
Abstract
Introduction
While surgical technique and implant technology for total hip arthroplasty (THA) has improved over the years, it is unclear whether recent progress has translated to improved clinical outcomes for young patients. The goal of this study is to determine trends in (1) indications, (2) surgical technique (3) clinical and radiographic outcomes, and (4) survivorship for THA in patients younger than 30 years of age.
Methods
MedLine, Cochrane, EMBASE, and Google Scholar were searched using several key phrases for articles focusing on THA performed on patients younger than 30 years of age between 1971 and 2020. A total of 34 qualifying articles were identified and stratified into three groups according to operative years and compared to one another on the basis of (1) indications; (2) fixation technique; (3) implant design; (4) clinical and radiographic outcomes; and (7) survivorship.
Results
The mean patient age at index THA were 20.5 (9–30), 22.1 (11–30) and 21.5 (10–30) years, respectively, for each study group. Over time, patients underwent fewer THAs for JRA (Juvenile Rheumatoid Arthritis) (p < 0.001) but more for post-treatment and iatrogenic avascular necrosis (p < 0.001; p < 0.001). Early THAs primarily used metal on UHMWPE (Ultra high molecular weight polyethylene) (71.7%, p < 0.001), modern THA predominantly use ceramic on HXLPE (Highly cross-linked polyethylene) (42.5%, p < 0.001). Early fixation methods used cement (60.4%, p < 0.001), and modern fixation primarily use press fit technology (95.9%, p < 0.001). Prevalence of radiographic loosening decreased significantly (p < 0.001) over time. There was no significant difference in clinical improvement on HHS. Lastly, fewer patients required THA revision in recent decades (p < 0.001).
Conclusions
Advances in surgical technique and technology have served to improve implant longevity. Surprisingly, subjective clinical scores showed no significant improvement over time, suggesting that early iterations of THA were extremely successful.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
With the introduction of Charnley’s low friction hip arthroplasty in the 1960’s, total hip arthroplasty (THA) has reshaped the natural history of hip arthritis. A disease formerly managed with soft-tissue interposition yielding meager results could suddenly be addressed with cement, metal and polyethylene with high rates of success [1]. THA has continued to gain popularity and it is estimated that 635,000 THAs will be performed annually by the year 2030 [2]. Over the last several decades, technological advancements have been made in surgical technique, implant design, and material science. In the United States cementless designs have generally replaced traditional cement fixation and several iterations of bearing surfaces have been developed to combat wear and osteolysis [3]. As implant longevity has significantly improved, younger patients are being considered candidates for THA.
Although THA is primarily used to address the effects of end stage osteoarthritis in older, lower demand individuals, an increasing number of extremely young patients are undergoing THA to address end stage hip disease [4]. Historically, the literature has shown decreased survivability and increased revision rates in THAs performed on young patients, but more recent reviews have begun to demonstrate significantly improved implant survivability [Wangen et al.; Chmell et al.; Lee et al.; Taheriazam and Saeidinia, “Short-Term Outcomes of One-Stage Bilateral Total Hip Arthroplasty in Young Patients (< 30 Years Old)”]. While one may conclude that improvements in THA outcomes and longevity may be attributable to advances in technique and technology, no study has provided conclusive evidence to support this assumption.
The goal of this systematic review and meta-analysis is to track the evolution of THAs performed patients less than 30 years of age to determine if any conclusions can be drawn comparing newer techniques and technologies to previous generations. We specifically evaluated: (1) changes in surgical indications, (2) implant related differences, (3) implant survivability, and (4) objective clinical and radiographic outcomes.
Materials and methods
Search strategy and criteria
A systematic review was conducted according to the Preferred Reported Items for Systematic Reviews and Meta-Analysis Statement for Individual Patient Data (PRISMA) [9]. All included studies were retrospective in nature, thereby making this review Level III evidence. Comprehensive database queries of MEDLINE, EMBASE, The Cochrane Library, and Google Scholar were performed including all articles published up to May of 2020. Articles were filtered using the following search terms: “Total hip arthroplasty” OR “Total hip replacement” OR “Hip Prosthesis” in combination with “Juvenile” OR “Immature” OR “Adolescent” OR “Young” OR “Under 30” OR “Under thirty.” Unpublished data and conference proceedings were excluded from the data set. Once a final list of articles had been obtained according to the inclusion and exclusion criteria listed below, the reference section from each study was reviewed to capture any article which may have been missed in our initial database search.
Inclusion and exclusion criteria
This review is specifically aimed at analyzing total hip arthroplasty performed on patients under 30 years of age; therefore, studies looking at hip resurfacing or hemiarthroplasty were excluded. Studies analyzing total knee arthroplasty in combination with THA were excluded from this review. All etiologies of end stage hip disease were considered.
Original articles written in English were considered and were included if the following criteria were met: (1) All patients in the study were under the age of 30; (2) All patients underwent THA; (3) Study population was greater than 5 patients; (4) Minimum of 2 years clinical follow–up; (5) Indications for THA were reported; (6) Radiographic outcomes reported; (7) Report of revision rates and indications; (8) Reporting of objective clinical outcome data. Studies were excluded if any of these criteria were not met. Review articles were also excluded.
Search results
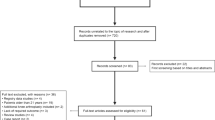
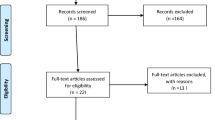
A total of 20,816 articles were identified and exported to citation management software (Mendeley, London, United Kingdome) where 10,291 duplicate articles were removed. The remaining 10,525 articles were manually processed to remove 6501 not primarily focusing on total hip arthroplasty and another 3907 which included patients > 30 years old. Abstracts for the remaining 118 articles were reviewed independently by two authors to select studies with the inclusion criteria listed above. Where disagreement between authors existed, a third reviewer was consulted. Figure 1 provides a summary of the review process according to PRISMA guidelines [9]. Full length manuscripts of the remaining articles were reviewed by a single author and the bibliographies were cross referenced for completeness. In total, thirty-four articles met our inclusion criteria (Table 1) [5, 7, 8, 10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42].

PRISMA flow chart outlining article review process
The years during which patients were collected for each study was recorded and the midpoint was calculated. To show trends in indications, technique, and outcomes over time, we split the included articles as evenly as possible into three groups. The timeframe of surgery was collected for each study and the midpoint of this timeframe was calculated. The articles were then evenly distributed into two groups of 11 and one group of 12. Patients in Group I underwent THA at study midpoints from 1971 to 1992, Group II from 1993 to 1999, and Group III from 2000 to 2015. Studies in Group I had an average of 31 patients undergoing 42 THAs with a total of 459 THAs performed, Group II studies averaged 54 patients undergoing 71 THAs with a total of 780 THAs performed and Group III studies had an average of 53 patients undergoing an average of 77 THAs with a total of 918 THAs performed.
For each manuscript, the following data were recorded where possible: history of previous hip surgery, indication for surgery, surgical details including fixation technique and bearing surface selection, radiographic and clinical outcome data, revision rates, and indications for revision.
Assessment of study quality
Studies were independently reviewed each study and the Methodological Index for Non-randomized Studies (MINORS) scoring system for non-randomized studies was used to quantify the quality of each study (Table 10 of the appendix) [43]. The average MINORS score for Groups I, II, and III were 10.4 (9–11), 10.7 (10–12), and 10.8 (10–12), respectively.
Data collection and analysis
Data points were retrieved from each of the 34 studies including history of previous hip surgery, indications for total hip arthroplasty, surgical technique, bearing surface, assessment of follow-up radiographic studies, revision rates, and indications as well as clinical outcome measures. Information on previous hip surgery was not available for the majority of included studies (21 of 34 studies not reporting history of previous intervention). All but one study included indications for THA and all studies reported surgical technique, bearing surface, radiographic outcome, survival, and clinical outcome measures.
Data analysis was performed through Excel (Microsoft, Redmond, WA) and GraphPad (PRISM, San Diego, CA) under a fixed effect model. Categorical variables were compared with either Chi squared or Fisher’s exact test where appropriate. We used the Cochrane–Mantel–Haenszel adjustment in subgroup analysis of categorical variables to address the use repeated 2 × 2 contingency tables. Continuous variables were verified for normal distribution using Kolmogorov–Smirnov, Shapiro–Wilk or D'Agostino & Pearson tests. Frequency weighted means were reported, and Welch’s Analysis of Variance (ANOVA) test was performed on normally distributed data followed by Turkey–Kramer subgroup analysis. Kruskal–Wallis intergroup analysis followed by Nemenyi test subgroup analysis was performed for non-normally distributed continuous data. For each category, all three groups were analyzed together (intergroup) and subgroup analysis (intra-group) was performed reflexively if a significant p value was obtained. A p value of < 0.05 was considered significant.
Results
Age demographics
Each study provided mean age at the time of index total hip. All but one study provided age ranges. The mean age at index THA for Group I was 20.5 years, Group II was 22.1 years and Group III was 21.5. A summary of this data can be found in Table 2.
Indications and history of previous hip surgery
The indications for THA significantly changed over time. In Group I, juvenile rheumatoid arthritis (JRA) was the most common indication for arthroplasty (40.8%) followed by congenital hip dislocation and post-traumatic arthritis. JRA remained the most common indication for THA in Group II (22.5%), with iatrogenic avascular necrosis (IAVN) being the most common indication for THA in Group III (41.5%). Overall, there was a decrease in the number of THAs performed for post-traumatic arthritis while the number of THAs performed for post-treatment AVN increased over time. Though congenital hip dislocations/developmental hip dysplasia was a common indication in all groupings, there was no significant change in rates of THAs performed for this condition (Table 3). Thirteen studies reported on prior history of hip surgery. As time progressed, proportionally more patients had undergone previous hip surgery prior to receiving THA (Group I—21.7%; Group II—30.8%, Group III—48.7%).
The average follow-up duration in Group I was 11.4 years, 11.5 years in Group II, and 6 years in Group III (Table 12 of the appendix).
Surgical fixation technique and bearing surface
There were significant differences in fixation technique between groups. The majority of patients in Group I underwent cementation of both the femoral and cup components (60.4%), Group II received primarily cementless components (65.6%) and Group III had nearly ubiquitous use of cementless fixation (95.9%) (Table 4).
A myriad of bearing surfaces were employed and various trends were recognized. The most common bearing surface in Group I was metal on ultra-high molecular weight polyethylene (UHMWPE) (71.7%) which was supplanted by ceramic-on-ceramic bearings in Group II (34.5%) and then ceramic on highly cross-linked polyethylene (HXLPE) in Group III (42.5%) (Table 5).
Implant survival and indications for revision
Overall, there was a significant decrease in revision rates over time. Nearly one-third of patients in Group I required a future revision THA (29.8%), dropping to 15.5% in Group II and further falling to 4.5% in Group III (Table 6). There was no significant difference in the average time to revision (Table 11 of the appendix).
The main indication for revision THA in all groups was aseptic loosening, though there was significant reduction in the rates of aseptic loosening over time (Group I—22.4%, Group II—9.9%, Group III—1.7%). Recurrent instability was the second most common cause for revision in Groups I and II (2.6% and 2.1%, respectively) but was not a frequent cause for revision in Group III. Lastly, there was a significant increase in revision THA performed secondary to wear in Group III compared to groups I and II (Table 7).
Radiographic and clinical outcome
Radiographic evidence of loosening was reported as either isolated femoral stem loosening, isolated cup loosening or combined cup and stem loosening. In all categories, there was a significant decrease in reported loosening over time (Table 8).
Clinical outcome data were reported via several different protocols. A total of seven studies in Groups I and II implemented the modified Merle d’Aubigne (modMdA) score to assess pre-operative and post-operative function. Improvement in modMdA score between Groups I and II were similar (7.9 and 7.7, respectively). The majority of included studies used Harris Hip Score (HHS) to assess clinical outcome. In total, 18 studies reported pre-operative HHS and 24 reported post-operative scores. Analysis showed no significant difference in HHS score improvement amongst the three groups of studies (Table 9).
Discussion
Total hip arthroplasty has served as an excellent long-term solution to end stage hip arthritis in older, lower demand patients but has historically demonstrated variable success in extremely young patients. While THA has undergone several iterations over the last 5 decades, it is unknown whether these advances have translated to improvements in extremely young patients requiring arthroplasty. A few systematic reviews and meta-analyses have been published investigating overall outcomes of THA in patients under 30 years old, but no review has established whether modern surgical techniques offer any improvement over previous generations [44,45,46]. The goal of this study was to track changes in surgical indications, technique, technology, survivability, and outcomes over time to determine if modern methods have resulted in patients benefit.
Regarding our first study objective on operative indications, over time we found that proportionally fewer patients were undergoing THA for a primary diagnosis of juvenile rheumatoid arthritis (JRA). This is consistent with the literature describing the overall rate of THA performed for rheumatic patients. In a large database review by Mertelsmann-Voss et al., the rate of arthroplasty performed in patients with JRA decreased at a rate of 3.6% per year from 1991 to 2005, and the mean age to arthroplasty rose substantially from 30.9 to 36.7 years. The authors primarily attributed this to the introduction of disease modifying antirheumatic drugs (DMARDS) beginning with methotrexate in the early 1990’s followed by the biologic DMARDS targeting tumor necrosis factor-alpha in 1998 [47].
Our review of the literature further demonstrated that the proportion of patients undergoing THA for idiopathic AVN had significantly increased over time. Reports have shown that the rates of idiopathic AVN have remained relatively stable, so this increase is likely a proportional and reciprocal response to the significant decrease in rates of THA for JRA [48, 49]. We also showed an increase in the proportion of patients undergoing THA as a result of treatment induced osteonecrosis of the femoral head, specifically resulting from glucocorticoid use. Studies have shown that the rates of post-treatment osteonecrosis of the femoral head doubled from 1989 to 2003, but it is thought to be the result of increased use of MRI in evaluating hip pathology rather than an actual increase in disease prevalance [50]. Lastly, we found that the proportion of THAs performed for post-traumatic arthritis was significantly lower in Group III compared to Groups I and II. This may be the result of improved management of fractures about the hip, but literature supporting this claim is limited.
In evaluating surgical technique, we assessed both the method of fixation as well as choice in bearing surface. As expected, Group I demonstrated the heaviest utilization of cement fixation for both the femoral and acetabular components. Cement fixation was supplanted by press fit technology in Group II, although there was still frequent reliance on cement fixation for one or both components. Modern implants are almost exclusively cementless designs. Literature comparing cemented to cementless technology suggests that cementless components may be less prone to late aseptic loosening compared their cemented counterparts [51,52,53]. Bearing surface selection is a controversial topic and this is reflected in the literature by the myriad of bearing surface combinations reported. Early studies were limited to metal heads articulating with monobloc ultra-high molecular weight polyethylene (UHMWPE) cups which were quickly supplanted with metal shells containing UHMWPE liners. The timeframe of Group II coincides with the development of highly cross-linked polyethylene (HXLPE) which exhibited improved wear properties over conventional UHMWPE and decreased osteolysis secondary to particulate wear products [54]. This period also demonstrated the highest proportions of ceramic-on-ceramic and metal-on-metal bearing interfaces in a continued search to combat issues with wear, durability and corrosion. Unfortunately, ceramic liners have been prone to fracture and metal-on-metal implants tend to demonstrate high levels of failure secondary to metal ion production [55,56,57]. While no consensus exists on bearing surface selection for younger patients, the most common combination (as demonstrated in Group III) is a ceramic head and a HXLPE liner which combines low wear rates with decreased fretting corrosion, virtually eliminates issues with metal ion production, and does not suffer from problems related to brittleness.
Implant survivorship was shown to improve significantly over time likely due to a synthesis of the factors mentioned above. It has been demonstrated that patients undergoing THA for JRA have worse implant survivorship compared to their primary osteoarthritis counterparts [6, 11, 12]. Thus, as the proportion of patients indicated for THA secondary to JRA decreased, implant survivorship reciprocally increased. Similarly, transitioning from cemented to cementless components has shown a decrease in late aseptic loosening as mentioned above. Lastly, as material science evolved, more stable bearing surfaces were developed which decreased the amount of peri-implant osteolysis secondary to particulate byproducts. Interestingly, our data show a proportional increase in the number of revisions performed secondary to wear in Group III compared with Groups I and II. The cause for this is likely twofold. First, the revision rate in Group III was extremely low compared to the other groups which magnifies the effect of individual patients. Second, patients in Group III may not have experienced early complications such as aseptic loosening or recurrent instability in their course of care thus allowing for a long-term mechanism (i.e. wear) to be a more prominent indication for revision.
In regard to radiographic outcomes, literature demonstrates a significant decrease in implant radiolucency over time. This is supported by the discussion above on indications, fixation strategy and bearing surface. Fewer patients with JRA, decreased use of cemented fixation and avoidance of bearing surfaces prone to peri-implant osteolysis all combine to improve prevalence of radiographic loosening. Interestingly, the literature did not show a significant difference in overall clinical improvement, measured by Harris Hip Score (HHS), over time. This indicates that despite improvements in implant survivability and decreased radiolucency as technology advanced, patients are receiving the same level of pain relief and functional improvement as they were 5 decades ago. This result must be taken with a word of caution as several early studies did not report pre-operative HHS or employed a completely different clinical outcome scoring system (Merle d’Aubigne, hip disability and osteoarthritis outcome score, etc.).
Though this is an exhaustive review of the current literature, it has several limitations. First, none of the studies meeting inclusion criteria were prospective, randomized controlled trials (RCTs) which limits the value of data pooling. Compounding the issue was a lack of standardized reporting of various categories of data. For instance, earlier studies frequently reported Merle d’Aubigne scores to assess clinical outcome while later studies employed Harris Hip Scores as standard. Other inconsistencies included failure to obtain pre-operative clinical scores in some studies, variability in radiographic reporting methods, and a majority of studies not including rates of previous hip surgery. Furthermore, splitting the studies into separate groups precluded performance of heterogeneity studies such as an I2 statistic. That being said, this collection of studies is the best available and conclusions should be viewed cautiously. There were several articles excluded from the final review as they were missing key data points. While inclusion of these studies could have bolstered support for other categories, we did not want to compromise on study quality especially in light of the fact that all included articles were retrospective. A final point to consider is the method used to group the studies. In an effort to ensure that each defined group had enough data, we decided to split the 34 studies as evenly as possible according to study midpoint. While this succeeded in providing a fairly consistent data volume across groupings, this method of grouping is susceptible to variability in publication rates on the topic of THA in patients under 30 years of age. This is illustrated by the fact that the studies included in Group I span several decades while Group II merely spans 8 years. Nevertheless, we believe that the frequency of published articles pertaining to this topic directly mirrors changes in industry and surgical techniques, thus justifying our method of study grouping.
In conclusion, this systematic review and meta-analysis has shown that indications for THA in patients younger than 30 years of age have changed over time transitioning from JRA to IAVN, though several etiologies can contribute to end stage hip disease. Fixation strategies have moved away from cemented implants and are nearly exclusively cementless. This shift in technique along with advances in bearing surface technology have significantly improved rates of revision and radiographic loosening. Nevertheless, post-operative improvement in clinical outcome scores have remained stable over the decades.
References
Learmonth ID, Young C, Rorabeck C (2007) The operation of the century: total hip replacement. Lancet 370(9597):1508–1519. https://doi.org/10.1016/S0140-6736(07)60457-7
Sloan M, Premkumar A, Np S (2018) Projected volume of primary total joint arthroplasty, pp 1455–1460
Khanuja BHS, Vakil JJ, Goddard MS, Mont MA (2011) Cementless femoral fixation in total hip arthroplasty. J Bone Jt Surg. https://doi.org/10.2106/JBJS.J.00774
Skyttä ET, Jarkko L, Antti E, Huhtala H, Ville R (2011) Increasing incidence of hip arthroplasty for primary osteoarthritis in 30-to 59-year-old patients: A population based study from the Finnish Arthroplasty Register. Acta Orthop 82(1):1–5. https://doi.org/10.3109/17453674.2010.548029
Wangen H, Lereim P, Holm I, Gunderson R, Reikeras O (2008) Hip arthroplasty in patients younger than 30 years: excellent ten to 16-year follow-up results with a HA-coated stem. Int Orthop 32(2):203–208. https://doi.org/10.1007/s00264-006-0309-2
Chmell MJ, Scott RD, Thomas WH, Sledge CB (1997) Total hip arthroplasty with cement for juvenile rheumatoid arthritis. Results at a minimum of ten years in patients less than thirty years old. J Bone Jt Surg Am 79(1):44–52. https://doi.org/10.2106/00004623-199701000-00005
Lee Y-K, Kim K-C, Yoon B-H, Kim T-Y, Ha Y-C, Koo K-H (2019) Cementless total hip arthroplasty with delta-on-delta ceramic bearing in patients younger than 30 years. Hip Int. https://doi.org/10.1177/1120700019889592
Taheriazam A, Saeidinia A (2018) Short-term outcomes of one-stage bilateral total hip arthroplasty in young patients (< 30 years old). Orthop Rev (Pavia) 10(2):65–69. https://doi.org/10.4081/or.2018.7542
Moher D et al (2009) Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. https://doi.org/10.1371/journal.pmed.1000097
Chandler H, Reineck F, Wixson R, McCarthy J (1981) Total hip replacement in patients younger than thirty years old. J Bone Jt Surg A 1426–1434 [Online]. http://jbjs.org/article.aspx?articleID=18389. Accessed 17 June 2020
Roach JW, Paradies LH (1984) Total hip arthroplasty performed during adolescence. J Pediatr Orthop 4(4):418–421. https://doi.org/10.1097/01241398-198408000-00005
Witt JD, Swann M, Ansell BM (1991) Total hip replacement for juvenile chronic arthritis. J Bone Jt Surg Ser B 73(5):770–773. https://doi.org/10.1302/0301-620x.73b5.1894663
Maric Z, Haynes RJ (1993) Total hip arthroplasty in juvenile rheumatoid arthritis. Clin Orthop Relat Res 290:197–199
Sochart DH, Porter ML (1997) The long-term results of Charnley low-friction arthroplasty in young patients who have congenital dislocation, degenerative osteoarthrosis, or rheumatoid arthritis. J Bone Jt Surg Am 79(11):1599–1617. https://doi.org/10.2106/00004623-199711000-00001
Sochart DH, Porter ML (1998) Long-term results of cemented Charnley low-friction arthroplasty in patients aged less than 30 years. J Arthroplasty 13(2):123–131. https://doi.org/10.1016/S0883-5403(98)90089-4
Gudmundsson GH, Harving S, Pilgaard S (1989) The Charnley total hip arthroplasty in juvenile rheumatoid arthritis patients. Orthopedics 12(3):385–388
Dudkiewicz I, Salai M, Israeli A, Amit Y, Chechick A (2003) Total hip arthroplasty in patients younger than 30 years of age. Isr Med Assoc J 5(10):709–712
Wroblewski BM, Purbach B, Siney PD, Fleming PA (2010) Charnley low-friction arthroplasty in teenage patients: the ultimate challenge. J Bone Jt Surg - Ser B 92(4):486–488. https://doi.org/10.1302/0301-620X.92B4.23477
Hyder N, Nevelos AB, Barabas TG (1996) Cementless ceramic hip arthroplasties in patients less than 30 years old. J Arthroplasty 11(6):679–686. https://doi.org/10.1016/S0883-5403(96)80006-4
Dudkiewicz I, Salai M, Ganel A, Blankstein A, Chechik A (2002) Total hip arthroplasty in patients younger than 30 years of age following developmental dysplasia of hip (DDH) in infancy. Arch Orthop Trauma Surg 122(3):139–142. https://doi.org/10.1007/s004020100307
Kitsoulis PB, Stafilas KS, Siamopoulou A, Soucacos PN, Xenakis TA (2006) Total hip arthroplasty in children with juvenile chronic arthritis: long-term results. J Pediatr Orthop 26(1):8–12. https://doi.org/10.1097/01.bpo.0000187997.84213.d9
Bilsel N, Gokce A, Kesmezacar H, Mumcuoglu E, Ozdogan H (2008) Long-term results of total hip arthroplasty in patients with juvenile rheumatoid arthritis. Acta Orthop Traumatol Turc 42(2):119–124. https://doi.org/10.3944/AOTT.2008.42.2.119
Busch VJJF, Clement ND, Mayer PFJ, Breusch SJ, Howie CR (2012) High survivorship of cemented sockets with roof graft for severe acetabular dysplasia. Clin Orthop Relat Res 470(11):3032–3040. https://doi.org/10.1007/s11999-012-2346-z
Busch V, Klarenbeek R, Slooff T, Schreurs BW, Gardeniers J (2010) Cemented hip designs are a reasonable option in young patients. Clin Orthop Relat Res 468(12):3214–3220. https://doi.org/10.1007/s11999-010-1355-z
Schmitz MWJL, Busch VJJF, Gardeniers JWM, Hendriks JCM, Veth RPH, Schreurs BW (2013) Long-term results of cemented total hip arthroplasty in patients younger than 30 years and the outcome of subsequent revisions. BMC Musculoskelet Disord 14:37. https://doi.org/10.1186/1471-2474-14-37
Hannouche D et al (2016) Ceramic-on-ceramic THA implants in patients younger than 20 years. Clin Orthop Relat Res 474(2):520–527. https://doi.org/10.1007/s11999-015-4546-9
Kim YH, Park JW, Kim JS (2012) Cementless metaphyseal fitting anatomic total hip arthroplasty with a ceramic-on-ceramic bearing in patients thirty years of age or younger. J Bone Jt Surg Ser A 94(17):1570–1575. https://doi.org/10.2106/JBJS.K.00697
Yoon HJ, Yoo JJ, Yoon KS, Koo K-H, Kim HJ (2012) Alumina-on-alumina THA performed in patients younger than 30 years: a 10-year minimum followup study. Clin Orthop Relat Res 470(12):3530–3536. https://doi.org/10.1007/s11999-012-2493-2
Tsukanaka M et al (2016) Implant survival and radiographic outcome of total hip replacement in patients less than 20 years old. Acta Orthop 87(5):479–484. https://doi.org/10.1080/17453674.2016.1212180
Girard J, Bocquet D, Autissier G, Fouilleron N, Fron D, Migaud H (2010) Metal-on-metal hip arthroplasty in patients thirty years of age or younger. J Bone Jt Surg Am 92(14):2419–2426. https://doi.org/10.2106/JBJS.I.01644
Pakos EE, Paschos NK, Xenakis TA (2014) Long term outcomes of total hip arthroplasty in young patients under 30. Arch Bone Jt Surg 2(3):157–162
Agrawal Y, Kerry RM, Stockley I, Hamer AJ (2020) Review of total hip arthroplasty in patients younger than 30 years: mid- to long-term results. Hip Int. https://doi.org/10.1177/1120700020901685
Daurka JS, Malik AK, Robin DA, Witt JD (2012) The results of uncemented total hip replacement in children with juvenile idiopathic arthritis at ten years. J Bone Jt Surg Br 94(12):1618–1624. https://doi.org/10.1302/0301-620X.94B12.29124
Clohisy JC et al (2010) Function and fixation of total hip arthroplasty in patients 25 years of age or younger. Clin Orthop Relat Res 468(12):3207–3213. https://doi.org/10.1007/s11999-010-1468-4
Shin EH, Moon KH (2018) Cementless total hip arthroplasty in young patients under the age of 30: a minimum 10-year follow-up. Hip Int 28(5):507–513. https://doi.org/10.1177/1120700017752339
D’Ambrosi R, Marciandi L, Frediani PV, Facchini RM (2016) Uncemented total hip arthroplasty in patients younger than 20 years. J Orthop Sci 21(4):500–506. https://doi.org/10.1016/j.jos.2016.03.009
Gililland JM, Anderson LA, Erickson J, Pelt CE, Peters CL (2013) Mean 5-year clinical and radiographic outcomes of cementless total hip arthroplasty in patients under the age of 30. Biomed Res Int 2013:649506. https://doi.org/10.1155/2013/649506
Finkbone PR, Severson EP, Cabanela ME, Trousdale RT (2012) Ceramic-On-ceramic total hip arthroplasty in patients younger than 20 years. J Arthroplasty 27(2):213–219. https://doi.org/10.1016/j.arth.2011.05.022
Byun J-W, Yoon T-R, Park K-S, Seon J-K (2012) Third-generation ceramic-on-ceramic total hip arthroplasty in patients younger than 30 years with osteonecrosis of femoral head. J Arthroplasty 27(7):1337–1343. https://doi.org/10.1016/j.arth.2011.07.004
Costa CR, Johnson AJ, Mont MA (2012) Use of cementless, tapered femoral stems in patients who have a mean age of 20 years. J Arthroplasty 27(4):497–502. https://doi.org/10.1016/j.arth.2011.07.005
Mardani-Kivi M, Karimi-Mobarakeh M, Asadi K, Hashemi-Motlagh K, Saheb-Ekhtiari K (2013) Evaluation of clinical outcomes of cementless total hip arthroplasty in patients under 30 years of age. Eur J Orthop Surg Traumatol 23(7):785–790. https://doi.org/10.1007/s00590-012-1084-y
Kamath AF, Sheth NP, Hosalkar HH, Babatunde OM, Lee G-C, Nelson CL (2012) Modern total hip arthroplasty in patients younger than 21 years. J Arthroplasty 27(3):402–408. https://doi.org/10.1016/j.arth.2011.04.042
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (Minors): development and validation of a new instrument. ANZ J Surg 73(9):712–716. https://doi.org/10.1046/j.1445-2197.2003.02748.x
Gee MJ, Ajuied A, Shah Z, George M, Bankes MJK (2013) Systematic review of total hip arthroplasty in patients under 30 years old. Hip Int 23(4):345–351. https://doi.org/10.5301/hipint.5000002
Walker RP et al (2016) Functional outcomes of total hip arthroplasty in patients aged 30 years or less: a systematic review and meta-analysis. Hip Int 26(5):424–431. https://doi.org/10.5301/hipint.5000376
Adelani MA, Keeney JA, Palisch A, Fowler SA, Clohisy JC (2013) Has total hip arthroplasty in patients 30 years or younger improved? A systematic review. Clin Orthop Relat Res 471(8):2595–2601. https://doi.org/10.1007/s11999-013-2975-x
Mertelsmann-Voss C, Lyman S, Pan TJ, Goodman SM, Figgie MP, Mandl LA (2014) US trends in rates of arthroplasty for inflammatory arthritis including rheumatoid arthritis, juvenile idiopathic arthritis, and spondyloarthritis. Arthritis Rheumatol (Hoboken NJ) 66(6):1432–1439. https://doi.org/10.1002/art.38384
Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y (2010) Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clin Orthop Relat Res 468(10):2715–2724. https://doi.org/10.1007/s11999-010-1292-x
Mankin HJ (1993) Nontraumatic necrosis of bone (Osteonecrosis). N Engl J Med 326(22):1473–1479
Weinstein RS (2012) Glucocorticoid-induced osteonecrosis. Endocrine 41(2):183–190. https://doi.org/10.1007/s12020-011-9580-0
Markel DC, Hora N, Grimm M (2002) Press-fit stability of uncemented hemispheric acetabular components: a comparison of three porous coating systems. Int Orthop 26(2):72–75. https://doi.org/10.1007/s00264-001-0314-4
Corten K, Bourne RB, Charron KD, Au K, Rorabeck CH (2011) What works best, a cemented or cementless primary total hip arthroplasty?: minimum 17-year followup of a randomized controlled trial. Clin Orthop Relat Res 469(1):209–217. https://doi.org/10.1007/s11999-010-1459-5
Emerson RH, Head WC, Emerson CB, Rosenfeldt W, Higgins LL (2002) A comparison of cemented and cementless titanium femoral components used for primary total hip arthroplasty: a radiographic and survivorship study. J Arthroplasty 17(5):584–591. https://doi.org/10.1054/arth.2002.32696
Kurtz SM, Gawel HA, Patel JD (2011) History and systematic review of wear and osteolysis outcomes for first-generation highly crosslinked polyethylene. Clin Orthop Relat Res 469(8):2262–2277. https://doi.org/10.1007/s11999-011-1872-4
Traina F, De Fine M, Bordini B, Toni A (2012) Risk factors for ceramic liner fracture after total hip arthroplasty. HIP Int 22(6):607–614. https://doi.org/10.5301/HIP.2012.10339
Traina F, De Fine M, Di Martino A, Faldini C (2013) Fracture of ceramic bearing surfaces following total hip replacement: A systematic review. Biomed Res Int. https://doi.org/10.1155/2013/157247
Garbuz DS, Tanzer M, Greidanus NV, Masri BA, Duncan CP (2010) The john charnley award: Metal-on-metal hip resurfacing versus large-diameter head metal-on-metal total hip arthroplasty: a randomized clinical trial. Clin Orthop Relat Res 468(2):318–325. https://doi.org/10.1007/s11999-009-1029-x
Acknowledgements
This study was carried out as a joint effort between the orthopaedic surgery departments of St. Luke’s University Health Network, University of Pennsylvania and Children’s Hospital of Philadelphia. It was not the beneficiary of any outside funding. Dr. Sheth is a paid consultant for Zimmer-Biomet, Smith and Nephew, Medacta, Microport, and SCA. He also receives royalties from Elsevier.
Funding
No funding was received to assist with the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by AK, CO, and BS. The first draft of the manuscript was written by AK and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Sheth is a paid consultant for Zimmer-Biomet, Smith and Nephew, Medacta, Microport, and SCA. He also receives royalties from Elsevier. None of the other listed authors have relevant financial or non-financial interests to disclose.
Ethical approval
This research study was conducted based on previously published data and did not require prior approval from an IRB committee.
Consent to participate
This study was performed based on previously published data with no direct access to patient records.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Konopitski, A., Okafor, C., Smith, B. et al. Evolution of total hip arthroplasty in patients younger than 30 years of age: A systematic review and meta-analysis. Arch Orthop Trauma Surg 143, 1081–1094 (2023). https://doi.org/10.1007/s00402-022-04357-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-022-04357-w