
Abstract
Aims
The evaluation of the cutoff value of I3M = 0.08 for discriminating black South African minors from adults, and its relationship with chronological age.
Material and methods
A sample of 833 panoramic radiographs of healthy black South African subjects (500 females and 333 males), in the age range of 14 to 24 years (mean age 17.67 years in females and 17.42 years in males), was retrospectively evaluated.
Results
ICC values were 99.10% (95% CI 97.70 to 99.70%) and 99.20% (95% CI 98.00 to 99.60%), for the intra- and inter-observer reliability, respectively. I3M decreased as the real age gradually increased in both sexes. According to the logistic regression model, the variable sex was not significant when the probability that an individual is 18 years or older was calculated. The I3M = 0.08 was valuable in discriminating between adults and minors. The overall accuracy (ACC = fraction of accurately classified subjects) is 0.90 (95% CI 0.87–0.91); the proportion of correctly classified subjects (Se = sensitivity) is 0.80 (95% CI 0.76–0.84), and specificity (Sp) is 0.95 (95% CI 0.93–0.97). The PPV (predictive positive value) is 0.96 (95% CI 0.95–0.97), and the negative predictive value is 0.76 (95% CI 0.72–0.80).
Conclusion
The results show that I3M is a valuable method to distinguish subjects who are around legal adult age in South Africa.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Adult or minor? It is a crucial question that requires an answer especially in a country like South Africa with a high rate of criminal actions, and legal and illegal immigration [1,2,3,4]. Since the current age estimation methods used across the world for estimating age of majority in some countries have been shown to be outdated and mostly inaccurate [5], there is also a clear need for a standardized age estimation to distinguish minors from adults in the South African population and migrants traveling to this region.
It is well known that all teeth, except for third molars, finish their development between 12 and 14 years of age and that, in the age span of 15.7–23.3 years, the third molars represent the only teeth still growing. Therefore, the assessment of legal age can only be carried out by observing and measuring the third molar maturation process [6,7,8]. In fact, the degree of development of this tooth may be recorded as a measure of observed tooth length [9, 10] or as a ratio of perceived tooth dimensions [10, 11], or classified in various stages according to scores assigned to its maturation and eruption [12]. According to the Study Group on Forensic Age Diagnostics of the German Society of Legal Medicine (AGFAD) and Forensic Anthropology Society of Europe (FASE), there is a general agreement about the suitable methods available for age estimation [13, 14]. The radiographic odontological examination seems to be more reliable compared to radiographic evaluation of their skeletal system as teeth development is less influenced by systemic factors [15].
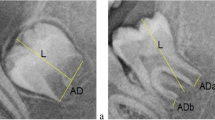
In 2008, Cameriere et al. proposed a new dental method for assessing adult age. This method is based on the relationship between age and the normalized measures of the open apices of the third molar, known as the third molar maturity index (I3M). This technique records continuous data and is based on ratios between measurements of apical pulp widths and tooth lengths. A cutoff value of I3M = 0.08 was determined to assign an individual to juvenile or adult age [16].
Cameriere et al.’s method showed that the I3M better discriminates adults and minors as being 18 years and older or younger than 18 years [16]. This study aimed to evaluate the cutoff value of I3M = 0.08, previously recommended by Cameriere et al. [16] for discriminating black South Africans between adults and minors.
Materials and methods
The studied sample consisted of 833 healthy subjects (females 500, males 333) with black African ethnicity from whom a panoramic radiograph was collected. All the X-rays were collected retrospectively from the database of a private dental clinic in Pretoria, South Africa (Table 1).
The inclusion criteria were as follows: age between 14 and 24 years at the time the panoramic radiographs were obtained, good-quality radiographs, and healthy subjects with known precise age and free of systemic disorders. The exclusion criteria were as follows: unclear radiographs or with radiographic distortion, gross pathology or history of orthodontic treatment, subjects of unknown age or without full dental records, and those with no third molars or third molars with developmental anomalies. Socioeconomic status or specific ethnic groups were not evaluated among the participants. Patient data was recorded in an excel file, recording patients’ identification number, sex, date of birth, and date of the X-rays. The CA (chronological age) for each subject was calculated by subtracting the date of the X-rays from the date of birth, and converted into decimal ages. The study was carried out in accordance with the ethical standards laid down by the Declaration of Helsinki (Finland) [17].
Measurements
As already proposed by Cameriere et al. [16], the dental maturity index (I3M) of the left lower third molar was evaluated. In order to manipulate the differences in magnification during X-ray imaging and processing, a ratio (I3M) between the sum of the inner side’s width of the open apices in third molar and the tooth’s length was calculated. If third molars were found with entirely closed roots, then I3M = 0.00 was recorded. The cutoff value of I3M = 0.08 was tested to discriminate adults (≥18 years) and minors (<18 years). X-ray images were processed by an open-source image computer-aided drafting program used to process and analyze digital images (ImageJ 1.49).
Statistical analysis
The names and surnames of all subjects and their sex, date of birth, and date of X-rays were recorded on the panoramic radiograph. However, during the estimation process, the observers were categorically blinded from the chronological age of each subject leaving only the sex to be known. Three observers, two forensic odontologists and a doctorate student in immuno-metabolic pathologies and with varying levels of experience, performed the observer error analysis, and intra-class correlation coefficient (ICC) was applied to calculate intra- and inter-observer variability. If the outcome variable is continuous, Lin stated that the appropriate index for measuring agreement between two observers is the concordance correlation coefficient (CCC) [18,19,20]. Nonetheless, the ICC is almost identical to Lin’s concordance correlation coefficient [18,19,20] and it may be calculated to measure reproducibility and repeatability. As suggested by Ferrante and Cameriere [21], the ICC based on the random-effects model for one-way analysis of variance (ANOVA) has been applied.
Repeated observations from the first author were used to assess intra-observer agreement, while inter-observer analysis was based on comparisons with those of two other observers. For this purpose, 50 radiographic panoramic images were randomly selected 4 weeks following the initial scoring to calculate percentage of agreement, for both intra- and inter-observer analyses. Scatter plot and box plot graphs and tables were used to show relationships between chronological age and different I3M values for both sexes.
Setting π as the probability that an individual was at least 18 years old, the dependence of this probability on I3M and sex with a linear logistic equation was modeled:
in which logit(π) is the natural logarithm of the ratioπ/(1−π), b0 is the intercept of the linear model, and b1 and b2 are coefficients of the predictor variables I3M (third molar maturity index) and sex (sex = 0 for females and 1 for males). In order to examine the effect of including one of the two variables in or excluding it from the model, the difference in deviance among different models, with or without sex and I3M, was considered.
In order to test the performance of the specific cutoff value of I3M, the results were also shown in a 2 × 2 contingency table that summarized the number of subjects who have I3M < 0.08 and are 18 years or older (true positive values), then subjects with I3M who are younger than 18 years (false-positive values), followed by those with I3M ≥ 0.08 who are 18 years or older (false-negative values), and finally those with I3M ≥ 0.08 who are younger than 18 years (true negative values). The 95% confidence interval (95% CI) was applied to describe the uncertainty associated with the statistical tests.
The accuracy of the test (ACC) and the sensitivity p1 (i.e., the proportion of subjects older than or equal to 18 years of age with I3M < 0.08), together with its specificity p2 (i.e., the proportion of individuals younger than 18 with I3M ≥ 0.08), were evaluated. Positive predictive values (PPVs) and negative predictive values (NPVs) were also calculated to determinate the probability that an individual with a positive screening result (I3M < 0.08) truly has the correct age (subjects older than or equal to 18 years of age). I3M may help to discriminate between individuals who are or not aged 18 years, or more, by the post-test probability of being 18 years of age or more (i.e., the proportion of individuals with I3M < 0.08 who are older than or equal to 18 years). According to Bayes’ theorem [22, 23], post-test probability may be described as in the following formula:
In the post-test probability p, p0 is the probability that a black South African individual is 18 years or older. This probability, p0, was evaluated with the data obtained from the Statistical Office of South Africa [STATS SA Mid-year population estimates 2017. Statistical release P0302, www.statssa.gov.za]. The threshold of significance was set at 5%. Statistical analysis was performed using R statistical software URL: https://www.R-project.org/ [24].
Results
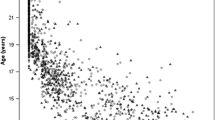
I3M values gradually decreased as age increased in both females and males (Figs. 1 and 2).

Scatter plot of the relationship between chronological age and I3M in black South African females. The horizontal line is at I3M = 0.08, and the vertical line is at 18 years old

Scatter plot of the relationship between chronological age and I3M in black South African males. The horizontal line is at I3M = 0.08, and the vertical line is at 18 years old
Concerning intra- and inter-observer agreement, the obtained results showed that no significant bias has been detected among the observers involved in the radiographic measurements. In detail, ICC values were 99.10% (95% CI 97.70 to 99.70%) and 99.20% (95% CI 98.00 to 99.60%), for the intra- and inter-observer reliability, respectively.
As reported in Table 2, the change in deviance on adding the variable sex to a model that includes a constant term alone (null model) was not significant. Instead, when I3M was added to the null model, the deviance was reduced by a highly significant amount (p < 0.001).
Therefore, the probability that an individual is 18 years or older depends on the degree of development of the third molar I3M, but it does not significantly depend on sex. Hence, the cutoff of I3M can be considered for discriminating black South African minors from adults pooling together males and females.
Classification of the sample
Table 3 displays the close association between adult age and positivity of the test (i.e., I3M < 0.08) in both females and males. The overall accuracy (ACC = fraction of accurately classified subjects) is 0.90 (95% CI 0.87–0.91); the proportion of correctly classified subjects (Se = sensitivity) is 0.80 (95% CI 0.76–0.84), and specificity (Sp = specificity) is 0.95 (95% CI 0.93–0.97). The PPV of the test, where the individuals whose I3M < 0.08 are 18 years old or older, is 0.96 (95% CI 0.95–0.97), and the NPV, where the individuals whose I3M ≥ 0.08 are younger than 18 years, is 0.76 (95% CI 0.72–0.80).
Discussion
The need and the interest in dental age estimation globally is rising [6]. Age estimation is especially difficult when it comes to the assessment of young persons (aged 15 years to early 20s) in which physical maturity does not necessarily equate to being an adult [25]. In addition, this is often complicated by various factors such as non-availability of collateral information, language barriers, and fear of providing any information because of risk of deportation, and a lack of population-specific charts to use to compare anthropometric measurements [26]. Third molars are the only permanent teeth still in development after the age of 15 so they are an important tool in the discrimination between adults and minors [7, 8, 27,28,29]. In the past, multiple studies have focused on analysis of the third molar mineralization using X-rays, where a continuous process of their development was divided into a finite number of stages [30,31,32,33,34]. Some reports were based on datasets of all permanent teeth either including or excluding third molars or on third molars only [35, 36]. Yet, the third molar has been often considered unreliable due to several factors such as varying presence, malposition, time of initial formation, and wide age range of mineralization, or that it could also be removed following a routine dental treatment [27, 37].
Previous studies, in specific racial groups (Zulu and Xhosa) of South African children, demonstrated that Demirjian’s age estimation method [34, 38, 39] overestimated the age of the examined subjects but they were not considered as reliable due to the small number of subjects in each age group [38, 39]. Although the stages of the dental maturity scoring system may be universal in application, it is well known that the original Demirjian study on a French Canadian population [34] led to an age overestimation in “all” other groups by about 6 months. An early development on the third molars of black South African children was also illustrated when they were compared to Japanese and German children [40]. Advanced growth in the black South African population can be related to the short formation times for enamel and dentine in this group [41]. The enamel formation time of Southern Africans seems to be shorter when compared with Northern Europeans; this could explain the overestimation of dental age in a black South African population [42].
The importance of third molar mineralization in black populations, and its use to discriminate minors from adults, has been described in previously published studies [35, 43,44,45,46]. Conversely, few investigations have been carried out on third molar development in black populations in Africa. One of the most critical problems is that several African countries operate with obsolete civil registration systems that do not ensure proper, if any, documentation of persons at birth and at death. As a result, it is common and considered ethically normal to perform age-cheating, falsification of documents, multiple identification, and impersonation of other individuals [47].
When considering the forensic and clinical literature, this is the first radiographic dental study of the usefulness of I3M for discriminating between adults and minors in a black South African sample of children and young adults. This would be beneficial in a series of cases in which the age of majority is in doubt such as weddings [48,49,50,51,52,53,54] and sexual offense acts [55]. With the reformation of the Children’s Act in 2007, the age of legal majority in South Africa was reduced from 21 to 18 years old [56].
As for the digital panoramic radiography, two advantages should be highlighted: (1) It is not an invasive technique and only requires exposure to small radiation doses (0.001–0.005 mSv) to acquire a suitable panoramic radiograph [57]; (2) it provides a large archive of developing teeth in otherwise healthy children, adolescents, and emerging adults. Despite the convincing evidence, this technique is not yet supported by all medical organizations [58]. In the last 10 years, due to the rapid increase in the demand for forensic age estimates of unaccompanied minors, it has been demonstrated that a simple panoramic radiograph may provide the forensic personnel with valuable information about an individual’s developmental status. In Germany, for example, the Administrative Court (VG) of Hamburg (Az. 3 E 1152/09) stated, “In accordance with the principle of proportionality, X-rays irradiation is a health hazard within the normal range, and not a health disadvantage in the meaning of the provision, for the person examined” [59].
In relation to the influence of sexual dimorphism in third molar development, some studies that used the method applied here showed that differences between females and males did not significantly influence age estimation formula [60]. However, some authors pointed out that sex differences should be considered because the third molar development is faster in females than in males [60, 61]. In this study, sex differences were not significant when considering the probability that an individual is 18 years or older. This showed that the probability depended more on the degree of development of the third molar (I3M) than on the sexual dimorphism.
As for the obtained results of sensitivity and specificity, PPV and NPV, they were almost similar to other findings from the previous studies on I3M in different populations from Africa and abroad. Taking into account two African studies performed on the population of Botswana and Libya, similar results were reported [62, 63]: in Botswana, Cavrić et al. [62] obtained values of specificity of 0.94 and 0.96 in males and females with a sensitivity of 0.88 in both the genders. In a Libyan sample, Dardouri et al. [63] obtained the following results: the sensitivity was 0.90 in both males and females, and the specificity was 1. A slight tendency exists in higher specificity over sensitivity values showing that I3M is more accurate in discriminating individuals younger than 18 years than the subjects older than that age.
As already demonstrated in some previous studies [64, 65], a chosen medical or screening test must be sensitive enough to detect if an individual is 18 years old or older. At the same time, it should possess a relatively high degree of specificity, which represents the probability that the test will create a true negative result (i.e., all individuals younger than 18 years should be correctly classified). False-negative results must also be considered as in those cases serious ethical consequences could be faced. Indeed, minors being erroneously assessed as over 18 years can be considered more improper than individuals over 18 years being erroneously assessed as minors [66]. Usually, this results in additional mental and physical strain and on attacks of their human rights. The Convention on the Rights of the Child (CRC) has set out several rights that may be breached when a child is assessed to be an adult by inappropriate age assessment methods (e.g., mistreatment of the individual, family separation, and deprivation of liberty) [67, 68].
Concerning the PPV and NPV, they are 0.96 (95% CI 0.95–0.97) and 0.76 (95% CI 0.72–0.80), respectively. These values describe an individual’s probability of being 18 years old, or older, once the results of his/her tests are already known. To many, the PPV or NPV are the key characteristics of a screening test because they accurately measure its strength [69]. A PPV of 0.96 means that 96% of the subjects with a positive test actually were 18 years old or older; an NPV of 0.76 means that 76% of the subjects were minors. The results from the present study showed that PPV and NPV are similar to those achieved from the Botswana sample in which the PPVs were 0.94 and 0.97 for males and females, respectively, whereas the NPVs were 0.88 and 0.87 for males and females, respectively. Unfortunately, Dardouri et al. [63] did not calculate the PPV and NPV for their Libyan sample. Finally, concerning the intra- and inter-observer agreement values, they are high and comparable to those studies using the staging system [34] and those in which I3M has already been applied. Among the African studies, the obtained results are almost similar: according to Cavrić et al. [62], ICC values were 0.99 (95% CI 0.98 to 0.99) and 0.98 (95% CI 0.97 to 0.99) for the intra- and the inter-observer agreement, respectively. In Dardouri et al. [63], the reliability of the data collection was evaluated calculating the concordance correlation coefficient (CCC) and no statistically significant difference between paired sets of measurements was detected: CCC = 1. The ICC has good intuitive interpretation because it includes components of both precision (degree of variation) and accuracy (degree of location or scale shift) [21, 70].
Due to this, such a coefficient has been often used to measure intra- and inter-observer agreement in several studies performed by Cameriere et al. showing high rates of agreement (between 0.75 and 1) [62, 63, 71,72,73,74,75,76,77,78]. This is the most important achievement of this quantitative technique, which depends strictly on the accurate measuring of specific projection points of third molars on a digital panoramic radiograph [62]; in fact, although each published article tries to instruct a particular observer when her/his practice varies from that of colleagues, it cannot specify how to adjust the measuring line segments of the tooth.
In this specific research, the higher inter-observer reliability is not per se a condition enough to validate completely the method. However, the fact that these values are recurring in previous studies, other than the present one, using the same method, represents a valuable contribution to its scientific validation.
Conclusion
The results obtained in this research show that I3M is a valuable method to distinguish subjects who are around legal adult age in South Africa. Regarding specificity, higher values have been also achieved for this sample confirming the general tendency of I3M to better discriminate those subjects who are younger than 18 years of age.
References
Annual Crime Report (ACR) of the South African Police Service (SAPS) (2017) Crime Statistics 2016–2017 financial year (www.saps.gov.za)
Campbell EK (2006) Reflections on illegal immigration in Botswana and South Africa. Afr Popul Stud 21:23–44
Statistics South Africa (2015) Documented immigrants in South Africa. Statistical release P0351.4. Pretoria http://www.statssa.gov.za/
United Nations High Commissioner for Refugees (2015) UNHCR operation in South Africa, Lesotho and Swaziland
Thevissen PW, Pittayapat P, Fieuws S, Willems G (2009) Estimating age of majority on third molars developmental stages in young adults from Thailand using a modified scoring technique. J Forensic Sci 54(2):428–432. https://doi.org/10.1111/j.1556-4029.2008.00961.x
Liversidge HM (2008) Dental age revisited. In: Irish JD, Nelson GC (eds) Technique and application in dental anthropology. Cambridge University Press, Cambridge, pp 234–252
Galić I, Vodanović M, Janković S, Mihanović F, Nakaš E, Prohić S, Galić E, Brkić H (2013) Dental age estimation on Bosnian-Herzegovinian children aged 6–14 years: evaluation of Chaillet’s international maturity standards. J Forensic Legal Med 20:40–45. https://doi.org/10.1016/j.jflm.2012.04.037
Cameriere R, Brkić H, Ermenc B, Ferrante L, Ovsenik M, Cingolani M (2008) The measurement of open apices of teeth to test chronological age of over 14-year olds in living subjects. Forensic Sci Int 174:217–221. https://doi.org/10.1016/j.forsciint.2007.04.220
Liversidge HM, Molleson TI (1999) Developing permanent tooth length as an estimate of age. J Forensic Sci 44:917–920
Thevissen PW, Fieuws S, Willems G (2011) Third molar development: measurements versus scores as age predictors. Arch Oral Biol 56(10):1035–1040. https://doi.org/10.1016/j.archoralbio.2011.04.008
Cameriere R, Ferrante L, Cingolani M (2006) Age estimation in children by measurement of open apices in teeth. Int J Legal Med 120:49–52. https://doi.org/10.1007/s00414-005-0047-9
Willems G (2001) A review of the most commonly used dental age estimation techniques. J Forensic Odontostomatol 19:9–17
Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Rösing FW, Rötzscher K, Geserick G (2008) Criteria for age estimation in living individuals. Int J Legal Med 122:457–460. https://doi.org/10.1007/s00414-008-0254-2
Baccino E (2005) Forensic Anthropology Society of Europe (FASE), a subsection of the IALM, is 1 year old. Int J Legal Med 119:N1-N
Feijoo G, Barberia E, De Nova J, Prieto JL (2012) Permanent teeth development in a Spanish sample. Application to dental age estimation. Forensic Sci Int 214(213):e1–e6. https://doi.org/10.1016/j.forsciint.2011.08.024
Cameriere R, Ferrante L, De Angelis D, Scarpino F, Galli F (2008) The comparison between measurement of open apices of third molars and Demirjian stages to test chronological age of over 18 year olds in living subjects. Int J Legal Med 122:493–497. https://doi.org/10.1007/s00414-008-0279-6
World Medical Association (2013) World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310:2191–2194
Lin L (2000) A note on the concordance correlation coefficient. Biometrics 56:324–325
Lin L (1989) A concordance correlation coefficient to evaluate reproducibility. Biometrics 45:255–268
Lin L (1992) Assay validation using the concordance correlation coefficient. Biometrics 48(2):599–604
Ferrante L, Cameriere R (2009) Statistical methods to assess the reliability of measurements in the procedures for forensic age estimation. Int J Legal Med 123:277–283. https://doi.org/10.1007/s00414-009-0349-4
Crawford JR, Garthwaite PH, Betkowska K (2009) Bayes’ theorem and diagnostic tests in neuropsychology: interval estimates for post-test probabilities. Clin Neuropsychol 23(4):624–644. https://doi.org/10.1080/13854040802524229
Ferrante L, Skrami E, Gesuita R, Cameriere R (2015) Bayesian calibration for forensic age estimation. Stat Med 34(10):1779–1790. https://doi.org/10.1002/sim.6448
R Core Team (2017) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna https://www.R-project.org/
Aynsley-Green A, Cole TJ, Crawley H, Lessof N, Boag LR, Wallace RMM (2012) Medical, statistical, ethical and human rights considerations in the assessment of age in children and young people subject to immigration control. Br Med Bull 102(1):17–42. https://doi.org/10.1093/bmb/lds014
Tiemensma M, Phillips VM (2016) The dilemma of age estimation of children and juveniles in South Africa. S Afr Med J 106(11):1061. https://doi.org/10.7196/samj.2016.v106i11.11407
Liversidge HM, Marsden PH (2010) Estimating age and the likelihood of having attained 18 years of age using mandibular third molars. Br Dent J 209:E13. https://doi.org/10.1038/sj.bdj.2010.976
Sisman Y, Uysal T, Yagmur F (2007) Third molar development in relation to chronological age in Turkish children and young adults. Angle Orthod 77(6):1040–1045. https://doi.org/10.2319/101906-430.1
Rai B, Kaur J, Jafarzadeh H (2010) Dental age estimation from the developmental stages of the third molars in Iranian population. J Forensic Med 17(6):309–311. https://doi.org/10.1016/j.jflm.2010.04.010
Gleiser I, Hunt EE Jr (1955) The permanent mandibular first molar: its calcification, eruption and decay. Am J Phys Anthropol 13:253–283
Kohler S, Schmelzle R, Loitz C, Puschel K (1994) Development of wisdom teeth as a criterion of age determination. Ann Anat 176:339–345
Thevissen PW, Fieuws S, Willems G (2013) Third molar development: evaluation of nine tooth development registration techniques for age estimations. J Forensic Sci 58:393–397. https://doi.org/10.1111/1556-4029.12063
Moorrees CF, Fanning EA, Hunt EE Jr (1963) Age variation of formation stages for ten permanent teeth. J Dent Res 42:1490–1502
Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol 45:211–227
Liversidge HM (2008) Timing of human mandibular third molar formation. Ann Hum Biol 35(3):294–321. https://doi.org/10.1080/03014460801971445
Cavrić J, Vodanović M, Marusić A, Galić I (2016) Time of mineralization of permanent teeth in children and adolescents in Gaborone, Botswana. Ann Anat 203:24–32. https://doi.org/10.1016/j.aanat.2015.08.001
Liversidge HM (2008) Predicting mandibular third molar agenesis from second molar formation. Acta Stomatol Croat 42:311–317
Phillips V, van Wyk Kotze T (2009) Dental age-related tables for children of various ethnic groups in South Africa. J Forensic Odontostomatol 27(2):29–44
Phillips V, van Wyk Kotze T (2009) Testing standard methods of dental age estimation by Moorrees, Fanning and Hunt and Demirjian, Goldstein and Tanner on three South African children samples. J Forensic Odontostomatol 27(2):20–28
Olze A, Schmeling A, Taniguchi M, Maeda H, van Niekerk P, Wernecke K (2004) Forensic age estimation in living subjects: the ethnic factor in wisdom tooth mineralization. Int J Legal Med 118(3):170–173. https://doi.org/10.1007/s00414-004-0434-7
Tompkins R (1996) Human population variability in relative dental development. Am J Phys Antropol 99:79–102
Reid D, Dean M (2006) Variation in modern human enamel formation times. J Hum Evol 50:329–346. https://doi.org/10.1016/j.jhevol.2005.09.003
Mincer HH, Harris EF, Berryman HE (1993) The A.B.F.O. study of third molar development and its use as an estimator of chronological age. J Forensic Sci 38:379–390
Blankenship JA, Mincer HH, Anderson KM, Woods MA, Burton EL (2007) Third molar development in the estimation of chronologic age in American blacks as compared with whites. J Forensic Sci 52:428–433. https://doi.org/10.1111/j.1556-4029.2006.00356.x
Olze A, van Niekerk P, Schmidt S, Wernecke KD, Rosing FW, Geserick G et al (2006) Studies on the progress of third-molar mineralisation in a Black African population. Homo internationale Zeitschrift fur die vergleichende Forschung am Menschen 57:209–217. https://doi.org/10.1016/j.jchb.2004.08.003
Harris EF, McKee JH (1990) Tooth mineralization standards for blacks and whites from the middle southern United States. J Forensic Sci 35:859–872
Tosam MJ (2015) The ethical and social implications of age-cheating in Africa. Int J Philos 3(1):1–11. https://doi.org/10.11648/j.ijp.20150301.11
Marriage Act (1961) Act 25 of 1961. South Africa
Civil Union Act (2006) Act No. 17 of 2006. South Africa
Recognition of Customary Marriages (1998) Act 120 of 1998. South Africa
United Nations Children’s Fund (UNICEF) (2005) Early marriage: a harmful traditional practice, New York
UNICEF (2001) Early marriage: child spouses, Innocenti Digest, Florence, Italy: UNICEF, No. 7 The Convention on the Rights of the Child (CRC, 1989)
African Charter on the Rights and Welfare of the Child OAU Doc. CAB/LEG/24.9/49 (1990)
Maswikwa B, Richter L, Kaufman J, Nandi A (2015) Minimum marriage age laws and the prevalence of child marriage and adolescent birth: evidence from sub-Saharan Africa. Int Perspect Sex Reprod Health 41(2):58–68. https://doi.org/10.1363/4105815
The Criminal Law (2007) Sexual offences and related matters. Amendment act, 2007 act no. 32 of 2007
Children’s Act (2007) No 38 of 2005. South Africa
Mettler FA, Huda W, Yoshizumi TT, Mahesh M (2008) Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 248:254–263. https://doi.org/10.1148/radiol.2481071451
AHRC (2012) An age of uncertainty: inquiry into the treatment of individuals suspected of people smuggling offences who say that they are children. Australian Human Rights Commission, Sydney
Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G (2016) Forensic age estimation. Methods, certainty, and the law. Dtsch Arztebl Int 113(4):44–50. https://doi.org/10.3238/arztebl.2016.0044
Santiago BM, Almeida L, Cavalcanti YW, Magno MB, Maia LC (2017) Accuracy of the third molar maturity index in assessing the legal age of 18 years: a systematic review and meta-analysis. IJLM. https://doi.org/10.1007/s00414-017-1766-4
AlQahtani S, Kawthar A, AlAraik A, AlShalan A (2017) Third molar cut-off value in assessing the legal age of 18 in Saudi population. Forensic Sci Int 272:64–67. https://doi.org/10.1016/j.forsciint.2017.01.004
Cavrić J, Galić I, Vodanović M, Brkić H, Gregov J, Viva S, Rey L, Cameriere R (2016) Third molar maturity index (I3M) for assessing age of majority in a black African population in Botswana. Int J Legal Med 130:1109–1120. https://doi.org/10.1007/s00414-016-1344-1
Dardouri A, Cameriere R, De Luca S, Vanin S (2016) Third molar maturity index by measurements of open apices in a Libyan sample of living subjects. Forensic Sci Int 267:230.e1–230.e6. https://doi.org/10.1016/j.forsciint.2016.07.020
Pepe MS (2003) The statistical evaluation of medical tests for classification and prediction. Oxford University Press, New York, pp 14–34
Sackett DL, Haynes RB, Guyatt GH, Tugwell P (1991) Clinical epidemiology: a basic science for clinical medicine. Little Brown and Co, New York, pp 51–68
Garamendi PM, Landa MI, Ballesteros J, Solano MA (2005) Reliability of the methods applied to assess age minority in living subjects around 18 years old. A survey on a Moroccan origin population. Forensic Sci Int 154(1):3–12. https://doi.org/10.1016/j.forsciint.2004.08.018
Pobjoy JM (2017) An Age-Sensitive Assessment of Risk. In: The child in international refugee law. Cambridge University Press, Cambridge, pp 79–99
Franklin D (2010) Forensic age estimation in human skeletal remains: current concepts and future directions. Leg Med (Tokyo) 12(1):1–7. https://doi.org/10.1016/j.legalmed.2009.09.001
Altman DG, Bland JM (1994) Diagnostic tests 2: predictive values. BMJ 309:102
Barnhart HX, Haber M, Song J (2002) Overall concordance correlation coefficient for evaluating agreement among multiple observers. Biometrics 58:1020–1027. https://doi.org/10.1111/j.0006-341X.2002.01020.x
Galić I, Lauc T, Brkić H, Vodanović M, Galić E, Biazevic MG et al (2015) Cameriere’s third molar maturity index in assessing age of majority. Forensic Sci Int 252(191):e1–e5. https://doi.org/10.1016/j.forsciint.2015.04.030
Deitos AR, Costa C, Michel-Crosato E, Galić I, Cameriere R, Biazevic MG (2015) Age estimation among Brazilians: younger or older than 18? J Forensic Legal Med 33:111–115. https://doi.org/10.1016/j.jflm.2015.04.016
Cameriere R, Santoro V, Roca R, Lozito P, Introna F, Cingolani M, Galić I, Ferrante L (2014) Assessment of legal adult age of 18 by measurement of open apices of the third molars: study on the Albanian sample. Forensic Sci Int 245C(205):e1–e5. https://doi.org/10.1016/j.forsciint.2014.10.013
Cameriere R, Pacifici A, Viva S, Carbone D, Pacifici L, Polimeni A (2014) Adult or not? Accuracy of Cameriere’s cut-off value for third molar in assessing 18 years of age for legal purposes. Minerva Stomatol 63:283–294
Gulsahi A, De Luca S, Cehreli SB, Tirali RB, Cameriere R (2016) Accuracy of the third molar index for assessing the legal majority of 18 years in Turkish population. Forensic Sci Int 584:e1–584.e6. https://doi.org/10.1016/j.forsciint.2016.04.034
Franklin D, Karkhanis S, Flavel A, Collini F, De Luca S, Cameriere R (2016) Accuracy of a cut-off value based on the third molar index: validation in an Australian population. Forensic Sci Int 266:575.e1–575.e6. https://doi.org/10.1016/j.forsciint.2016.06.032
Zelic K, Galic I, Nedeljkovic N, Jakovljevic A, Milosevic O, Djuric M, Cameriere R (2016) Accuracy of Cameriere's third molar maturity index in assessing legal adulthood on Serbian population. Forensic Sci Int 259:127–132. https://doi.org/10.1016/j.forsciint.2015.12.032
Quispe Lizarbe RJ, Solís Adrianzén C, Quezada-Márquez MM, Galić I, Cameriere R (2017) Demirjian’s stages and Cameriere’s third molar maturity index to estimate legal adult age in Peruvian population. Leg Med (Tokyo) 25:59–65. https://doi.org/10.1016/j.legalmed.2017.01.003
Acknowledgements
The authors would like to thank the anonymous reviewers for their valuable comments and suggestions to improve the quality of the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was carried out in accordance with the ethical standards laid down by the Declaration of Helsinki (Finland)
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Angelakopoulos, N., De Luca, S., Velandia Palacio, L.A. et al. Third molar maturity index (I3M) for assessing age of majority: study of a black South African sample. Int J Legal Med 132, 1457–1464 (2018). https://doi.org/10.1007/s00414-018-1818-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-018-1818-4