
Abstract
Objectives
Lip and palate deformities are an important craniofacial congenital anomaly that negatively affects the anatomy of the nasal cavity and maxilla. This study aimed to evaluate the nasal septum deviation in individuals with a unilateral cleft lip and palate.
Methods
The sample consists of 22 unilateral cleft lip–palate patients and 20 controls with non-cleft skeletal Class III. Maximal septal deviation angle and linear dimension were measured on cone-beam computed tomography images. The localization of maximal septal deviation was determined. The data were analyzed and compared between unilateral cleft lip–palate patients and skeletal Class III individuals.
Results
For septal deviation, a significant discrepancy between unilateral cleft patients and skeletal Class III subjects was detected at the anterior nasal spine (ANS) level, the posterior nasal spine (PNS) level and the ANS–PNS midpoint level (p < 0.05). The maximum septal deviation angle of individuals with a unilateral cleft was significantly greater than individuals with skeletal Class III (p < 0.05). No statistically significant differences were found in the localization of maximum septal deviation between the unilateral cleft patients and the Class III individuals.
Conclusion
Our results demonstrated that the maximum septal deviation angle and dimension had significant differences in individuals with a unilateral cleft, compared to a skeletal Class III control group. However, no statistically significant discrepancy was observed between three levels (ANS, PNS and ANS–PNS middle levels) in the unilateral cleft patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cleft lip and palate (CLP) is a common deformity of the craniofacial region. CLP occurs as a result of an inadequate fusion of the embryological extensions of the face during fetal life. Environmental and genetic factors play a role in its etiology [1]. CLP patients have not only oronasal insufficiency, but also experience nasal problems [2]. Mouth-breathing, paranasal sinus problems, snoring, and obstructive sleep apnea have also been reported [3, 4].
The nasal bone growth and facial morphology may be affected by nasal septal changes. Previous studies have reported that the prevalence of nasal septal deviation was up to 80% in healthy individuals [5]. The nasal septum is a significant structure in the growth of premaxilla [6]. Nasal septum deformity and deviation usually occur in patients with CLP. The nasal septum in the unilateral CLP patients often shows convexity toward the cleft side, and the deviation direction is toward the cleft defect [3]. Although nasal obstruction has various etiological factors, such as mucosal congestion, choanal stenosis/atresia, adenoid hypertrophy and others, a deviated nasal septum is one of the common causes of nasal obstruction [7,8,9,10]. This obstruction can lead to significant functional and cosmetic effects such as malocclusions and abnormal facial appearance [11, 12]. One of the common findings in individuals with CLP is skeletal Class III malocclusion [2].
The nasal airway and deformity were evaluated with morphometric measurements using lateral cephalometric image and computed tomography (CT) [13, 14]. Cone-beam computed tomography (CBCT) is commonly used in dental and medical imaging. CBCT technology allows three-dimensional assessment of the craniofacial region with higher resolutions, isotropic voxel values and a lower radiation dose, compared to CT [15]. In addition, the overlapping anatomical points, common enlargement errors and image distortion in cephalometric images are not present in CBCT images [11].
Previous studies have examined the nasal septum anatomy in CLP patients via CBCT [3, 15, 16]. In these studies, unilateral CLP patients were compared with a healthy or general control group, and these individuals not evaluated in terms of skeletal inter-maxillary relationships. CLP individuals often have a skeletal Class III inter-maxillary relationship [2, 17]. Therefore, it would be more suitable to compare CLP patients with skeletal Class III subjects [2]. To the best of our knowledge, no studies assessed the nasal septal deviation between CLP patients and individuals with non-cleft Class III malocclusion. Therefore, the present study aimed to investigate the three-dimensional morphology of nasal septum deviation in unilateral CLP patients, compared to non-cleft Class III individuals.
Methods
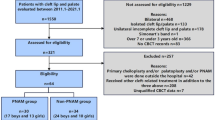
Ethical approval of this study was obtained from Gazi University Ethics Committee (No: 2018-406). Twenty-two patients with unilateral CLP who underwent CBCT scanning at the Dentomaxillofacial Radiology Department of the Gazi University between 2012 and 2018 were examined retrospectively. The criteria for cleft patients included were as follows: individuals at least 14 years old, non-syndromic individuals and unilateral CLP patients. The control group was selected from angle skeletal Class III individuals (ANB > 4°). Lateral cephalometric images were obtained from the CBCT scans and ANB angle was measured on these images (researcher: IE). The skeletal Class III individuals were selected from patients without CLP who underwent CBCT for various reasons. The CBCT images were excluded if there was presence of movement artefacts, previous history of surgery or trauma and images not clearly showing the nasal region.
The images were acquired with a Planmeca Promax 3D unit (Helsinki, Finland), radiation dose: 90 KVp, 8 mA; imaging parameter: 0.4 mm with voxel size, and field of view: 20 × 10 cm. Evaluations were made using the Romexis Viewer 4.6.2.R software. The images were examined by one experienced oral radiologist (GA). To assess the intra-observer agreement, 20% of the measurements were repeated by the same observer after 3 weeks.
The distance between the anterior nasal spine (ANS) and the posterior nasal spine (PNS) on the mid-sagittal section was measured (length of the hard palate). Measurements for nasal septal deviation were made in three levels (ANS level, PNS level, ANS–PNS middle level). The septal deviation was measured as the longest distance drawn from the midline to the deviated segment of the nasal septum on the coronal section (Fig. 1). The midline was described as a line drawn from the maxillary or palatal spine to the crista galli [5, 16].

Linear measurements on CBCT images; a distance between ANS and PNS (length of the hard palate) on the mid-sagittal section, b the septal deviation was measured as the longest distance drawn from the midline to the deviated segment of the nasal septum on the coronal section (red line)
The nasal septal deviation angle was measured on coronal CBCT images as the angle between the midline and the line drawn from the crista galli to the maximum deviation point of the septum (Fig. 2). The three-dimensional position of maximal septal deviation was also determined according to the axial plane, inferior or superior (according to the midline of the skull base and the nasal floor); according to the sagittal plane, right or left of midline; according to the coronal plane, posterior or anterior (according to midline of ANS and PNS). The maximal septal deviation was localized by the turbinate: middle turbinate, inferior turbinate or between the inferior and middle turbinate.

The nasal septal deviation angle was measured on coronal CBCT images as the angle between the midline and the line drawn from the crista galli to the maximum deviation point of the septum
Statistical analysis
In this study, depending on the distributional violations, nonparametric statistical analysis was used. For testing the normality assumption, Kolmogorov–Smirnov test was performed. The comparisons were evaluated using Friedman and Mann–Whitney U tests. For analysis of the categorical variables, Fisher’s exact test and Chi-square test were used. The intra-observer consistency was assessed using intra-class correlation coefficient (ICC). The data obtained were analyzed using the SPSS version 23.0 (Armonk, New York). p < 0.05 was taken as statistically significant.
Results
Twenty-two patients with unilateral CLP, 11 females and 11 males, had a mean age of 20.77 ± 6.56 years, ranging from 14 to 35 years. In the non-cleft Class III control group (n = 20), 11 females and 9 males had a mean age of 24.45 ± 6.04 years, ranging from 15 to 35 years.
The difference between unilateral cleft patients and control groups regarding septal deviation, ANS–PNS distance (length of the hard palate) and maximum septal deviation angle was analyzed by the Mann–Whitney U test (Table 1). For septal deviation, statistically significant differences between unilateral CLP patients and subjects with Class III malocclusion were detected in the ANS level (p = 0.001), in the PNS level (p = 0.000), and in the ANS–PNS middle level (p = 0.013). The comparison of ANS, PNS and ANS–PNS middle levels in the unilateral cleft patients and in the control group was evaluated by a nonparametric Friedman test. For septal deviation in the unilateral cleft patients, the difference between three levels was considered null (p = 0.554). On the other hand, for the Class III control group, the septal deviation was found to be higher in the ANS–PNS middle level, compared to the ANS and PNS levels (p = 0.009). The distance between ANS and PNS (length of the hard palate) was found to be higher in non-cleft Class III individuals (p = 0.000). There was a significant difference in the maximum septal deviation angle (p = 0.039); the patients with unilateral CLP have a higher mean than the Class III control group.
The effect of gender was also analyzed by the Mann–Whitney U test for patients with unilateral CLP and the Class III control group separately (Table 2). The effect of gender was found to be insignificant in all measurements (p > 0.05).
The localization of maximum septal deviation between the unilateral cleft patients and the Class III control group was compared. Statistically significant differences were not found in the localization of maximum septal deviation between the unilateral cleft group and the Class III control group (p > 0.05). The comparison between unilateral CLP patients and control group is summarized in Table 3.
The intra-observer reliability was assessed by using ICC and the values ranged between 0.844 and 0.992.
Discussion
Severe septum deviation leads to the development of a mouth-breathing habit together with inadequate nasal airway formation [13]. This condition is one of the causes of the exacerbation of malocclusion in CLP patients [3]. Studies have shown a strong correlation between nasal septum deviation and asymmetric facial growth [18]. Multiple departments (orthodontic, otolaryngology and surgery) plan treatment of patients with CLP. Therefore, the evaluation of nasal asymmetry is important in the multidiscipline treatment of the CLP individuals to achieve a better result, both functionally and esthetically [3]. To our knowledge, no study has evaluated the nasal septal anatomy differences between patients with unilateral CLP and non-cleft, skeletal Class III individuals. Our results demonstrated that there are significant differences regarding septal deviation between patients with unilateral CLP and non-cleft, skeletal Class III individuals. These findings were confirmed with the study of Massie et al. [15], who reported that septal deviation was significantly worse in CLP patients than the control group.
Previous studies have shown that the posterior part of the nasal septum deviates more from the anterior part in unilateral, complete, cleft lip–palate patients [14]. Massie et al. [15] reported that septal deviation was significantly more deviated at the ANS–PNS midpoint levels than at the ANS level. Friel et al. [16] observed that the nasal septum posterior to the ANS–PNS midpoint comprises 96% bone in unilateral CLP patients. In their study, the septal deviation dimension was measured in the anteroposterior midpoint of the hard palate (mean value 5.7 mm) [16]. In the present study, the septal deviation dimensions of ANS, PNS and ANS–PNS middle levels in the unilateral CLP patients were compared. The dimension of nasal septal deviations was observed to be higher at the ANS–PNS middle level (mean value 7.11 mm). However, no significant differences in the septal deviation between the three levels (ANS, PNS and ANS–PNS middle levels) in the unilateral CLP were found. The discrepancy between studies may be due to different cleft types or different age distribution. In the study of Massie et al. [15], the mean age of the patients (for unilateral and bilateral CLP patients) was 21 years (15–33 years). Friel et al. [16] examined younger, unilateral CLP individuals (mean age for CLP 10.8 years). In another study, the mean age was 16 years [3]. Nasal bone growth is thought to be completed in girls between the ages of 11–12 and between 13–14 years of age in boys [15, 19]. The images of unilateral CLP in individuals who were 14 years old and older were examined in this study.
In the literature, a significant asymmetry in the midfacial area in patients with unilateral CLP has been reported, and asymmetry is limited to the cleft, nasal and nasal septum regions. Other studies have reported that asymmetry includes deeper midfacial structures [20]. In the study of Massie et al. [15], the septal deviation of individuals with CLP was significantly worse in all anatomical planes than the control group. They found a maximal septal deviation of the posterior half of the nasal airways in more than 68% of patients with CLP [15]. Dedeoglu et al. [21] found that the incidence of anterior nasal septal deviation in the unilateral cleft patients was significantly higher than that in the control group. Jiang et al. [3] demonstrated that the posterior part in the unilateral CLP patients had a greater deviation than the anterior part. According to the results of this study, a statistically significant discrepancy was not observed in the localization, including anterior or posterior, between unilateral CLP patients and the skeletal Class III control group.
Jiang et al. [3] demonstrated that the maximal septal deviation often happened at the inferior turbinate level for cleft patients. In the present study, localization of maximal septal deviation was observed almost equally at the inferior turbinate, middle turbinate and inter-turbinate levels, and no statistically significant difference was determined. Our results showed that significant differences were not detected in the localization of maximum septal deviation between unilateral CLP individuals and the Class III control group.
A significant relationship was found between the severity of the cleft and the grade of the septum deviation in cleft individuals [3, 14]. Septal deviation angle was a commonly used parameter to evaluate the septal deviation [3]. In the present study, septal deviation angle was calculated and our results showed that the patients with unilateral CLP had significantly higher deviation than the skeletal Class III control group. This result was consistent with those of Jiang et al. [3] and Massie et al. [15].
The association between maxilla and nasal septum is significant due to morphological and functional interaction [22]. In this study, we evaluated the distance between ANS and PNS (length of the hard palate). Our results showed that the hard palate length was significantly higher in Class III individuals than in patients with unilateral CLP. To our knowledge, no studies have evaluated the hard palate length in CLP patients via CBCT.
In the literature, the gender effect on septal deviation has been evaluated in cleft subjects. Jiang et al. [3] reported that the septal deviation angle between genders showed significant differences in a cleft group. Contrary to the study of Jiang et al. [3], in this study, the difference between females and males in the unilateral CLP patients was not found to be statistically significant in the maximum septal deviation angle.
The CBCT scan is a useful aid to the clinician in assessing complex craniofacial structures and dental relationships [16]. In recent years, CBCT images have been frequently used in the pre-operative evaluation before surgical and orthodontic treatments [23]. CBCT offers great advantages such as high resolution, low radiation dose and less observation of motion artifacts with a shorter scan time, compared to traditional CT [4].
The limitation of the current study includes a restricted sample size due to its retrospective design. The assessment of the nasal airway and septal deviation is of vital importance in patients with CLP when planning orthodontic and surgical treatment [11]. Further analyses with a larger sample size are necessary to examine the nasal septal morphology among various cleft types.
Conclusion
The results of this study showed that the septal deviation angle and dimension were statistically significant different in unilateral CLP patients, compared to a non-cleft, skeletal Class III control group. However, no statistically significant discrepancy was observed between three levels (ANS, PNS and ANS–PNS middle levels) in the unilateral CLP patients. The results obtained may be important in the pre-treatment and the treatment prognosis.
References
Vieira AR. Genetic and environmental factors in human cleft lip and palate. Front Oral Biol. 2012;16:19–31.
Ertaş Ü, Ataol M. Evaluation of nasal airway volume of operated unilateral cleft lip and palate patients compared with skeletal Class III individuals. Cleft Palate Craniofac J. 2019;56:15–20.
Jiang M, You M, Wang S, et al. Analysis of nasal septal deviation in cleft palate and/or alveolus patients using cone-beam computed tomography. Otolaryngol Head Neck Surg. 2014;151:226–31.
Karia H, Shrivastav S, Kariaa AK. Three-dimensional evaluation of the airway spaces in patients with and without cleft lip and palate: a digital volume tomographic study. J Orthod Dentofac Orthop. 2017;152:371–81.
Serifoglu I, Oz İİ, Damar M, Buyukuysal MC, Tosun A, Tokgöz Ö. Relationship between the degree and direction of nasal septum deviation and nasal bone morphology. Head Face Med. 2017;28(13):3.
Delaire J, Precious D. Influence of the nasal septum on maxillonasal growth in patients with congenital labiomaxillary cleft. Cleft Palate J. 1986;23:270–7.
Fettman N, Sanford T, Sindwani R. Surgical management of the deviated septum: techniques in septoplasty. Otolaryngol Clin N Am. 2009;42(2):241–viii.
Gandomi B, Bayat A, Kazemei T. Outcomes of septoplasty in young adults: the nasal obstruction septoplasty effectiveness study. Am J Otolaryngol. 2010;31(3):189–92.
Hsu DW, Suh JD. Anatomy and physiology of nasal obstruction. Otolaryngol Clin N Am. 2018;51:853–65.
Veloso NC, Mordente CM, de Sousa AA, et al. Three-dimensional nasal septum and maxillary changes following rapid maxillary expansion in patients with cleft lip and palate: a case-series analysis. Angle Orthod. 2020. https://doi.org/10.2319/090719-583.1.
Farzal Z, Walsh J, Lopes de RezendeBarbosa G, et al. Volumetric nasal cavity analysis in children with unilateral and bilateral cleft lip and palate. Laryngoscope. 2016;126:1475–80.
Pimenta LA, de Rezende Barbosa GL, Pretti H, et al. Three-dimensional evaluation of nasopharyngeal airways of unilateral cleft lip and palate patients. Laryngoscope. 2015;125:736–9.
D’Ascanio L, Lancione C, Pompa G, et al. Craniofacial growth in children with nasal septum deviation: a cephalometric comparative study. Int J Pediatr Otorhinolaryngol. 2010;74:1180–3.
Nagasao T, Miyamoto J, Yasuda S, et al. An anatomical study of the three-dimensional structure of the nasal septum in patients with alveolar clefts and alveolar-palatal clefts. Plast Reconstr Surg. 2008;121:2074–83.
Massie JP, Runyan CM, Stern MJ, et al. Nasal septal anatomy in skeletally mature patients with cleft lip and palate. JAMA Facial Plast Surg. 2016;18:347–53.
Friel MT, Starbuck JM, Ghoneima AM, et al. Airway obstruction and the unilateral cleft lip and palate deformity: contributions by the bony septum. Ann Plast Surg. 2015;75:37–43.
Lin Y, Fu Z, Ma L, Li W. Cone-beam computed tomography-synthesized cephalometric study of operated unilateral cleft lip and palate and non-cleft children with Class III skeletal relationship. Am J Orthod Dentofac Orthop. 2016;150(802):810.
Kim YM, Rha KS, Weissman JD, Hwang PH. Most SP Correlation of asymmetric facial growth with deviated nasal septum. Laryngoscope. 2011;121:1144–8.
Akgüner M, Barutçu A, Karaca C. Adolescent growth patterns of the bony and cartilaginous framework of the nose: a cephalometric study. Ann Plast Surg. 1998;41:66–9.
Suri S, Utreja A, Khandelwal N, et al. Craniofacial computerized tomography analysis of the midface of patients with repaired complete unilateral cleft lip and palate. Am J Orthod Dentofac Orthop. 2008;134:418–29.
Dedeoglu N, Altun O, Kucuk EB, et al. Evaluation of the anatomical variation in the nasal cavity and paranasal sinuses of patients with cleft lip and palate using cone beam computed tomography. Bratisl Med J. 2016;117:691–6.
Emi K, Shintaro K, Kazutaka K. Morphological characteristics of nasomaxillary complex and cranial base in maxillary retrognathism. Int J Oral Med Sci. 2019;18:27–35.
Wörtche R, Hassfeld S, Lux CJ, et al. Clinical application of cone beam digital volume tomography in children with cleft lip and palate. Dentomaxillofac Radiol. 2006;35:88–9.
Funding
There are no financial or other relations that could lead to a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human rights statement and informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Ethical approval
The study procedure was approved by the Gazi University Ethics Committee, Ankara (No: 2018-406).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Akay, G., Eren, İ., Karadag, Ö. et al. Nasal septal deviation in the unilateral cleft lip and palate deformities: a three-dimensional analysis. Oral Radiol 37, 567–572 (2021). https://doi.org/10.1007/s11282-020-00491-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-020-00491-6