
Abstract
The diagnostic accuracy of the I3M to assess the legal age of 18 years has already been tested in several specific-population samples. The left lower third molar has been extensively used for discriminating between minors and adults. This research aimed to compare the usefulness of lower third molar maturity indexes, from both left and right side (I3ML and I3MR), in samples originating from four distinct continents in order to examine possible differences in their accuracy values. For this purpose, a sample of 10,181 orthopantomograms (OPGs), from Europe, Africa, Asia and America, was analysed and previously scored in other studies. The samples included healthy subjects with no systemic disorders with both third molars and clear depicted root apices. Wilcoxon Signed Rank test for left and right asymmetry did not show any significant differences. Data about sensitivity, specificity, predictive values, likelihood ratio and accuracy were pooled together and showed similar results for I3ML and I3MR, respectively. In addition, all these quantities were high when only the I3MR was considered to discriminate between adults and minors. The present referable database was the first to pool third molar measurements using panoramic radiographs of subjects coming from different continents. The results highlighted that both I3ML and I3MR are reliable indicators for assessing the legal age of 18 years old in those jurisdictions where this legal threshold has been set as the age of majority.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Forensic practitioners often face challenging cases where they have to determine whether an individual is a minor or an adult [1, 2]. Human identification for humanitarian reasons in civil and criminal cases involving young people, cases of adoption, mass disaster scenarios, illegal trafficking, migration, unaccompanied minors seeking asylum, early marriage and child labour are just some cases [1, 2].
In this context, several specialists are often involved in providing a reliable age assessment for legal purposes and according to the standard principles of patient confidentiality and professional conduct. For this reason, multiple techniques from different forensic disciplines can be used in order to attain a result that is the closest to reality [3].
According to guidelines published by the International Study Group on Forensic Age Diagnostics (AGFAD: Arbeitsgemeinschaft für Forensische Altersdiagnostik) (https://www.medizin.uni-muenster.de/en/rechtsmedizin/schmeling/agfad/about/home), forensic age estimation in minors is a standardized process in which the radiographic study of the hand-wrist bones and the study of third molar development are often the most useful methods for determining whether an individual has attained the age of majority [3, 4]. In countries where ionizing radiation imaging techniques are forbidden for application in medico-legal cases, other techniques may include specialized modalities, such as computed tomography (CT) or magnetic resonance imaging (MRI) [3].
Several guidelines for assessing the age of suspected minors have been proposed, showing that estimating chronological age in living individuals is complex [5]. Age indicators can be applied, with different degrees of accuracy, throughout age groups [6]. Radiographs of the left hand can be used to analyse the form and size of bone elements and the degree of epiphyseal ossification in adolescents and young adults [3, 7]. One of this method’s limitations is that changes in the hand-wrist bones are not clear after the age of 14–16 years [3, 7].
In a later stage of development, third molar analysis is very important for age assessment between adolescence and adulthood because it is the only tooth still in development during that period. All teeth, except for third molars, finish their development between 12 and 14 years of age, and, in the age span of 15.7–23.3 years, the third molars represent the only teeth still growing. Therefore, assessing legal age can only be carried out by observing and measuring the third molar maturation process [8,9,10].
The third molar is characterized by high variability in formation and large-scale diversity in presence or absence [11, 12]. Sometimes, this tooth is useless for analysis because of its position or rotation in such a way that it cannot be analysed. Some individuals do not grow third molars at all. In some cases, matured (stage H) third molars may appear as early as 15 years of age, whereas, in others, they may have not appeared at all, even at the age of 25 [13, 14]. The worldwide average of third molar agenesis is 22.6% [15]. The ratio of bilateral to unilateral third molar agenesis is also significantly higher [16]. In addition, pathology, such as unrestorable caries, non-treatable pulpal and/or periapical pathology, infection, internal or external resorption of the tooth or adjacent teeth, and disease of the follicle including cysts or tumours are all well-defined criteria for lower third molar removal [17, 18].
Differences in the development rate of third molars between dental arches and left–right symmetry have also been highlighted in previous studies. Kasper et al. (2009) could not find evidence for left–right symmetry in third molar development [19]. Mincer et al. (1993) reported a slight but random difference between the development of third molars of the same arch [20]. Conversely, Levesque et al. [21], Olze et al. [22], De Angelis et al. [23], and Thevissen et al. [24] reported the absence of a significant difference between the development of left and right third molars.
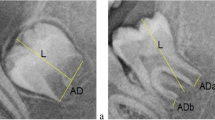
In 2008, Cameriere et al. [25] developed a new dental method for assessing adult age. This method is based on the relationship between age and the normalised measures of the third molar’s open apices, known as the third molar maturity index (I3M).
This technique records continuous data and is based on ratios between measurements of apical pulp widths and tooth lengths. A cut-off value of 0.08 was determined to assign an individual to a juvenile or adult age [25]. Since I3M was introduced, several authors have tested and validated this method in various populations [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56]. This method evaluates the left lower third molar, and in cases where they are missing, the right ones are examined and measured. Cameriere et al. [25] demonstrated that the I3M better discriminates between adults and minors as being 18 years and older or younger than 18 years, both in males and females, since it has high accuracy for estimating adulthood regarding forensic purposes according to a recent systematic review and meta-analysis [1].
This study aimed to validate the cut-off value of I3M (I3M < 0.08 suggests that the subject is older than 18 years; I3M ≥ 0.08 suggests that the subject is younger than 18 years) [25] on both the right (I3MR) and left (I3ML) lower third molars and to estimate the risk of error in those cases in which only one of them is available (e.g. hypodontia, unilateral lower third molar agenesis, early extraction or forced removal of the tooth), using a large multi-ethnic sample.
Materials and methods
Sample
A total of 10,181 orthopantomograms (OPGs) from four continents was evaluated: 1631 subjects from Africa; 861 from North and South America; 3919 from Asia; and 3770 from Europe. The sample distribution, according to sex and age, is shown in Table 1. The following I3M ranges categories were considered to analyse the relationship between index and real age (years) of each subject: (0, 0.04); (0.04, 0.08); (0.08, 0.3); (0.3, 0.5); (0.5, 0.7); (0.7, 0.9); (0.9, 1.2); (1.2, 1.5); (1.5, 1.8); (1.8, 2.1); (2.1, 2.4); (2.4, 2.7).
These categories were chosen according to the available published research on the I3M [1]. Their primary function is to graphically represent how the third molar root apices gradually close as a subject age increases. According to the literature, the narrower the ranges, the more precise the graphic display of the I3M is in relation to the continuous phenomenon of root apices closure [1].
The sample selection criteria were as follows: clear OPGs and all permanent teeth present, including left and right third molars. The presence of any visible dental and bone pathology (e.g. large carious lesions or endodontic treatments), children with any systemic diseases or endocrine anomalies (e.g. dysmorphology, abnormally short roots) and subjects with previous root canal treatment in the lower permanent teeth were excluded from the study. Heavily rotated and impacted third molar with no visible roots were also excluded from this study.
No identification data were collected, and images were saved with high resolution in the JPEG file format, and automatically anonymised before the selection process. All data were recorded in an Excel file and the columns indicated as follows: continent, subject’s identification number, sex, date of birth and date of OPGs.
Intra- and inter-observer variabilities
Three forensic odontologists with varying levels of experience performed the observer error analysis. Repeated observations from the first author (NA) were used to determine intra-observer agreement, while inter-observer analysis was based on comparisons with those of two other observers (IG and LGJ). For this purpose, 100 OPGs were randomly selected 1 month after the initial scoring to calculate the agreement’s percentage for both intra- and inter-observer test. During the process, the observers were categorically blinded from the chronological age and sex of each subject. Intraclass correlation coefficient (ICC) was applied to calculate intra- and inter-observer variability.
Statistical analysis
The real age was classified as a binary variable, divided into adults (18.00 years or older) and minors (13–17.99 years old). The normality distribution for both the I3ML and I3MR was evaluated by the Kolmogorov–Smirnov test, which showed to be non-normal distribution data (p < 0.05). The I3ML and I3MR were compared according to the categories of age (adult or minor) according to each continent by Wilcoxon Signed Rank test, in order to evaluate possible differences between the measurements.
Each subject was classified as minor or adult according to the application of a cut-off developed by Cameriere et al. [25] in both third molars (I3ML and I3MR): I3ML and I3MR values < 0.08 classified a subject as an adult, and values ≥ 0.08 classified a subject as minor. Then, the estimated classifications for both I3ML and I3MR were compared to a real classification of individual’s age, and the diagnostic values of prediction were observed.
Specific descriptive statistics (also known as quantities) were calculated according to sex and third molar: contingency tables (confusion matrices) were generated, and the respective predictive values of sensitivity and specificity (Se and Sp, including 95% CI), positive and negative predictive values (PV + and PV − , including 95% CI), positive and negative likelihood ratio (LR + and LR − , including 95% CI) and accuracy (Acc) of estimates were determined. The LR + is the true positivity rate divided by the false positivity rate (sensitivity/1-specificity). It shows how much to increase the probability of being an adult, given a positive test result. The LR − is the false negative rate divided by the true negative rate (1-sensitivity/specificity) and indicates how much to decrease the probability of being an adult, given a negative test result [57]. The main advantage of LRs (over other measures of diagnostic accuracy, such as sensitivity and specificity) is that they can be used to quickly compare different diagnostic strategies and thus refine judgment and decision in the forensic daily practice.
All the analyses were performed using the R software (version 3.6.3, R Core Team, R Foundation for Statistical Computing, Vienna, Austria) and SPSS software (version 26.0, Armonk, IBM Corporation, NY, USA), adopting a significance level of 5%.
Results
Regarding the measurement process, the intra-observer agreement values were 0.993 (95% CI: 0.990–0.996) and 0.976 (95% CI: 0.964–0.984), for the L3M and R3M, respectively. The values for inter-observer agreement were 0.983 (95% CI: 0.976–0.988) and 0.974 (95% CI: 0.959–0.983), for the L3M and R3M, respectively.
As shown in Figs. 1, 2, 3 and 4, I3M values gradually decreased as age (years) increased across all the age groups in both molars according to each sex.
The distribution of the sample according to sex and measurements of I3ML and I3MR is described in Table 2. The lower third molar mineralisation varies according to sex, and it occurred earlier in males than in females for both I3ML and I3MR, mostly evident at the stages between 0 and 0.04, 0.04–0.08, 0.08–0.3, 0.3–0.5, 0.5–0.7, and 0.7–0.9 (Table 2).

Boxplots of the relationship between chronological age and I3ML in females. The horizontal red dotted line is at 18 years of age.

Boxplots of the relationship between chronological age and I3ML in males. The horizontal red dotted line is at 18 years of age

Boxplots of the relationship between chronological age and I3MR in females. The horizontal red dotted line is at 18 years of age

Boxplots of the relationship between chronological age and I3MR in males. The horizontal red dotted line is at 18 years of age
Table 3 showed the sample’s descriptive statistics according to each continent: the I3ML and I3MR were compared giving the categories of “adult” and “minor”. The Wilcoxon Signed Rank Test for left and right asymmetry found no significant difference for each side separately, confirming left–right symmetrical third molar development, except for minors in the African group, and for adults in the Asian and European ones.
Regarding the Acc, values of 80% or more were obtained when the I3ML and I3MR were used (Table 4). The Acc values were similar in the African, American and European samples according to the I3ML (around 83%). Meanwhile, American and European samples had similar Acc if the I3MR was used (around 85%) and a slightly better Acc than that obtained for the African sample (82.6%). Low Acc was achieved in the Asian sample if both I3ML and the I3MR were considered (73%). Concerning the Se, all the obtained values from both left and right third molar were smaller than the Sp values. PV + and PV − showed different values, whereas the high values for LR + (values were greater than 1), and the low ones observed for LR − (values were between 0 and 1), indicated greater discriminating ability.
Tables 4 and 5 show the pooled data according to the continent and both lower third molars, and when the I3M was considered for prediction, respectively. According to the quantity statistics derived from the contingency table, it is evident that both classifications demonstrated high values of Sp and PV − in comparison with Se and PV + , and high values of LR + and low values of LR − .
In Table 6, the number of subjects correctly classified is indicated when one of the third molars classified them differently from their real age.
Discussion
Age estimation of a living person is a complex multidisciplinary process due to the important humanitarian, civil and criminal implications that it often entails [1, 7]. Depending on the age threshold under scrutiny, selecting the most appropriate age indicator for accuracy and availability is necessary.
A specific challenge in forensic age estimation is assessing age of majority of asylum seekers lacking valid information relative to their identity. In this ethically sensitive scenario, a low number of false negatives has higher priority compared with a low number of false positives [58, 59].
As mentioned before, different age indicators have different applicability throughout age groups, and third molar is an advantageous indicator in the transition between adolescence and adulthood. Therefore, its use is fundamental for estimating age during these phases and, particularly, to accurately distinguish an adult subject from a minor [8,9,10, 36]. While there are several issues related to the application of third molar for age estimation, such as some authors vehemently disregarding its use both for ethical and methodological reasons, the progress observed in the search for more accurate and reliable methods is undeniable [57, 60].
The I3M method, the focus of this investigation, is a distinct result of these efforts, reinforced by its validation in different populations. Nonetheless, developmental variability still raises issues, for example, regarding differences between sexes, left/right asymmetry and possible lack of this tooth. These issues need to be addressed in order to improve scientific interpretation of discrepant results found in a diachrony of investigations. Thus, this study aims to evaluate I3M between left and right third molars using a multi-ethnic sample and the impact of unilateral absence of the third molar for assessing age of majority.
Considered as ground-breaking in forensic sciences and dentistry, this is the first dental study targeting both left and right third molar measurements on panoramic radiographs of subjects from different continents.
The results confirmed that the lower third molar’s mineralisation proceeds in a directly proportional manner with increasing age. The rate of development varies according to sex, with a longer delay in females than males for both I3ML and I3MR by a mean of 0.3 years between stages 0 and 0.9. Willershausen et al. [61] obtained similar results by analysing a multi-ethnic sample of 1202 panoramic x-rays and demonstrated that third molar roots generally develop at a faster pace in the maxilla than in the mandible, with delayed development of both the upper and lower third molars in girls as compared to boys by a mean of 0.7 years. Sex differences in third molar development have been reported with contradictory results in studies of samples from different origins. In separate research studies, Deitos et al. [49], Cameriere et al. [51], AlQahtani et al. [54], and Kumagai et al. [31] reported earlier third molar mineralisation in males of different geographic origins. Nevertheless, while other works indicated no statistically significant differences between groups, the I3M cut-off value performance was still assessed for males and females separately [42, 45, 47]. The sex differences in third molar maturation are often attributed to a reverse sexual dimorphism, explained by the fact that these rates contradict the female tendency of presenting a faster maturation, thus the need for sex-specific standards [54, 62]. Nonetheless, it is argued that the absence of sex differences on maturation rates of the third molar found in some research studies may be due to, in a later stage of development, males and females acquiring a similar developmental rhythm [48].
This study found no significant differences in the ability to discriminate between adults and minors using the left or the right I3M separately for each continent. This fact confirms the hypothesis that the development is generally symmetrical for both sides, according to the results obtained in previous research [19, 61].
According to the Wilcoxon Signed Ranked Test, some significative differences were observed in the Asian, European and African groups. Although these differences are not observed in the values of medians and values of first and third quartiles, they reflect those cases in which the lower third molars’ development does not occur in a similar way in the same age range of the same population. These results are in agreement with the concept of “fluctuating asymmetry” proposed by Bassed et al. [63]. They stated that when all of the identified asymmetric cases are assessed separately (i.e. minors from the Asian group and adults from the European and African ones), it is seen that asymmetric development is an issue on an individual basis. Therefore, in all these cases in which differences were observed, age estimations based on one of the third molars may not provide the best estimate for an identified subject.
Given the quantity statistics shown in Table 5, it was observed that the accuracy obtained from the assessment of I3M of both sides (> 80%) does not differ significantly from that obtained by analysing the individual sides: in the African, American and European samples, the accuracy values obtained by examining the I3ML separately (about 85%, 86% and 85%, respectively) are very similar to those obtained from the estimate made with the I3MR (about 84%, 88% and 86%, respectively) with a slightly better result for the I3MR of the American group. The most significant discrepancy is evident between the different continents rather than between the right/left side. In fact, compared to the other continents, the Asian sample obtained a slightly lower accuracy value on both sides (corresponding to about 75% of the I3ML with 74% of the I3MR).
It is not clear whether this reflects a true ethnic or geographic difference. This heterogeneity may be due to some study-specific factors (such as rather training and experience and imaging settings) rather than to real ethnic differences [64].
When the I3M is compared with a staging method, such an accuracy does not increase much more than in the current research. In Thevissen et al. [65], every available third molar was scored following the 10-point scoring system described by Gleiser and Hunt [66] and modified by Köhler et al. [67] within 9 country-specific populations. The percentage of correctly identified adults ranged between 72 and 93%, the percentage of correctly identified juveniles was between 33 and 87%, and the percentage of correctly identified juveniles and adults (all subjects) ranged between 71 and 85%. In a recent meta-analysis and systematic review [68], the diagnostic accuracy in the entire cohort was 71.3%. In the age range of 15–20.9, diagnostic accuracy was 64.6%.
However, when all quantities are taken into account as a set of connected variables, it is evident that the performed test discriminated very well between the two age categories (i.e., at least 18 years of age and younger than 18). Both classifications demonstrated high values of Sp and PV − in comparison with Se and PV + , and high values of LR + and low values of LR − , indicating that the age estimation by I3MR method is as accurate as that obtained by using the I3ML. This low sensitivity and high specificity for the age prediction threshold of 18 years is visible in all the geographic groups, thus indicating that this threshold favours a low number of adults misclassified as minors.
In those cases, in which one of the lower third molars is absent, or not completely developed, it is possible to use the opposite side. In this work, the high values of LR + for both I3MR and I3ML means that a mature third molar is more likely in a subject of the older category than those of the younger than 18 years old. Conversely, the low values of LR − showed that a subject with a negative test is more likely to be found if aged at least 18 than if their age is in the younger category.
These findings are especially interesting since the problems due to the lack of one of the third molars are unique as regards the anatomical districts evaluable for age (such as hand, clavicle and knee). Third molar agenesis has been reported as the most frequently occurring dental alteration, but it is not the only one [15, 69, 70]. In the literature, the reported reasons for third molar absence include the risk of impaction associated with caries, pericoronitis, periodontal defects in the distal surface of second molars, odontogenic cysts and dental crowding [71,72,73,74,75]. Finally, besides different biological or iatrogenic causes, the lack of a third molar may also be due to the deliberate act of extracting this tooth in an attempt to avoid the routine procedures for assessing age in minors seeking asylum [2].
In case of agreement between the I3MR-I3ML results, the ability to correctly identify a minor subject is approximately 86% (R) to 88% (L) for the African continent, 89% (L) to 90% (R) for the American continent, 93% (L) to 94% (R) for the European continent and 92% (L) to 91% (R) for the Asian continent. On the contrary, identifying an adult subject is about 10% lower for both I3MR and I3ML for the American and African samples, 15% for the European sample and 30% for the Asian sample. This means that, in general, the I3M method shows high specificity and low sensitivity with a higher risk of false negatives in identifying adults than minors. Concerning the LR + and LR − , these tests showed very high LR + and very low LR − , thus indicating greater discriminating ability. These values are independent of prevalence and relevant to express the probability of a diagnostic test result at the subject level: the larger the magnitude of the positive valence to the LR + , the more accurate the screening cut score is. Furthermore, LR-s range from zero to 1 with values closer to zero, representing a stronger likelihood that I3M screening performance at that particular cut score accurately categorizes the subject as minor.
Bassed et al. [63] assessed the effect of left/right asymmetry in dental and skeletal elements through the analyses of CT-scans, and in which the third molar was scored according to Demirjian et al. stages [76]. This study found that, in terms of left⁄right asymmetry, 12.6% of individuals differed in development by one stage, but only 1% by two stages in a sample of 570 individuals who had both lower third molars present [63]. Notwithstanding, the degree of asymmetry between left and right sides demonstrated that there was a good statistical agreement between contralateral sides, which supports this investigation’s findings. These authors also reported that left/right asymmetry presented a higher impact on age estimation through the clavicle than with the third molar analyses. Additionally, Bassed’s work [63] reported that asymmetry does not induce a significant bias when a sufficiently large sample is evaluated; however, with individual cases, its effect needs to be considered in forensic practice. Therefore, while our results show an agreement between I3MR and I3ML, it is necessary to evaluate its application when aiming to determine between adults and minors, thus offering an estimate which is as accurate and reliable as possible.
In fact, although the sample analysed in our study showed a high concordance between right and left, in 8% of the subjects, the evaluation of the I3ML is opposite to the I3MR, i.e. the evaluation of one side identifies an adult subject while the other identifies a minor. These cases of discrepancy are mainly represented by subjects who, in reality, are of an adult age. This finding invokes an interpretation of the scientific data which is very different from that normally given by the law, which states that in cases of doubt, the subject is considered a minor [77, 78]. However, with a greater likelihood of identifying an adult as a minor than the reverse, the minor’s rights are considerably safeguarded, lowering the possibility of producing ethically unacceptable errors in age assessment [59].
When these results are compared with those obtained by applying a qualitative method, outcomes may vary depending on the population under analysis [79]. However, the systematic reviews focusing on the “diagnostic performance” of mature third molars (apex closed) to distinguish between subjects younger or older than 18 years are still scarce. This hampers any reliable comparison between these two procedures [14].
The stage of mineralisation is classified according to various scales; the most commonly used is that of Demirjian et al. (A–H) [76]. On the one hand, it has been demonstrated that the staging techniques are slightly more accurate than those based on measurements and ratios [80]. On the other hand, a study [59] showed that, especially in those cases involving the possible criminal liability of the supposed minor (criminal proceedings), since the staging procedures may increase the number of false positives (ethically unacceptable errors), the forensic personnel have often considered the obtained error as significant.
Thevissen et al. [80] pointed out that ratios and measurements of third molars are less accurate age predictors than the stages of developing third molars and that measurements and ratios added no clinically relevant information to age prediction from third molar stage. In 2013, Thevissen et al. [65] compared third molar development registration techniques showing that the least accurate age predictions were achieved when the model based on the Cameriere’s registration technique was applied.
In general, the most serious issue of developmental stages is trying to assign the stage when the tooth in development has reached somewhere in-between the two available stages of development [45].
The I3M showed a more precise measure of the continuous process of maturation of third molar, regardless of ethnicity [64]. This index allows recording of the smallest visible open apex of this tooth and provides an accurate tool to overcome wide gap between Se and Sp for Demirjian’s stages G and H.
Cameriere et al. [25] demonstrated that, if the root apices of the third molar are closed (i.e. the third molar is at terminal grade H), then there is a high probability that the subject is at least 18 years of age. In addition, selecting a cut-off of 0.08 for the I3M allows avoiding an increase in the number of false positives when stage G of Demirjian’s technique is considered as a marker of adult age. Sharma et al. [81] demonstrated that, if stage 8 is selected as a predictor of adult age [82], it improves test sensitivity with respect to stage 9, but it evidently increases the number of false positives, which is considered an ethically unacceptable error in the judiciary system. If the I3M is used to estimate the legal adult age of 18 years, the same authors highlighted that it significantly increases test sensitivity with respect to stage 9. Furthermore, it minimises the number of false positive subjects. According to Liversidge and Marsden [83], when the Demirjian’s technique is applied, the probability of being at least 18, if the third molar is totally mature, changes from 0.75 to 0.98.
In summary, these qualitative techniques may be valuable age indicators, but considering the limitations of the last stage on adult age estimation (stage H) [76], and according to the high rate of false positives, they are not likely to be considered as useful as the continuous data in discriminating between minors and adults.
Limitations and future directions of this research
The main strength of this research was the possibility to gather reliable data from the global regions that are represented in these samples of ascertained ethnic backgrounds, from healthy subjects and known age. However, limitations were the relatively uneven age distribution of the sample and the difficulty in collecting data from certain geographical areas. In fact, since the OPGs were selected retrospectively from data obtained for dental care, a limited number of OPGs was collected in Australia and North America, where no further information was available from entire regions.
Concerning the current challenges and future perspectives, this research could be the foundation for a further novel study in which a combined approach left–right third molar is reproduced on a potentially larger dataset and by applying an appropriate statistical methodology to verify its usefulness in obtaining better age assessment. Further studies can include and analyse all four third molars and compare the results with cases that consider one or both mandibular third molars.
Conclusion
According to the literature, this is the first work in which I3M is explored on both left and right lower third molar, utilizing a vast sample with origins in four different continents: Africa, America, Asia and Europe. The results presented here validated the use of both I3ML and I3MR in the process of assessing age in cases of legal inquiry on the 18-year-old threshold since the accuracy attained for I3M on both right and left sides was high and did not differ significantly. This work indicates that there is a need to further explore data interpretation in their transition to legal and civil contexts.
References
Santiago BM, Almeida L, Cavalcanti YW, Magno MB, Maia LC (2018) Accuracy of the third molar maturity index in assessing the legal age of 18 years: a systematic review and meta-analysis. Int J Legal Med 132(4):1167–1184. https://doi.org/10.1007/s00414-017-1766-4
De Luca S, Biagi R, Begnoni G, Farronato G, Cingolani M, Merelli V, Ferrante L, Cameriere R (2014) Accuracy of Cameriere’s cut-off value for third molar in assessing 18 years of age. Forensic Sci Int 235:102.e1-102.e1026. https://doi.org/10.1016/j.forsciint.2013.10.036
Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Rösing FW, Rötzscher K, Geserick G (2008) Criteria for age estimation in living individuals. Int J Legal Med 122(6):457–460
Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto JL, Schuliar Y et al (2009) The problem of ageing human remains and living individuals: a review. Forensic Sci Int 193:1e13
Adserias-Garriga J (2019) Evolution of methods and state-of-the-art in dental age estimation. Age Estimation 77–87. https://doi.org/10.1016/b978-0-12-814491-6.00006-6
Schmeling A, Black S (2010) An introduction to the history of age estimation in the living. In: Black S, Aggrawal A, Payne-James J (eds) Age Estimation in the Living. Wiley-Blackwell, West Sussex, pp 1–18.
Buken B, Safak AA, Yazici B, Buken E, Mayda AS (2007) Is the assessment of bone age by the Greulich-Pyle method reliable at forensic age estimation for Turkish children? Forensic Sci Int 173(2–3):146–153. https://doi.org/10.1016/j.forsciint.2007.02.023
Liversidge HM (2008) Dental age revisited. In: Irish JD, Nelson GC (eds) Technique and application in dental anthropology. Cambridge University Press, Cambridge, pp 234–252
Galić Vodanović Janković Mihanović Nakaš Prohić Galić Brkić IMSFESEH (2013) Dental age estimation on Bosnian- Herzegovinian children aged 6–14 years: evaluation of ’ ’Chaillet’s international maturity standards. J Forensic Legal Med 20:40–45. https://doi.org/10.1016/j.jflm.2012.04.037
Cameriere R, Brkić ErmencFerranteOvsenikCingolani HBLMM (2008) The measurement of open apices of teeth to test chronological age of over 14-year-olds in living subjects. Forensic Sci Int 174:217–221. https://doi.org/10.1016/j.forsciint.2007.04.220
Banks HV (1934) Incidence of third molar development. Angle Orthod 4:223–233. https://doi.org/10.1043/0003-3219(1934)004%3c0223:IOTMD%3e2.0.CO;2
Celikoglu M, Kazanci F, Miloglu O, Oztek O, Kamak H, Ceylan I (2010) Frequency and characteristics of tooth agenesis among an orthodontic patient population. Med Oral Patol Oral Cir Bucal 15:e797–e801. https://doi.org/10.4317/medoral.15.e797
Cole TJ (2015) The evidential value of developmental age imaging for assessing age of majority. Ann Hum Biol 42:379–388. https://doi.org/10.3109/03014460.2015.1031826
Rolseth V, Mosdøl A, Dahlberg PS, Ding Y, Bleka Ø, Skjerven-Martinsen M, Straumann GH, Delaveris GJM, Vist GE (2019) Age assessment by Demirjian’s development stages of the third molar: a systematic review. Eur Radiol 29(5):2311–2321. https://doi.org/10.1007/s00330-018-5761-z
Carter K, Worthington S (2015) Morphologic and demographic predictors of third molar agenesis: a systematic review and meta-analysis. J Dent Res 94(7):886–894. https://doi.org/10.1177/0022034515581644
Scheiwiller M, Oeschger ES, Gkantidis N (2020) Third molar agenesis in modern humans with and without agenesis of other teeth. Peer J 8:e10367. https://doi.org/10.7717/peerj.10367
De Bruyn L, Vranckx M, Jacobs R, Politis C (2020) A retrospective cohort study on reasons to retain third molars. Int J Oral Maxillofac Surg 49:816–821. https://doi.org/10.1016/j.ijom.2019.10.003
Van der Linden W, Cleaton-Jones P, Lownie M (1995) Diseases and lesions associated with third molars: review of 1001 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol 79(2):142–145
Kasper KA, Austin D, Kvanli AH, Rios TR, Senn DR (2009) Reliability of third molar development for age estimation in a Texas Hispanic population: a comparison study. J Forensic Sci 54(3):651–657. https://doi.org/10.1111/j.1556-4029.2009.01031.x
Mincer HH, Harris EF, Berryman HE (1993) The A.B.F.O. study of third molar development and its use as an estimator of chronological age. J Forensic Sci 38(2):379–390
Levesque GY, Demirjian A, Tanguay R (1981) Sexual dimorphism in the development, emergence, and agenesis of the mandibular third molar. J Dent Res 60(10):1735–1741
Olze A, Reisinger W, Geserick G, Schmeling A (2006) Age estimation of unaccompanied minors. Part II. Dental aspects. Forensic Sci Int 159(1):65–7
De Angelis D, Gibelli D, Merelli V, Botto M, Ventura F, Cattaneo C (2014) Application of age estimation methods based on teeth eruption: how easy is Olze method to use? Int J Legal Med 128:841–844
Thevissen PW, Pittayapat P, Fieuws S, Willems G (2009) Estimating age of majority on third molars developmental stages in young adults from Thailand using a modified scoring technique. J Forensic Sci 54(2):428–432
Cameriere R, Ferrante L, De Angelis D, Scarpino F, Galli F (2008) The comparison between measurement of open apices of third molars and Demirjian stages to test chronological age of over 18-year-olds in living subjects. Int J Legal Med 122(6):493–497. https://doi.org/10.1007/s00414-008-0279-6
Scandoni R, Zolotenkova GV, Vanin S, Pigolkin YI, Cameriere R (2020) Forensic validity of the third molar maturity index (I3M) for age estimation in a Russian population. Biomed Res Int Article ID 6670590. https://doi.org/10.1155/2020/6670590
Albernaz Neves J, Antunes-Ferreira N, Machado V, Botelho J, Proença L, Quintas A, Delgado AS, Mendes JJ, Cameriere R (2020) Validation of the Third molar maturation index (I3M) to assess the legal adult age in the Portuguese population. Sci Rep 10(1):18466. https://doi.org/10.1038/s41598-020-75324-x
Gómez Jiménez L, Palacio LAV, De Luca S, Vasquez YR, Capellán MC, Cameriere R (2019) Validation of the third molar maturity index (I3M): study of a Dominican Republic sample. J Forensic Odontostomatol 3(37):27–33
Khare P, Li J, Velandia Palacio LA, Galić I, Ferrante L, Cameriere R (2020) Validation of the third molar maturity index cut off value of <0.08 for indicating legal age of 18 years in Eastern Chinese region. Leg Med (Tokyo) 42:101645. https://doi.org/10.1016/j.legalmed.2019.101645
Nóbrega JBM, Protasio APL, Ribeiro ILA, Valença AMG, Santiago BM, Cameriere R (2019) Validation of the third molar maturation index to estimate the age of criminal responsibility in Northeastern Brazil. Forensic Sci Int 304:109917. https://doi.org/10.1016/j.forsciint.2019.109917
Kumagai A, Takahashi N, Palacio L, Giampieri A, Ferrante L, Cameriere R (2019) Accuracy of the third molar index cut-off value for estimating 18 years of age: validation in a Japanese samples. Leg Med (Tokyo) 38:5–9. https://doi.org/10.1016/j.legalmed.2019.03.001
Tafrount C, Galić I, Franchi A, Fanton L, Cameriere R (2019) Third molar maturity index for indicating the legal adult age in southeastern France. Forensic Sci Int 294:218.e1-218.e6. https://doi.org/10.1016/j.forsciint.2018.10.013
Spinas E, De Luca S, Lampis L, Velandia Palacio LA, Cameriere R (2018) Is the third molar maturity index (I3M) useful for a genetic isolate population? Study of a Sardinian sample of children and young adults. Int J Legal Med 132(6):1787–1794. https://doi.org/10.1007/s00414-018-1933-2
Różyło-Kalinowska I, Kalinowski P, Kozek M, Galić I, Cameriere R (2018) Validity of the third molar maturity index I3M for indicating the adult age in the Polish population. Forensic Sci Int 290:352.e1-352.e6. https://doi.org/10.1016/j.forsciint.2018.06.034
Antunovic M, Galic, I, Zelic K, Nedeljkovic N, Lazic E, Djuric M, Cameriere R (2018) The third molars for indicating legal adult age in Montenegro. Leg Med (Tokyo) 33:55–61. Advance online publication. https://doi.org/10.1016/j.legalmed.2018.05.006
Angelakopoulos N, De Luca S, Velandia Palacio LA, Coccia E, Ferrante L, Cameriere R (2018) Third molar maturity index (I3M) for assessing age of majority: study of a black South African sample. Int J Legal Med 132(5):1457–1464. https://doi.org/10.1007/s00414-018-1818-4
Cameriere R, Velandia Palacio LA, Pinares J, Bestetti F, Paba R, Coccia E, Ferrante L (2018) Assessment of second (I2M) and third (I3M) molar indices for establishing 14 and 16 legal ages and validation of the Cameriere’s I3M cut-off for 18 years old in Chilean population. Forensic Sci Int 285:205.e1-205.e5. https://doi.org/10.1016/j.forsciint.2017.12.043
Kelmendi J, Cameriere R, Koçani F, Galić I, Mehmeti B, Vodanović M (2018) The third molar maturity index in indicating the legal adult age in Kosovar population. Int J Legal Med 132(4):1151–1159. https://doi.org/10.1007/s00414-017-1761-9
Boyacıoğlu Doğru H, Gulsahi A, Çehreli SB, Galić I, van der Stelt P, Cameriere R (2018) Age of majority assessment in Dutch individuals based on Cameriere’s third molar maturity index. Forensic Sci Int 282:231.e1-231.e6. https://doi.org/10.1016/j.forsciint.2017.11.009
Balla SB, Galic IPK, Vanin S, De Luca S, Cameriere R (2017) Validation of third molar maturity index (I3M) for discrimination of juvenile/adult status in South Indian population. J Forensic Leg Med 49:2–7. https://doi.org/10.1016/j.jflm.2017.05.003
Quispe Lizarbe RJ, Solís Adrianzén C, Quezada-Márquez MM, Galić I, Cameriere R (2017) Demirjian’s stages and Cameriere’s third molar maturity index to estimate legal adult age in Peruvian population. Leg Med (Tokyo) 25:59–65. https://doi.org/10.1016/j.legalmed.2017.01.003
Dardouri A, Cameriere R, De Luca S, Vanin S (2016) Third molar maturity index by measurements of open apices in a Libyan sample of living subjects. Forensic Sci Int 267:230.e1-230.e6. https://doi.org/10.1016/j.forsciint.2016.07.020
Franklin D, Karkhanis S, Flavel A, Collini F, DeLuca S, Cameriere R (2016) Accuracy of a cut-off value based on the third molar index: Validation in an Australian population. Forensic Sci Int 266:575.e1-575.e6. https://doi.org/10.1016/j.forsciint.2016.06.032
Gulsahi A, De Luca S, Cehreli SB, Tirali RE, Cameriere R (2016) Accuracy of the third molar index for assessing the legal majority of 18 years in Turkish population. Forensic Sci Int 266:584.e1-584.e6. https://doi.org/10.1016/j.forsciint.2016.04.034
Cavrić J, Galić I, Vodanović M, Brkić H, Gregov J, Viva S, Rey L, Cameriere R (2016) Third molar maturity index (I3M) for assessing age of majority in a black African population in Botswana. Int J Legal Med 130(4):1109–1120. https://doi.org/10.1007/s00414-016-1344-1
De Luca S, Aguilar L, Rivera M, Palacio LA, Riccomi G, Bestetti F, Cameriere R (2016) Accuracy of cut-off value by measurement of third molar index: Study of a Colombian sample. Forensic Sci Int 261:160.e1-160.e1605. https://doi.org/10.1016/j.forsciint.2016.01.026
Zelic K, Galic I, Nedeljkovic N, Jakovljevic A, Milosevic O, Djuric M, Cameriere R (2016) Accuracy of Cameriere’s third molar maturity index in assessing legal adulthood on Serbian population. Forensic Sci Int 259:127–132. https://doi.org/10.1016/j.forsciint.2015.12.032
De Luca S, Pacifici A, Pacifici L, Polimeni A, Fischetto SG, Velandia Palacio LA, Vanin S, Cameriere R (2016) Third molar development by measurements of open apices in an Italian sample of living subjects. J Forensic Leg Med 38:36–42. https://doi.org/10.1016/j.jflm.2015.11.007
Deitos AR, Costa C, Michel-Crosato E, Galić I, Cameriere R, Biazevic MG (2015) Age estimation among Brazilians: Younger or older than 18? J Forensic Leg Med 33:111–115. https://doi.org/10.1016/j.jflm.2015.04.016
Galić I, Lauc T, Brkić H, Vodanović M, Galić E, Biazevic MG, Brakus I, Badrov J, Cameriere R (2015) Cameriere’s third molar maturity index in assessing age of majority. Forensic Sci Int 252:191.e1-191.e1915. https://doi.org/10.1016/j.forsciint.2015.04.030
Cameriere R, Santoro V, Roca R, Lozito P, Introna F, Cingolani M, Galić I, Ferrante L (2014) Assessment of legal adult age of 18 by measurement of open apices of the third molars: Study on the Albanian sample. Forensic Sci Int 245:205.e1-205.e2055. https://doi.org/10.1016/j.forsciint.2014.10.013
Cameriere R, Pacifici A, Viva S, Carbone D, Pacifici L, Polimeni A (2014) Adult or not? Accuracy of Cameriere’s cut-off value for third molar in assessing 18 years of age for legal purposes. Minerva Stomatol 63(9):283–294
Moukarzel M, Angelakopoulos N, De Luca S, Velandia Palacio LA, Aquilanti L, Coccia E, Pigolkin YI, Cameriere R (2020) Validity assessment of the third molar maturity index (I3M) in a Lebanese sample of adolescents and young adults. Aust J Forensic Sci. https://doi.org/10.1080/00450618.2020.1805008
AlQahtani S, Kawthar A, AlAraik A, AlShalan A (2017) Third molar cut-off value in assessing the legal age of 18 in Saudi population. Forensic Sci Int 272:64–67. https://doi.org/10.1016/j.forsciint.2017.01.004
Balla SB, Galic I, Karunakar P et al (2017) Validation of third molar maturity index (I3M) for discrimination of juvenile/adult status in South Indian population. J Forensic Legal Med 49:2–7. https://doi.org/10.1016/j.jflm.2017.05.003
Ribier L, Saint-Martin P, Seignier M, Paré A, Brunereau L, Rérolle C (2020) Cameriere’s third molar maturity index in assessing age of majority: a study of a French sample. Int J Legal Med 134(2):783–792. https://doi.org/10.1007/s00414-019-02123-z\
Aynsley-Green A (2009) Unethical age assessment. Br Dent J 206(7):337
Sykes L, Bhayat A, Bernitz H (2017) The effects of the refugee crisis on age estimation analysis over the past 10 years: a 16-country survey. Int J Environ Res Public Health 14(6):630. https://doi.org/10.3390/ijerph14060630
Garamendi PM, Landa MI, Ballesteros J, Solano MA (2005) Reliability of the methods applied to assess age minority in living subjects around 18 years old. A survey on a Moroccan origin population. Forensic Sci Int 154:3–12. https://doi.org/10.1016/j.forsciint.2004.08.018
Kapadia F, Stevens J, Silver D (2020) Dental radiographs for age estimation in US asylum seekers: methodological, ethical, and health issues. Am J Public Health 110(12):1786–1789
Willershausen B, Löffler N, Schulze R (2001) Analysis of 1202 orthopantograms to evaluate the potential of forensic age determination based on third molar developmental stages. Eur J Med Res 6(9):377–384
Blankenship JA, Mincer HH, Anderson KM, Woods MA, Burton EL (2007) Third molar development in the estimation of chronologic age in American blacks as compared with whites. J Forensic Sci 52(2):428–433
Bassed RB, Briggs C, Drummer OH (2012) The incidence of asymmetrical left/right skeletal and dental development in an Australian population and the effect of this on forensic age estimations. Int J Legal Med 126:251–257. https://doi.org/10.1007/s00414-011-0621-2
Cameriere R, De Luca S, Ferrante L (2021) Study of the ethnicity’s influence on the third molar maturity index (I3M) for estimating age of majority in living juveniles and young adults. Int J Legal Med. https://doi.org/10.1007/s00414-021-02622-y
Thevissen PW, Fieuws S, Willems G (2010) Human third molars development: Comparison of 9 country specific populations. Forensic Sci Int 201(1–3):102–105
Gleiser I, Hunt E (1955) The permanent mandibular first molar: its calcification, eruption and decay. Am J Phys Anthropol 13:253–283
Köhler S, Schmelzie R, Loitz C, Püschel K (1994) Development of wisdom teeth as a criterion of age determination. Ann Anat 176:339–345
Haglund M, Mörnstad H (2019) A systematic review and meta-analysis of the fully formed wisdom tooth as a radiological marker of adulthood. Int J Legal Med 133(1):231–239. https://doi.org/10.1007/s00414-018-1842-4
Koussoulakou DS, Margaritis LH, Koussoulakos SL (2009) A curriculum vitae of teeth: evolution, generation, regeneration. Int J Biol Sci 5(3):226
Upadhyaya C, Adhikari BR, Kafle D, Humagain M (2012) Agenesis of third molars in orthodontic patients attending Dhulikhel Hospital. Orthod J Nepal 2(1):32–35
Normando D (2015) Third molars: to extract or not to extract? Dental Press J Orthod 20(4):17–18. https://doi.org/10.1590/2176-9451.20.4.017-018.edt
Blakey GH, Marciani RD, Haug RH et al (2002) Periodontal pathology associated with asymptomatic third molars. J Oral Maxillofac Surg 60(11):1227–1233. https://doi.org/10.1053/joms.2002.35717
Fisher EL, Garaas R, Blakey GH et al (2012) Changes over time in the prevalence of caries experience or periodontal pathology on third molars in young adults. J Oral Maxillofac Surg 70(5):1016–1022. https://doi.org/10.1016/j.joms.2011.10.016
Vigneswaran AT, Shilpa S (2015) The incidence of cysts and tumors associated with impacted third molars. J Pharm Bioallied Sci 7(1):S251–S254. https://doi.org/10.4103/0975-7406.155940
Santosh P (2015) Impacted mandibular third molars: review of literature and a proposal of a combined clinical and radiological classification. Ann Med Health Sci Res 5(4):229–234. https://doi.org/10.4103/2141-9248.160177
Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol 211–227
Doyle E, Márquez-Grant N, Field L, Holmes T, Arthurs OJ, van Rijn RR, Garamendi PM (2019) Guidelines for best practice: imaging for age estimation in the living. J Forensic Radiol Imaging 16:38–49
Lucas VS, McDonald F, Andiappan M, Roberts G (2017) Dental age estimation: periodontal ligament visibility (PLV)-pattern recognition of a conclusive mandibular maturity marker related to the lower left third molar at the 18-year threshold. Int J Legal Med 131(3):797–801. https://doi.org/10.1007/s00414-016-1468-3
Liversidge HM, Molleson TI (1999) Developing permanent tooth length as an estimate of age. J Forensic Sci 44(5):917–920 (PMID: 10486941)
Thevissen PW, Fieuws S, Willems G (2011) Third molar development: measurements versus scores as age predictor. Arch Oral Biol 56(10):1035–1040
Sharma P, Wadhwan V, Sharma N (2018) Reliability of determining the age of majority: a comparison between measurement of open apices of third molars and Demirjian stages. J Forensic Odontostomatol 36(2):2–9
Chaillet N, Demirjian A (2004) Dental maturity in South France: a comparison between Demirjian’s method and polynomial functions. J Forensic Sci 49:1059–1066
Liversidge HM, Marsden PH (2010) Estimating age and the likelihood of having attained 18 years of age using mandibular third molars. Br Dent J 209(8):E13. https://doi.org/10.1038/sj.bdj.2010.976
Acknowledgements
The authors would like to thank Adriana Santos, Ana Rodrigues and Rui Santos, researchers from the Portuguese Institution CEAUL, under FCT – Fundação para a Ciência e a Tecnologia and the project UIDB/00006/2020, and the Clinic of Dentistry at the Universidad Científica del Sur (Perú).
Funding
Inês Oliveira-Santos is supported by a FCT-Fundação para a Ciência e Tecnologia grant (SFRH/BD/139158/2018).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This research study was conducted retrospectively from OPGs obtained for clinical purposes. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
According to the journal’s submission guidelines, an informed consent to participate in the study is not necessary for images such as x-rays.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Angelakopoulos, N., Galić, I., Balla, S.B. et al. Comparison of the third molar maturity index (I3M) between left and right lower third molars to assess the age of majority: a multi-ethnic study sample. Int J Legal Med 135, 2423–2436 (2021). https://doi.org/10.1007/s00414-021-02656-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-021-02656-2