
Abstract
Objective
A greater understanding of the lower limb geometry is necessary for the correction of lower limb torsional deformities. The purpose of our study was to measure the normal values of knee torsion using CT and to introduce the neck–malleolar angle as an alternative for measuring lower limb torsion.
Patients and Methods
We studied 77 consecutive CT studies performed from 2007 to 2009 in our clinic. In 67 cases, there was evidence of old trauma or surgical intervention to one limb, whereas the contralateral limb was healthy. The remaining 10 patients had no history of trauma or surgical intervention and were available for paired analysis in order to find the normal intraindividual variability. The whole limb, femoral and tibial torsion were measured according to the “Ulm method”. Finally, the knee joint rotational angle and the neck–malleolar angle (the angle between the femoral neck axis and the bimalleolar axis) were measured.
Results
The average knee joint rotation angle was 2.4 ± 6.4° while the neck–malleolar angle was 13.2 ± 10.2°. Right to left side differences in healthy paired limbs for total limb rotation, knee joint rotation and the neck–malleolar angle were 6.1 ± 4.1°, 3.9 ± 2.8° and 7.5 ± 4.3° respectively. The mean absolute rotational differences between injured and healthy limbs was 14.5 ± 10.1°, whereas the mean absolute neck–malleolar differences amounted to 12.5 ± 9.9° (p = 0.013) indicating that the knee compensates for torsional asymmetries.
Conclusions
The neck–malleolar angle takes into consideration the buffering effects of the knee joint in the transverse plane and contributes valuable additional information. Further studies including the long-term results of patients with torsional errors are important.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Rotational malalignment after intramedullary nailing for femoral or tibial shaft fractures is a well-known problem [1–3]. Braten et al. [1] described a 43% incidence for torsion errors of more than 10° following closed nailing of femoral fractures, whereas Puloski et al. [3] found an incidence of 22% for torsion errors of more than 10° after intramedullary nailing of tibial shaft fractures. Corrective osteotomies for lower limb rotational abnormalities are performed in most institutes when the limb torsional differences are greater than 15° [4–6].
Computed tomography represents the current gold standard for these measurements [7]. One of the most popular techniques for measuring femoral, tibial and limb torsion was described by Waidelich et al. as the “Ulm method” [8]. According to this method the lower limb torsion is calculated from the differences in the femoral and tibial torsions (internal rotation is shown by a minus sign). However, these measurements do not take into account the variability of knee joint rotation angle (femorotibial angle) which is the angle between the posterior tangent line of the femoral condyles and that of the proximal tibia). This observation might explain why many patients with torsional differences of the lower limb of more than 15° are asymptomatic [1].
The purpose of our study was to determine the average knee joint rotation angle in healthy limbs and to propose the use of a new angle (neck–malleolar angle) for the measurement of total lower limb torsion. Furthermore, we will try to answer the following questions:
-
1.
What right to left differences in the neck–malleolar angles are observed in a population with healthy paired limbs?
-
2.
Does knee torsion compensate for torsional differences in patients with one injured limb?
Patients and methods
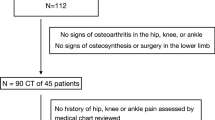
We studied 77 consecutive digital CT studies performed in our clinic from 2007 to 2009 to assess the torsional and length differences between both limbs. The patients were divided into two groups. The first group, which comprised 67 patients with evidence of old trauma or surgical intervention to one limb, was analysed to find the role of the knee joint in buffering torsional asymmetries. Thirty-seven of these patients had a history of a femoral fracture and 30 a history of a tibial fracture. All CT studies were performed for postoperative control after intramedullary nailing. In the second group, 10 patients with 20 healthy limbs were analysed to find the normal intra-individual differences. These CT studies were performed as a planning procedure before femoral or tibial lengthening. All healthy limbs of both groups were analysed to find the normal range of the femorotibial and neck–malleolar angles in a healthy population. Forty of the patients were male and 37 female. The mean age was 37 ± 16 (range, 16–77) years. The research was performed in accordance with the Declaration of Helsinki principles.
Technique of CT determination of the above angles
Scans were obtained with LightSpeed QX/I CT equipment (GE Healthcare, USA). The limbs were extended during examination and mounted on a footrest to stabilise the position during scans. Sections of 1.25-mm thickness were taken through the hip, knee and ankle joints with both limbs in the same positions.
All measurements were performed by qualified radiologists who were familiar with the assessment of the rotation profile of the lower extremities using the Ulm method [8]. The rotational profile was measured by defining four different angles measured each time between a defined axis and a horizontal line. These axes are the femoral neck axis, the femoral condylar axis, the axis of the proximal tibial condyles and the bimalleolar axis (Fig. 1). Internal torsion is assigned a minus (−) sign and external torsion a positive (+) sign. With the help of these four angles, the next step was to calculate the femoral neck anteversion angle, tibial torsion angle and total limb rotation angle (according to the Ulm method). The femoral neck anteversion is calculated by subtracting the femoral condylar angle from the femoral neck angle, the tibial torsion by subtracting the proximal tibial angle from the bimalleolar angle, while the total limb rotation is simply calculated by subtracting the femoral neck anteversion from the tibial torsion angle.

Measurement of a the femoral neck angle, b the femoral condyle angle, c the tibial condyle angle and d the malleolar angle
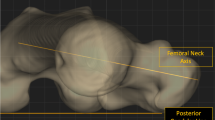
Our two new measured angles are the knee joint rotation angle and the neck–malleolar angle. The knee joint rotation angle is the angle between the femoral condylar axis and the proximal tibial axis while the neck–malleolar angle is between the femoral neck axis and the bimalleolar axis (Fig. 2). These angles are recorded for each patient and each limb.

Calculation of a the femoral torsion, b the tibial torsion, c the knee rotation and d the neck-malleolar angle
Statistical analysis
Average values, standard deviations as well as the range for all the measured angles were calculated for all limbs. Paired limbs were compared with each other to find side-to-side differences. We used the paired sample t test to detect statistically significant differences between our groups. A p value <0.05 (two-tailed) was considered to be statistically significant. All statistical analyses were performed using SPSS 15.0 (SPSS, Chicago, IL, USA). All values are presented in the form of mean ± SD (standard deviation).
Results
Femoral neck anteversion for all healthy limbs (87 limbs) was 17.8 ± 10.2°, tibial torsion was 28.5 ± 7.6° and total lower limb rotation was 10.8 ± 11.4°. The average knee joint rotation angle for all healthy limbs was 2.4 ± 6.4° while the neck–malleolar angle was 13.2 ± 10.2°. Angles falling beyond 2 standard deviations are considered to be abnormal. Right to left side differences for total limb rotation, knee joint rotation and neck–malleolar angle in the second group of patients were 6.1 ± 4.1°, 3.9 ± 2.8° and 7.5 ± 4.3° respectively. The mean absolute rotational difference between injured and healthy limbs in the first group of patients was 14.5 ± 10.1°, whereas the mean absolute neck–malleolar difference was 12.5 ± 9.9°. This difference was statistically significant (p = 0.013) indicating that the knee joint can compensate for torsional deformities. Tables 1, 2, 3 summarise our results.
Discussion
According to Paley, for the measurement of the frontal plane alignment, the mechanical axis deviation (MAD), hip–knee–ankle (HKA) angle, the mechanical lateral proximal femoral angle (mLPFA), the mechanical lateral distal femoral angle (mLDFA), mechanical proximal medial tibial angle (mMPTA), the mechanical lateral distal tibial angle (mLDTA) and the joint line convergence angle (JLCA) have to be calculated [9]. Similar to the JLCA, the knee torsion angle and the neck–malleolar angle take into account the role of the knee joint in the transverse plane alignment. Terminal degrees of knee extension are associated with obligatory external rotation of the tibia on the femur, which is caused partly by the differential radius between the medial femoral condyle and the smaller lateral femoral condyle. This automatic rotation is conventionally termed the screw home mechanism [10]. Furthermore, it is well known that internal and external rotation of the tibia on the femur is minimal at full extension (locking of the knee joint) and no significant rotation is apparent until after 10 to 20° of flexion [11].
Consequently, the magnitude of this rotational movement during knee extension is dependent on the individual anatomy of the femoral condyles. Moreover, if the lower extremities are fixed in comparable extended positions, the knee joint rotation angle should be nearly equal on both sides to fulfill the assumption that the bony anatomy is matched on both sides of the same individual. Taking into account all these considerations, it becomes apparent that the knee joint rotation angle is one part of the anatomical elements of the lower extremities' rotational profile. To include this angle in our measurements of the total lower limb rotation, we are proposing the use of the neck–malleolar angle, which is a direct measurement of the angle between the femoral neck axis and the bimalleolar axis. This angle gathers all three elements of total lower limb rotation: femoral neck anteversion, tibial torsion and knee joint rotation.
In our study, the lower limbs were fixed by a footboard on the table and the knees were extended to provide a reproducible position. The ranges of femoral neck anteversion, tibial torsion and total lower limb rotation of healthy individuals were comparable to the results of Waidelich and Strecker [8, 12]. The knee joint rotation angle for healthy limbs ranged from −22° to 14.8°, while the neck–malleolar angle from −15° to 48°. Comparing torsional differences measured by the Ulm and the neck–malleolar method in patients with unilateral fractures of the femur or tibia shaft, we found that although knee torsion in extension is mainly affected by the osseous anatomy, compensatory effects of the knee are evident in post-traumatic cases.
Takai et al. [13] were the first to measure the femorotibial angle with CT to find the torsional alignment of the lower limb in gonarthrosis. The torsion of the leg was measured as the inclination between the dorsal tangent to the femoral condyles and the line between the malleoli. Reikeras and Hoiseth [14] used the same method to measure the torsion of the leg in a normal adult population. However, there is a serious drawback to this methodology; the femoral torsion cannot be assessed without considering the femoral neck axis.
Yagi et al. [15] also measured knee joint rotation angles in patients with medial unicompartmental osteoarthritis and compared them with a control group of healthy individuals. They reported that there was no significant difference between the two groups and the range of the measured angle in the healthy individuals was 9° of internal rotation to 26° of external rotation.
The results of our study correlate highly with the findings of Waidelich and Strecker [8, 12] as far as the femoral, tibial and whole limb torsion are concerned. One important limitation in this study was the small number of patients with healthy paired limbs, which limits analysis for the intraindividual differences in the limb, femoral and tibial torsion angles. This also applies to differences of the neck–malleolar angles.
The neck–malleolar angle constitutes additional valuable information in the hands of orthopaedic surgeons. The average right to left side differences in healthy paired limbs for knee joint rotation and the neck–malleolar angle are 3.9 ± 2.8° and 7.5 ± 4.3° respectively. Moreover, we found that torsional differences in a population of patients with one injured limb could be compensated through the knee joint rotational angle. Consequently, not all abnormal limb torsion angles should be corrected. Further studies, including the long-term results of patients with torsional errors are necessary to find which angles best describe best the deformities that should be operatively corrected.
References
Braten M, Terjesen T, Rossvoll I. Torsional deformity after intramedullary nailing of femoral shaft fractures. Measurement of anteversion angles in 110 patients. J Bone Joint Surg Br. 1993;75:799–803.
Jaarsma RL, Pakvis DF, Verdonschot N, Biert J, van Kampen A. Rotational malalignment after intramedullary nailing of femoral fractures. J Orthop Trauma. 2004;18:403–9.
Puloski S, Romano C, Buckley R, Powell J. Rotational malalignment of the tibia following reamed intramedullary nail fixation. J Orthop Trauma. 2004;18:397–402.
Eckhoff DG. Effect of limb malrotation on malalignment and osteoarthritis. Orthop Clin North Am. 1994;25:405–14.
Turner MS. The association between tibial torsion and knee joint pathology. Clin Orthop Relat Res. 1994;(302):47–51.
Yagi T. Tibial torsion in patients with medial-type osteoarthrotic knees. Clin Orthop Relat Res. 1994;(302):52–6.
Tomczak RJ, Guenther KP, Rieber A, et al. MR imaging measurement of the femoral antetorsional angle as a new technique: comparison with CT in children and adults. AJR Am J Roentgenol. 1997;168:791–4.
Waidelich HA, Strecker W, Schneider E. Computed tomographic torsion-angle and length measurement of the lower extremity. The methods, normal values and radiation load. Rofo. 1992;157:245–51.
Paley D, Herzenberg JE, Tetsworth K, McKie J, Bhave A. Deformity planning for frontal and sagittal plane corrective osteotomies. Orthop Clin North Am. 1994;25:425–65.
Nagao N, Tachibana T, Mizuno K. The rotational angle in osteoarthritic knees. Int Orthop. 1998;22:282–7.
Simon S. Kinesiology in orthopaedic basic science, 2nd edition. Rosemont, IL: AAOS; 1994.
Strecker W, Keppler P, Gebhard F, Kinzl L. Length and torsion of the lower limb. J Bone Joint Surg Br. 1997;79:1019–23.
Takai S, Sakakida K, Yamashita F, Suzu F, Izuta F. Rotational alignment of the lower limb in osteoarthritis of the knee. Int Orthop. 1985;9:209–15.
Reikeras O, Hoiseth A. Torsion of the leg determined by computed tomography. Acta Orthop Scand. 1989;60:330–3.
Yagi T, Sasaki T. Tibial torsion in patients with medial-type osteoarthritic knee. Clin Orthop Relat Res. 1986:177–82.
Conflict of interest statement
There was no financial support for this study. None of the authors has received or will receive benefits for professional or personal use from a commercial party related directly or indirectly to the subject of this article. Each author certifies that he has no commercial associations (e.g. consultancies, stock ownership, equity interest etc.) that might pose a conflict of interest in connection with the submitted article.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was performed at the Medical School Hannover, Hannover, Germany
Rights and permissions
About this article
Cite this article
Liodakis, E., Aljuneidi, W., Krettek, C. et al. The neck–malleolar angle: an alternative method for measuring total lower limb torsion that considers the knee joint rotation angle. Skeletal Radiol 40, 617–621 (2011). https://doi.org/10.1007/s00256-010-1039-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-010-1039-5