
Abstract
Objectives
Even though many patients undergoing auditory steady-state response (ASSR) testing have some degree of hearing loss, some have normal hearing and ASSR often overestimates the behavioral thresholds in this group. In most commercial ASSR systems such as Chartr EP, a default correction factor is applied to compensate for this difference. Little is known, however, as how the correction factor compensates for the difference between ASSR and pure tone audiometry (PTA) thresholds as a function of carrier or modulation frequency (MF) in a commercial ASSR system. Our goal is to evaluate this relationship.
Methods
Twenty-four normal hearing adults were examined for both PTA and ASSR (Chartr EP system, GN Otometrics). ASSR thresholds were obtained at three MFs (20, 40, and 80 Hz). The difference scores were obtained by subtracting PTA from ASSR thresholds at each frequency for each subject. The corrected ASSR thresholds, then, were compared with the PTA thresholds across MFs and carrier frequencies.
Results
The default correction factors in the ASSR equipment differed significantly from the difference scores at all MFs and carrier frequencies (n = 24, p < 0.005). The correlation between corrected ASSR and PTA thresholds at most MFs and carrier frequencies were medium to poor.
Conclusions
At most MFs and carrier frequencies, the default correction factors defined by the manufacturer do not compensate for the difference between ASSR and PTA thresholds in normal hearing adults. The use of the default correction factors in Chartr EP system for the normal hearing adults needs special considerations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pure tone audiometry (PTA) has long been considered as the gold standard for hearing evaluation. However, in several types of patients with normal hearing including those with developmental/neurological disabilities, in pediatric groups, and among patients who have nonorganic hearing loss, valid PTA results are difficult to obtain [1]. Other objective tests of auditory function, such as auditory brainstem response (ABR) and otoacoustic emissions (OAEs), have been beneficial in identifying hearing thresholds for such patients [2, 3]. While these techniques offer useful alternatives to PTA, they also present limitations such as difficulty in obtaining frequency-specific information in ABR [4] and dealing with the complicated relationship between the type of hearing loss and OAEs [5]. These limitations led audiologists to consider another objective audiometry technique, the auditory steady-state responses (ASSRs) [6].
ASSR is evoked brain responses to continuous modulated pure tones with different carrier frequencies, usually octave frequencies of 500–4000 Hz [7]. Since ASSR is an objective test and can lead to frequency-specific hearing evaluation, it has been considered as a good alternative test for screening and diagnosis of hearing problems, especially in patients who are unable or unwilling to participate in subjective hearing evaluations [8]. Even though many patients undergoing ASSR testing have some degree of hearing loss, some have normal hearing. Thus, it is critical that those subjects are also correctly diagnosed.
Despite the broad use of ASSR, its relationship with PTA thresholds is complex. This is in part, due to several factors such as hearing thresholds, type and degree of hearing loss, the tested modulation frequencies (MFs) and carrier frequencies that affect the relationship between ASSR and PTA [8, 9]. For example, a study by Ozdek et al. [10] shows that correlation between hearing thresholds obtained using ASSR and PTA in normal hearing adults is weaker than subjects with sensory-neural hearing loss (SNHL) [10]. Meanwhile, ASSR has been found to be a more accurate prediction of hearing thresholds in SNHL group compared to normal hearing adults [11, 12]. This has even been supported by more recent studies using other types of stimuli such as E-chirps [13, 14], where despite improvement in prediction of hearing thresholds using these stimuli, still ASSR is a less accurate predictor of hearing thresholds in normal hearing subjects.
To compensate for the difference between ASSR and PTA in commercial systems, a correction factorFootnote 1 is often proposed based on carrier frequencies by the manufacturer. Surprisingly, despite the possible effect of MF on the obtained ASSR thresholds, these correction factors are similarly defined for all MFs. On the other hand, several studies targeted relationship between ASSR and PTA [11, 12, 15, 16], but no studies were found to investigate this relationship based on MF in a commercial system. For example, a study by Petitot et al. [9] using a noncommercial system (Rotman MASTER Research system), suggest that 40 Hz is a better MF for estimating hearing thresholds [9]. However, it is not clear whether the results of that study could be generalized to commercial systems and clinical testing conditions as the recording algorithms are not similar.
As the ultimate purpose of research on such techniques is to improve their application for clinical applications, research on the accuracy of hearing evaluation using commercial ASSR systems will inform the research and industry community for improving the application of these systems for clinical purposes.
In the current study by obtaining binaural multiple ASSR thresholds at various carrier frequencies and MFs using a commercial ASSR system, we investigated the relationship between ASSR and PTA thresholds. After measuring PTA and ASSR thresholds at four octave frequencies and three MFs, the recommended correction factors by the ASSR acquisition system were compared with the obtained difference between ASSR and PTA at each MF and carrier frequency.
Methods
Ethical considerations
The study was approved by the local ethics committee (Ethic no: BP-QP-110–01) at Tehran University of Medical Sciences and informed consent was obtained from each subject.
Subjects
Twenty-four normal hearing adults (15 females and 9 males, 25–40 years old) with hearing thresholds at or better than 20 dBHL at 6 octave frequencies: 250, 500, 1000, 2000, 4000, and 8000 Hz participated in this study. Participants with abnormal findings in otoscopy (e.g., tympanic membrane perforation, middle ear effusion), abnormal middle ear measurements or acoustic reflexesFootnote 2 were excluded from the study. PTA thresholds were obtained using TDH39 earphone with AC40 system (Interacoustics, Denmark). All tests were performed in an acoustic sound-proof booth. Both electrophysiological ASSR and PTA thresholds were measured using Hughson–Westlake method (10 down, 5 up) [17].
ASSR
Air-conducted stimuli were introduced into each ear through an ER-3A insert earphone (Etymotic Research). Stimuli were generated and presented by the Chartr EP system (version 5.3, GN Otometrics) and presented to right and left ear simultaneously. All the stimuli were 100% amplitude modulated (AM) and 20% frequency modulated as well. Response confidence was set to 95%. The response confidence is a measure of signal to noise ratio and the chance of finding a response. When a good signal-to-noise ratio by the response confidence bar ≥ 95% was obtained, the test was extended so that the threshold could be obtained. The response confidence in this system is based on an algorithm of magnitude-squared coherence (MSC) to detect the probability of response presence relative to surrounding noise [18]. Four carrier frequencies: 500, 1000, 2000, and 4000 Hz were tested using multiple ASSR technique. As a result, at each MF, four carrier frequencies were tested simultaneously in both ears. For testing ASSRs at different MFs, the following modulation rates are predefined by the manufacturer as the set-up for performing daily ASSR test: modulation rates for the 40 Hz MF stimuli in multiple ASSR are 39, 43, 47, and 51 Hz for 500, 1000, 2000, and 4000 Hz carrier frequencies in the right ear and 41, 45, 49, and 53 Hz for the left ear, respectively. For 80 Hz MF stimuli, modulation rates are 84, 88, 92, and 96 Hz for the right and 86, 90, 94, and 98 Hz for the left ear, respectively. Finally, for the same carrier frequencies, modulation rates for 20 Hz MF are 24, 31, 33, and 26 Hz for the right and 29, 27, 30, and 23 Hz for the left ear. Modulation rates for the 20 Hz MF ASSR were chosen based upon previous work [19] indicating that the modulation rates for different carrier frequencies may be separated by as little as 4 Hz without affecting the response. The range of tested intensities was between 10- and 80-dB HL.
During each session, subjects relaxed in a supine position on a comfortable bed. Participants were asked to sleep or relax during 80 Hz multiple ASSR testing. As 20 and 40 Hz ASSR responses are more related to thalamus and cortical auditory areas in the brain, they are affected by sleep [20]. Thus, during 40 and 20 Hz multiple ASSR, participants were not allowed to sleep.
Responses were recorded via three scalp electrodes: the active electrode was placed on the upper forehead and the ground electrode on the lower forehead. The reference electrode was placed on the nape. The impedance of the electrodes was periodically checked during recordings to maintain low impedance and good connection (less than 3 KΩ). To minimize any artifacts and noise due to head and body movements, participants were asked to stay still during recording.
All statistical analysis were performed using IBM SPSS Statistics version 24. Multiple comparisons were adjusted using Bonferroni correction. All graphs were prepared using Microsoft Excel 2016.
Results
Estimation of thresholds
The mean PTA and ASSR thresholds for 24 normal hearing participants are summarized in Table 1. ASSR thresholds were obtained at MFs of 20, 40, and 80 Hz. The PTA thresholds were corrected to dB sound pressure level (SPL) based on ANSI S3.6-1996 standard. The majority of ASSR thresholds at all MFs ranged between 30- and 60-dB SPL. Among all MFs, 40 Hz resulted in the least variability in the obtained thresholds across all carrier frequencies (n = 24 subjects; SD40Hz = 5.88–9.77, SD80Hz = 4.64–10.41, SD20Hz = 8.83–13.98). Further, compared to 20 Hz and 80 Hz MFs, 40 Hz MF yielded better (lower) thresholds at 500 and 1000 Hz carrier frequencies (40 Hz MF: n = 24; M500Hz = 36.67 dB; SD = 7.02; M1000Hz = 34.6 dB; SD = 7.02; 20 Hz MF: n = 24; M500Hz = 47.92 dB; SD = 11.02; M1000Hz = 42.5 dB; SD = 10.73; 80 Hz MF: n = 24; M500Hz = 40.83 dB; SD = 6.5; M1000Hz = 38.75 dB; SD = 7.4). However, when comparing thresholds across all MFs at 2000 Hz and 4000 Hz, better thresholds were observed at 80 Hz MF. At all times, the average thresholds at 20 Hz were worse (i.e., higher) than the other two MFs (see Table 1).
To determine how well the default correction factors in ASSR system compensate for the differences between ASSR and PTA thresholds, we first subtracted PTA from ASSR thresholds to obtain difference scores [16]. The average difference scores based on ear, carrier frequencies, and MFs are shown in Table 2. Based on our data, at all carrier frequencies, the largest difference scores are measured at 20 Hz MF. Figure 1 depicts the averaged right and left ear difference scores based on carrier frequencies and MFs in an audiogram. The largest difference scores and standard deviations at 20 Hz MF are noticeable here. At 40 Hz, the difference score is more consistent across all carrier frequencies (see Table 2 for detailed statistics). The smallest difference between ASSR and PTA thresholds was observed in left ear at 80 Hz MF for 2000 and 4000 Hz (M2000Hz = 20.58 dB, SD2000Hz = 6.06; M4000Hz = 20.17 dB, SD4000Hz = 6.54), whereas 40HZ ASSR resulted in the smallest difference scores in the right ear at 500 and 1000 Hz (M500Hz = 22.12 dB, SD500Hz = 6.39; M1000Hz = 23.21 dB, SD1000Hz = 5.61).

The average pure tone audiometry (PTA) and auditory steady-state response (ASSR) thresholds for a 20 Hz, b 40 Hz, and c 80 Hz modulation frequencies (MFs) measured at 500, 1000, 2000, and 4000 Hz. Error bars represent standard deviations for each represented threshold. The tested MF is shown in a box at up right corner of the figure. The average PTA thresholds are replotted in each audiogram and is similar for all the panels (n = 24 subjects)
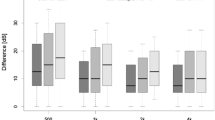
To examine how well the default correction factors by ASSR system compensate for the difference between ASSR and PTA thresholds, we applied the correction factors to the obtained ASSR thresholds and then, used paired t test to compare the corrected ASSR thresholds with PTA thresholds for each subject. This test showed a significant difference for all comparisons across all MFs for both right and left ear (n = 24, for all comparisons p < 0.0005, for the detailed statistics see Table 3). Figure 2 shows the boxplots for PTA and corrected ASSR thresholds based on MF for each ear. As it is shown in Fig. 2, at 40 Hz, an overlap between the distribution of the interquartile range (the distribution between the first and third quartile) of corrected ASSR and PTA thresholds at 500 Hz is noticeable. This is the only frequency where the difference between corrected ASSR and PTA thresholds is not significant (t(23) = 1.63, p = 0.117). At no other carrier frequencies and MFs, this overlap exists. The median of the distribution of thresholds between corrected ASSR and PTA thresholds do not match (Fig. 2). This suggests that the distribution of the corrected ASSR thresholds based on the default correction factors only minimally overlaps with the distribution of behavioral thresholds in the two ears.

Boxplots representing the distribution of the thresholds for pure tone audiometry (PTA) and corrected auditory steady-state response (ASSR) thresholds for 500, 1000, 2000, and 4000 Hz. The tested modulation frequency (MF) is represented in the box at the top right corner of each figure. The tested ear is shown at the top of the panel. Corrected ASSR thresholds were obtained by applying default correction factors to ASSR thresholds. Each single boxplot represents the distribution of the thresholds between first and third quartile, whiskers represent minimum and maximum of the data, and outliers are shown as a dot at the bottom or top of each boxplot (n = 24 subjects, for all comparisons p < 0.005)
Correlation coefficient
A Pearson product-moment correlation coefficient was computed to assess the relationship between PTA and corrected ASSR thresholds for all subjects. The scatterplots for these correlations and the average trendlines for each carrier frequencies and MFs are shown in Fig. 3. At 40 Hz MF positive correlation was found between ASSR and PTA at most frequencies in the right ear (r = 0.41, 0.40, and 0.52 for 500 HZ, 1000 Hz, and 4000 Hz, respectively; see Table 4 for the detailed statistics). The strongest correlation between ASSR and PTA thresholds was seen at 20HZ (r = 0.59 and 0.65, for 500 Hz and 1000 Hz, respectively, for both comparisons p > 0.05). The correlation between ASSR and PTA thresholds was stronger for right ear vs left ear. However, there was no significant difference between ASSR and PTA thresholds in right vs left ear (for all comparisons n = 24, p > 0.05). At all MFs and among all carrier frequencies, 1000 Hz showed better correlations between PTA and corrected ASSR thresholds (r = 0.4–0.59, n = 24, p < 0.05) (see Table 4 for the detailed statistics).

Scatterplots representing the relationship between pure tone audiometry (PTA) and corrected auditory steady-state response (ASSR) thresholds for four carrier frequencies (500, 1000, 2000, and 4000 Hz). The regression line for each plot is shown in the scatterplots (see Table 4 for the detailed statistics). The tested modulation frequency (MF) and ear are shown at the right side of each row. Corrected ASSR thresholds were obtained by applying default correction factors to ASSR thresholds (n = 24 subjects, for all comparisons p < 0.005)
Discussion
For the first time, the current study investigated the efficacy of correction factors in ASSR to compensate for the difference between ASSR and PTA in a clinical setting using a commercial ASSR acquisition system in normal hearing adults. Even though many patients undergoing ASSR testing have some degree of hearing loss, some have normal hearing. Thus, it is critical that those subjects are also correctly diagnosed. We found that the corrected ASSR thresholds based on the default correction factors in recording equipment significantly differ from the measured PTA thresholds. As a result, the different scores between ASSR and PTA thresholds for normal hearing adults do not match the suggested correction factors by the ASSR acquisition system. The Pearson product correlation coefficient showed good correlation in some, but medium to poor in most frequencies between the thresholds obtained using PTA and ASSR. Overall, our findings suggest that the use of correction factors for compensating the difference between ASSR and PTA thresholds in normal hearing group needs special considerations.
The effect of modulation and carrier frequency
When examining the effect of MF on ASSR thresholds, we found that decreasing MF did not improve the obtained ASSR thresholds. The present study, as well as others [9, 19] suggest that 40 Hz MF results in lower (i.e., better) multiple ASSR thresholds in normal hearing adults. Further, due to less variability in the thresholds obtained using 40 Hz ASSR, this MF resulted in the “strongest” correlation coefficients across carrier frequencies. In terms of difference scores, ASSR thresholds and the difference scores varied with MFs and carrier frequencies. For example, at 80 Hz ASSR, the difference scores at higher frequencies (2000 and 4000 Hz) were better (i.e., smaller). Some researchers suggest that this observation is resulted from a high-frequency hearing loss [20]. However, the subjects in the current study, as well as others [19] have normal hearing at all frequencies. This interaction between MF and carrier frequency which has previously been reported in several other studies [21,22,23], is more noticeable with ipsilateral rather than contralateral stimulation [14]. The reason for such an interaction is not clear yet.
Predictability of hearing thresholds using ASSR
The measured difference scores in our study are higher than those reported in research ASSR instruments by others [9, 23]. This could be due to the experimental variables such as the analysis algorithm and the behavioral hearing thresholds which significantly contribute to variability in the reported ASSR thresholds [16]. A systematic study by Hatzopolous et al. [16] shows that the algorithm used for obtaining hearing thresholds from ASSR potentials could contribute to the estimated thresholds using each ASSR acquisition system. In that study ASSR thresholds of the same subjects were compared between two different analysis systems (Chartr EP and Audera). The results of that study suggest that Chartr EP results in higher (worse) thresholds for the same subjects compared to Audera [16].
On the other hand, in subjects with SNHL, ASSRs give a better estimate of behavioral hearing thresholds. Thus, the measured difference scores in these subjects are significantly smaller than in normal hearing group [6, 12]. The poorer temporal integration [20] and electrophysiological recruitment [12] in SNHL subjects contribute to this observation. Due to the better estimate of behavioral thresholds using ASSR in SNHL subjects, pooling ASSR data from normal hearing and subjects with hearing loss results in lower average difference scores and a better correlation between ASSR and PTA thresholds in various studies [15, 24]. Thus, such an interpretation can lead to error in generalizing findings to normal hearing groups. Further, combining the data from both SNHL and normal hearing group could result in underestimation of correction factors in the ASSR systems for normal hearing adults. The present study as well as others [9, 16] addressed this issue by only including normal hearing adults. In both studies and in the current work, ASSR thresholds overestimate hearing thresholds in normal hearing adults. The correlation between ASSR and behavioral data in the normal hearing group is often non-significant or poor [10, 25]. These results are somewhat supported by the present findings which show poor-to-medium correlation between ASSR and PTA in most MFs and carrier frequencies.
Another factor to consider when comparing our difference scores to others’ is the age range focus of the tested subjects. In many of those studies, ASSRs were tested in infants [26, 27] or children [28]. Studies show that ASSR technique results in significantly larger magnitude responses in children than in adults with the same hearing range [29]. As the shape and properties of the ear canal in children are different from adults, less intensity will generate larger dBSPL at the eardrum in younger ages and less dBSPL in adults [30]. Thus, the difference scores in the current study are not comparable with those reported in infants and children.
One of the main aims of our study was to evaluate the credibility of equipment's default correction factors in predicting ASSR and PTA thresholds difference. In the present study, for most of the MFs and carrier frequencies, the correction factors suggested by Chartr EP system did not match the measured difference scores. This mismatch is likely due to defining smaller and similar correction factors for all carrier frequencies for the equipment. As the difference between ASSR and PTA changes based on MFs and carrier frequencies, applying similar correction factors does not compensate for the difference between these two measurements. This results in a significant statistical difference between the corrected ASSR and behavioral thresholds which is demonstrated in the current study. Applying correction factors ubiquitously to all degrees of hearing loss and carrier frequencies can result in over amplification of hearing aids in some frequencies [31], while the amplification in other frequencies might be insufficient [20]. On the other hand, this might result in unnecessary hearing aid fitting in normal hearing subjects.
Some recent studies have reported improved accuracy of hearing thresholds obtained using E-chirps by ASSR acquisition systems. Despite this progress, lower carrier frequencies still show poorer thresholds in normal hearing groups [14, 26].
Conclusion
While the goal of research on ASSR is refining the application of this frequency-specific hearing assessment tool in audiology, the lack of research on commercial equipment is noticeable. Defining more specific correction factors based on the degree of hearing loss and the tested frequencies will result in better application of this system to patients in clinics. The change in difference scores for various MFs and carrier frequencies is an important factor to be considered in defining the correction factors in commercial ASSR acquisition systems. Further, similar correction factors could not be applied to ASSR thresholds in subjects with a wide range of age and hearing thresholds. Having specific correction factors based on each MF, carrier frequency, and tested ear will result in a more accurate prediction of hearing thresholds using this objective audiometry technique. Further, ASSR can be a beneficial technique for objective hearing assessment in infants, children, and adults with a wide range of hearing if the correction factors are specifically defined for those populations. This means that defining correction factors requires considering the testing criteria and a more comprehensive evaluation of larger populations without pooling the data from various hearing ranges, ages, and MFs. This could help in a better hearing aidfitting that is prescribed and programmed based on the reported ASSR thresholds and the patient’s needs.
Notes
Correction factors are measured based on the difference between ASSR and PTA thresholds in subjects with a wide age and hearing range.
Static compliance less than 0.3 or more than 1.6 cc and middle ear pressure less than -100 or more than + 50 dapa.
References
Dobie RA, Van Hemel S (2004) Testing adult hearing: conclusions and recommendations. In: Hearing loss: determining eligibility for social security benefits. National Academies Press, Washington
Sininger YS, Abdala C (1996) Hearing threshold as measured by auditory brain stem response in human neonates. Ear Hear 17:395–401
Hall JW, Rupp KA (1997) Auditory brainstem response: recent developments in recording and analysis. Adv Otorhinolaryngol 53:21–45
Stapells DR, Oates P (1997) Estimation of the pure-tone audiogram by the auditory brainstem response: a review. Audiol Neurootol 2:257–280
Wagner W, Plinkert PK (1999) The relationship between auditory threshold and evoked otoacoustic emissions. Eur arch otorhinolaryngol 256:177–188
Dimitrijevic A, John MS, Van Roon P et al (2002) Estimating the audiogram using multiple auditory steady-state responses. J Am Acad Audiol 13:205–224
Purcell DW, John SM, Schneider SM, Picton TW (2004) Human temporal auditory acuity as assessed by envelope following responses. J Acoust Soc Am 116:3581–3593
Picton TW, John MS, Dimitrijevic A, Purcell D (2003) Human auditory steady-state responses. Int J Audiol 42:177–219
Petitot C, Collett L, Durrant JD (2005) Auditory steady-state responses (ASSR): effects of modulation and carrier frequencies. Int J Audiol 44:567–573
Ozdek A, Karacay M et al (2010) Comparison of pure tone audiometry and auditory steady-state responses in subjects with normal hearing and hearing loss. Eur Arch Otorhinolaryngol 267:43–49
Herdman AT, Stapells DR (2003) Auditory steady-state response thresholds of adults with sensorineural hearing impairments. Int J Audiol 42:237–248
Picton TW, Dimitrijevic A, Perez-Abalo MC, Van Roon P (2005) Estimating audiometric thresholds using auditory steady-state responses. J Am Acad Audiol 16:140–156
Lee MY, Ahn SY et al (2016) Narrow band CE-Chirp auditory steady-state response is more reliable than the conventional ASSR in predicting the behavioral hearing threshold. Auris Nasus Larynx 43:259–268
Jalaei B, Shaabani M, Zakaria MN (2017) Mode of recording and modulation frequency effects of auditory steady state response thresholds. Braz J Otorhinolaryngol 83:10–15
Hatzopoulos S, Prosser S et al (2010) Threshold estimation in adult normal-and impaired-hearing subjects using auditory steady-state responses. Med Sci Monit 16:21–27
Hatzopoulos S, Petruccelli J et al (2012) Hearing threshold prediction with Auditory Steady State Responses and estimation of correction functions to compensate for differences with behavioral data, in adult subjects: Part 1: Audera and Chartr EP devices. Med Sci Monit 18:47–53
Carhart R, Jerger JF (1959) Preferred method for clinical determination of pure-tone thresholds. J speech hear disord 24(4):330–345
Cone-Wesson B, Dowell RC, Tomlin D, Rance G, Ming WJ (2002) The auditory steady-state response: comparisons with the auditory brainstem response. J Am Acad Audiol 13:173–187
John MS, Lins OG, Boucher BL, Picton TW (1998) Multiple auditory steady-state responses (MASTER): stimulus and recording parameters. Audiology 37:59–82
Van Maanen A, Stapells DR (2005) Comparison of multiple auditory steady-state responses (80 vs 40 Hz) and slow cortical potentials for threshold estimation in hearing-impaired adults. Int J Audiol 44:613–624
Savio G, Cardenas J, Perez Abalo M, Gonzalez A, Valdes J (2001) The low and high frequency auditory steady state responses mature at different rates. Audiol Neurotol 6:279–287
Ross B, Draganova R, Picton TW, Pantev C (2003) Frequency specificity of 40-Hz auditory steady-state responses. Hear Res 186:57–68
Picton TW, van Roon P, John MS (2009) Multiple auditory steady state responses (80–101 Hz): effects of ear, gender, handedness, intensity and modulation rate. Ear Hear 30:100–109
Herdman AT, Stapells DR (2001) Thresholds determined using the monotic and dichotic multiple auditory steady-state response technique in normal-hearing subjects. Scan Audiol 30:41–49
Komazec Z, Lemajić-Komazec S, Jović R, Nadj Č, Jovančević L, Savović S (2010) Comparison between auditory steady-state responses and pure-tone audiometry. Vojnosanit pregl 67:761–765
Sininger YS, Hunter LL, Hayes D, Roush PA, Uhler KM (2018) Evaluation of speed and accuracy of next-generation auditory steady state response and auditory brainstem response audiometry in children with normal hearing and hearing loss. Ear Hear 39:1207–1223
Aimoni C, Crema L et al (2018) Hearing threshold estimation by auditory steady state responses (ASSR) in children. Acta Otorhinolaryngol Ital 38:361–368
Rance G, Rickards F (2002) Prediction of hearing threshold in infants using auditory steady-state evoked potentials. J Am Acad Audiol 13:236–245
Tlumak AI, Durrant JD, Delgado RE, Boston JR (2012) Steady-state analysis of auditory evoked potentials over a wide range of stimulus repetition rates: Profile in children vs adults. Int J Audiol 51:480–490
Stapells DR (2011) Frequency-specific ABR and ASSR threshold assessment in young infants. In: Tharpe AM, Seewald R (eds) Comprehensive handbook of pediatric audiology, 1st edn. Plural Publishing, San Diego, pp 409–448
Scherf F, Brokx J, Wuyts FL, Van de Heyning PH (2006) The ASSR: clinical application in normal-hearing and hearing-impaired infants and adults, comparison with the click-evoked ABR and pure-tone audiometry. Int J Audiol 45:281–286
Acknowledgements
The authors would like to thank Kristin Yeager, Bruna Mussoi, Sara Newman, and Jeff Wenstrup for their helpful comments. The current work has been supported by Tehran University of Medical Sciences. Some of the results were presented at Association for Research in Otolaryngology conference on February 2014 in Baltimore, Maryland.
Author information
Authors and Affiliations
Contributions
ZG, SF conceived/designed study, analyzed data and wrote manuscript. ZG performed experiments.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ghasemahmad, Z., Farahani, S. Validity of correction factors applied to auditory steady-state responses (ASSRs) in normal hearing adults in chartr EP system. Eur Arch Otorhinolaryngol 276, 2171–2180 (2019). https://doi.org/10.1007/s00405-019-05451-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-019-05451-3