
Abstract
Multiple Sclerosis (MS) results in color vision impairment regardless of optic neuritis (ON). The exact location of injury remains undefined. The objective of this study is to identify the region leading to dyschromatopsia in MS patients’ NON-eyes. We evaluated Spearman correlations between color vision and measures of different regions in the afferent visual pathway in 106 MS patients. Regions with significant correlations were included in logistic regression models to assess their independent role in dyschromatopsia. We evaluated color vision with Hardy–Rand–Rittler plates and retinal damage using Optical Coherence Tomography. We ran SIENAX to measure Normalized Brain Parenchymal Volume (NBPV), FIRST for thalamus volume and Freesurfer for visual cortex areas. We found moderate, significant correlations between color vision and macular retinal nerve fiber layer (rho = 0.289, p = 0.003), ganglion cell complex (GCC = GCIP) (rho = 0.353, p < 0.001), thalamus (rho = 0.361, p < 0.001), and lesion volume within the optic radiations (rho = –0.230, p = 0.030). Only GCC thickness remained significant (p = 0.023) in the logistic regression model. In the final model including lesion load and NBPV as markers of diffuse neuroaxonal damage, GCC remained associated with dyschromatopsia [OR = 0.88 95 % CI (0.80–0.97) p = 0.016]. This association remained significant when we also added sex, age, and disease duration as covariates in the regression model. Dyschromatopsia in NON-eyes is due to damage of retinal ganglion cells (RGC) in MS. Color vision can serve as a marker of RGC damage in MS.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The perception of color begins when cones, photoreceptor cells sensitive to red, green, and blue light, detect incoming light spectra and transmit this information to bipolar and retinal ganglion cells (RGCs). These signals continue along the color vision pathway until they ultimately reach parvocellular and koniocellular neurons in the lateral geniculate nucleus (LGN). Axons of the LGN neurons form optic radiations (OR) and project to the primary visual cortex (V1). After this, color signals are further propagated to cortical areas beyond V1, specifically the secondary visual cortex (V2) and associative visual cortex regions such as fusiform and lingual gyrus (see Fig. 1) [1, 2].

The color vision pathway. The perception of color begins when cones, photoreceptor cells sensitive to red, green, and blue light, detect incoming light spectra. Cones are mainly present in the central five degrees of the retina with an even distribution regarding each color type (20 red, 40 green, one blue), but blue cones are more peripherally distributed. Cones transmit this information to bipolar and retinal ganglion cells (RGCs). RGCs axons form the optic nerve, optic chiasm, and optic tract, and finally project to the parvocellular (red-green) and koniocellular (blue-yellow) neurons in the lateral geniculate nucleus (LGN). Axons of the LGN neurons form optic radiations (OR) and project to the primary visual cortex (V1). After this, color signals are further propagated to cortical areas beyond V1, specifically the secondary visual cortex (V2) and associative visual cortex regions such as fusiform and lingual gyrus
Axonal loss in Multiple Sclerosis (MS) patients has been reported in the retina, optic nerve, optic chiasm, optic tract, LGN, optic radiations (OR), and both primary and associative visual cortex regions. Taken together, these findings indicate that MS can lead to damage along the entire color vision pathway [3–5]. However, while dyschromatopsia is well documented in MS patients, even in those without a history of Acute Optic Neuritis (AON) [6, 7], the precise site of injury producing color vision impairment remains unknown. The strong correlation between quantitative color vision assessment scores and Optical Coherence Tomography (OCT) retinal measurements suggests that the primary process underlying acquired dyschromatopsia in MS patients is damage to the anterior visual pathway [8]. Nevertheless, no studies have examined which other structures may have an influence on color vision impairment, such as those in the posterior or associative visual pathways. Thus, these results do not exclude the possibility that damage to such regions also contributes to color vision impairment in MS [8]. It is also possible that this strong association actually reflects secondary retinopathy due to retrograde axonal degeneration, such as in cases of undiagnosed subclinical AON.
In this study, we sought to pinpoint the location of the injury leading to dyschromatopsia in MS patients’ eyes without a previous history of AON (MS-NON-eyes). Identification of the region leading to color vision impairment can be used to improve bedside prognosis tools and can provide a new end-point for clinical trials aimed at preventing disability accumulation and advancing neuroprotection.
Methods
Study design
The MS-VisualPath cohort is an ongoing prospective study of patients with MS conducted at the Hospital Clinic of Barcelona (Spain). The Research Ethics Committee of the Hospital Clinic of Barcelona approved the study and all participants provided written informed consent prior to enrollment. The design and methods of the MS-VisualPath cohort have previously been described in detail [9]. We included MS patients according to McDonalds Criteria [Criteria 2005 and 2010] without any psychiatric, neurological, or ocular disorders that may interfere with the aims of the study. As of April 2015, 120 patients were included in the MS-VisualPath Cohort. Eight patients were excluded for having prior history of AON in both eyes (no fellow eye available for analysis), two patients were excluded for congenital dyschromatopsia, three patients did not have OCT segmentation performed, and one patient had not yet undergone Magnetic Resonance Imaging (MRI) analysis at the time this study began. Thus, 106 patients of the cohort were included in this study.
Clinical evaluation
We collected demographic (sex and age) and MS-related variables (onset and diagnosis date, disease type and duration, AON history, MS treatment, and clinical disability). The presence of prior AON was assessed in the subject’s Electronical Medical Record, using the criteria from the Optic Neuritis Treatment Trial [10] and confirmed by careful ophthalmological assessment, MRI of the optic nerve (T2 sequence), and/or by identifying significant asymmetry in the retinal nerve fiber layer (RNFL) by OCT and in the mean deviation of the visual field. A mean plus 1 standard deviation of the inter-ocular asymmetry of registered AON cases was set as the cutoff point for abnormality. We have previously used this approach to rule out subclinical AON episodes that would have a large impact on OCT and visual outcomes [11].
Color vision assessment
Color vision was tested in each eye independently using Hardy, Rand, and Rittler (HRR) pseudoisochromatic plates. The test includes three types of plates, beginning with 4 (1–4) non-scored demonstration plates. There are 6 (5–10) scored screening plates with a total of 10 symbols designed to classify eyes as either having normal color vision or dyschromatopsia. The final 14 plates (11–24), with a total of 26 symbols, are scored plates that serve as type and severity assessment. For this study, color vision outcome was measured quantitatively based on the number of correctly identified symbols in the 20 scored HRR plates, with a maximum of 36 symbols. Furthermore, color vision was qualitatively estimated based on the number of symbols correctly identified in the screening plates. As previously described, we used two errors as cutoff points to ensure a sensitivity of 1.0 [12]. Two or more errors in the NON-eye served to classify the patient as having dyschromatopsia. Further information about how HRR pseudoisochromatic plates can be used to assess color vision in MS has been described in detail [9].
Optical coherence tomography
We performed spectral domain retinal OCT (Spectralis; Heidelberg Engineering, Carlsbad, CA) as previously described [9]. Using the 6.0c version of the Spectralis segmentation algorithm, we quantified layer thickness from the macular acquisition of the macular RNFL, macular ganglion cell complex (GCL + IPL), macular inner nuclear layer (INL), macular outer complex (OPL + ONL), and macular Photoreceptors (PHR), including inner and outer segments of photoreceptors. Thicknesses were calculated as the mean value of both eyes except for patients with a history of AON, where only the fellow eye was included.
Magnetic resonance imaging
The MRIs were performed using a 3T scanner (Trim Trio; Siemens, Malvem, PA, USA). For this study, we obtained a 3-dimensional structural T1-weighted magnetization-prepared rapid acquisition gradient echo (MPRAGE) sequence. T1 lesion masks were manually created from T1-MPRAGE scans via ITK-SNAP software [13]. To avoid pixel misclassification after creation of the T1 lesion mask [14], we applied lesion filling [FSL] and thereafter a fully automated FIRST and SIENAX segmentation/registration tool to quantify thalamus volume (FIRST) and Normalized Brain Parenchymal (NBPV), Gray Matter (NGMV), and White Matter Volume (NWMV). We used Freesurfer to evaluate the volume of primary, secondary, and associative visual cortical areas that have been connected to color vision (Freesurfer). The Brodmann Area Maps (BA Maps) atlas from Freesurfer was used for primary (V1 = BA17) and secondary (V2 = BA18) visual cortex volume quantification [15]. We employed the Desikan-Killiany Atlas for lingual and fusiform volume assessment [16]. Lingual and fusiform areas have been previously identified as visual color processing areas [17, 18]. The Jülich probabilistic MRI atlas was used to obtain binary masks of the OR [19]. We calculated lesion load in the T1-MPRAGEs and lesion volume within the OR by counting the number of lesion voxels within the brain and OR masks, respectively.
Statistical analysis
We first performed descriptive statistics to characterize the sample with absolute numbers and proportions for qualitative variables and means and standard deviations for quantitative variables. HRR score does not have a normal distribution (Kolmogorov–Smirnov test to compare HRR distribution with a reference normal distribution test p < 0.001). Next, we evaluated associations between color vision outcome by HRR and OCT and MRI measurements of visual cortex regions using the Spearman Rank correlations. Parameters that reached statistical significance were included as independent variables in a logistic regression model to evaluate the independent role each plays in predicting color vision impairment. Two-tailed p-values <0.05 were considered statistically significant. All analyses were performed with the Statistical Package IBM-SPSS (SPSS Inc. Chicago, IL, USA) software version 20.0.
Results
Demographic and MS-related features of Study population
We studied a cohort of 106 MS patients (Table 1), mainly composed of relapsing-remitting MS (RRMS) mildly disabled patients (mean Annualized Rate of Relapse (ARR) 2 years prior to study of 0.35 and an average Expanded Disability Status Scale (EDSS) lower than 2). The mean disease duration from MS onset to study inclusion was 8.67 years. 17 (16 %) out of 106 patients suffered dyschromatopsia in the NON-eye and the mean HRR score of the population was 35.36 (range 24.5–36).
Correlations between color vision and retinal thickness by OCT
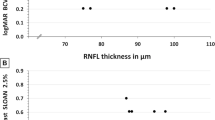
We began by using OCT Raster scan measurements to determine the correlation between HRR color vision scores and retinal layer thickness in NON-eyes (Table 2). We found a moderate yet significant positive correlation with the macular RNFL (rho = 0.289, p = 0.003), and GCC (rho = 0.353, p < 0.001). There were no significant correlations between color vision impairment and the thickness of the INL, outer complex layer (OCL), or PHR.
Correlations between color vision and brain volumes by MRI
After evaluating the association between color vision impairment and retinal layer thickness, we used MRI to assess the correlation between HRR scores and volumes of the thalamus, primary and secondary visual cortex cortical areas, and associative visual areas that have been shown to play a role in color information processing such as the fusiform and lingual gyrus. We found a positive correlation with thalamus volume (rho = 0.361, p < 0.001). We did not find any correlations in the primary, secondary, and associative visual areas. We found a negative correlation between HRR score and lesion volume within ORs (rho = −0.230 p = 0.030) (Table 3).
Risk of dyschromatopsia by retinal and brain damage
We ran a logistic regression model to assess the independent role of retinal damage and brain damage in the development of dyschromatopsia in NON-eyes with MS. In this model including GCC thickness, thalamus volume, and lesions within the ORs, only GCC thickness remained statistically significant [OR = 0.89 95 % CI (0.81–0.98) p = 0.023]. When we added disease duration, age, and sex also as covariates to the previous model, the results were similar and only GCC thickness was statistically associated with dyschromatopsia [OR = 0.89 95 % CI (0.81–0.99) p = 0.049].
HRR scores have been linked to disease severity and neuroaxonal damage [6]. Moreover, Saidha S and colleagues have recently described that retinal atrophy parallels brain atrophy [20]. Our results are in line with their findings, the Pearson correlation coefficient between GCC thickness and NBPV was r = 0.40 (p < 0.001) and r = 0.36 (p < 0.001), when we adjusted for age, disease duration and sex. We ran another model including GCC thickness, global lesion load, and NBPV to assess the role GCC thickness plays in the development of dyschromatopsia independently of these parameters, which generally serve as markers of diffuse neuroaxonal damage. Both GCC thickness [b = −0.123 OR = 0.88 95 % CI (0.80–0.97) p = 0.016] and NBPV [b = −0.008 OR = 0.99 95 % CI (0.98–1.00) p = 0.046] were independently associated with a lower probability of dyschromatopsia. When we included disease duration, age and sex also as covariates to the previous model, only GCC thickness remained significant [b = −0.121 OR = 0.88 95 % CI (0.80–0.98) p = 0.022].
These models predict that a MS patient with a GCC one micron thinner in a NON-eye has a 12 % [(1 − 0.88) × 100 = 12] greater risk of dyschromatopsia than a MS patient with a one micron thicker GCC. The odds ratio for five microns thinner GCC was estimated as follows: OR = e−0.123 × 5 = 0.54. Thus, a five microns GCC thinning in NON-eyes of MS patients results in a 46 % greater risk of color vision impairment.
Discussion
In this study, we found statistically significant correlations between color vision outcome and macular RNFL and GCC thicknesses, thalamus volume, and lesion load within optic radiations in NON-eyes of MS patients. However, when we controlled for brain volumes, only macular GCC thickness was independently associated with a higher probability of dyschromatopsia. This association remained significant after including T1-MPRAGE lesion load and NBPV as markers of diffuse neuroaxonal damage. We did not find any associations between color vision outcomes and the primary, secondary, and associative visual cortex. These results suggest that damage of RGC in the macula drives dyschromatopsia in MS NON-eyes.
The visual pathway is highly susceptible to damage in MS. Thus, it is not surprising that visual dysfunction has been ranked as the second leading cause of loss of quality of life by MS patients [21]. However, commonly used disability scales such as EDSS and Multiple Sclerosis Functional Composite do not adequately capture this key dimension from the patient’s perspective. For this reason, it is important to include a visual function test in clinical practice. Color vision was assessed using HRR plates because they are fast, easily administered at bedside, and have been found to be a more sensitive and accurate tool for color vision assessment, including the yellow and blue axis, than standard tests such as the Ishihara pseudoisochromatic plates [12, 22].
Our results revealed a significant, positive correlation between HRR color vision scores and macular RNFL [axons of RGC] and GCC [soma and dendrites of RGC] OCT thickness measurements. Moreover, we found that macular GCC thinning led to a risk of dyschromatopsia in MS. These results suggest that the loss of RGC spurs color vision impairment in MS and support previous findings that RGC damage is a driving factor in MS visual loss pathogenesis in terms of high and low contrast visual acuity [23]. Furthermore, the lack of correlation between color vision impairment and the thicknesses of the OCL and PHR layers, neither of which include RGC, supports this conclusion as well as our previous finding that foveal measurement that is characterized by the absence of ganglion cells is not associated with color vision outcomes [8].
In order to exclude other possible explanations for color impairment in MS NON-eyes, we performed MRI segmentation analysis to examine the relationship between HRR score and the volumes of other regions involved in the color vision pathway. We found a positive association with thalamus volume (including the LGN) and a negative association with lesion load within the ORs. However, these correlations with dyschromatopsia did not remain statistically significant in the logistic regression model. We did not find any correlations with the primary, secondary, or associative visual cortex. Some authors have suggested that occipital–temporal regions, including the lingual and fusiform regions, are involved in color vision processing [17, 18, 24], whereas other results did not support this role [25]. Nevertheless, these results confirm that damage to the anterior visual pathway is responsible for dyschromatopsia in MS NON-eyes and rule out injury to posterior or accessory pathways as contributing factors.
Given that dyschromatopsia has been linked to disease severity and markers of diffuse neuroaxonal damage [6], we assessed the role of GCC thickness in dyschromatopsia development in MS independently of NBPV and T1 MPRAGE lesion load. We found that preserving one micron in GCC thickness was associated with a 12 % lower probability of color vision impairment.
Our study presents some limitations. First, we did not differentiate between red-green and blue-yellow color deficiency and therefore cannot speak to potential differences in their acquisition. However, prior studies have not established a standard pattern of color vision impairment in MS. Future studies should seek to better understand the differences between these two deficiencies. Second, while HRR plates can confidently be used to detect red-green and blue-yellow color deficiency, they are designed as a screening test and more precise evaluation of severity requires further assessment via the D-15 and FM-100 tests or anomaloscope analyses [12].
Ultimately, our results show that dyschromatopsia in MS NON-eyes is specifically associated with RGC damage. These results suggest that color vision impairment can serve as an accurate marker of retinal, normal-appearing gray matter damage in MS [RGC]. It can also help evaluate GCC damage in MS independently of AON. These findings have clinical implications; while administering an OCT requires a specialized technician and expensive machinery, the HRR color vision assessment takes 5 min and can easily be administered bedside. Furthermore, now that we have pinpointed the cause of acquired dyschromatopsia in MS, we can apply this information to monitor central nervous system damage in MS patients and use color vision as a clinical outcome in trials aimed at preserving retina tissue and function.
References
Solomon SG, Lennie P (2007) The machinery of colour vision. Nat Rev Neurosci 8:276–286
Gegenfurtner KR (2003) Cortical mechanisms of colour vision. Nat Rev Neurosci 4:563–572
Evangelou N, Konz D, Esiri MM, Smith S, Palace J, Matthews PM (2001) Size-selective neuronal changes in the anterior optic pathways suggest a differential susceptibility to injury in multiple sclerosis. Brain 124:1813–1820
Sepulcre J, Goñi J, Masdeu JC, Bejarano B, Vélez de Mendizábal N, Toledo JB, Villoslada P (2009) Contribution of white matter lesions to gray matter atrophy in multiple sclerosis: evidence from voxel-based analysis of T1 lesions in the visual pathway. Arch Neurol 66:173–179
Castro SMC, Damasceno A, Damasceno BP, Vasconcellos JP, Reis F, Iyeyasu JN, Carvalho KM (2013) Visual pathway abnormalities were found in most multiple sclerosis patients despite history of previous optic neuritis. Arq Neuropsiquiatr 71:437–441
Martínez-Lapiscina EH, Ortiz-Pérez S, Fraga-Pumar E, Martínez-Heras E, Gabilondo I, Llufriu S, Bullich S, Figueras M, Saiz A, Sánchez-Dalmau B, Villoslada P (2014) Colour vision impairment is associated with disease severity in multiple sclerosis. Mult Scler 20:1207–1216
Moura ALDA, Teixeira RAA, Oiwa NN, Costa MF, Feitosa-Santana C, Callegaro D, Hamer RD, Ventura DF (2008) Chromatic discrimination losses in multiple sclerosis patients with and without optic neuritis using the Cambridge Colour Test. Vis Neurosci 25:463–468
Villoslada P, Cuneo A, Gelfand J, Hauser SL, Green A (2012) Color vision is strongly associated with retinal thinning in multiple sclerosis. Mult Scler 18:991–999
Martínez-Lapiscina EH, Fraga-Pumar E, Gabilondo I, Martínez-Heras E, Torres-Torres R, Ortiz-Pérez S, Llufriu S, Tercero A, Andorra M, Roca MF, Lampert E, Zubizarreta I, Saiz A, Sanchez-Dalmau B, Villoslada P (2014) The multiple sclerosis visual pathway cohort: understanding neurodegeneration in MS. BMC Res Notes 7:910
Cleary PA, Beck RW, Anderson MM, Kenny DJ, Backlund JY, Gilbert PR (1993) Design, methods, and conduct of the Optic Neuritis Treatment Trial. Control Clin Trials 14:123–142
Gabilondo I, Martínez-Lapiscina EH, Martínez-Heras E, Fraga-Pumar E, Llufriu S, Ortiz S, Bullich S, Sepulveda M, Falcon C, Berenguer J, Saiz A, Sanchez-Dalmau B, Villoslada P (2014) Trans-synaptic axonal degeneration in the visual pathway in multiple sclerosis. Ann Neurol 75:98–107
Cole BL, Lian KY, Lakkis C (2006) The new Richmond HRR pseudoisochromatic test for colour vision is better than the Ishihara test. Clin Exp Optom 89:73–80
Yushkevich PA, Piven J, Hazlett HC, Smith RG, Ho S, Gee JC, Gerig G (2006) User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. Neuroimage 31:1116–1128
Sdika M, Pelletier D (2009) Nonrigid registration of multiple sclerosis brain images using lesion inpainting for morphometry or lesion mapping. Hum Brain Mapp 30:1060–1067
Fischl B, Rajendran N, Busa E, Augustinack J, Hinds O, Yeo BT, Mohlberg H, Amunts K, Zilles K (2008) Cortical folding patterns and predicting cytoarchitecture. Cereb Cortex 18:1973–1980
Desikan RS, Ségonne F, Fischl B, Quinn BT, Dickerson BC, Blacker D, Buckner RL, Dale AM, Maguire RP, Hyman BT, Albert MS, Killiany RJ (2006) An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 31:968–980
Zeki S, Watson JD, Lueck CJ, Friston KJ, Kennard C, Frackowiak RS (1991) A direct demonstration of functional specialization in human visual cortex. J Neurosci 11:641–649
Beauchamp MS, Haxby JV, Jennings JE, DeYoe EA (1999) An fMRI version of the farnsworth-munsell 100-hue test reveals multiple color-selective areas in human ventral occipitotemporal cortex. Cereb Cortex 9:257–263
Eickhoff SB, Stephan KE, Mohlberg H, Grefkes C, Fink GR, Amunts K, Zilles K (2005) A new SPM toolbox for combining probabilistic cytoarchitectonic maps and functional imaging data. Neuroimage 25:1325–1335
Saidha S, Al-Louzi O, Ratchford JN, Bhargava P, Oh J, Newsome SD, Prince JL, Pham D, Roy S, van Zijl P, Balcer LJ, Frohman EM, Reich DS, Crainiceanu C, Calabresi PA (2015) Optical coherence tomography reflects brain atrophy in MS: a four year study. Ann Neurol. doi:10.1002/ana.24487
Heesen C, Böhm J, Reich C, Kasper J, Goebel M, Gold SM (2008) Patient perception of bodily functions in multiple sclerosis: gait and visual function are the most valuable. Mult Scler 14:988–991
Huna-Baron R, Glovinsky Y, Habot-Wilner Z (2013) Comparison between Hardy-Rand-Rittler 4th edition and Ishihara color plate tests for detection of dyschromatopsia in optic neuropathy. Graefes Arch Clin Exp Ophthalmol 251:585–589
Walter SD, Ishikawa H, Galetta KM, Sakai RE, Feller DJ, Henderson SB, Wilson JA, Maguire MG, Galetta SL, Frohman E, Calabresi PA, Schuman JS, Balcer LJ (2012) Ganglion cell loss in relation to visual disability in multiple sclerosis. Ophthalmology 119:1250–1257
Hansen KA, Kay KN, Gallant JL (2007) Topographic organization in and near human visual area V4. J Neurosci 27:11896–11911
Heywood CA, Gadotti A, Cowey A (1992) Cortical area V4 and its role in the perception of color. J Neurosci 12:4056–4065
Acknowledgments
We are extremely grateful to the MS-VisualPath participants and fieldworkers without whose contribution this study would not be possible.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
PV has received consultancy fees from Heidelberg Engineering regarding the clinical applications of OCT. On behalf of all authors, the corresponding author states that there is no conflict of interest for all other authors.
Funding
This study was supported by Instituto de Salud Carlos III, Spain: PS09/00259 and RD07/0060/01 to PV and RD12/0032/0002 to AS. EHML was supported by a fellowship from the Instituto de Salud Carlos III, Spain (Rio Hortega program: CM13/00150). The funding agencies had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
Rights and permissions
About this article

Cite this article
Lampert, E.J., Andorra, M., Torres-Torres, R. et al. Color vision impairment in multiple sclerosis points to retinal ganglion cell damage. J Neurol 262, 2491–2497 (2015). https://doi.org/10.1007/s00415-015-7876-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-015-7876-3