
Abstract
Introduction
Re-establishing anatomic rotational alignment of shaft fractures of the lower extremities remains challenging. Clinical evaluation in combination with radiological measurements is important in pre- and post-surgical assessment. Based on computed tomography (CT), a range of reference values for femoral torsion (FT) and tibial torsion (TT) have historically been reported, which require standardization to optimize the significant intra- and inter-observer variability. The aims of this study were (re-)evaluation of the reference FT and TT angles, determination of the normal intra-individual side-to-side torsional differences to aid the surgical decision-making process for reoperation, and development of a novel 3D measurement method for FT.
Materials and methods
In this retrospective study, we included 55 patients, without any known torsional deformities of the lower extremities. Two radiologists, independently, measured the rotational profile of the femora using the Hernandez and Weiner CT methods for FT, and the tibiae using the bimalleolar method for TT. The intra-individual side-to-side difference in paired femora and paired tibiae was determined. A 3D technique for FT assessment using InSpace® was designed.
Results
FT and TT demographic values were lower than previously reported, with mean FT values of 5.1°–8.8° and mean TT values of 25.5°–27.7°. Maximal side-to-side differences were 12°–13° for FT and 12° for TT. The Weiner method for FT was less variable than the Hernandez method. The new 3D method was equivocal to the conventional CT measurements.
Conclusion
The results from this study showed that the maximal side-to-side tolerance in asymptomatic normal adult lower extremities is 12°–13° for FT and 12° for TT, which could be a useful threshold for surgeons as indication for revision surgery (e.g., derotational osteotomy). We developed a new 3D CT method for FT measurement which is similar to 2D and could be used in the future for virtual 3D planning.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The rotational assessment of long-bone shaft fractures of the lower extremity remains a challenging problem. The operative treatment (i.e., with intramedullary nailing) of these fractures is associated with an increased incidence of rotational malalignment and malunion, especially in comminuted or segmental varieties. Rotational malalignment after femoral fractures occurs in 27.6–40% [1, 2], resulting in excessive internal or external maltorsion. Internal maltorsion is clinically more disabling because of an in-toeing gait [3]. Therefore, maltorsion must be recognized before healing occurs in the early post-operative period to obtain correction with the least invasive approach [4]. While clinical evaluation is important in pre- and post-surgical assessment of these torsional deformities, it serves primarily to raise suspicion and indicates advanced imaging.
Computed tomography (CT) is the current gold standard for measuring lower extremity rotational profiles, although new (semi-) automated three-dimensional (3D) methods may be significantly more accurate [5]. Knowledge of the normal anatomical proportions is essential to evaluate the indication for and degree of complex corrective osteotomies that are precisely planned. New techniques such as 3D printed patient-specific guides [6] and virtual reduction planning have been described [2, 7, 8]. Standardization of these torsional measurements, i.e., femoral torsion (FT) and tibial torsion (TT), is required to optimize the significant intra- and inter-observer variability, caused in part by various reported methods for the (often arbitrary) determination of the femoral neck axis (FNA) and distal tibial axis (DTA). Further error stems from difficulty identifying known landmarks such as the posterior proximal tibial condylar axis [9]. A significant range of reference FT and TT values based on adult populations using different landmarks have been reported (Table 1). This lack of standardization for the measurement technique leads to different threshold values for surgical indication and confuses surgeons [3].
The maximal side-to-side (right versus left) torsional tolerance is an important threshold value to assess whether or not a post-traumatic or post-surgical difference should be considered as pathologic rotational malalignment. Reported norms for maximal differences are 9° for FT [14], 15° for TT [14], and 5°–10° [28] to 15° [1, 17, 23, 29] for whole-leg torsion. However, the indication for corrective osteotomies depends not only on the radiological torsion difference but also on the clinical impairment of gait, and the patient’s perceived disability when compared with the unaffected contralateral limb.
We aimed to evaluate the standard values of FT in a normal adult population using the Hernandez and Weiner methods and those of TT using the bimalleolar method. In addition, we determined the normal intra-individual side-to-side torsional differences in paired femora and tibiae which may help to guide surgical decision-making with respect to derotational osteotomy. Moreover, we compared the Hernandez and Weiner methods for FT measurement using CT, and we developed a novel 3D measurement method for FT.
Materials and methods
Definitions
Variable descriptive terms are used, with torsion being the rotation within a bone segment and rotation being the range of movement of joints between the segments [17]. In this article, we prefer the term torsion to describe version.
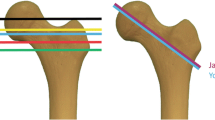
FT is defined as the twist between the proximal and distal parts of the femur in the axial plane [3]. It is measured on axial CT sections of the proximal and distal femur acquired at the level of the joints as the angle between the femoral neck axis (FNA) and a line tangent to the posterior border of the femoral condyles (distal femoral axis) in their widest anteroposterior diameters (“table-top method”) [27]. Various methods have been described to define the FNA [3], which is a line through the femoral head and neck on single or superimposed slices in axial or oblique planes. FT can be either an anteversion or antetorsion (positive angle) or a retroversion (negative angle).
TT is the angle between the proximal reference line and the distal tibial axis (DTA), measured on transverse CT sections acquired through the proximal and distal tibia. The proximal section is at the level of the knee joint just above the fibular head, with a line tangent to the posterior border of the tibial condyles/plateau (proximal tibial axis). The distal section for the distal tibial axis is a line through the medial and lateral malleolus at the level of the ankle joint displaying the tibial pilon in its largest dimension [27]. TT can be either an external torsion (positive angle) or an internal torsion (negative angle).
Total lower limb torsion, the angle between the femoral neck axis and the intermalleolar axis, was not measured for this study. It should be noted that the knee joint (space between the distal femoral condylar axis and the proximal tibial condylar axis) can harbor some torsional deformity, which would contribute to the total limb torsion.
Subjects
The study was conducted at the University Hospitals Leuven. We performed a retrospective search query between July 1st 2015 and August 31st 2016 (Fig. 1) on all patients in our institution that had undergone a CT angiography of the lower limbs for other than fracture-related disease entities, resulting in a total number of 583 obtained scans. Informed consent of all patients was obtained as for standard radiologic examinations. Patient hospital charts were reviewed and none of the patients had a known torsional deformity of the lower limbs or clinical gait impairment. We randomly selected 55 patients, which is an arbitrary form of inclusion. There were 36 male and 19 female patients with a mean age of 64 years (range 50–85 years). Exclusion criteria (Fig. 1) were limbs with a prothesis (e.g., hip or knee arthroplasty) or osteosynthetic material, (history of) fracture, (movement) artifacts, and segmentary scans of the lower leg. In total, 19 femora and 12 tibiae were excluded, as shown in detail in Fig. 1. Exclusion resulted in sample sizes of 91 femora and 98 tibiae, and used for CT measurements and determination of demographic torsional profiles. Out of these sample sizes, 88 paired femora (44 patients) and 94 paired tibiae (47 patients) were used for side-to-side difference measurements. For statistical power, we aimed for a maximum of included cases instead of using similar FT and TT sample sizes. The difference in FT and TT sample sizes was not relevant because of the separate statistical analysis. To test a newly designed 3D measurement method, we randomly selected 34 paired femora (17 patients) among the sample size of 88 paired femora. Sample size calculation for an expected standard deviation of 7° with r (correlation) being 0.9 and alpha 0.05 estimated 16 patients necessary in each group to detect a minimal difference of 2.92° with a power of 95%.

Flow diagram showing the selection process of the study population. FT femoral torsion, TT tibial torsion, CT computed tomography, 3D three-dimensional
Scans were obtained with a Siemens (Erlangen, Germany) CT Somaton Force®. Acquisition parameters were dual energy, a slice thickness of 1 mm, a slice increment of 0.5 mm, and a collimation of 192 × 0.6 mm. The reason for our use of angiographic CT scans was the fact that these were scanned continuously and not segmentary, the latter being a common protocol for torsion measurements in our institution for the purpose of radioprotection. Continuous scans were necessary with regard to 3D reconstructions later on and were taken from the level of the femoral head reaching beyond the level of the tibial malleoli.
Observation
The rotational profiles were measured independently by two radiologists. The methods and objectives of this research were clarified at the start of the study. The images were assessed in the DICOM® (Digital Imaging and Communications in Medicine, NEMA-MITA, Arlington, VA 22209, USA) display on BARCO® (Kortrijk, Belgium) screens in our PACS® (Picture Archiving and Communication System).
Femoral torsion: CT
Various methods have been described to define the FNA. In this study, we compared the Hernandez with the Weiner method defined by Liodakis et al. [29]. These are single-slice methods that are frequently used in our institution. These techniques may be easier to perform by orthopaedic trauma surgeons, as they often do not have access to software for measuring on superimposed slices or modeling data sets in an oblique plane. The Hernandez method [30] draws a line passing through the center of the femoral head and the midpoint of the femoral neck in a CT cut where the femoral head, the isthmus of the femoral neck, and the superior border of the greater trochanter are evident. The Weiner method [29, 31] draws a line passing through the middle of the neck, on a CT cut obtained distal to the femoral head, where the ventral and dorsal cortices are approximately parallel to each other.
FT was measured in 91 femora (47 patients) and bilateral FT values were obtained in 88 paired femora (44 patients). The FT on each CT scan was independently evaluated by both of the observers using the Hernandez method and subsequently remeasured using the Weiner method with at least 1 week in between to avoid memorization of the results with the other methods. Inter-observer correlation and variability were evaluated and side-to-side differences were calculated.
Femoral torsion: 3D
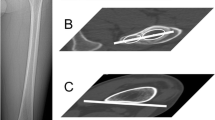
We randomly selected 34 paired femora (17 patients) among our data set of 88 paired femora to test a newly designed 3D method for FT using a volume-rendered 3D imaging software computer model reconstructed from digitized femoral bone contours using the commercial program Siemens (Erlangen, Germany) MMWP InSpace®. Three basic axes are obtained by manual placement of 3D reference points (Fig. 2). The FNA is found in the sagittal plane by turning the femoral neck on its axis (with the femoral neck and femoral head contour projecting as concentric circles) to place the two proximal and distal 3D reference points (Fig. 2a) on the surface of the femoral head and the lateral femur surface in the center of these concentric circles. The long mechanical axis (Fig. 2b) is formed by a point on the narrowest intercondylar region and a point on the surface of the femoral head where the distal 3D point projects in the center of the femoral head sphere. The femoral condylar axis is formed by the placement of two 3D points (Fig. 2c) in lateral views on the posterior surface of the femoral condyles in their widest anteroposterior diameters. Finally, femoral torsion is measurement in a craniocaudal view (“table-top”) (Fig. 3). To neutralize the influence on torsional measurement of the long mechanical axis, the 3D model is turned in such a way that the 3D reference points of this axis project on each other.

a Proximal (green circle) and distal (purple circle) 3D reference points on the femoral head surface and the lateral femoral surface respectively, forming the FNA, projecting in the center of the concentric spheres. The yellow circle shows the proximal 3D reference point of the long mechanical axis. b Distal (caudocranial view, left) and proximal (craniocaudal view, right) 3D reference points (as small yellow dots) of the long mechanical axis. c Side views and dorsal overview of the 3D reference points (orange circles) of the distal condylar axis. The yellow circle shows the distal 3D reference point of the long mechanical axis

Femoral torsion measurement in a craniocaudal view. The contour of the femoral head is shown by the black arrows. In the yellow circle, the 3D reference points of the long mechanical axis (Fig. 2b) project on each other. The proximal (green) and distal (purple) 3D reference points form the femoral neck axis (red). The distal condylar axis is shown in orange. The white arrow indicates how we drag the parallel FNA down (yellow line) to intersect with the distal condylar axis for angle determination. In this patient, the right femoral anteversion was 8.9° (white frame)
Tibial torsion
Various methods have been described to define the DTA on a single CT image. In this study, we used the bimalleolar method defined by Reikerås et al. [9]. This is the line connecting the centers of the medial and lateral malleolus at the level of the ankle joint displaying the tibial pilon in its largest dimension, which has the greatest inter- and intra-observer reliability.
TT was measured using the bimalleolar method in 98 tibiae (51 patients) and bilateral TT values were obtained in 47 patients. Inter-observer correlation and variability were evaluated and side-to-side differences were calculated.
Statistical analysis
Statistical processing was performed with the statistical commercial program Analyse-it® (Leeds, LS3 1HS, United Kingdom). First, inter-observer correlation was evaluated using the Pearson correlation test for continuous data. A Pearson correlation coefficient (Pearson’s r) larger than 0.9 indicates a very good correlation between the observers. Second, inter-observer variability was evaluated using the paired Student’s t test for numerative data. A p value less than 0.05 was considered as a significant inter-observer difference with a confidence interval (CI) of 95%. Third, FT demographics were calculated for left and right extremities with the Hernandez, Weiner and 3D methods; the side-to-side difference in paired femora; and the ‘3D versus Hernandez’ and ‘3D versus Weiner’ differences. Following the inter-observer correlation and variability statistical evaluation, mean results from both observers were used for the calculation of the torsional profiles, side-to-side differences, and 3D versus CT differences. This required a good inter-observer correlation and small inter-observer variability. We continued with mean results instead of those of the most experienced observer, because the latter would have deleted the statistical input of the less experienced observer, which is common practice in statistical analysis.
Results
Femoral torsion
Hernandez method: although there seemed to be a good inter-observer correlation (r = 0.921 left and r = 0.925 right), there were minor but statistically significant (p < 0.0001) mean inter-observer differences of 2.3° (95% CI 1.4°–3.3°) for left femora and 2.5° (95% CI 1.4°–3.5°) for right femora.
Weiner method: although there seemed to be a good inter-observer correlation (r = 0.933 left and r = 0.951 right), there was a minor but statistically significant (p < 0.0009) mean inter-observer difference of 1.4° (95% CI 0.6°–2.1°) for right femora. No significant difference was observed for left femora (p = 0.0558).
Demographic values for FT in right and left femora with the Hernandez, Weiner, and 3D method are shown in Table 2. Mean FT values have a range between 5.1° and 8.8°. Maximal FT has a range between 18.3° and 23.7°.
For 88 paired femora, no significant side-to-side difference was observed with the Hernandez method (p = 0.4294), nor with the Weiner method (p = 0.1177). Femoral torsion values were slightly larger in left femora compared to right femora with a mean difference of 0.7° (SD 5.6°) with the Hernandez method and 1.4° (SD 5.8°) with the Weiner method. The maximal side-to-side difference observed was 12° with the Hernandez method and 13.2° with the Weiner method (Table 3).
For 34 paired femora, the difference between the 3D method and the Hernandez and Weiner methods was calculated. No significant difference between the 3D method and the Hernandez method was observed for left (p = 0.5581) and right (p = 0.2305) femora. No significant difference between the 3D method and the Weiner method was observed for left (p = 0.5503) and right (p = 0.1502) femora.
Tibial torsion
A good inter-observer correlation without a significant inter-observer difference (variability) was observed for both left (r = 0.921, p = 0.5479) and right (r = 0.938, p = 0.3589) tibial torsion measurements.
Demographic values for tibial torsion using the bimalleolar method in left and right tibiae are shown in Table 4. Left and right tibiae had a mean torsion value of 25.5° and 27.7° and a maximum torsion value of 41° and 42°, respectively.
For 94 paired tibiae, a significant side-to-side difference (p = 0.0075) was observed. TT values were larger in right tibiae compared to left tibiae with a mean difference of 2.5° (SD 6.2°) and a maximal side-to-side difference of 12° (Table 3).
Discussion
Rotational malalignment of shaft fractures of the lower limb (i.e., femur and tibia) remains a difficult problem, even in the hands of experienced orthopedic trauma surgeons. Although this is a well-known problem, until today, there is no consensus on the diagnosis (i.e., technique used, degrees of maltorsion acceptable after treatment) and treatment (i.e., surgical technique for correcting the maltorsion) of this disabling complication. Beside clinical evaluation remaining crucial for the early detection, radiological torsional measurement serves as a critical diagnostic tool for evaluating maltorsion after fracture treatment, as well. In daily practice, a combination of both clinical and radiological evaluation is necessary to accurately evaluate the need for a complex corrective osteotomy.
The first aim of our study was (re-) evaluation of the reference FT and TT angles. Despite extensive research on the subject, results on standard demographic torsional profiles keep varying over a significant and inconsistent range (Table 1). Important textbooks and journal publications show mean FT values of 10°–15° [27] to 24.1° [17], and mean TT values of 20°–30° [27] to 34.9° [17]. In this study, we aimed to (re-) evaluate these values (Tables 2, 4). Our mean FT values with the Weiner method were 6.9° (SD 7.6°) for left femora and 5.1° (SD 7.9°) for right femora. Our mean FT values with the Hernandez method were 7.3° (SD 7.9°) for left femora and 6.1° (SD 8.5°) for right femora. The Hernandez values were lower than reported in the literature, for which, to date, no clear explanation can be provided. Kaiser et al. [3] found a higher mean of 11.4° (SD 7.4°), using the Hernandez method, in 26 cadaver femora with four observers. The men–women ratio was around 2-1 in our study, but these lower values can only be partially explained by the known sex difference [5, 20]. For tibial torsion, left and right tibiae had a mean torsion value of 25.5° and 27.7°, slightly lower than in the literature.
The second aim of our study was determination of the normal intra-individual side-to-side torsional differences to aid the surgical decision-making process for reoperation. The normal intra-individual side-to-side torsional difference was determined in 88 paired femora and 94 paired tibiae (Table 3). No significant femoral side-to-side difference was found. The maximal side-to-side difference observed was 12° with the Hernandez method and 13.2° with the Weiner method. A significant tibial side-to-side difference was observed. Tibial torsion values were larger in right tibiae compared to left tibiae with a mean difference of 2.5° (SD 6.2°) and a maximal side-to-side difference of 12°. These upper limits of left–right FT and TT differences in a normal population are essential as cut-off values in clinical pre-operative assessment to decide whether or not a post-traumatic or post-surgical difference is still situated within the normal anatomical range or should rather be regarded as a rotational malalignment and thus planned for a derotational osteotomy. A threshold value of 15° is postulated in the literature. Bråten et al. [32, 33] concluded that a side difference of 15° or more should be regarded as a true torsional deformity after femoral shaft fracture. However, Bråten et al. measured torsion with ultrasound, which is not the current golden standard, and referred to older X-ray and retrospective studies to conclude to the cut-off of 15°. Baumann et al. [34] also referred to the cut-off of 15°, but stated that most patients with deviations even greater than 15° are asymptomatic. In our opinion, 15° should be regarded as an absolute upper limit, as our ‘anatomical’ threshold based on CT measurements showed a maximal tolerance of 12°–13°. A combination of both clinical and radiological evaluation in each individual case is necessary to accurately evaluate the need for a complex surgical revision. Future studies could focus on side-to-side differences in lower limbs that underwent fracture treatment (e.g., intramedullary nailing), which will probably show a significant overlap with healthy limbs, to determine a cut-off value that has the best risk–benefit ratio for surgery. A combined diagnostic pathway including clinical orthopaedic trauma and radiological assessment should be designed.
Total lower limb torsion gathers femoral neck anteversion, tibial torsion, and knee joint rotation as a ‘mean lower limb torsion’, and is helpful in clinical assessment. Mean reported values are 9.8° [17] to 10.8° [23] with a 99% value of intra-individual side-to-side difference of 15.6° [17]. We intuitively presumed that femur positioning does not influence the outcome. However, positioning of the lower extremity during the CT scan should be in the neutral position (with the longitudinal axis of the limb parallel to the z-axis of the CT scanner), because the knee joint rotation angle can only be assessed in a fixed extended position. The latter is due to the screw home mechanism [23], which is the terminal torsion component during the last 30° of knee extension. Due to the angiographic indication for the scans in this study, the limbs were not fixed by a foot-rest on the table. In our opinion, this limitation in our study resulted in a non-reproducible position and, hence, unreliable total lower limb torsion measurement.
The third aim of our study was the development of a novel 3D measurement method for FT. CT is currently the gold standard. On axial slices, various methods for FT measurement have been described with a significant inter- and intra-observer variability because of the (often arbitrary) way in which the FNA is determined. In general, it is difficult to measure the FNA using 2D transverse CT slices that pass obliquely through the neck. This is especially problematic in patients with a high neck shaft angle where only a small portion of the neck is visible per slice. Methods that use two-slice superimposed images or oblique reconstructions can be helpful in high neck shaft angles [3], but, as previously mentioned in this study, we preferred the Hernandez and Weiner techniques, which are frequently used in our institution. These simple two-slice methods may be easier to perform by orthopaedic trauma surgeons, as they often do not have access to software for measuring on superimposed slices or modeling data sets in an oblique plane. Furthermore, we should keep in mind that variation exists in normal anatomy and the impact medical specialty and experience have on using any kind of measurement technique [35, 36]. Therefore, these methods may be equivocal and the estimated range of error unreliable. Standardization with a generally accepted reference method is required to reduce this variability. The same could be said about the DTA in TT measurement.
A gold standard should be designed for clinical practice to optimize the patient’s treatment outcome. However, nowadays, the reliability of the measurement method is more important than the accuracy, as there is no gold standard for comparison [29]. A reference model cannot exist without first obtaining consensus on the measurement method [37]. Nevertheless, ongoing experimental and clinical research on 3D torsional measurements for approximation of the true FT shows that a 3D image is the best approach to a complex 3D anatomical structure and that algorithmically detected correspondences are more precise than those obtainable from human measurements [5]. Literature on 3D TT measurements is scarce [38]. Throughout the years, an evolution from manual to (semi-) automated 3D femur modeling emerged. At first, experimental 3D femur modeling using manual placement of anatomical landmarks was designed [18, 39]. In 2000, Kim et al. [19, 40, 41] conducted three pioneering studies by fitting spheres to the femoral head and combining the centroids of multiple FNA slices with 3D rendering based on the neck axis, the long axis, and the knee axis. Commercial 3D programs have been tested and modified [42, 43]. Next, semi-automated [37, 41, 44, 45] and fully automated [5, 21, 22, 46] methods were developed. A 3D study of Hartel et al. [5] in 1070 left femora showed a mean FT of 14.2° leading to the conclusion that 3D FT measurements are significantly more accurate than the conventional 2D methods. The specific procedure of the 3D method described in our article may look complicated, but is very straightforward in reality. However, it still takes about 10 min after training and requires the availability of Syngo InSpace®, which may not be a generally available program. This 3D technique seems to have future potential in the development of virtual 3D modeling, which has already been available for specific other indications with respect to deformity correction (e.g., CASPA software (Balgrist CARD AG, Zurich, Switzerland) with surgical guides manufactured by Medacta SA (Castel San Pietro, Switzerland) [47]). Future research could focus on validating a 3D technique in normal tibiae and femora with a known rotational malalignment.
In this study, an inter-observer comparison of the Hernandez and Weiner methods was performed. A smaller and more robust inter-observer variability was observed for the Weiner method compared to the Hernandez method. The Weiner method can, thus, be regarded as a better and more reliable method. However, in femora with a curved femoral neck, the Weiner method is less evident [18, 29]. No significant differences were observed comparing 3D and the Weiner or Hernandez methods, which means that 3D might be equivocal to the conventional CT methods. Our inability to detect a difference may be related to the high level of training that the authors had in obtaining CT measurements.
All subjects in our study were adults, mainly elderly patients. In children and adolescents, however, 3D models based on biplanar radiography are comparable to CT measurement results [48]. We did not use the valid biplanar radiography method [e.g., EOS® (Paris, France) [49]], useful in low-dose paediatric radiology, because this requires a standing position, often impossible in trauma, and the presence of osteosynthetic (e.g., metal) artifacts. The 3D measurements using EOS® (Paris, France) are based on generic computer modeling and may not accurately represent the true torsional profile. Regarding the important topic of radioprotection, continuous scans (that were used in this study) have a larger radiation exposure than segmentary scans. The absorbed dose (i.e., the concentration of energy deposited in tissue) of the angiographic CTs included in this study was 550–750 mGy/cm. Future studies could prospectively use and compare a low-dose protocol for the torsional measurements on continuous scans.
We realize that this study has limitations, as it is a retrospective analysis of 55 middle-aged adult patients with torsion measured on CT scans for angiographic indications by only two observers. We randomly selected 55 patients from our database, which is an arbitrary form of inclusion. For statistical power, we aimed for a maximum of included cases instead of using similar FT and TT sample sizes. The difference in FT and TT sample sizes was not relevant because of the separate statistical analysis. Intra-observer variability could not be calculated due to the single measurements by the observers. The Weiner method is less evident in femora with a curved femoral neck. The minor but statistically significant mean inter-observer differences with the Hernandez method (right and left femora) and the Weiner method (right femora) stress the fact that the surgeon should remeasure the torsional values independently. The 3D measurement method requires the availability of Siemens (Erlangen, Germany) MMWP InSpace®, which may not be a generally available program. Including a larger 3D measurement cohort could have changed the results, but a power analysis showed that we could reach statistical significance with a sample size of 17 patients. Total lower limb torsion measurement was not performed because of the non-reproducible position during the scans.
Conclusion
This study showed that the maximal side-to-side tolerance in asymptomatic normal adult lower extremities is 12°–13° for FT and 12° for TT, which is a useful threshold for surgeons as an indication for revision surgery (e.g., derotational osteotomy). Demographic values for FT and TT were lower than previously reported. The Weiner method shows slightly less variability compared to the Hernandez method. We developed a new 3D CT method for FT measurement, which is equivocal to 2D and could be used in the future for virtual 3D planning.
Abbreviations
- FT:
-
Femoral torsion
- FNA:
-
Femoral neck axis
- TT:
-
Tibial torsion
- CT:
-
Computed tomography
- 3D:
-
Three-dimensional
References
Lindsey JD, Krieg JC (2011) Femoral malrotation following intramedullary nail fixation. J Am Acad Orthop Surg 19(1):17–26
Omar M, Suero EM, Hawi N, Decker S, Krettek C, Citak M (2015) Preoperative virtual reduction reduces femoral malrotation in the treatment of bilateral femoral shaft fractures. Arch Orthop Trauma Surg 135:1385–1389
Kaiser P, Attal R, Kammerer M, Thauerer M, Hamberger L, Mayr R et al (2016) Significant differences in femoral torsion values depending on the CT measurement technique. Arch Orthop Trauma Surg 136(9):1259–1264
Dugdale TW, Degnan GG, Turen CH (1990) The use of computed tomographic scan to assess femoral malrotation after intramedullary nailing. A case report. Clin Orthop Relat Res 279:258–263
Hartel MJ, Petersik A, Schmidt A, Kendoff D, Nüchtern J, Rueger JM et al (2016) Determination of femoral neck angle and torsion angle utilizing a novel three-dimensional modeling and analytical technology based on CT datasets. PLoS One 11(3):1–10
Hoekstra H, Rosseels W, Sermon A, Nijs S (2016) Corrective limb osteotomy using patient specific 3D-printed guides: a technical note. Injury 47(10):2375–2380
Citak M, Citak M, Kendoff D, O’Loughlin PF, Tavassol F, Jagodzinski M et al (2009) Estimation of pretraumatic femoral antetorsion in bilateral femoral shaft fractures. Skelet Radiol 38:1183–1187
Stübig T, Hawi N, Min W, Krettek C, Arvani M, Citak M (2012) Accuracy of measurement of femoral anteversion in femoral shaft fractures using a computer imaging software: a cadaveric study. Arch Orthop Trauma Surg 132:613–616
Reikerås O, Høiseth A (1989) Torsion of the leg determined by computed tomography. Acta Orthop Scand 60(3):330–333
Kingsley PC, Olmsted KL (1948) A study to determine the angle of anteversion of the neck of the femur. J Bone Jt Surg 30(3):745–751
Dunlap K, Shands AR Jr, Hollister LC Jr, Gaul JS Jr, Streit HA (1953) A new method for determination of torsion of the femur. J Bone Jt Surg Am 35-A(2):289–311
Budin E, Chandler E (1957) Measurement of femoral neck anteversion by a direct method. Radiology 69(2):209–213
Jend HH (1986) Computed tomographic determination of the anteversion angle. Premises and possibilities. Rofo 144(4):447–452 (Article in German)
Waidelich H, Strecker W, Schneider E (1992) Computed tomographic torsion-angle and length measurement of the lower extremity. The methods, normal values and radiation load. Computertomographische Torsionswinkel- und Längenmessung an der unteren Extremität. Fortschr Röntgenstr 157(9):245–251
Tomczak RJ, Guenther KP, Rieber A, Mergo P, Ros PR, Brambs HJ (1997) MR imaging measurement of the femoral antetorsional angle as a new technique: comparison with CT in children and adults. Am J Roentgenol 168(3):791–794
Schneider B, Laubenberger J, Jemlich S, Groene K, Weber HM, Langer M (1997) Measurement of femoral antetorsion and tibial torsion by magnetic resonance imaging. Br J Radiol 70(834):575–579
Strecker W, Keppler P, Gebhard F, Kinzl L (1997) Length and torsion of the lower limb. J Bone Jt Surg Br 79(6):1019–1023
Sugano N, Noble PC, Kamaric E (1998) A comparison of alternative methods of measuring femoral anteversion. J Comput Assist Tomogr 22:610–614
Kim JS, Park TS, Park SB, Kim JS, Kim IY, Kim SI (2000) Measurement of femoral neck anteversion in 3D. Part 2: 3D modelling method. Med Biol Eng Comput 38(6):610–616
Jain AK, Maheshwari AV, Nath S, Singh MPNM (2003) Anteversion of the femoral neck in Indian dry femora. J Orthop Sci 8:334–340
Casciaro ME, Ritacco LE, Milano F, Risk M, Craiem D (2010) Angle estimation of human femora in a three-dimensional virtual environment. 2010 Annu Int Conf IEEE Eng Med Biol Soc EMBC’10 1:3946–3949
Casciaro ME, Craiem D (2012) Towards automatic measurement of anteversion and neck–shaft angles in human femurs using CT images. Comput Methods Biomech Biomed Eng 5842:1–9 (Taylor & Francis)
Liodakis E, Aljuneidi W, Krettek C, Ettinger M, Kenawey M (2011) The neck–malleolar angle: an alternative method for measuring total lower limb torsion that considers the knee joint rotation angle. Skelet Radiol 40(5):617–621
Park J, Kim J-Y, Kim HD, Kim YC, Seo A, Je M et al (2017) Analysis of acetabular orientation and femoral anteversion using images of three-dimensional reconstructed bone models. Int J Comput Assist Radiol Surg. https://doi.org/10.1007/s11548-016-1514-0
Hutter CG Jr, Scott W (1949) Tibial torsion. J Bone Jt Surg Am 31A:511–518
Jakob RP. Haertel M, Stüssi E (1980) Tibial torsion calculated by computerised tomography and compared to other methods of measurement. J Bone Jt Surg Br 62-B(2):238–242
Waldt S (2013) Lower limb alignments. In: Waldt S, Woertler K (eds) Measurements and classifications in musculoskeletal radiology. George Thieme Verlag KG, New York, pp 5–10
Widjaja PM, Ermers JW, Sijbrandij S, Damsma H, Klinkhamer AC (1985) Technique of torsion measurement of the lower extremity using computed tomography. J Comput Assist Tomogr 9:466–470
Liodakis E, Doxastaki I, Chu K, Krettek C, Gaulke R, Citak M et al (2012) Reliability of the assessment of lower limb torsion using computed tomography: analysis of five different techniques. Skelet Radiol 41(3):305–311
Hernandez RJ, Tachdjian MO, Poznansk AK, Dias LS (1981) CT determination of femoral torsion. Am J Roentgenol 137(1):97–101
Weiner DS, Cook AJ (1980) Computed tomography in the measurement of femoral anteversion. Isr J Med Sci 16(4):288–294
Bråten M, Terjesen T, Rossvoll I (1992) Femoral anteversion in normal adults. Acta Orthop Scand 63(1):29–32
Bråten M, Terjesen T, Rossvoll I (1993) Torsional deformity after intramedullary nailing of femoral shaft fractures. J Bone Jt Surg 75-B:799–803
Baumann F, Angerpointner K, Nerlich M, Neumann C (2015) The relevant axial deviation. Diagnostics and therapy for correction osteotomies of the femur. Chirurg 86:935–941
Yoon RS, Koerner JD, Patel NM, Sirkin MS, Reilly MC, Liporace FA (2013) Impact of specialty and level of training on CT measurement of femoral version: an interobserver agreement analysis. J Orthop Traumatol 14(4):277–281
Panou A, Stanitski DF, Stanitski C, Peccati A, Portinaro NM (2015) Intra-observer and inter-observer errors in CT measurement of torsional profiles of lower limbs: a retrospective comparative study. J Orthop Surg Res 10:67
Berryman F, Pynsent P, McBryde C (2010) A semi-automated method for measuring femoral shape to derive version and its comparison with existing methods. Int J Numer Method Biomed Eng 26(1):807–827
Shin S-Y, Yoon H, Lee S, Oh M-K, Kim R, Park JM et al (2011) The availability of radiological measurement of tibial torsion: three-dimensional computed tomography reconstruction. Ann Rehabil Med 35:673–679 (Internet)
Mahaisavariya B, Sitthiseripratip K, Tongdee T, Bohez ELJ, Vander Sloten J, Oris P (2002) Morphological study of the proximal femur: a new method of geometrical assessment using 3-dimensional reverse engineering. Med Eng Phys 24:617–622
Kim JS, Choi KW, Kim SI (1998) Femoral anteversion: estimation by 3D modelling. Stud Health Technol Inform 52:1025–9
Kim JS, Park TS, Park SB, Kim JS, Kim IY, Kim SI (2000) Measurement of femoral neck anteversion in 3D. Part 1: 3D imaging method. Med Biol Eng Comput 38(6):603–609
Lee YS, Oh SH, Seon JK, Song EK, Yoon TR (2006) 3D femoral neck anteversion measurements based on the posterior femoral plane in ORTHODOC system. Med Biol Eng Comput 44(10):895–906
Wright D, Whyne C, Hardisty M, Kreder HJ, Lubovsky O (2011) Functional and anatomic orientation of the femoral head. Clin Orthop Relat Res 469:2583–2589
Bonneau N, Libourel PA, Simonis C, Puymerail L, Baylac M, Tardieu C, Gagey O (2012) A three-dimensional axis for the study of femoral neck orientation. J Anat 221:465–476
Sangeux M, Pascoe J, Graham HK, Ramanauskas F, Cain T (2015) Three-dimensional measurement of femoral neck anteversion and neck shaft angle. J Comput Assist Tomogr 39(1):83–85
Schröder M, Gottschling H, Reimers N, Hauschild M, Burgkart R (2014) Automated morphometric analysis of the femur on large anatomical databases with highly accurate correspondence detection. Open Med J 1:15–22
Hirsiger S, Schweizer A, Miyake J, Nagy L, Fürnstahl P (2018) Corrective osteotomies of phalangeal and metacarpal malunions using patient-specific guides: CT-based evaluation of the reduction accuracy. Hand 13(6):627–636
Rosskopf AB, Ramseier LE, Sutter R, Pfirrmann CWA, Buck FM (2014) Femoral and tibial torsion measurement in children and adolescents: comparison of 3D models based on low-dose biplanar radiography and low-dose CT. Am J Roentgenol 202(3):285–291
Illés T, Somoskeöy S (2012) The EOS imaging system and its uses in daily orthopaedic practice. Int Orthop 36(7):1325–1331
Acknowledgements
The technical and intellectual guidance of Mr. Walter Coudyzer (University hospitals Leuven, Belgium) during the design of this novel three-dimensional measurement method of femoral torsion using Siemens (Erlangen, Germany) MMWP InSpace®, and the statistical processing of Mr. Frederik De Keyzer with Analyse-it® (Leeds, LS3 1HS, United Kingdom) was greatly appreciated. Figures 2 and 3 are courtesy of the Department of Osteo-articular Radiology of the University Hospitals Leuven, Belgium.
Funding
There is no funding source.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Prof. Dr. Willem-Jan Metsemakers is a consultant for DepuySynthes. Dr. Austin Fragomen is a consultant for DepuySynthes, Smith Nephew, NuVasive, and Globus. Prof. Dr. Harm Hoekstra is a member of the lecture bureau of DepuySynthes. Furthermore, all authors hereby disclose any financial and personal relationships with other people or organisations that could inappropriately influence this work.
Ethical approval
Ethical approval was obtained from the Education-Support Committee of the Catholic University Leuven (KULeuven), Belgium.
Informed consent
Informed consent of all patients was obtained as for standard radiologic examinations.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vanhove, F., Noppe, N., Fragomen, A.T. et al. Standardization of torsional CT measurements of the lower limbs with threshold values for corrective osteotomy. Arch Orthop Trauma Surg 139, 795–805 (2019). https://doi.org/10.1007/s00402-019-03139-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-019-03139-1