
Abstract
Purpose
Pelvic organ prolapse (POP) impairs quality of life (QoL) due to vaginal bulge symptoms and changes in bladder/bowel and sexual function. The effect of alloplastic meshes on QoL is still being discussed. The purpose of this study was to prospectively evaluate the effect of mesh implantation on QoL and sexual function over 1 year.
Methods
289 women with cystocele > stage I were included in this prospective multicenter study, with nine hospitals participating (ClinicalTrials.gov NCT01084889). Mesh exposures rates and pelvic floor-related QoL using the validated German version of the p-QoL questionnaire were evaluated as the primary endpoints. Based on a single-sided binominal test with α = 0.05 and a power of 0.80, a sample size of 225 for the mesh exposures was calculated. The mesh used was a 6-arm mesh with titanium coating (TILOOP® Total 6, sponsor pfm medical ag, Germany). Preoperative data were compared to 6 and 12 months postoperative data, using Wilcoxon test.
Results
The mean age of the patients was 67 years (min 43, max 87). All domains of QoL improved significantly compared after surgery: mean prolapse score dropped from 73.7 to 19.4 after 6 and 16.2 after 12 months (p < 0.001). Sexual function also improved significantly. The rate of dyspareunia was lower at follow-up.
Conclusions
In this prospective trial, a significant positive effect of mesh implantation on pelvic floor-related QoL was observed. These findings remained stable 1 year after surgery with further improvement. This trial adds further data to the ongoing discussion on the role and risk of meshes in POP surgery.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Quality of life (QoL) has become an increasingly important outcome measure in the treatment of various medical conditions during the past decades. Pelvic organ prolapse (POP) is a common condition and has high impact on QoL. Symptoms may be far-reaching such as prolapse symptoms, voiding difficulties or pelvic floor pain [1]. Furthermore, sexual dysfunction can be an accompanying symptom with subsequent worse POP-related quality of life [2].
In most cases, impairment of quality of life is the indication for surgical repair of the prolapse. Therefore, POP surgery should both restore anatomy and improve patients’ QoL. The launch of alloplastic vaginal meshes has contributed profoundly to pelvic floor surgery, but there are specific risks, especially mesh exposure [3]. Other risks, like pelvic floor pain or dyspareunia, are not specific for meshes as they may result from native tissue repair, too. After widespread use of meshes in POP surgery, these numbers dropped after two warnings from the US food and drug administration (FDA) in 2008 and 2011 [4]. On the other hand, the recent Cochrane review stated that the use of vaginal grafts reduces the risk of prolapse symptoms and recurrent anterior vaginal prolapse on examination when compared to native tissue repair [4].
The aim of this multicentre, prospective trial was to evaluate the effect of implantation of a titanium-coated mesh for POP repair on QoL and sexual function. Titanium-coated meshes are used in hernia repair. The hydrophylity of a titanium coating increases the biocompatibility and therefore decreases, e.g. inflammatory reactions [5]. QoL data were collected before surgery and both 6 and 12 months after surgery. We hypothesized that POP-related quality of life and sexual function would improve 6 months after surgery.
Materials and methods
Study design
The study was designed as a prospective multicenter observational trial (ClinicalTrials.gov NCT01084889). Nine urogynecologic centers in Germany participated. Positive votes were obtained from the appropriate ethical review committees for each investigating center. All patients with symptomatic cystocele > stage I (POP-Q classification) and age >18 were eligible for participation. Exclusion criteria were pregnancy, intolerance to the mesh implants under investigation, history of carcinoma in the last 12 months or of radiotherapy in the pelvic area, status post-mesh implantation, systemic steroid treatment or participation in another clinical investigation. Patients were allowed to withdraw the informed consent at any time.
Quality of life data
The trial had two primary endpoints: the effect of mesh implantation on patients’ quality of life after 6 months and furthermore mesh exposure rates after 12 months. In order to reliably evaluate QoL, the German translation of a validated questionnaire on pelvic floor function was used [6, 7]. Among other questions, it comprises nine domains: general health perceptions, prolapse impact, role limitations, physical limitations, social limitations, personal relationships, emotions, sleep/energy and severity measures. A higher total score represents a greater impairment of quality of life, while a low score indicates good quality of life (range 0–100) [6].
To evaluate the effect on sexual function, three questions from the p-QoL questionnaire were chosen:
-
Does your prolapse impair your sex life?
-
Does your prolapse impair the relationship with your partner?
-
Do you have a vaginal bulge which impedes sex?
Additionally, a large variety of clinical data were obtained before, including adverse events, further surgeries, estrogen therapy, etc. Furthermore, questions on pull pain and foreign body feeling were posted. The questionnaires were filled in by the patients before and after surgery as a paper version and then transferred into an electronic case report form (eCRF). The acquired data were validated 100 % by an external monitor in order to minimize input data error [8]. The trial was controlled on a regular basis by an independent external clinical event committee with evaluation of all adverse events. Patients were seen for follow-up checks at the treating hospital by the treating physician. These visits were scheduled for 6 and 12 months after surgery. In case patients were not available for follow-up checks (illness, etc.), we tried to evaluate adverse events by telephone interview or contacted the external physicians.
Surgery and alloplastic mesh
The mesh used is a commercially available titanium-coated polypropylene mesh with six arms (TiLOOP® Total 6; pfm medical ag, Germany). The thickness of the titanium coating is 30–50 nm, and the pores of the mesh are ≥1 mm. Insertion of the mesh is performed with tunnelers for the transobturator and ischiorectal passage. All patients received preoperative local estrogen therapy and a single-shot antibiotic prophylaxis intraoperatively. After colpotomy and preparation of the vesicovaginal fascia, the mesh was implanted according to the manufacturer’s advice. The anterior arms were fastened transobturatically, the middle arms through the posterior angle of the obturator foramen, and the posterior arms in the sacrospinous ligament. After tension-free implantation of the mesh, the colpotomy was closed using a continuous absorbable suture and a vaginal packing was placed for 24–48 h. In case of additional rectocele, repair of the posterior compartment was performed. When considered necessary by the surgeon, hysterectomy or implantation of a suburethral sling was allowed.
Statistical analysis
A mean erosion rate of 7.9 ± 5.4 % is evaluated from comparable studies. With this erosion rate and a delta of 5.4 %, based on a single-sided binomial test with an alpha of 0.05 and a power 0.80, a sample size of 225 was calculated. The Wilcoxon test was used for analyzing the difference in QoL and sexual function between pre- and postoperative values. The subgroup analysis between hysterectomy and uterus preserving surgery was performed with the Mann–Whitney U test. Throughout, two-sided p values <5 % were considered statistically significant. As a further tool to define the clinical relevance of the data, we used the minimal clinically important difference (MCID). This is a statistical model trying to define the smallest change in a treatment outcome that a patient would identify as being important [9]. IBM SPSS®, Version 22 was used for statistical calculations.
Results
Demographic data
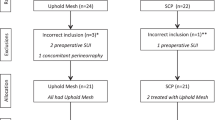
292 patients were eligible for participation, but three were excluded because they did not require surgery or mesh implantation. The remaining 289 patients underwent surgery between April 2010 and December 2012 in one of the participating centers. The demographic data in the trial were comparable to all patients undergoing surgery for POP in Germany in 2012 and are depicted in Table 1 [10]. The mean age of the patients at the time of surgery was 67 years (min. 43, max. 87). Follow-up checks were carried out at the treating hospital between October 2010 and May 2014. The median follow-up time of the first visit was 186 days, for the second 370 days. 280/289 (97 %) women were seen for the first follow-up check and 286/289 (99 %) for the second. The flowchart of participants is shown in Fig. 1.

Flowchart of participants
Preoperative pelvic organ prolapse quantification system (POP-Q) values were as follows: uterine/vaginal vault prolapse stage IV n = 9 (3.1 %), stage III n = 144 (49.8 %) and stage II n = 136 (47.1 %). Cystoceles were stage III n = 138 (47.8 %) and stage II n = 151 (52.2 %). The minority of patients had undergone previous hysterectomy or prolapse surgery (31.8 % and 14.9 %). Among those patients who had not had a hysterectomy before, it was performed in 53.3 %. 74 women (25.6 %) had additional mesh-augmented repair of the posterior compartment. For further intra- and postoperative data and POP-Q stages see Table 1.
Quality of life
Before surgery, patients had the worst scores regarding prolapse impact (73.7, min 0, max 100), and role limitations (58.5, min 0, max 100), but also physical limitations showed a mean score of 55.3. At the time of the 6 months’ visit, a significant improvement in quality of life could be observed. This was true for all nine domains of the questionnaire. For example, prolapse impact dropped from 73.7 to 19.4 (p < 0.001). This positive effect on quality of life remained stable at the 12-month follow-up check, with even further improvement from 6 to 12 months. Furthermore, the criteria of a minimal clinically important difference were met in all domains. The results of all domains are shown in Fig. 2. Among those patients who had not undergone hysterectomy before, there was no significant difference between patients with concomitant hysterectomy and those with uterus preserving surgery (data not shown).

Change of pelvic floor-related quality of life as measured with p-QoL
Sexual function
Regarding the impact of the prolapse on the relationship, we observed a significant reduction in patients answering “slightly”, “moderately” or “a lot” from 37.9 to 16.8 % after 6 months and further to 11.6 % after 12 months (p < 0.001). Impairment of sex life dropped accordingly from 48.6 to 20.2 % and further to 17.5 %, when looking at women answering “slightly”, “moderately” or “a lot” (p < 0.001). Furthermore, only a minority of women reported a vaginal bulge feeling after the operation (43.5 % preoperatively, 5.7 % at 6 months and 4.1 % at 12 months, p < 0.001). Of those patients who reported dyspareunia before the operation (n = 44/286, 15.4 %), seven patients still reported this problem after 12 months. At the same time point, the rate of de novo dyspareunia was 12/286 (4.2 %).
Impact on pull pain and foreign body feeling
The number of patients who reported pull pain or foreign body feeling dropped significantly after 6 months: 77.9–3.6 % (foreign body feeling) and 48.4–8.9 % (pull pain). This remained largely stable after 12 months (6 % foreign body feeling and 5.6 % pull pain, see Fig. 3).

Pre- and postoperative pull pain and foreign body feeling
Anatomical outcome and mesh exposure rates
Recurrent prolapse was defined as POP-Q > stage I. During a follow-up of 1 year, 2.1 % (6/286) of women had a recurrent cystocele, two of which needed surgery. In the posterior compartment, 39/286 patients (13.6 %) had a compensatory rectocele. In the same time, 30/286 (10.5 %) mesh exposures were detected. 56 % of the patients with an erosion were asymptomatic. In 13 cases the mesh exposure required surgery under anesthesia. No mesh had to be explanted.
Discussion
We performed a prospective, multicenter trial to evaluate the effect of mesh implantation for pelvic organ prolapse on patients’ quality of life, with special attention to sexual function. As with every surgery for POP, the implantation of alloplastic meshes entails risks such as recurrent prolapse, chronic pelvic pain or dyspareunia. However, the anatomical outcome seems to be superior compared to that of native tissue repair [3]. The discussion regarding the safety of alloplastic meshes is ongoing, especially after the FDA warnings in 2008 and 2011 [4]. Also the Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) of the European Commission recently stated that the clinical outcome following mesh implantation is influenced by material properties, product design, mesh size, route of implantation, patient characteristics, associated procedures and the surgeon’s experience. The report recommends that such aspects should be taken into account when choosing the kind of therapy [11]. For the evaluation of success after POP surgery, different outcome measures have been defined [12]. Besides the anatomic result, the subjective outcome should be the main goal of surgery. Due to POP, patients may have voiding difficulties, may refrain from sports or sexual intercourse, and chronic pelvic pain due to stretching of the ligaments is frequent. In most cases, impairment of QoL is the reason for patients to seek medical help and in some cases, to decide for surgical therapy. Therefore, implications on women’s quality of life should be explicitly evaluated when counseling women on the necessity of POP surgery.
The implantation of an alloplastic, titanium-coated mesh significantly improved the pelvic floor-related quality of life after 6 months. This effect continued after 12 months, showing even better results. We observed a significant improvement in all domains of the pelvic floor-specific questionnaire. Regarding dyspareunia after the implantation of suburethral slings for stress incontinence, there is inconsistent data [13, 14]. In line with this, the risk of dyspareunia is present in any pelvic floor surgery, but special concern is raised in mesh-augmented POP repair [15]. In this trial, we explicitly looked at women´s sexual function and observed a significant improvement. Dyspareunia was not increased after the surgery, and problems during sexual intercourse decreased. The rate of de novo dyspareunia was low, in line with other recent reports [16]. Rates of mesh exposures and recurrences were comparable to other published data [3]. We could not show a lower mesh exposure rate due to the titanium coating. However, there was no direct comparison between the titanium-coated mesh and other polypropylene meshes.
Recently, the question on the necessity of hysterectomy during prolapse surgery has been frequently discussed. More and more women request uterus preserving therapy, and with the implantation of alloplastic mesh this is even easier. Therefore, we tested for a difference between patients undergoing hysterectomy and those with uterus preserving therapy as a subgroup analysis and could not determine any difference in QoL.
Of note, limitations to our study need to be mentioned. First, there is no control group. Therefore, we cannot state whether the improvement in QoL is superior to that after native tissue repair. Furthermore, we did use a validated questionnaire on pelvic floor function but not on sexual function. During follow-up we recognized that in the discussion about the role of mesh surgery sexual function is an important item, we added further questions on sexual function. A validated questionnaire on sexual function was not used. Apart from mesh implantation, additional surgeries were performed which possibly added to the improvement in QoL. Last but not least, this was an industry-sponsored trial. However, the manufacturer´s support made possible the external monitoring implementation of a clinical event committee, but did not influence the interpretation and publication of these data.
To summarize, pelvic floor-related quality of life and pull pain improved significantly 6 months after implantation of an alloplastic mesh with titanium coating compared to preoperative values. Twelve months after surgery, there was further improvement. We consider this data of a prospective multicenter trial to be important for the ongoing discussion on the use of alloplastic meshes in POP surgery.
Abbreviations
- POP:
-
Pelvic organ prolapse
- QoL:
-
Quality of life
- FDA:
-
US food and drug administration
- eCRF:
-
Electronic case report form
- MCID:
-
Minimal clinically important difference
- POP-Q:
-
Pelvic organ prolapse quantification system
References
Jelovsek JE, Maher C, Barber MD (2007) Pelvic organ prolapse. Lancet 369(9566):1027
Karabulut A, Ozkan S, Koçak N, Alan T (2014) Evaluation of confounding factors interfering with sexual function in women with minimal pelvic organ prolapse. Int J Gynaecol Obstet 127(1):73–76
Maher C, Feiner B, Baessler K, Schmid C (2013) Surgical management of pelvic organ prolapse in women. Cochrane Database Syst Rev 4:CD004014. doi:10.1002/14651858.CD004014.pub5
FDA Safety Communication (2013) Update on serious complications associated with transvaginal placement of surgical mesh for pelvic organ prolapse. http://www.fda.gov/medicaldevices/safety/alertsandnotices/publichealthnotifications/ucm061976.htm
Köckerling F, Schug-Pass C (2014) What do we know about titanized polypropylene meshes? An evidence-based review of the literature. Hernia 18(4):445–457. doi:10.1007/s10029-013-1187-3 (Epub 2013 Nov 20. Review)
Digesu GA, Khullar V, Cardozo L, Robinson D, Salvatore S (2005) P-QOL: a validated questionnaire to assess the symptoms and quality of life of women with urogenital prolapse. Int Urogynecol J Pelvic Floor Dysfunct 16(3):176–181
Lenz F, Stammer H, Brocker K, Rak M, Scherg H, Sohn C (2009) Validation of a German version of the P-QOL questionnaire. Int Urogynecol J Pelvic Floor Dysfunct 20(6):641–649. doi:10.1007/s00192-009-0809-x
Brosteanu O, Houben P, Ihrig K, Ohmann C, Paulus U, Pfistner B, Schwarz G, Strenge-Hesse A, Zettelmeyer U (2009) Risk analysis and risk adapted on-site monitoring in noncommercial clinical trials. Clin Trials. 6(6):585–596. doi:10.1177/1740774509347398
Norman GR, Sloan JA, Wyrwich KW (2003) Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care 41(5):582–592
Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) (2015) Preliminary Opinion on the safety of surgical meshes used in urogynecological surgery. European Union, 2015. ISSN 1831-4783 ISBN 978-92-79-43917-9. doi:10.2772/63702
Barber MD, Brubaker L, Nygaard I, Wheeler TL 2nd, Schaffer J, Chen Z, Spino C (2009) Pelvic floor disorders network. Defining success after surgery for pelvic organ prolapse. Obstet Gynecol 114(3):600–609. doi:10.1097/AOG.0b013e3181b2b1ae
Zyczynski HM, Rickey L, Dyer KY, Wilson T, Stoddard AM, Gormley EA, Hsu Y, Kusek JW, Brubaker L (2012) Urinary incontinence treatment network. Sexual activity and function in women more than 2 years after midurethral sling placement. Am J Obstet Gynecol 207(5):421.e1–6
Rogers RG, Kammerer-Doak D, Darrow A, Murray K, Olsen A, Barber M, Qualls C (2004) Does sexual function change after surgery for stress urinary incontinence and/or pelvic organ prolapse? A multicenter prospective study. Am J Obstet Gynecol 191:206–210
Barski D, Otto T, Gerullis H (2014) Systematic review and classification of complications after anterior, posterior, apical, and total vaginal mesh implantation for prolapse repair. Surg Technol Int 24:217–224
Marschke J, Hengst L, Schwertner-Tiepelmann N, Beilecke K, Tunn R (2015) Transvaginal single-incision mesh reconstruction for recurrent or advanced anterior vaginal wall prolapse. Arch Gynecol Obstet 291(5):1081–1087. doi:10.1007/s00404-014-3497-9 (Epub 2014 Oct 4)
Acknowledgments
We thank Mr. Arim Shukri for the statistical analysis and Mr. Lutz Sternfeld for the external monitoring.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was sponsored by pfm medical ag, Cologne, Germany.
Conflict of interest
We have had full control of all primary data and agree to allow the Journal to review our data if requested.
Rights and permissions
About this article

Cite this article
Farthmann, J., Mengel, M., Henne, B. et al. Improvement of pelvic floor-related quality of life and sexual function after vaginal mesh implantation for cystocele: primary endpoint of a prospective multicentre trial. Arch Gynecol Obstet 294, 115–121 (2016). https://doi.org/10.1007/s00404-016-4014-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-016-4014-0