
Abstract
Purpose
This study aimed to examine reports of cardiovascular adverse events (CV AEs) observed in the real-world during treatment with aclidinium, tiotropium, glycopyrronium, and umeclidinium alone or in combination with a LABA and, in the context of triple therapy, with the addition of an ICS, and submitted to the food and drug administration adverse event reporting system (FAERS).
Methods
A retrospective disproportionality analysis was conducted utilizing CV AE reports submitted to the FAERS from January 2020 to 30 September 2023. Disproportionality was measured by calculating the reporting odds ratio.
Results
Compared with ipratropium, tiotropium was associated with fewer reports of CV AEs. Compared with tiotropium, other LAMAs were more likely to be associated with reports of CV AEs. Combinations of glycopyrronium with indacaterol or formoterol and umeclidinium with vilanterol significantly reduced reports of CV AEs compared with the respective LAMA. The addition of an ICS to these combinations further reduced the risk of CV AE reports.
Conclusion
Our study suggests that inhaled LAMAs are not free from cardiac AE risks. This risk may be more evident when the newer LAMAs are used, but it is generally significantly reduced when COPD patients are treated with dual bronchodilators or triple therapy. However, these results do not prove that LAMAs cause CV AEs, as FAERS data alone are not indicative of a drug’s safety profile. Given the frequency with which COPD and cardiovascular disease co-exist, a large study in the general population could shed light on this very important issue.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Long-acting muscarinic receptor (mAChR) antagonists (LAMAs), given as monotherapy or in combination with a long-acting β2-agonist (LABA) and, often, an inhaled corticosteroid (ICS), are widely prescribed for the treatment of chronic obstructive pulmonary disease (COPD) [1]. However, there are concerns about possible associations between their use and cardiovascular disease (CVD) [2, 3].
One observational study using health administrative data from Ontario (Canada) reported a significantly increased CV risk associated with the new use of LAMAs compared with to non-use of this class of bronchodilators [4]. However, according to a systematic review and meta-analysis of the currently available literature on their CV adverse events (AEs), LAMAs appear to be safe even in patients with heart disease, compared with other active drugs or a placebo [5].
Although pivotal clinical trials have provided much of the current information, the AE rates seen in such trials may not reflect those seen in real-world practice [6]. Therefore, real-world studies are needed to identify high-risk individuals who may benefit from electrocardiogram (ECG) monitoring [3], particularly as the CV response to mAChR blockade may vary between patients and with underlying comorbidities [7].
Four LAMAs are approved for the treatment of COPD: aclidinium bromide, tiotropium bromide, glycopyrronium bromide, and umeclidinium bromide. While the pharmacological profiles of these LAMAs differ, all four have a longer residence time at the M3 mAChR, whose blockade causes airway smooth muscle relaxation, and a shorter residence time at the M2 mAChR compared to short-acting mAChR antagonists (SAMAs), such as ipratropium bromide, which have non-selective binding properties [8]. Differences in the pharmacological properties of these LAMAs suggest that there may be different effects on the heart depending on the agent used. However, no clinical trials have addressed this issue, and there is still a lack of general analysis of the potential CV risk of different LAMAs.
In this study, we reviewed data from the US Food and Drug Administration’s (FDA) adverse event reporting system (FAERS) to examine reports of CV AEs observed in the real-world during treatment with aclidinium, tiotropium, glycopyrronium, and umeclidinium alone or in combination with a LABA and, in the context of triple therapy, with the addition of an ICS.
Materials and Methods
The FAERS is a centralized, computerized information database that collects spontaneous reports of AEs associated with the administration of drugs and therapeutic biologics submitted directly by healthcare personnel and consumers or indirectly through manufacturers from the US and other countries using MedWATCH program submission forms [9]. It provides a helpful insight into the AE profile of drugs because of the broad exposure to a given drug in the real-world population and the large sample size with a wide range of AE reports [10].
The FAERS codes AEs based on the preferred term (PT) level of the standardized terminology of the medical dictionary for regulatory activities (MedDRA) Version 26.1. In the present analysis, AEs coded by PTs belonging to the MedDRA system organ classes “cardiac disorder’” were considered outcomes of interest. A narrower version examined standardized MedDRA queries. We assessed “cardiac arrhythmias,” “cardiac failure,” and “ischemic heart disease” because there is evidence that inhaled mAChR antagonists induce pro-arrhythmic and pro-ischemic effects [11], and there is also some, although inconsistent, evidence of an increased risk of heart failure (HF) with the use of these drugs [12]. We were aware that each report could include one or more CV AEs, as highlighted by FEARS.
Disproportionality in pharmacovigilance occurs when a drug is associated with an AE [13]. Since only odds ratios can be obtained for studies in which it is typically not possible to estimate the population at risk [14], as in the case of our investigation, we used the reported odds ratio (ROR) to find statistical associations between CV AEs and LAMAs. The ROR is a disproportionate measure based on the ratio of the odds of cases in reports for a given drug to the odds in reports where that drug is not present in the FAERS database [15]. A 95% confidence interval (CI) lower limit greater than one was considered a statistically significant ROR if there were at least 3 cases [16].
For the scope of the present study, we considered reports submitted to the FAERS database from January 2020 to 30 September 2023. All reports with generic LAMA names (aclidinium bromide, glycopyrrolate, glycopyrronium, tiotropium, tiotropium bromide, tiotropium bromide anhydrous, tiotropium bromide monohydrate, umeclidinium, umeclidinium bromide) were extracted. As a significant effect of exposure to ipratropium bromide on the risk of CV AEs has been reported [17], we also included data on this relatively non-selective SAMA (ipratropium, ipratropium bromide, ipratropium bromide anhydrous) in the analysis for comparison with tiotropium. Tiotropium was the first LAMA to enter daily use and remains the most prescribed compound in this class of bronchodilators, at least in the US [18].
As data in the FAERS database are anonymized, ethics committee approval was not required for this analysis.
Results
We examined 18,208 reports of AEs that occurred during treatment with a LAMA, with the majority (12,472) attributed to tiotropium. There were more AEs in females than in males (9832 vs. 6231), at least in cases where sex was reported. The highest prevalence of AEs was in the age group 65–85 years (5771 reports), followed by the age group younger than 65 years (5054 reports).
There were 2261 CV AEs reported (12.4% of the total), with a higher number of males (1055) than females (940). The age group 65–85 years also had the highest number of reports of CV AEs (941), followed by the age group younger than 65 years (702 reports).
Compared to ipratropium, tiotropium was associated with fewer reports of CV AEs [ROR 0.53 (0.48–0.58)].
Table 1 shows the number of reported cases of cardiac disorders with each LAMA, then subdivided by sex and age of patients.
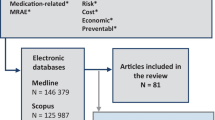
Compared to tiotropium, other LAMAs were more likely to be associated with reports of CV AEs. In this case, the ROR was the ratio of the odds of the number of CV events associated with tiotropium to those associated with other LAMAs [aclidinium: ROR 1.60 (1.36–1.89); glycopyrronium: ROR 2.26 (1.99–2.57); umeclidinium: ROR 1.95 (1.73–2.19)] (Fig. 1).

Forest plots of disproportionality [reported odds ratio (ROR)] of LAMAs and cardiovascular events compared with tiotropium
As glycopyrronium and umeclidinium were developed with a LABA and as part of a triple therapy with an ICS, we calculated the ROR of dual bronchodilators and triple combinations compared with LAMA monotherapy (Fig. 2). Compared with glycopyrronium monotherapy, glycopyrronium/indacaterol and glycopyrronium/indacaterol/mometasone were associated with significantly fewer reports of CV AEs, with RORs of 0.79 [0.64–0.97] and 0.62 [0.37–1.02], respectively. This was also the case when formoterol was added to glycopyrronium, with a ROR compared to glycopyrronium monotherapy of < 1 [0.12 (0.06–0.20)]. The addition of budesonide did not significantly change this ROR [0.17 (0.14–0.20)]. Similarly, umeclidinium/vilanterol and umeclidinium/vilanterol/fluticasone furoate were associated with significantly fewer reports of CV AEs compared to umeclidinium alone [ROR 0.35 (0.30–0.41) and 0.20 (0.18–0.23), respectively].

Forest plots of disproportionality [reported odds ratio (ROR)] of dual bronchodilation and triple therapy including glycopyrronium or umeclidinium, respectively, and cardiovascular events compared with glycopyrronium or umeclidinium. F formoterol, FF fluticasone furoate, G glycopyrronium, I indacaterol, M mometasone, U umeclidinium, V vilanterol
Table 2 describes the impact of each LAMA on the three main subgroups of CV AEs (arrhythmia, HF, and ischemic heart disease). Compared to all reports of CV AEs in the three groups considered, aclidinium had the lowest percentage of events assigned to the arrhythmia group. In contrast, more than 50% of the reports of CV AEs during treatment with umeclidinium were assigned to this group. The opposite was true when looking at events in the ischemic heart disease subgroup, with umeclidinium having the lowest and aclidinium the highest percentage compared to the total number of CV AEs reported.
Discussion
The results of this retrospective pharmacovigilance analysis documented that the use of tiotropium significantly reduced the reporting of CV AEs compared with ipratropium while the other three LAMAs (aclidinium, glycopyrrolate, and umeclidinium), which were introduced into clinical use after tiotropium, were found to be associated with more reported cardiac AEs than tiotropium, although the available evidence from randomized controlled trials (RCTs) generally emphasizes the CV safety of these LAMA.
The glycopyrronium data were completely unexpected. It is the only mAChR antagonist to date to have a greater relative affinity for M3 than M2 mAChRs [19]. Glycopyrronium had a lower M2 mAChR occupancy and a safer CV profile than tiotropium in an integrated rat model [20]. The percentage of patients with new or worsened clinically significant QTcF values was slightly higher with tiotropium (5.8%) than with glycopyrronium (4.0%) when these two LAMAs were compared in the GLOW5 clinical trial [21]. However, two patients on glycopyrronium had QTcF values > 480 ms compared with none on tiotropium and the percentage of patients with an increase in QTcF of 30–60 ms from baseline was slightly higher in the glycopyrronium group (3.4% vs. 3.0%). Furthermore, in a recent real-world study on the safety and efficacy of glycopyrronium in Japanese patients with COPD, the incidence of cardiac AEs was 2.98% [22]. The common AEs were HF in 0.55%, myocardial infarction in 0.39%, angina pectoris and ventricular extrasystoles in 0.31% of patients each.
Aclidinium also exhibits M3 mAChRs versus M2 mAChRs selectivity and, unlike other LAMAs, is rapidly hydrolyzed in human plasma into an acid and an alcohol metabolite, neither of which binds to mAChRs [23]. A post-approval safety study, conducted in the United Kingdom using de-identified data from primary care practices, showed that the crude incidence rates per 1000 person-years of acute myocardial infarction during current use were 10.29 for aclidinium, 11.33 for tiotropium, and 11.86 for other LAMAs, while those for major adverse cardiac events (MACE) were 16.00, 17.98, and 18.18, respectively [24]. In addition, a North American RCT proved that aclidinium was non-inferior to placebo for the risk of MACE in patients with COPD and increased CV risk over 3 years [25].
Umeclidinium exhibits kinetic selectivity for M3 over M2 mAChRs and dissociates more slowly from M3 mAChRs than from M2 mAChRs (half-lives: 82 and 9 min, respectively) [26]. Its dissociation from M2 and M3 mAChRs is faster than that of tiotropium (approximately four and three times faster, respectively). Studies using monotherapy for more than four weeks showed that both umeclidinium 62.5 μg and 125 μg caused cardiac-related AEs compared to placebo [27]. Supraventricular tachycardia, atrial ectopy, and atrial fibrillation were the most common AEs. However, there was no evidence of a higher risk of significant MACEs with either doses of umeclidinium compared to placebo. On the other hand, umeclidinium was associated with a higher incidence of several CV events and post-baseline ECG abnormalities in subjects with underlying CV risk factors compared to placebo [28]. However, to the best of our knowledge, there is no direct or indirect comparison between umeclidinium monotherapy and tiotropium monotherapy in terms of CV risk.
It is difficult to explain the discrepancy between what has been reported in the literature and what was observed in this study. It has been suggested that there may be a variable CV response to mAChR antagonism in individual patients [29]. Regulator of G protein signaling 6 (RGS6), which accelerates the deactivation kinetics of the G protein-gated K+ channel (IKACh) in sinoatrial node cells and atrial myocytes, thereby limiting parasympathetic activation to avoid parasympathetic override and severe bradycardia, controls the duration of G protein activation in the heart [30]. Altered parasympathetic signaling through the M2 mAChR-IKACh pathway may affect ventricular electrophysiological properties distinct from its influence on atrial physiology [31]. A genetic predisposition associated with a modification of RGS6 may influence the onset of CV AEs [32]. The chance of treating patients who are particularly sensitive to M2 mAChR blockade is certainly greater in an unselected general population. However, this does not explain the difference between tiotropium and the other LAMAs.
Cell-to-cell communication and ACh-induced endothelium-dependent dilation of coronary arteries are mediated by activation of M3 mAChRs present in cardiac cells [33], which also stimulates the delayed rectifier potassium current, thereby regulating cardiac rhythm and repolarization and exerting cytoprotective effects against myocardial damage, including ischemia [34, 35]. The function of these mAChRs may become prominent in pathological conditions such as cardiac ischemia, pathological cardiac hypertrophy, arrhythmia, and HF [34]. Blocking M3 mAChRs with mAChR antagonism abolishes this protective effect.
When cardiac M3 mAChR activity is increased, a greater M3/M2 mAChR selectivity may be an issue. Aclidinium [36], glycopyrrolate [37], and umeclidinium [26] have higher M3/M2 mAChR selectivity than tiotropium, which may explain why more CV AEs have been reported in users of these three LAMAs. However, lack of specific information on pathological conditions of patients with reported cardiac disorders prevents confirmation of this hypothesis. Given the frequency with which COPD and CVD co-exist, an appropriate study could shed light on this issue that is of great importance [29, 38].
Not surprisingly, the addition of a LABA to a LAMA reduces the likelihood of reported cardiac events. Although there are concerns about the possible association between the use of dual bronchodilators and CV morbidity in patients with COPD, as LABAs also have a high potential to influence cardiac activity [6], the COPD and Systemic Consequences-Comorbidities Network (COSYCONET) observational study documented the beneficial effect of dual bronchodilation on the CV system [39]. In addition, a systematic review with meta-analysis that included data from trials of at least 3 months duration showed that umeclidinium/vilanterol appeared to provide a protective signal against cardiac AEs, whereas glycopyrrolate/indacaterol significantly protected against such events compared with mono-components [40]. However, the data from these studies were mainly derived from patients selected for enrollment in RCTs, who generally do not have severe CV morbidity.
A likely explanation for the reduced risk of cardiac AEs with dual bronchodilation is related to the deflating effect of this therapy, with less compression of the pulmonary microcirculation and increasing perfusion [41]. In patients with moderate to severe COPD and pulmonary hyperinflation, a 14-day course of LAMA + LABA resulted in significant lung deflation, normalized biventricular end-diastolic volumes, and improved cardiac filling [42]. Another closely related mechanism is improved regional ventilation due to bronchodilation [43]. An increase in regional ventilation could improve the ventilation-perfusion mismatch, thereby improving the venous blood flow in the left heart.
Adding an ICS to glycopyrronium/indacaterol and umeclidinium/vilanterol extended the significant reduction in the risk of CV AEs observed with dual bronchodilation versus LAMA alone. This is not surprising, as a recent random-effects meta-analysis documented an association between ICS-containing medications and reduced CV risk in COPD patients [44]. In any case, it should be mentioned that glycopyrronium/indacaterol/mometasone has only been approved for asthma treatment.
While the results of this research are certainly interesting, they do not document that LAMAs cause CV AEs [9]. The reliance on FAERS data alone is not sufficient to determine the safety profile of a drug [9]. In fact, stablishing a cause-and-effect relationship between a drug and an AE is not possible with FAERS data because the total number of patients using the drug is not available in the database. Consequently, the incidence of AEs cannot be accurately calculated and only a rough estimate based on the signal strength (ROR value) is possible. Furthermore, it is important to recognize that our analysis is subject to inherent bias due to the FAERS spontaneous reporting mechanism. AE reports are voluntarily submitted by healthcare providers, consumers, and manufacturers. Therefore, they may contain false, exaggerated, inaccurate, incomplete, and delayed information. In addition, these reports often lack medical review, increasing the likelihood of misclassification of cases. In our study, the fact that most reports concerned tiotropium and that it was not possible to adjust for underlying comorbidities and duration of treatment were other limitations.
Nevertheless, despite these limitations, our study suggests that inhaled LAMAs are not free from cardiac AE risks. This risk may be more evident when the newer LAMAs are used but it is generally significantly reduced when COPD patients are treated with dual bronchodilators or triple therapy.
References
Bloom CI, Montonen J, Jöns O, Garry EM, Bhatt SP (2022) First maintenance therapy for chronic obstructive pulmonary disease: retrospective analyses of US and UK healthcare databases. Pulm Ther 8(1):57–74. https://doi.org/10.1007/s41030-021-00179-0
Cazzola M, Page C, Matera MG (2013) Long-acting muscarinic receptor antagonists for the treatment of respiratory disease. Pulm Pharmacol Ther 26(3):307–317. https://doi.org/10.1016/j.pupt.2012.12.006
Stolz D, Cazzola M (2020) Characterising the cardiovascular safety profile of inhaled muscarinic receptor antagonists. In: Martínez-García MA, Pépin J-L, Cazzola M (eds) Cardiovascular complications of respiratory disorders (ERS monograph). European Respiratory Society, Sheffield, pp 238–250
Gershon A, Croxford R, Calzavara A, To T, Stanbrook MB, Upshur R, Stukel TA (2013) Cardiovascular safety of inhaled long-acting bronchodilators in individuals with chronic obstructive pulmonary disease. JAMA Intern Med 173(13):1175–1185. https://doi.org/10.1001/jamainternmed.2013.1016
Zhang C, Zhang M, Wang Y, Xiong H, Huang Q, Shuai T, Liu J (2021) Efficacy and cardiovascular safety of LAMA in patients with COPD: a systematic review and meta-analysis. J Investig Med 69(8):1391–1398. https://doi.org/10.1136/jim-2021-001931
Matera MG, Rogliani P, Calzetta L, Cazzola M (2016) Safety considerations with dual bronchodilator therapy in COPD: an update. Drug Saf 39(6):501–508. https://doi.org/10.1007/s40264-016-0402-4
Cazzola M, Calzetta L, Rogliani P, Matera MG (2017) Tiotropium formulations and safety: a network meta-analysis. Ther Adv Drug Saf 8(1):17–30. https://doi.org/10.1177/2042098616667304
Matera MG, Belardo C, Rinaldi M, Rinaldi B, Cazzola M (2020) Emerging muscarinic receptor antagonists for the treatment of asthma. Expert Opin Emerg Drugs 25(2):123–130. https://doi.org/10.1080/14728214.2020.1758059
U.S. Food and Drug Administration (2023) FDA adverse event reporting system (FAERS) public dashboard. https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard. Accessed 15 Dec 2023
Silberstein SD, Reshef S, Cohen JM, Gandhi S, Seminerio M, Ramirez Campos V, Kessler Y, Thompson SF, Blumenfeld A (2023) Adverse events reported with therapies targeting the CGRP pathway during the first 6 months post-launch: a retrospective analysis using the FDA adverse events reporting system. Adv Ther 40(2):445–459. https://doi.org/10.1007/s12325-022-02346-4
Singh S, Loke YK, Enright P, Furberg CD (2013) Pro-arrhythmic and pro-ischaemic effects of inhaled anticholinergic medications. Thorax 68(1):114–116. https://doi.org/10.1136/thoraxjnl-2011-201275
Verhamme KM, Afonso AS, van Noord C, Haag MD, Koudstaal PJ, Brusselle GG, Sturkenboom MC (2012) Tiotropium Handihaler and the risk of cardio- or cerebrovascular events and mortality in patients with COPD. Pulm Pharmacol Ther 25(1):19–26. https://doi.org/10.1016/j.pupt.2011.10.004
Caster O, Aoki Y, Gattepaille LM, Grundmark B (2020) Disproportionality analysis for pharmacovigilance signal detection in small databases or subsets: recommendations for limiting false-positive associations. Drug Saf 43(5):479–487. https://doi.org/10.1007/s40264-020-00911-w
Sedgwick P (2013) Case-control studies: measures of risk. BMJ 346:f1185. https://doi.org/10.1136/bmj.f1185
Rothman KJ, Lanes S, Sacks ST (2004) The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidemiol Drug Saf 13(8):519–523. https://doi.org/10.1002/pds.1001
Zhai Y, Ye X, Hu F, Xu J, Guo X, Zhuang Y, He J (2019) Endocrine toxicity of immune checkpoint inhibitors: a real-world study leveraging US Food and drug administration adverse events reporting system. J Immunother Cancer 7(1):286. https://doi.org/10.1186/s40425-019-0754-2
Ogale SS, Lee TA, Au DH, Boudreau DM, Sullivan SD (2010) Cardiovascular events associated with ipratropium bromide in COPD. Chest 137(1):13–19. https://doi.org/10.1378/chest.08-2367
ClinCalc.com (2023) Tiotropium. Drug usage statistics, United States, 2013–2020. https://clincalc.com/DrugStats/Drugs/Tiotropium. Accessed 18 Dec 2023
Tashkin DP, Gross NJ (2018) Inhaled glycopyrrolate for the treatment of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis 13:1873–1888. https://doi.org/10.2147/COPD.S162646
Trifilieff A, Ethell BT, Sykes DA, Watson KJ, Collingwood S, Charlton SJ, Kent TC (2015) Comparing the cardiovascular therapeutic indices of glycopyrronium and tiotropium in an integrated rat pharmacokinetic, pharmacodynamic and safety model. Toxicol Appl Pharmacol 287(1):9–16. https://doi.org/10.1016/j.taap.2015.05.012
Chapman KR, Beeh KM, Beier J, Bateman ED, D’Urzo A, Nutbrown R, Henley M, Chen H, Overend T, D’Andrea P (2014) A blinded evaluation of the efficacy and safety of glycopyrronium, a once-daily long-acting muscarinic antagonist, versus tiotropium, in patients with COPD: the GLOW5 study. BMC Pulm Med 14:4. https://doi.org/10.1186/1471-2466-14-4
Kato C, Wang D, Nakamura N, Sasajima T, Yoshisue H (2022) Real-world safety and efficacy of glycopyrronium bromide in Japanese patients with COPD: a 52-week post-marketing surveillance. Open Respir Med J 16:e187430642112240. https://doi.org/10.2174/18743064-v16-e2112240
Gavaldà A, Ramos I, Carcasona C, Calama E, Otal R, Montero JL, Sentellas S, Aparici M, Vilella D, Alberti J, Beleta J, Miralpeix M (2014) The in vitro and in vivo profile of aclidinium bromide in comparison with glycopyrronium bromide. Pulm Pharmacol Ther 28(2):114–121. https://doi.org/10.1016/j.pupt.2014.05.005
Rebordosa C, Plana E, Rubino A, Aguado J, Martinez D, Lei A, Daoud S, Saigi-Morgui N, Perez-Gutthann S, Rivero-Ferrer E (2022) Risk assessment of acute myocardial infarction and stroke associated with long-acting muscarinic antagonists, alone or in combination, versus long-acting beta2-agonists. Int J Chron Obstruct Pulmon Dis 17:1715–1733. https://doi.org/10.2147/COPD.S363997
Wise RA, Chapman KR, Scirica BM, Bhatt DL, Daoud SZ, Zetterstrand S, Reisner C, Gil EG (2019) Effect of aclidinium bromide on major cardiovascular events and exacerbations in high-risk patients with chronic obstructive pulmonary disease: the ASCENT-COPD randomized clinical trial. JAMA 321(17):1693–1701. https://doi.org/10.1001/jama.2019.4973
Salmon M, Luttmann MA, Foley JJ, Buckley PT, Schmidt DB, Burman M, Webb EF, DeHaas CJ, Kotzer CJ, Barrett VJ, Slack RJ, Sarau HM, Palovich MR, Lainé DI, Hay DW, Rumsey WL (2013) Pharmacological characterization of GSK573719 (umeclidinium): a novel, long-acting, inhaled antagonist of the muscarinic cholinergic receptors for treatment of pulmonary diseases. J Pharmacol Exp Ther 345(2):260–270. https://doi.org/10.1124/jpet.112.202051
Babu KS, Morjaria JB (2017) Umeclidinium in chronic obstructive pulmonary disease: latest evidence and place in therapy. Ther Adv Chronic Dis 8(4–5):81–91. https://doi.org/10.1177/2040622317700822
Donohue JF, Niewoehner D, Brooks J, O’Dell D, Church A (2014) Safety and tolerability of once-daily umeclidinium/vilanterol 125/25 mcg and umeclidinium 125 mcg in patients with chronic obstructive pulmonary disease: results from a 52-week, randomized, double-blind, placebo-controlled study. Respir Res 15(1):78. https://doi.org/10.1186/1465-9921-15-78
Cazzola M, Calzetta L, Rinaldi B, Page C, Rosano G, Rogliani P, Matera MG (2017) Management of chronic obstructive pulmonary disease in patients with cardiovascular diseases. Drugs 77(7):721–732. https://doi.org/10.1007/s40265-017-0731-3
Posokhova E, Ng D, Opel A, Masuho I, Tinker A, Biesecker LG, Wickman K, Martemyanov KA (2013) Essential role of the m2R-RGS6-IKACh pathway in controlling intrinsic heart rate variability. PLoS ONE 8(10):e76973. https://doi.org/10.1371/journal.pone.0076973
Kulkarni K, Xie X, Fernandez M, de Velasco E, Anderson A, Martemyanov KA, Wickman K, Tolkacheva EG (2018) The influences of the M2R-GIRK4-RGS6 dependent parasympathetic pathway on electrophysiological properties of the mouse heart. PLoS ONE 13(4):e0193798. https://doi.org/10.1371/journal.pone.0193798
Rorabaugh BR, Chakravarti B, Mabe NW, Seeley SL, Bui AD, Yang J, Watts SW, Neubig RR, Fisher RA (2017) Regulator of G protein signaling 6 protects the heart from ischemic injury. J Pharmacol Exp Ther 360(3):409–416. https://doi.org/10.1124/jpet.116.238345
Patanè S (2014) M3 muscarinic acetylcholine receptor in cardiology and oncology. Int J Cardiol 177(2):646–649. https://doi.org/10.1016/j.ijcard.2014.09.178
Hang P, Zhao J, Qi J, Wang Y, Wu J, Du Z (2013) Novel insights into the pervasive role of M3 muscarinic receptor in cardiac diseases. Curr Drug Targets 14(3):372–377. https://doi.org/10.2174/138945013804998963
Saternos HC, Almarghalani DA, Gibson HM, Meqdad MA, Antypas RB, Lingireddy A, AbouAlaiwi WA (2018) Distribution and function of the muscarinic receptor subtypes in the cardiovascular system. Physiol Genom 50(1):1–9. https://doi.org/10.1152/physiolgenomics.00062.2017
Gavaldà A, Miralpeix M, Ramos I, Otal R, Carreño C, Viñals M, Doménech T, Carcasona C, Reyes B, Vilella D, Gras J, Cortijo J, Morcillo E, Llenas J, Ryder H, Beleta J (2009) Characterization of aclidinium bromide, a novel inhaled muscarinic antagonist, with long duration of action and a favorable pharmacological profile. J Pharmacol Exp Ther 331(2):740–751. https://doi.org/10.1124/jpet.109.151639
Buhl R, Banerji D (2012) Profile of glycopyrronium for once-daily treatment of moderate-to-severe COPD. Int J Chron Obstruct Pulmon Dis 7:729–741. https://doi.org/10.2147/COPD.S36001
Cazzola M, Rogliani P, Matera MG (2015) Cardiovascular disease in patients with COPD. Lancet Respir Med 3(8):593–595. https://doi.org/10.1016/S2213-2600(15)00279-9
Kellerer C, Kahnert K, Trudzinski FC, Lutter J, Berschneider K, Speicher T, Watz H, Bals R, Welte T, Vogelmeier CF, Jörres RA, Alter P (2021) COPD maintenance medication is linked to left atrial size: results from the COSYCONET cohort. Respir Med 185:106461. https://doi.org/10.1016/j.rmed.2021.106461
Calzetta L, Rogliani P, Matera MG, Cazzola M (2016) A systematic review with meta-analysis of dual bronchodilation with LAMA/LABA for the treatment of stable COPD. Chest 149(5):1181–1196. https://doi.org/10.1016/j.chest.2016.02.646
Cazzola M, Page C, Rogliani P, Calzetta L, Matera MG (2022) Dual bronchodilation for the treatment of COPD: from bench to bedside. Br J Clin Pharmacol 88(8):3657–3673. https://doi.org/10.1111/bcp.15390
Hohlfeld JM, Vogel-Claussen J, Biller H, Berliner D, Berschneider K, Tillmann HC, Hiltl S, Bauersachs J, Welte T (2018) Effect of lung deflation with indacaterol plus glycopyrronium on ventricular filling in patients with hyperinflation and COPD (CLAIM): a double-blind, randomised, crossover, placebo-controlled, single-centre trial. Lancet Respir Med 6(5):368–378. https://doi.org/10.1016/S2213-2600(18)30054-7
Vogel-Claussen J, Schönfeld CO, Kaireit TF, Voskrebenzev A, Czerner CP, Renne J, Tillmann HC, Berschneider K, Hiltl S, Bauersachs J, Welte T, Hohlfeld JM (2019) Effect of indacaterol/glycopyrronium on pulmonary perfusion and ventilation in hyperinflated patients with chronic obstructive pulmonary disease (CLAIM): a double-blind, randomized crossover trial. Am J Respir Crit Care Med 199(9):1086–1096. https://doi.org/10.1164/rccm.201805-0995OC
Gadhvi K, Kandeil M, Raveendran D, Choi J, Davies N, Nanchahal S, Wing O, Quint J, Whittaker H (2023) Inhaled corticosteroids and risk of cardiovascular disease in chronic obstructive pulmonary disease: a systematic review and meta-regression. Chronic Obstr Pulm Dis 10(3):317–327. https://doi.org/10.15326/jcopdf.2022.0386
Funding
Open access funding provided by Università degli Studi di Roma Tor Vergata within the CRUI-CARE Agreement. The authors have not disclosed any funding.
Author information
Authors and Affiliations
Contributions
MGM and MC contributed to the study design. MGM and MC contributed to the data collection and collation. MC was responsible for the statistical analysis. All authors contributed to the interpretation of the data, participated in the writing and critical revision of the manuscript, and have approved the final version for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Matera, M.G., Calzetta, L., Rogliani, P. et al. Cardiovascular Events with the Use of Long-Acting Muscarinic Receptor Antagonists: An Analysis of the FAERS Database 2020–2023. Lung 202, 119–125 (2024). https://doi.org/10.1007/s00408-024-00677-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-024-00677-3