
Abstract
Introduction
While most people believe the nasal septum to have intrinsic deviation and overgrowth in patients seeking rhinoplasty, an alternative concept is that a mal-oriented premaxilla causes extrinsic septal buckling and external extrusion of the septal cartilage. In this sense, the premaxillary bone plays a significant role in the pathogenesis of septal deviation. This study was performed to determine if non-traumatically acquired septal/nasal functional and aesthetic pathology or septal deviation may be related to the orientation of the premaxilla relative to the skullbase.
Methods
A retrospective, single-center study of patients in the general population who underwent maxillofacial CT scans and presented for the evaluation of nasal obstruction. CT scans were used to measure features of both pathologic and non-pathologic nasal septums.
Results
A total of 68 subjects were evaluated. When comparing patients with a premaxillary-skullbase angle of greater than 81° (the mean of the study group) to those of less than 81°, and a more obtuse nasolabial angle was observed (p = 0.0269). When comparing the extremes of premaxillary rotation, specifically, greater than 87° (mean 91.7°, SD 5.1) and less than 77° (mean 70.7°, SD 3.6), the differences were more pronounced with regard to caudal septal excess (p = 0.0451) and septal deviation in the axial plane (p = 0.0150).
Conclusion
Septal developmental changes may involve an overly rotated or more vertically oriented premaxillary bone relative to the skull base. An understanding of the cause of septal deformity may provide insight into the design of improved treatments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Deviation of the midline nasal septum may contribute to both aesthetic deformity of the nose and nasal obstruction. The prevalence of septal deviation varies widely in the literature, but has been reported to be as high as 90% and is known to occur in both the pediatric and adult populations [1]. The etiology of septal deviation is poorly understood; however, it may result from a variety of causes, including mechanical injuries, nasal polyps, neoplasia, infections, genetic influences, congenital malformations, and impingement by growth of the facial and cranial bones [2, 3]. Most surgeons have inferred that septal deviation is intrinsic to the cartilage, and thus, surgical techniques such as cartilage scoring and submucous resection have been developed and are commonly used to overcome this intrinsic deviation.
Recent reports, however, suggest the possibility that the septum is not intrinsically overgrown and deviated, but instead is compressed internally by a petite bony aperture and extruded externally [4]. The internal compression results in a buckling, commonly referred to as deviation, and the external extrusion results in dorsal and caudal fullness that creates a classic nasal deformity. The extreme form of this deformity is referred to as a “tension nose” [5], defined by Johnson et al. as “a high nasal dorsum and overprojected and inferiorly displaced nasal tip cartilages with accompanying nasolabial angle blunting with apparent shortening of the upper lip.” In reality, almost all septal deviations and dorsal humps requiring rhinoplasty exist within this spectrum. While Johnson et al. assumed that the septal cartilage was overgrown, several studies have demonstrated that the septum surface area remains conserved amongst individuals, and is just over-sized relative to its bony aperture [4]. Furthermore, while some authors have attempted to classify types of septal deviation, these classification systems just represent different patterns and degrees of buckling [6] .
Septal deviation is known to be associated with disorders of the nasal floor and palate, as well as the angle of the cranial base [6, 7]. During development, the septum forms as a down-growth of the fused medial nasal process and nasofrontal process, ultimately fusing with the nasal floor and premaxilla to divide the nose into two distinct cavities [8]. This downward growth in the direction of the premaxilla, the embryologic unit of bone situated anterior to the incisive foramen of the hard palate and which contains all four upper incisors, the nasal spine, and maxillary crest), works well in the setting of a normally positioned premaxillary bone [1]. However, we believe that, if the premaxilla is not in ideal position, the growing septum may run out of adequate room to expand, resulting in a buckling (deviation) and extrusion (dorsal and caudal fullness). In line with this thinking, authors have described an overly-angulated premaxilla relative to the skull base as a “cranial pincer” [9].
Premaxillary positioning and angulation can be measured by comparing its position relative to the skullbase. We hypothesize that the orientation of the premaxilla relative to the skullbase in normal versus pathologic noses would show substantial differences in degree of deviation and extrusion due to this influence of premaxillary orientation on septal development. Using sagittal, axial, and coronal CT scans in both pathologic and normal patients, we tested this hypothesis by comparing degree of septal deviation, presence of the tension nose deformity with angle of the premaxilla relative to the skullbase. To evaluate this, maxillofacial CT scans of the general population were analyzed and angulation of the premaxilla was assessed in relation to the presence of nasal septal deformity.
Methods
The study was approved by the Institutional Review Board of the Albert Einstein College of Medicine at Jacobi Medical Center in Bronx, NY. A total of 68 patients underwent maxillofacial CT scans and were retrospectively reviewed. These were sequential facial CT scans identified from the general database of our hospital, and were not selected based on pathology, or lack of pathology.
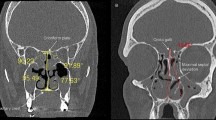
Scan were identified in a query that was 6 weeks from the date of review. The scans were originally ordered for a variety of different reasons, including evaluation of sinusitis and in the setting of non-nasal trauma. Exclusion criteria included history of significant facial trauma, congenital craniofacial anomalies, neoplasm, nasal bone fracture, and previous septal surgery. CT scans were used to measure features of both pathologic and non-pathologic septums. These included nasolabial angle, nasofrontal angle, caudal septal excess below the nasal spine, septal deviation in the coronal plane, presence or absence of a dorsal hump, septal deviation in the axial plane, lip length, and anterior displacement of the nasal base were measured from coronal and midline sagittal CT scans using the measuring tool in Agfa Healthcare N.V (Mortsel, Belgium) PACS software. This software automatically calibrates CT measurements with actual size at the time of CT scan, requiring no additional measurement calibration between subjects. Of note, the angle of the premaxilla was measured by the intersection of the line from the sella to the nasion to estimate the angle of the skull base and the line drawn from the orientation of the maxillary central incisor (Fig. 1). The mean and median of the study population were identified. Using the median angle of the premaxilla in our study group (81°) as a cutoff, patients were separated into two groups, and their radiographic septal features were compared using an unpaired t test.

Angle of the premaxilla. The angle of the premaxilla is the intersection of the line from the sella to the nasion with the line drawn from the orientation of the maxillary central incisor. The premaxilla is outlined in red, containing the maxillary crest, nasal spine and incisors, and in this pathologic example, is rotated anteriorly
Results
A total of 68 patients with maxillofacial CT scans were evaluated. Demographic information and results are listed in Table 1. The mean premaxillary-skull base angle was determined to be 81°. When comparing patients with a premaxillary-skull base angle greater than 81° to those less than 81°, a more obtuse nasolabial angle was observed. This difference was statistically significant. Differences in the remaining parameters evaluated did not reach statistical significance. When comparing the extremes of premaxillary rotation, specifically those greater than 87° (mean 91.7°, SD 5.1) and less than 77° (mean 70.7°, SD 3.6), differences were more pronounced with regard to caudal septal excess and septal deviation in the axial plane and were statistically significant (Table 2). Patients who demonstrated less steep premaxillary orientations 3 relative to the skull base were found to have more acute nasolabial angles, decreased septal deviation in an axial plane, and similar nasofrontal angles, presence of a dorsal hump, anterior displacement of the nasal base and lip lengths when compared to patients with greater angles of premaxillary orientation.
Discussion
Previously, it has been shown that septal deformity may be due to an inadequate bony septal aperture that essentially squeezes the septal quadrangular cartilage, causing it to buckle and extrude externally, dorsally, and caudally into the external nose [4]. This may explain why external nasal deformity and septal deviation commonly occur together. Importantly, this study shows, specifically, that this reduced bony septal aperture may be due to a malrotation of the premaxillary bone relative to the cranial base. This finding is consistent with that of the previous studies that have shown an association of septal deviation with certain cranial base angles [7, 9]. In cases of severe septal deviation not due to trauma, the premaxillary bone is rotated in a way that the incisors are rotated inward (retroclination), the nasal spine is rotated anteroinferiorly, and the maxillary crest is rotated antero-superiorly. These rotations result in three clinical manifestations: (1) the maxillary crest interferes with the downward growth of the septum and causes it to buckle; (2) the nasal spine downwardly rotates and causes the nose to appear long, contributing to a caudal deformity and fullness (‘tension nose deformity’) [5]; and (3) retroclination of the incisors causes the nose to look overly large and the teeth to appear long relative to the lip (Figs. 2, 3).

Sagittal schematic of the premaxilla and septum. a Normal anatomy with normal positioning of the quandrangular cartilage and premaxilla. b Rotated premaxilla (yellow counterclockwise arrow is direction) causing overlap of the septum with the bony components. This results in deviation at overlap locations (***) and external extrusion of the septum, causing the typical tension nose deformity

Septal deviation in the coronal view and axial views. Non-contrast CT maxillofacial shows a C-shaped septum with deviation in the coronal as well as axial views
Our findings suggest that septal pathology may be the result of skeletal changes causing septal buckling and extrusion rather than inherent cartilaginous pathology. In contrast to the article by Johnson et al. describing the tension nose deformity, we have shown that this version of extreme septal problems is actually due to a flaw of rotation of the premaxilla relative to the skull base. This has several important implications. First, while there is currently no well-accepted method to adjust the premaxilla relative to the skull base, techniques ranging from more efficient septal surgery to orthodontia should be considered to try and achieve enhanced results. Surgical techniques such as partial excision of the nasal spine or maxillary crest or reduction of the caudal L-strut to permit the septum to exist unencumbered in the midline may be effective in this regard (Fig. 4). Our findings also belabor the importance of a comprehensive examination for all patients presenting with functional or aesthetic nasal complaints, including assessment of the position of the incisors. A retroclined incisor position may motivate referral for orthodontic evaluation when present. Finally, early diagnosis of a tension deformity during childhood or adolescence may prompt early intervention and use of orthodontic-like devices similar to those that used for palate expansion and mandibular distraction, thus potentially mitigating the need for future nasal surgery in a certain population of patients.

Patient with classic ‘tension nose’ deformity and septal deviation before and after septal resizing and respositioning septorhinoplasty. a Base view. b Right lateral view. c Frontal view
There are several limitations of this study. The fact that our results did not demonstrate statistically significant differences in parameters such lip shortening, anterior displacement of the nasal base and presence of a dorsal hump may be explained by the relatively small sample size, as well as the fact that only relatively small differences exist between angulation of the premaxilla in patients. Furthermore, the ‘shortening’ of the upper lip typically associated with the tension deformity is not true soft tissue deficiency, but rather a perceived shortening due to nasolabial angle blunting and caudle septal excess and extrusion.
Conclusion
An excessively small bony nasal aperture may result from a more vertically oriented premaxillary bone relative to the skull base and may contribute to septal deviation and the tension nose deformity. Proper diagnosis of this deformity and use of appropriately surgical techniques are necessary to maximize both aesthetic and functional outcomes.
References
Reitzen SD, Chung W, Shah AR (2011) Nasal septal deviation in the pediatric and adult populations. Ear Nose Throat J 90(3):112–115
Takahashi R (1988) The evolution of the nasal septum and the formation of septal deformity. Rhinol Suppl 6:1–23
Kim YM, Rha KS, Weissman JD, Hwang PH, Most SP (2011) Correlation of asymmetric facial growth with deviated nasal septum. Laryngoscope 121(6):1144–1148
Weinstock MS, Stupak HD (2018) Bony/cartilaginous mismatch: a radiologic investigation into the cause of tension nose deformity. Plast Reconstr Surg 141(2):312–321
Johnson CM Jr, Godin MS (1995) The tension nose: open structure rhinoplasty approach. Plast Reconstr Surg 95(1):43–51
Mladina R (1987) The role of maxillar morphology in the development of pathological septal deformities. Rhinology 25(3):199–205
Mladina R, Krajina Z (1990) The influence of palato-cranial base (basomaxillary) angle on the length of the caudal process of the nasal septum in man. Rhinology 28(3):185–189
Sykes JM, Kim JE, Shaye D, Boccieri A (2011) The importance of the nasal septum in the deviated nose. Facial Plast Surg 27(5):413–421
Mladina R, Cujic E, Subaric M, Vukovic K (2008) Nasal septal deformities in ear, nose, and throat patients: an international study. Am J Otolaryngol 29(2):75–82
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no potential conflicts of interest.
Ethical standards
This study was IRB-approved by Jacobi Medical Center/Albert Einstein College of Medicine.
Human/animal rights
Human subjects were involved in this study; however, all data were accumulated and analyzed in a retrospective nature, and therefore, informed consent was not necessary
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hyman, A.J., Fastenberg, J.H. & Stupak, H.D. Orientation of the premaxilla in the origin of septal deviation. Eur Arch Otorhinolaryngol 276, 3147–3151 (2019). https://doi.org/10.1007/s00405-019-05618-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-019-05618-y