
Abstract
Purpose
Few studies have examined locations of noninvasive ventilation (NIV) application for acute respiratory failure (ARF). We aimed to track actual locations of NIV delivery and related outcomes.
Methods
Observational cohort study based at 8 acute care hospitals in Massachusetts on adult patients admitted for ARF requiring ventilatory support during pre-determined time intervals.
Results
Of 1225 ventilator starts, 499 were NIV; 209 (42 %) in intensive care units (ICU), 185 (37 %) in emergency departments (ED), 91 (18 %) on general wards, and 14 (3 %) in other units. Utilization (% of all ventilator starts) (1), success (2) and in-hospital mortality (3) rates for patients initiated on NIV in ICU, ED, and general and other wards were (1) 38, 36, 73, and 52 %, (2) 60, 77, 68, and 93 % and (3) 25, 12, 17, and 0 %, respectively (p < 0.05 for all). Patients with acute-on-chronic lung disease (ACLD) and acute pulmonary edema (APE) were begun on NIV most often in EDs and patients with ‘de novo’ ARF and neurologic disorders most often in ICU’s. Approximately 2/3 of patients begun on NIV outside of ICUs were transferred within 72 h to ICUs, wards or other units.
Conclusions
Most NIV starts occurred in ICUs and EDs but utilization rate was highest (>50 %) on general wards where a fifth of NIV starts took place. Actual location depended on etiology of ARF as patients with ACLD and APE were started more often in EDs and “de novo” ARF in ICU. NIV failure and mortality rates were higher in ICUs related to the greater proportion of patients with “de novo” ARF.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Noninvasive mechanical ventilation (NIV) has been increasingly used worldwide for acute respiratory failure (ARF), mainly in patients with chronic obstructive pulmonary disease (COPD) and acute pulmonary edema (APE) [1–12]. Location of NIV treatment is an important predictor of NIV success which is associated with favorable outcomes of ARF [4, 10, 13]. The patient’s severity of illness, need for monitoring and capabilities of the location to provide monitoring and skilled, experienced staff are important in deciding on the location of NIV application [13–18].
In our prior survey done between 2002 and 2003 in Massachusetts and Rhode Island; over half of the NIV starts took place in intensive care units (ICU), approximately a quarter in emergency departments (ED) and one fifth in general hospital wards [19]. Given the current focus on optimal use of resources, there has been increasing pressure to treat NIV patients outside of the ICU [20–27]. However, few studies have examined locations and associated outcomes of NIV application in acute care hospitals.
Therefore, we conducted an observational cohort study with on-site data collection at selected hospitals that participated in our previous survey [18] to determine rates for utilization, success, and mortality for NIV management as well as patient characteristics and outcomes in different hospital locations and the flow of patients between different locations.
Methods
Study Design and Patient Population
Eight of 76 medical centers from our prior survey [19] were selected as described previously [11]. The Institutional Review Boards of participating institutions approved the study (Tufts ID #7642) and waived the need for patient consent. The database was accrued for a block design study testing the impact of an educational intervention on NIV use and its outcomes for patients with ARF (The results of the impact of educational intervention will be reported separately). Characteristics of the hospitals randomized either to control or educational intervention groups are shown in Table 1.
Participants were enrolled prospectively at each institution during sequential 3-month periods: 1-at baseline (Pre) between January 1, 2004 and August 3, 2007, and 2-after the intervention or control periods (Post) between August 25, 2005 and December 26, 2009. Given that there were no significant time-related differences, the pre and post periods were combined to increase the number of enrollees.
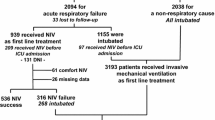
All patients in whom NIV (continuous positive airway pressure (CPAP) or pressure support ventilation and positive end expiratory pressure) or invasive mechanical ventilation (INV) was initiated at any time throughout their hospitalization were screened. To maximize the number of patients for this analysis, patients in the interventional and control and pre- and post-surveys were combined. Although NIV utilization rates increased from 31 to 41 % of all ventilator starts in each unit in test centers after the educational intervention (with no significant difference in control centers), it was significant only in ICUs (from 26 to 42 % of all ventilator starts in ICU) (p < 0.05). Screened patients were enrolled into the study if they required ventilator support for ARF. Patients were excluded if they were 1-intubated for surgery/procedures or prior to admission, 2-chronic NIV users without any acute deterioration, 3-younger than 18 years old, 4-tracheostomized, or 5-recorded with insufficient data (Fig. 1).

Flow chart of patients, including consort diagram showing locations of initiation and initial transfer and success rates of patients placed on NIV for ARF (Continued ventilator management was assessed within 72 h of NIV initiation. NIV success rate written in each box belongs to patients mentioned in that box.). ARF acute respiratory failure, ED emergency department, ICU intensive care unit, INV invasive mechanical ventilation, NIV noninvasive mechanical ventilation, pts patients, SR success rate, UR utilization rate. (1) Twenty-seven of the enrolled patients were admitted to ‘other’ wards and NIV was initiated in 14 of them (UR = 52 %). (2) Includes 3 patients (1 intubated) transferred to other acute care hospitals
Data Collection
Respiratory therapists from each hospital prospectively enrolled patients and at the time of enrollment completed standardized data as previously described [11]. The main indications for ventilatory support were classified into 6 groups [11]: (1) acute-on-chronic lung disease (ACLD) (i.e., COPD and other chronic lung diseases); (2) “de novo” ARF (i.e., pneumonia, ARDS); (3) APE; (4) ARF associated with neurologic diseases; (5) cardiopulmonary arrest, and (6) others (post-extubation failure, immune-suppressed with ARF, sepsis, shock and other diseases).
Outcome Variables
Patients were placed into four groups based on the location of NIV initiation: ED, ICU, general wards, and other (including step-down units). The primary outcome was the utilization rate of NIV as a percentage of all ventilator starts to treat ARF in each unit. Rates of NIV success (avoidance of ETI or death during use of NIV or the subsequent 48 h) [11] and in-hospital mortality per unit were secondary outcomes. Other secondary outcomes included patient characteristics, etiology of ARF, vital signs, gas exchange parameters, duration of mechanical ventilation use, and length of stay in hospital.
Statistical Analysis
Statistical analysis was performed using SPSS statistical analysis software, version 12.0 (SPSS Inc, Chicago, IL, USA). Continuous variables were expressed as median with interquartile range (IQR) and compared using Mann–Whitney U test or Kruskal–Wallis tests. The chi-square test (with Monte Carlo method) was used for categorical data when appropriate. A two-tailed p value <0.05 was considered statistically significant.
Results
Location of NIV Initiation and Continuation
Of 2310 screened cases initiated on mechanical ventilation at our 8 hospitals, 1085 cases were excluded and 1225 ventilator starts in 1208 patients were enrolled into our study. NIV was used as a first-line modality in 499 (41 %) of all ventilator starts. Most patients were initiated in the ED or ICU, in almost equal numbers (Fig. 1). In both locations, most patients were placed on INV whereas on the wards/step-down units, most patients were placed on NIV initially. Among those begun on NIV, initial disposition depended on the location of initiation as shown in Fig. 1. Twenty four patients [mainly with APE (8 patients), ACLD (7) and pneumonia (6)] were managed solely in the ED, with a success rate of 88 %.
Of all 1225 ventilator starts, 27 were initiated in other units (Table 2). Considering that this group was so small and comprised 7 different units, it was excluded from further analysis.
Patient Characteristics at Baseline
NIV patients were older, heavier, and more apt to have a DNI/DNR status than INV patients (Table 3). Additionally, they were less tachycardic, more tachypneic, and had higher blood pressures. They were also less severely ill than INV patients, with lower SAPS II scores and higher pHs and PaCO2s. Among NIV patients initiated in different units; patients on wards had higher BMIs than patients in EDs or ICUs, and vital signs and arterial blood gas findings were significantly different between units with the most severe acidosis and hypercapnia in EDs.
Utilization rates of NIV differed for etiologies of ARF between units; being highest for all etiologies in general wards (p < 0.05) (Table 3). Patients with ACLD, APE, or a DNR or DNI status were begun on NIV most commonly in ED’s; whereas patients with ‘de novo’ ARF were most often begun in ICUs (p < 0.05, except for those with a DNI status). NIV utilization rates for the various units were significantly different between participating hospitals, as well (Fig. 2).

Distribution of NIV utilization rates for all ventilator starts in each unit among participating hospitals (Numbers given on the bars are the absolute number of NIV patients.). Abbreviations as per Fig. 1. Also C community, T teaching. p < 0.05 for NIV utilization rates in each unit among participating hospitals
Characteristics of NIV Patients Transferred Between Units
Patients transferred to the ICU from either the ED or wards were more tachypneic, acidotic, and hypercapnic and had higher SAPS II scores than patients who remained in those units, associated with a higher rate of NIV failure (Table 4). Compared to those transferred to wards, patients transferred to ICUs were younger, less often had a DNI status, and had lower success rates and longer hospital stays.
NIV Failure and Mortality Rates and Other Outcomes
NIV success rates were better among patients begun on NIV in the ED and on the wards than in the ICU (p < 0.05) (Table 5). Mortality and lengths of stay were greater for NIV starts in the ICU than in the ED, related to the lower prevalence of ACLD/CPE diagnoses in ICU (p < 0.05) (Table 3). As would be expected, mortality rates were lower for NIV than INV in all units. Success and mortality rates of 96 NIV patients with a DNI order were not significantly different between units.
Initial IPAP, EPAP, and CPAP settings were 12.5 ± 2.5, 5.5 ± 1.2, and 9.2 ± 2.4 cm H2O, respectively, and were similar between units (data not shown; p > 0.05). Complications such as pneumonia, pneumothorax, and vomiting into the mask were similarly infrequent among the units; whereas patients were intolerant of NIV more often when initiated in wards (17 %) and less often in EDs (7 %) (p < 0.05). Sedation/analgesia (especially morphine and lorazepam) was used in 91 patients (19 %), with similar rates in units (20, 15, and 25 % of NIV patients in ICU, ED and wards, respectively). Propofol and fentanyl were used only in the ICU; whereas benzodiazepines, morphine, and other opioids were used in all units.
Discussion
In this study, we found that most patients with ARF were started on NIV in closely monitored settings, including the ICU and ED; whereas roughly one fifth of NIV starts occurred on general wards. On the other hand, the highest rate of NIV use as a percentage of all ventilator starts was on general wards, followed by other units (including step-down units), ICU’s and ED’s. The location for NIV start was associated with causal diagnosis of ARF, with starts for ACLD and APE occurring more often in EDs and “de novo” ARF in ICUs. We also observed that most NIV patients were transferred to other locations soon after initiation, except for those started in the ICU. NIV failure and in-hospital mortality rates were significantly different between units, being higher in ICU patients, explained by differing diagnoses.
Evidence of benefits of NIV for selected patients with ARF has accrued over the past couple of decades, not only for patients treated in ICUs, but also outside of the ICU [6, 12, 21–24, 28–30]. Although ICUs provide an appropriate, safe environment for NIV use, bed availability is limited and cost is much higher [14]. Moreover, hospital staff, both inside and outside of the ICU, is gaining skill and knowledge with the implementation of NIV as they gain more experience, rendering out-of-ICU NIV use safer.
We found that although only a fifth of our NIV patients were started on general wards, NIV utilization rate was highest for general wards (73 %), reflecting the higher rates of ACLD and DNI status there compared to other units. These patients were not as acutely ill as those started in the ED, as indicated by their lower heart and respiratory rates and less hypercapnia, and NIV success rate for patients managed on general wards was quite favorable, in the 80–90 % range. These results are consistent with current guidelines that recommend use of NIV in EDs and ICUs, as well as on general wards, as long as patients are appropriately selected and managed by medical staff with adequate training [2, 3].
In our prior survey done between 2002 and 2003 in the same region [19], 55 % of NIV starts were in the ICU, 26 % in the ED and 18 % on general wards, similar to another Massachusetts study from a single teaching hospital that reported in 2001 that 47 % of NIV starts occurred in the ICU as opposed to 33 % on general wards and 20 % in the ED [25]. The higher percentage of NIV starts in the ED (36 %) in our current study may reflect increasing use of NIV in EDs prior to ICU or ward admission. Paus-Jenssen et al. reported from a single Canadian tertiary care institution that 32 % of NIV starts occurred in the ED, 27 % in the ICU, 23 % in a ward observation unit and 18 % on general wards [31]. Sinuff et al. reported even higher rates for NIV starts in the ED (62 %) from another Canadian Teaching Hospital [32]. These variations may reflect different times of data collection as well as differences between individual institutions as detected in the current study (Fig. 2). Such differences are very challenging to explain given the many uncontrolled confounding variables, such as differences in patient populations, knowledge and skill levels, resource and staffing levels, and availability of intermediate care units, to name just a few.
Factors that were associated with the site of NIV initiation in our study included the causal diagnosis of ARF. NIV was started most commonly in the ED for patients with ACLD, APE, or DNI/DNR status and in the ICU for cases with ‘de novo’ ARF, consistent with other studies [28, 33]. Patients in our study who started NIV in the ED were more tachypneic, tachycardic, acidotic, and hypercarbic than those started in other units. Considering that delay in NIV initiation can lead to increased mortality [34, 35], initiation of NIV of these sicker patients in EDs rather than awaiting transfer elsewhere, is almost certainly beneficial.
Our study also tracked transfers of patients within 72 h of initiating NIV. Most patients starting in the ED were transferred to the ICU, whereas the majority of patients starting in the ICU or on the wards or other units remained where they started. Thirteen per cent of NIV patients starting in the ED remained there, a few due to death but most due to sufficient recovery to discontinue NIV. In total, 72 % of all patients started on NIV ended up being treated in the ICU. Likewise, several single-center studies from North America have found that most patients starting NIV in the ED are transferred to higher acuity units [25, 31, 32]. However, the percent of patients begun outside, and then transferred to the ICU varies considerably between studies, from one tenth in Italy to 56 % in Australia [20, 24]. One Italian study found that only 10 % of NIV patients begun on wards required transfer to the ICU [23]. However, it is important to emphasize that this low transfer rate was achieved using a specially organized medical emergency team [36] that is not available in most institutions. In our study, ICU transfers were more tachypneic, acidotic, and hypercapnic with higher SAPSII scores and less often had a DNI status than ward transfers, thus having a higher perceived need for intensive monitoring.
In our study as in others [6, 25, 28], location of NIV initiation was related to NIV success and in-hospital mortality. NIV success rate was lowest in the ICU (60 %), undoubtedly reflecting the more common diagnosis of “de novo” ARF as opposed to the more common diagnoses of ACLD and APE encountered among patients started in the ED or on general wards where success rates were 77 and 68 %, respectively.
NIV is frequently offered for management of ARF in patients with a DNI order as the ceiling of ventilator care or palliative therapy [37–39]. Thus, as expected, the rate of DNI status was higher in our NIV patients treated in the ED or on general wards than in the ICU. The in-hospital mortality rate of DNI patients managed with NIV in our study was much lower than reported in recent studies [37, 40], perhaps related to a higher rate of ACLD and APE and lower severity scores in our patients.
Limitations of our study include its observational design, precluding conclusions about the efficacy of care in different units. Additionally, although the total number of patients enrolled is greater than most previous epidemiologic studies, we are still limited by small numbers when comparing sub-groups of patients. Also, considering that this is a regional study, the results may not be generalizable to other regions in the US, or to other countries. This is particularly true for use of intermediate care or step-down units, which were present in only 3 of our 8 institutions and were used infrequently for NIV so that we excluded these for purposes of analysis. Our study also has strengths, including our prospective data collection with efforts to detect every NIV application during a particular time period and our use of multiple hospitals, both community and teaching, to obtain a “real world” glimpse of NIV use.
In conclusion, we found that patients with ARF started NIV mainly in the ED and ICU, with about one fifth starting on general wards; however, the utilization rate was highest for the wards. Once started on NIV, most patients in the ED were transferred to the ICU and most started in the ICU or on general wards remained there. NIV was started proportionately more often in EDs and less often in ICUs than in our earlier survey, perhaps related to a greater awareness of NIV in EDs. Success rates were higher and mortality rates were lower among patients started on NIV in the ED and on wards, probably reflecting the greater prevalence of diagnoses favoring use of NIV, such as ACLD and APE, compared to ICU patients, but also supporting the idea that NIV is being applied appropriately for most patients in these settings. These findings suggest that NIV is being applied in multiple different locations in acute care hospitals with specific location determined by patient and hospital characteristics.
Abbreviations
- ACLD:
-
Acute-on-chronic lung disease
- APE:
-
Acute pulmonary edema
- ARF:
-
Acute respiratory failure
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive pulmonary disease
- CPAP:
-
Continuous positive airway pressure
- ED:
-
Emergency department
- EPAP:
-
Expiratory positive airway pressure
- ETI:
-
Endotracheal intubation
- ICU:
-
Intensive care unit
- INV:
-
Invasive mechanical ventilation
- IPAP:
-
Inspiratory positive airway pressure
- LOS:
-
Length of stay
- MV:
-
Mechanical ventilation
- NIV:
-
Noninvasive mechanical ventilation
References
Keenan SP, Sinuff T, Burns KE et al (2011) Clinical practice guidelines for the use of noninvasive positive-pressure ventilation and noninvasive continuous positive airway pressure in the acute care setting. CMAJ 183:E195–214
American Thoracic Society (2001) European Respiratory Society, European Society of Intensive Care Medicine, Societe de Reanimation de Langue Francaise. International consensus conferences in intensive care medicine: noninvasive positive pressure ventilation in acute respiratory failure. Am J Respir Crit Care Med 163:283–291
British Thoracic Society Standards of Care Committee (2002) Non-invasive ventilation in acute respiratory failure. Thorax 57:192–211
Walkey AJ, Wiener RS (2013) Use of noninvasive ventilation in patients with acute respiratory failure, 2000–2009: a population-based study. Ann Am Thorac Soc 10:10–17
Stefan MS, Shieh MS, Pekow PS et al (2013) Epidemiology and outcomes of acute respiratory failure in the United States, 2001 to 2009: a national survey. J Hosp Med 8:76–82
Demoule A, Girou E, Richard JC et al (2006) Increased use of noninvasive ventilation in French intensive care units. Intensive Care Med 32:1747–1755
Esteban A, Ferguson ND, Meade MO et al (2008) Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med 177:170–177
Nava S (2013) Behind a mask: tricks, pitfalls, and prejudices for noninvasive ventilation. Respir Care 58:1367–1376
Hess DR (2013) Noninvasive ventilation for acute respiratory failure. Respir Care 58:950–972
Chandra D, Stamm JA, Taylor B et al (2011) Outcomes of noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease in the United States, 1998–2008. Am J Respir Crit Care Med 185:152–159
Ugurlu AO, Sidhom SS, Khodabandeh A et al (2014) Use and outcomes of noninvasive positive pressure ventilation in acute care hospitals in Massachusetts. Chest 145:964–971
Schnell D, Timsit JF, Darmon M et al (2014) Noninvasive mechanical ventilation in acute respiratory failure: trends in use and outcomes. Intensive Care Med 40:582–591
Ambrosino N (2012) Should we perform noninvasive ventilation anywhere? Expert Rev Respir Med 6:131–133
Hill NS (2009) Where should noninvasive ventilation be delivered? Respir Care 54:62–70
Elliott MW, Confalonieri M, Nava S (2002) Where to perform noninvasive ventilation? Eur Respir J 19:1159–1166
Lorencio C, Sirvent JM (2012) Noninvasive ventilation: when, how and where? Med Intensiva 36:601–603
Demoule A (2009) Non-invasive ventilation: how far away from the ICU? Intensive Care Med 35:192–194
Kacmarek RM, Villar J (2012) Acute application of noninvasive ventilation outside the ICU: when is it safe? Respir Care 57:815–816
Maheshwari V, Paioli D, Rothaar R et al (2006) Utilization of noninvasive ventilation in acute care hospitals: a regional survey. Chest 129:1226–1233
Cabrini L, Antonelli M, Savoia G et al (2011) Non-invasive ventilation outside of the intensive care unit: an Italian survey. Minerva Anestesiol 77:313–322
Plant PK, Owen JL, Elliott MW (2000) Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trial. Lancet 355:1931–1935
Farha S, Ghamra ZW, Hoisington ER et al (2006) Use of noninvasive positive-pressure ventilation on the regular hospital ward: experience and correlates of success. Respir Care 51:1237–1243
Cabrini L, Idone C, Colombo S et al (2009) Medical emergency team and non-invasive ventilation outside ICU for acute respiratory failure. Intensive Care Med 35:339–343
Schneider AG, Calzavacca P, Mercer I et al (2011) The epidemiology and outcome of medical emergency team call patients treated with non-invasive ventilation. Resuscitation 82:1218–1223
Schettino G, Altobelli N, Kacmarek RM (2008) Noninvasive positive-pressure ventilation in acute respiratory failure outside clinical trials: experience at the Massachusetts General Hospital. Crit Care Med 36:441–447
Harris C, Saskin R, Burns KE (2010) Noninvasive ventilation initiation in clinical practice: a six-year prospective, observational study. Can Respir J 17:123–131
Hess DR, Pang JM, Camargo CA Jr (2009) A survey of the use of noninvasive ventilation in academic emergency departments in the United States. Respir Care 54:1306–1312
Wang S, Singh B, Tian L et al (2013) Epidemiology of noninvasive mechanical ventilation in acute respiratory failure—a retrospective population-based study. BMC Emerg Med 13:6
Scala R, Corrado A, Confalonieri M et al (2011) Increased number and expertise of italian respiratory high-dependency care units: the second national survey. Respir Care 56:1100–1107
Tomii K, Seo R, Tachikawa R et al (2009) Impact of noninvasive ventilation (NIV) trial for various types of acute respiratory failure in the emergency department; decreased mortality and use of the ICU. Respir Med 103:67–73
Paus-Jenssen ES, Reid JK, Cockcroft DW et al (2004) The use of noninvasive ventilation in acute respiratory failure at a tertiary care center. Chest 126:165–172
Sinuff T, Cook D, Randall J et al (2000) Noninvasive positive-pressure ventilation: a utilization review of use in a teaching hospital. CMAJ 163:969–973
Browning J, Atwood B, Gray A (2006) Use of non-invasive ventilation in UK emergency departments. Emerg Med J 23:920–921
Conti G, Antonelli M, Navalesi P et al (2002) Noninvasive vs. conventional mechanical ventilation in patients with chronic obstructive pulmonary disease after failure of medical treatment in the ward: a randomized trial. Intensive Care Med 28:1701–1707
Roberts CM, Stone RA, Buckingham RJ et al (2010) Acidosis, non-invasive ventilation and mortality in hospitalised COPD exacerbations. Thorax 66:43–48
Winck JC, Goncalves MR (2011) Noninvasive ventilation: on the road to organization or towards the Tower of Babel? Minerva Anestesiol 77:263–265
Nava S, Ferrer M, Esquinas A et al (2013) Palliative use of non-invasive ventilation in end-of-life patients with solid tumours: a randomised feasibility trial. Lancet Oncol 14:219–227
Azoulay E, Kouatchet A, Jaber S et al (2012) Noninvasive mechanical ventilation in patients having declined tracheal intubation. Intensive Care Med 39:292–301
Azoulay E, Demoule A, Jaber S et al (2011) Palliative noninvasive ventilation in patients with acute respiratory failure. Intensive Care Med 37:1250–1257
Azoulay E, Kouatchet A, Jaber S et al (2013) Noninvasive mechanical ventilation in patients having declined tracheal intubation. Intensive Care Med 39:292–301
Acknowledgments
Dr. Hill received support from the Eli Lilly Distinguished Scholar Award of the Chest Foundation of the American College of Chest Physicians. The study also received support from a generous gift from Respironics, Inc. Dr. Ozsancak Ugurlu received research Grant from The Scientific and Technological Research Council of Turkey (TUBITAK). The authors would also like to thank the Respiratory Therapy Departments and therapists of the following hospitals: Boston Medical Center, Boston, MA, Cape Cod Hospital, Hyannis MA, Jordan Hospital, Plymouth MA, Lowell General Hospital, Lowell MA, Morton Hospital, Taunton MA, Saints Memorial Medical Center, Lowell MA, Tufts Medical Center, Boston MA, Winchester Hospital, Winchester MA.
Author Contribution
Drs. Ozsancak Ugurlu, Sidhom, Khodabandeh and Hill all participated in study design, data acquisition and analysis and preparation of the manuscript. Drs. Ozsancak Ugurlu, Sidhom, and Hill are guarantors of the entire manuscript. Dr. Maheshwari participated in study design, data acquisition, and preparation of the manuscript. Drs. Ieong, Mohr, Lin, Buchwald, Bahhady, and Wengryn participated in data acquisition and preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Hill received Research Grants from Respironics, Inc and Breathe Technologies. No other authors report any conflicts of interest.
Additional information
Clinical Trial Registration: Tufts Medical Center, Clinicaltrials.gov #NCT00458926.
Rights and permissions
About this article

Cite this article
Ozsancak Ugurlu, A., Sidhom, S.S., Khodabandeh, A. et al. Where is Noninvasive Ventilation Actually Delivered for Acute Respiratory Failure?. Lung 193, 779–788 (2015). https://doi.org/10.1007/s00408-015-9766-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-015-9766-y