with cervical dystonia. J Neurol Sci 308:103–109. https://doi.org/10.1016/j.jns.2011.05.041
Acknowledgements
This study was performed at and with support from the Multidisciplinary Motor Centre Antwerp (M2OCEAN) that was established by means of a Hercules Grant type 2 for medium-sized research infrastructure from the Flemish Research Council (AUHA/09/006).
Funding
University Antwerp (G815).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
No conflict of interest is to be reported.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
De Pauw, J., Cras, P., Truijen, S. et al. The effect of a single botulinum toxin treatment on somatosensory processing in idiopathic isolated cervical dystonia: an observational study. J Neurol 265, 2672–2683 (2018). https://doi.org/10.1007/s00415-018-9045-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-018-9045-y