
Abstract
Background
Complementary to clinical and experimental studies, computational cardiac modeling serves to obtain a comprehensive understanding of the cardiovascular system in order to analyze dysfunction, evaluate existing, and develop novel treatment strategies.
Objectives
We describe the basics of multiscale computational modeling of cardiac electrophysiology from the molecular ion channel to the whole body scale. By modeling cardiac ischemia, we illustrate how in silico experiments can contribute to our understanding of how the pathophysiological mechanisms translate into changes observed in diagnostic tools such as the electrocardiogram (ECG).
Materials and methods
Quantitative in silico modeling spans a wide range of scales from ion channel biophysics to ECG signals. For each of the scales, a set of mathematical equations describes electrophysiology in relation to the other scales. Integration of ischemia-induced changes is performed on the ion channel, single-cell, and tissue level. This approach allows us to study how effects simulated at molecular scales translate to changes in the ECG.
Results
Ischemia induces action potential shortening and conduction slowing. Hence, ischemic myocardium has distinct and significant effects on propagation and repolarization of excitation, depending on the intramural extent of the ischemic region. For transmural and subendocardial ischemic regions, ST segment elevation and depression, respectively, were observed, whereas intermediate ischemic regions were found to be electrically silent (NSTEMI).
Conclusions
In silico modeling contributes quantitative and mechanistic insight into fundamental ischemia-related arrhythmogenic mechanisms. In addition, computational modeling can help to translate experimental findings at the (sub-)cellular level to the organ and body context (e. g., ECG), thereby providing a thorough understanding of this routinely used diagnostic tool that may translate into optimized applications.
Zusammenfassung
Hintergrund
Das mechanistische Verständnis des Herz-Kreislauf-Systems ist von grundlegender Bedeutung, wenn man Fehlfunktionen verstehen, Behandlungsmöglichkeiten bewerten und neue Therapien entwickeln will. Die quantitative In-silico-Modellierung kann klinische und experimentelle Studien ergänzen.
Fragestellung
Wir beschreiben die Grundlagen einer computergestützten Multiskalenmodellierung der kardialen Elektrophysiologie und des Elektrokardiogramms (EKG) – von Ionenkanälen auf molekularer Ebene bis hin zur Ebene des Gesamtorganismus. Am Beispiel der Modellierung der kardialen Ischämie veranschaulichen wir, wie In-silico-Experimente zum Verständnis der Zusammenhänge zwischen fundamentalen pathophysiologischen Mechanismen und Diagnosewerkzeugen wie dem EKG beitragen können.
Material und Methoden
Die numerische Herzmodellierung integriert viele zeitlich-räumliche Skalen: Von der Ionenkanalbiophysik bis hin zu EKG-Signalen. Für jede der Skalen beschreiben mathematische Gleichungen die elektrophysiologische Funktion in Beziehung zu den anderen Skalen. Die Integration von ischämieinduzierten Veränderungen erfolgt auf Ionenkanal‑, Einzelzell- und Gewebeebene. Mit diesem Ansatz lässt sich untersuchen, wie sich aus simulierten Effekten auf molekularer Ebene Änderungen im simulierten EKG ergeben.
Ergebnisse
Aufgrund der Verkürzung des Aktionspotenzials und der Leitungsverlangsamung haben ischämische Bereiche unterschiedlicher transmuraler Ausdehnung einen deutlichen Effekt auf die Erregungsausbreitung und die Repolarisation. Eine ST-Segment-Hebung bzw. -Senkung zeigte sich für transmurale bzw. subendokardiale ischämische Regionen. Ischämische Regionen mittlerer Ausdehnung waren elektrisch unauffällig (NSTEMI).
Schlussfolgerung
Die In-silico-Modellierung kann quantitative und mechanistische Erkenntnisse zu fundamentalen ischämiebezogenen arrhythmogenen Mechanismen liefern. Darüber hinaus erlaubt die computergestützte Modellierung, experimentelle Ergebnisse von der (sub-)zellulären Ebene auf die Organ- und EKG-Ebene zu übertragen. Somit trägt sie zu einem tieferen Verständnis des routinemäßig eingesetzten EKGs und zu einer Optimierung dieses Werkzeugs bei.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over the past decades, computational modeling has emerged as a research method in the field of cardiac electrophysiology, complementary to classical experimental approaches including animal experiments and clinical studies. Modeling can span multiple spatiotemporal scales and bridge levels of integration. Moreover, hypotheses can be tested quantitatively under perfectly controlled conditions. In this review article, we acquaint the reader with the basic concepts of multiscale modeling of cardiac electrophysiology and present its application through the example of acute cardiac ischemia.
Multiscale modeling of cardiac electrophysiology
Mathematical representations of the heart spanning multiple spatiotemporal scales and levels of integration provide means to gain mechanistic insight into clinically relevant phenomena. Such in silico models have the advantage of providing a controlled environment allowing one to study how changes of certain parameters affect the overall system quantitatively, while causing no harm to patients or animals. In this way, computational models can help to identify and characterize basic physiological mechanisms, to improve diagnosis and therapy, and to design and refine in vitro and in vivo experiments. While models build on basic and well-established principles of physics like conservation of energy or the propagation of fields, there are always a number of parameters that need to be defined before using a model. On the one hand, this gives the opportunity to tailor computational models to specific phenotypes (e. g., diseases like atrial fibrillation or acute ischemia). On the other hand, computational models need to be appropriately constrained using adequate data from other experimental platforms.
In the case of cardiac electrophysiology, the smallest physiological structure being considered are often single ion channels of the cell membrane. Their kinetics, i. e., the opening and closing of the gates controlling ionic current flow through the channels, are mostly described using so-called ordinary differential equations (ODEs, Fig. 1a). An ODE is a type of equation that describes a variable (e. g., the open probability of a gate) in terms of its derivatives (i. e., the rate of change, in this case, the rate of opening or closing). The derivative (rate) can depend on other parameters, such as ion concentrations or transmembrane voltage (Vm). Solving an ODE describing the rate of change of a variable yields a description of the behavior of that variable itself over time, i. e., the time course of this variable. Ion channel models can take into account modifications by genetic mutations, drugs, or altered experimental conditions such as acute ischemia.

Hierarchy of multiscale cardiac electrophysiology models ranging from ion channels (a) via integrated cell models (b) and tissue level models (c) to the body surface and electrocardiogram (d)
Electrophysiological models consider the various ion channels present in the membrane of cardiac myocytes. All ion channels are coupled via Vm and the dynamically changing ion concentrations in different spatial domains (i. e., extracellular, intracellular, and several subcellular compartments like the sarcoplasmic reticulum). They are represented by a system of coupled ODEs (Fig. 1b). Such single-cell models yield action potentials (AP) upon stimulation and can be adjusted to represent different cell states, e. g., disease-induced remodeling.
As cardiac myocytes form a functional syncytium, excitation propagates through cardiac tissue, causing spatiotemporal changes in Vm. The coupling between neighboring cells can mathematically be represented in a so-called reaction-diffusion system by using tissue level simulations. Such a system is described with so-called partial differential equations (PDEs, Fig. 1c). While the (channel-level) ODEs include time dependency, the PDEs additionally incorporate a spatial component. The reaction part describes how a cell experiencing an influence by its neighbors responds with an AP. The diffusion part describes how the excitation of one cell spreads to neighboring cells, which in turn react themselves. Such a reaction-diffusion system allows calculating, for instance, the propagation of an activation wavefront. By representing conduction barriers and specific anatomy in such tissue models, it is possible to include for example various levels of fibrosis and thereby enable personalization of computational models.
Finally, the local differences of Vm throughout the heart cause currents that represent the source of an electric field extending into the torso and up to the body surface. The field distribution is described by Poisson’s equation and depicts the body surface potentials and, thus, allows recording virtual ECGs from these models (Fig. 1d).
Cellular level
The AP of a cardiac myocyte is triggered by a stimulus causing the opening of sodium channels. The inflow of sodium ions depolarizes the cell to positive voltages of around +40 mV. The following plateau phase of the AP is due to a balanced flow of potassium and calcium currents. Eventually, potassium currents dominate and repolarize the cardiac myocyte back to the resting Vm of around −80 mV. The human ventricular AP lasts about 300–400 ms.
During cardiac ischemia, this behavior changes depending on the time after initiation of the insult. The different experimentally identified phases of ischemia which are considered here are: phase 1a (after 5 min) and phase 1b (between 20 and 30 min) [2]. In phase 1a, mainly three effects can be observed: hyperkalemia, acidosis, and hypoxia. These, in turn, cause a reduction of the AP amplitude and AP duration while the resting Vm is increased (less negative) [25]. Phase 1a is often subclassified as stage 1 (5 to 7 min) and stage 2 (10 to 12 min). Phase 1b is characterized by additional cellular uncoupling causing a decrease in intercellular conductance. Also, the extracellular potassium concentration ([K+]o) and the intracellular calcium concentration ([Ca2+]i) increase, favoring initiation of arrhythmias [2].
Single-cell modeling
The seminal work by Hodgkin and Huxley provided the first mathematical reconstruction of the electrophysiological behavior of cells by modelling the AP of a neuron [10]. In principle, they describe the cell as an electric network (Fig. 1b). Charges are separated by the cellular membrane, which is thus modelled as a capacitor. Currents can flow through ion channels, which are described as conductances (or conversely as resistors). The different reversal potentials for different channels are taken into account by connecting batteries in series with the conductances. The conductances and reversal potentials are not constant over time but depend on the ion concentrations and ODEs describing the channel gating.
Based on the neuronal work of Hodgkin and Huxley and on early cardiac models of Purkinje cells by Noble, more specific models have been developed for cardiac myocytes of several species [6]. These include additional coupled ODEs describing various channels, exchangers, pumps, and other processes that influence intracellular ion concentrations. For the different ion channels, the current Ix (where X can stand for any given channel type, e. g., INa, IK1) depends on the respective maximal channel conductance gx, the reversal potential, Vm, and on so-called gating variables po (Fig. 1a). Gating variables are formulated as ODEs defining their rate of change, for instance of the form
Here, \(\alpha _{p_{o}}\) and \(\beta _{p_{o}}\)are rate constants describing the transition from a closed to an open state and vice versa [6]. These gates describe the biophysical processes of activation and inactivation of ion channels. The rate constants may depend on Vm or ion concentrations. The membrane is still modelled as a capacitance that separates charges between the intra- and extracellular space. Mathematically, that results in the equation
describing the change of Vm over time, dependent on the membrane capacitance Cm, a stimulus current Istim, and the currents through all transmembrane ion channels, pumps and exchangers that are summed up in Iion. Thus, Iion is the sum of several currents Ix, including any given channel/exchanger/pump type (e. g., INa, IK1, INa/K). Repetitively solving (2) and thus, mathematically speaking, integrating Vm over time, yields an AP which presents the time course of Vm.
Specific human ventricular in silico AP models have been developed. One prominent example is the model by ten Tusscher and Panfilov [24]. This model includes a refined representation of intracellular calcium handling and electrophysiological heterogeneity across the ventricular wall (subepicardial, mid-myocardial, and subendocardial variants of the cell model).
Example: ischemia
The ten Tusscher and Panfilov model [24] can serve as a basis to numerically represent the effects of ischemia on human ventricular electrophysiology [25, 27]. At the different phases of ischemia, hyperkalemia, acidosis, and hypoxia influence different parameters in the model [27]. The model also contains an ATP-sensitive channel (IK,ATP) [25, 27] to incorporate further hypoxia effects.
In addition to the temporal phases, spatial differences in ion channel activity are considered. For example, IK,ATP varies from subendo- to subepicardium [25]. The occlusion of a vessel has a regional effect on the cells. Oxygen-deprived cells, located in the central ischemic zone (CIZ), are affected by the complete set of ischemic changes. Other cells which are still sufficiently perfused by normal or collateral vessels are not affected at all (normal zone, NZ). In-between lies the border zone (BZ) with distinct transitions of hyperkalemia, acidosis, and hypoxia (illustrated in inset of Fig. 2b). As an example, the APs of subepicardial cells in the CIZ at different temporal ischemia phases are illustrated in Fig. 2a. The AP duration (APD) at 90% repolarization is shortened from 309 ms (control), to 116 ms (phase 1a, stage 1), 72 ms (phase 1a, stage 2), and 56 ms (phase 1b). Similarly, the resting Vm becomes less negative: −85 mV (control), −74 mV (phase 1a, stage 1), −64 mV (phase 1a, stage 2), and −58 mV (phase 1b).

Temporally and regionally resolved effects of ischemia. Action potentials (AP) of subepicardial myocytes at different temporal stages of ischemia (a). Examples of ischemic regions with varying transmural extent due to occlusion of the left anterior descending coronary artery and the related levels of hyperkalemia, acidosis, and hypoxia (b). (Images reproduced with permission from [27] (a) and [28] (b))
Tissue level
The cardiomyocytes in the ventricular wall are surrounded by extracellular components and are electrically coupled by gap junctions. The Vm difference between neighboring cells induces a current through the gap junctions and the extracellular space, allowing excitation to spread. Gap junction density is highest at the short ends of myocytes. That makes cell-to-cell conduction about 10 times stronger along the long axis of myocytes than perpendicular to them. The ratio of longitudinal to transversal conductivity is called anisotropy ratio. Extracellular conduction is also stronger along myocytes than perpendicular to them, although less pronounced than for intracellular conduction. Therefore, conduction velocity (CV) is faster along the long axis of cells than perpendicular to them.
The ventricular myocardium is electrically activated by the Purkinje system causing excitation propagation from apex to base and from endo- to epicardium. Due to intrinsic electrical heterogeneities (apico-basal, transmural, and interventricular), the APD distribution is not homogeneous in the ventricles and the repolarization follows a specific sequence generating the concordant T‑wave in the ECG [12].
Both depolarization and repolarization are affected by ischemia. As stated above, temporal and regional effects are seen depending on the time after occlusion and the occlusion site. The longer ischemia lasts, the more severe are the effects (Fig. 2a). Moreover, a distal occlusion will influence mostly the endocardial side of the ventricular wall, while a proximal occlusion would lead to a fully transmural ischemia. Therefore, the central ischemic zone and the border zone will vary in size and position, leading to spatial differences in APD during ischemia. In addition, the higher ATP sensitivity of IK,ATP towards the epicardium further contributes to APD gradients.
Tissue modeling
The basic idea of tissue modelling is to assemble the electric network representations of several cells by intra- and extracellularly coupling of the individual cells. However, doing so for every cell in the heart (or just a region of interest) would result in a huge electrical network. Commonly, excitation spread is therefore modeled with macroscopic approaches describing the tissue as a continuum. Thereby, one computational node (one instance of an electric network representation of a cell) represents multiple myocytes. We create virtual geometries of a heart (or a piece of tissue) and can place the nodes in distances in the order of 0.1 to 0.5 mm. At every node, the electrical properties representative for the myocytes in the vicinity can be recorded, i. e., an AP as well as the ion channel dynamics.
Tissue models also have to consider the currents between neighboring nodes that are caused by locally differing Vm. The so-called bidomain model does that by electrically connecting the intra- and extracellular ends of each node to the respective ends of every neighboring node. These electrical connections include a conductance that considers the myocyte orientation (i. e., an intracellular conductance along myocyte direction could be 10 times that of a perpendicular conductance). The bidomain model can be described by two PDEs. A very common simplification, known as the monodomain model, is to assume equal anisotropy ratios for the intra- and extracellular space. In that case, the model reduces to just one PDE [3]:
where \(\nabla\) is a spatial derivative operator (producing larger values where the difference between neighboring nodes is larger), \(\upsigma \,\)is the so-called anisotropic conductivity tensor (a mathematical object describing the tissue conductivity in longitudinal and transversal direction), and \(\upbeta \,\)is the cell surface-to-volume ratio. Like in the single-cell models, \(\frac{\mathrm{d}V_{m}}{\text{dt}}\) describes the temporal rate of change of Vm. This PDE represents a reaction-diffusion system and thereby enables the calculation of the propagation of excitation. Numerical aspects of this equation and appropriate schemes to solve it can be found elsewhere [3].
To simulate a realistic propagation, a cardiac geometry, e. g., derived from medical imaging systems, and a description of myocyte orientation in combination with the conductivity of the tissue is needed. Most tissue models do not include the Purkinje network, but instead emulate it by using a stimulation protocol, where Purkinje-muscle junctions are electrically stimulated at fixed time points [11].
Example: ischemia
In the in silico ischemia cases presented here, the anatomical model of the ventricles was derived from magnetic resonance (MR) images of a healthy volunteer. The myocyte orientation was modeled using a rule-based method [12]. Both activation sequence and physiological heterogeneity were set based on [12]. In most of the work, an occlusion of the left anterior descending coronary artery was modeled using ellipsoidal regions of varying transmural extent (subendocardial region as smallest to transmural region as largest ischemic region).
Overall excitation outside the central ischemic zone and the border zone was not significantly influenced by the ischemia. Depending on the transmural extent and the time after occlusion, the CV in the ischemic region was reduced. Due to the shorter APD in the ischemic region, the cells in it start to repolarize first, leading to a Vm gradient across the wall (being responsible for the so-called injury current). This is shown for different phases and transmural extent in Fig. 3 for a time point 200 ms after initiation of excitation.

Vm distribution of different ischemia setups at t = 200 ms. The transmural extent of the ischemic region and the stage of ischemia were varied. (Image reproduced with permission from [27])
Electrocardiogram
Depolarization and repolarization of cardiac tissue are reflected in electric body surface potentials as described by the bidomain theory. By recording the time course of these body surface potentials at defined electrode positions, an electrocardiogram (ECG) is obtained. Activation of the ventricles, i. e., depolarization, leads to the QRS complex of the ECG. During the AP plateau, all myocytes in healthy ventricles are at almost the same Vm, i. e., the spatial gradient is very small, yielding an almost isoelectrical ST-segment. After the ST-segment, the T‑wave reflects repolarization of the ventricular myocytes.
To diagnose acute myocardial ischemia, depression or elevation of the ST-segment of the ECG are important indications depending on the location of the ischemic region within the heart and its transmural extent. In the physiological case, almost no spatial differences of Vm exist shortly after the activation of the ventricles due to the plateau phase of the AP (isoelectric ST segment). However, the ischemia-induced changes of the AP discussed above give rise to injury currents flowing between healthy and ischemic tissue during the plateau phase of the AP [7]. These currents are the source of the electrical field reflected in the non-isopotential ST-segment. However, not all cases of ischemia cause changes in the ECG, which is reflected by the categorization into ST-elevation (STEMI) and non-ST-elevation myocardial infarction (NSTEMI), the latter also being known as electrically silent. Computational modeling can help to elucidate the fundamental principles causing ST elevation and depression, to identify the reasons for electrically silent ischemia, and to optimize the diagnostic potential of the ECG as detailed below.
Electrocardiogram modeling
The challenge to derive a body surface ECG from a given spatiotemporal distribution of Vm is known as the forward problem of electrocardiography. The spatial gradient of Vm at each time point impresses a current density on the tissue as described by the bidomain theory ([12]; Fig. 1d). The result is a PDE similar to the tissue model presented above:
Thus, the extracellular potentials \(\Phi _{e}\)in the whole torso including the body surface can be computed based on the macroscopic intra- and extracellular conductivities \(\sigma _{i}\) and \(\sigma _{e}\), and the Vm distribution in the heart. By tracing the potential difference between electrodes on the virtual body surface over time, a virtual ECG is obtained.
Example: ischemia
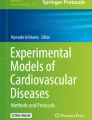
The ischemia-induced changes of the AP and the excitation propagation alter the spatial distribution of Vm during the cardiac cycle and therefore also affect the ECG. Based on experimental findings and the in silico results described above, we investigated where these changes stem from and how different locations and transmural extents affect them. When ischemia is restricted to the subendocardial layer of the ventricular wall, a small transmural Vm gradient causes ST-segment depression in leads close to the ischemic region [26]. If ischemia persists and the region extends transmurally, this gradient turns in opposite direction leading to ST segment elevation [26]. With intermediate transmural ischemic extension, these effects balance and cause electrically silent ischemia (Fig. 4a, c; [28]). In a case study of such an electrically silent ischemia, Potyagaylo et al. [19] demonstrated that the simulated magnetocardiogram (MCG) did not show any changes of the ST-segment either (like in the non-ischemic control case either), suggesting that electrically silent ischemia is also magnetically silent.

Electrocardiogram lead V4 for ischemia of varying transmural extent in stage 2 (a) and varying duration of a transmural ischemia (b). Ventricular Vm and body surface \(\Phi _{e}\)distribution during the action potential plateau (t = 200 ms) for ischemia of varying transmural extent in stage 2 (c). (Images reproduced with permission from [26] (a, b), and [27] (c))
In computational models, it was shown that duration of ischemia not only influences the transmural extent of ischemia but also affects the resulting ECG. Wilhelms et al. [26] investigated the three temporal phases within the first 30 min after the occlusion described above and observed distinct characteristics in the ECG (Fig. 4b). After 30 min, almost no excitation was initiated in the CIZ. In transmural ischemia, the difference between subendocardial and subepicardial ischemic tissue decreases during phase 1b compared to earlier stages. Consequently, ST segment elevation attenuates after 20–30 min showing that besides the transmural extent of the ischemic region, also the temporal stage of ischemia affects the ECG and the direction of the ST segment shift.
In a large computational study comprising 765 stage 2 ischemia scenarios of different location, size, and width of the BZ, and using different anatomical models, we showed that the larger the ischemic region and the smaller the BZ, the easier is its detection by ECG changes. Assuming realistic noise conditions, a sensitivity of 57% was observed considering all ischemic setups, in contrast to 71 and 86% when only considering ischemic regions with a radius greater than 5 and 10 mm, respectively [14]. Moreover, the sensitivity showed considerable interindividual variability ranging from 41–71% for the three anatomical models included [14].
As the ECG-based diagnosis of ischemia is mostly based on the standard 12-lead ECG, it could potentially be improved by considering additional electrode locations. In [15], different lead systems were analyzed and optimized. The 12-lead ECG performed better (64.2 ± 24.9% detection rate) than a 3-lead system (41.4 ± 11.8%). In contrast, adding right-sided Wilson leads had negligible effect. Considering optimally placed additional electrodes increased the detection rate by only 2–3% depending on the desired specificity suggesting that the added value of additional ECG electrode locations is limited. However, an alternative feature of ST-segment deviation was proposed based on the in silico results, i. e., the K‑point which is defined as the baseline deviation at the minimum of the ST-segment envelope signal. Using the K‑point as a parameter for ischemia detection increased specificity by 7–10% compared to standard features.
Further aspects of modeling acute ischemia
Beyond the methods used in the examples presented above, computational modelling has further applications in investigating cardiac ischemia, from its underlying mechanisms to its effects on the heart. On the microscopic level, for instance, it can be used to investigate the effects of ischemia on tissue conductivity. To do this, three-dimensional models of blocks of tissue containing several connected cardiac myocytes are created (e. g., based on image data). In simulations, the blocks are subjected to an electric field as if each block were between two electrodes. The tissue block models can be altered according to the effects of acute ischemia, including collapse of the interstitial space, cell swelling, closure of gap junctions, and fibrosis. Subjecting these altered blocks to the same electric field results in changes of the overall tissue conductivity that can be used to adapt the conductivity tensors \(\sigma\) from Eq. 3 for tissue-level simulations of ischemia [21, 23].
Other computational works focus on the secondary effects of ischemia, such as arrhythmogeneity. Here, computational models can be used to investigate hypotheses on how ventricular arrhythmias are facilitated by ischemic regions [5]. Computational tissue simulations also allow easy recording of arrhythmia-associated parameters such as APDs, refractoriness, and CV [4]. Tissue models can even be used in patient-specific simulations, where the computational model is derived from image data (e. g., MR) and can include ischemic regions. That allows to conduct patient-specific simulations of ventricular tachycardia (VT) for risk stratification [9].
Computational modeling can also help to link experimental animal studies (e. g., in rabbits) to the human scenario by comparing computational models of the animal and the human heart [20]. Animal computational models are also used to study initiation and maintenance of VT, and the mechanisms of defibrillation [1]. An emerging technique employs so-called model populations, a number of models where parameters vary slightly within (patho-)physiological ranges. Model populations allow considering interindividual and physiological variability, but can also be adapted to pathological conditions. Not all combinations of parameters lead to a physiological AP. However, it was found that under ischemic conditions, more of the slightly varied models produce an AP that can be considered valid. That may be implying that physiological variability plays a role in the alterations of electrophysiological properties that are seen during acute ischemia [8].
Naturally, mechanical effects play an important role in many aspects of cardiac physiology. Accordingly, computational models can include mechanical components, such as mechanosensitive channels. This way, computer simulations were, for instance, used to mechanistically study the precordial thump and its efficacy in terminating VT [13].
In light of studies showing electrotonic coupling between cardiac myocytes and nonmyocytes (e. g., fibroblasts), computational modeling has been used to investigate the effects of these heterocellular interactions. For this purpose, cellular models of cardiac myocytes can be coupled electrically to similar models of fibroblasts or other cells. This way, it was, for instance, suggested that fibroblast–myocyte coupling can alter repolarization behavior and [Ca]i alternans, which are linked to arrhythmogenesis in ischemic hearts [29, 30]. Similarly, a model of human mesenchymal stem cells (hMSCs) was developed to investigate their therapeutic potential for ischemic hearts. Coupling between hMSC and cardiac myocytes was suggested to have an impact on contractility and arrhythmogenic potential [16, 17].
Computational modeling of ischemia also has applications beyond electrophysiology and electromechanics: for instance, computational models were used to characterize metabolite responses to ischemia in order to investigate intervention strategies to change the outcome of reperfusion [18]. Blood flow can also be simulated based on mathematical equations. Such models have been demonstrated to be able to identify cases of ischemia from cardiac computed tomography angiography derived images [22].
Conclusion
In this focus article, we presented multiscale computational modeling as a valuable research approach in cardiac electrophysiology complementary to classical experiments. We illustrated the method by applying it to acute myocardial ischemia and showed how it has successfully been applied to bridge the gap between different levels of integration by translating experimental findings on the cell membrane level to the organ and body (ECG) context. This was done to elucidate fundamental ischemia-related arrhythmogenic mechanisms, to foster our understanding of routinely used diagnostic tools, and to suggest optimizations of these tools. We highlighted the advantages (perfectly controlled conditions, single parameter manipulations, ethical and financial cost, feasibility of experiments, comprehensive sensitivity analyses) and limitations (input data to constrain models, validation) and believe that a tight interplay between in silico, in vitro, and in vivo experiments brings about great opportunities. We hope that we have convinced the reader to view computational modeling of cardiac electrophysiology as an extension to conceptual modelling that is involved in all data interpretation and hypothesis formation. Computational modeling is complementary to classical experimental settings and we encourage the reader to consider this approach in their own research for providing quantitative and mechanistic insight.
References
Arevalo HJ, Boyle PM, Trayanova NA (2016) Computational rabbit models to investigate the initiation, perpetuation, and termination of ventricular arrhythmia. Prog Biophys Mol Biol 121:185–194
Carmeliet E (1999) Cardiac ionic currents and acute ischemia: from channels to arrhythmias. Physiol Rev 79:917–1017
Clayton RH, Bernus O, Cherry EM et al (2011) Models of cardiac tissue electrophysiology: progress, challenges and open questions. Prog Biophys Mol Biol 104:22–48
Dutta S, Mincholé A, Quinn TA, Rodriguez B (2017) Electrophysiological properties of computational human ventricular cell action potential models under acute ischemic conditions. Prog Biophys Mol Biol 129:40–52. https://doi.org/10.1016/j.pbiomolbio.2017.02.007
Dutta S, Mincholé A, Zacur E et al (2016) Early afterdepolarizations promote transmural reentry in ischemic human ventricles with reduced repolarization reserve. Prog Biophys Mol Biol 120:236–248
Fink M, Niederer SA, Cherry EM et al (2011) Cardiac cell modelling: observations from the heart of the cardiac physiome project. Prog Biophys Mol Biol 104:2–21
Foster DB (2007) Twelve-lead electrocardiography: theory and interpretation. Springer, Berlin
Gemmell P, Burrage K, Rodríguez B, Quinn TA (2016) Rabbit-specific computational modelling of ventricular cell electrophysiology: using populations of models to explore variability in the response to ischemia. Prog Biophys Mol Biol 121:169–184
Hanna G, Trayanova N, Graham, Ukwatta E (2016) Evaluation of a T1 mapping technique for stratifying patient risk: A preliminary study using computer simulations of cardiac electrophysiology. In: 2016 IEEE EMBS Int. Student Conf. IEEE, S 1–4
Hodgkin AL, Huxley AF (1952) A quantitative description of membrane current and its application to conduction and excitation in nerve. Bull Math Biol 117:500–544
Kahlmann W, Poremba E, Potyagaylo D et al (2017) Modelling of patient-specific Purkinje activation based on measured ECGs. Curr Dir Biomed Eng 3:171
Keller DUJ, Weiss DL, Dössel O, Seemann G (2012) Influence of IKs heterogeneities on the genesis of the T‑wave: a computational evaluation. IEEE Trans Biomed Eng 59:311–322
Li W, Kohl P, Trayanova N (2006) Myocardial ischemia lowers precordial thump efficacy: an inquiry into mechanisms using three-dimensional simulations. Heart Rhythm 3:179–186
Loewe A, Schulze WHW, Jiang Y et al (2011) Determination of optimal electrode positions of a wearable ECG monitoring system for detection of myocardial ischemia: A simulation study. Comput Cardiol (2010) 38:741–744
Loewe A, Schulze WHW, Jiang Y et al (2014) ECG-based detection of early myocardial ischemia in a computational model: impact of additional electrodes, optimal placement, and a new feature for ST deviation. Biomed Res Int 530352:1–11
Mayourian J, Cashman TJ, Ceholski DK et al (2017) Experimental and computational insight into human mesenchymal stem cell paracrine signaling and heterocellular coupling effects on cardiac contractility and arrhythmogenicity. Circ Res 121:411–423
Mayourian J, Savizky RM, Sobie EA, Costa KD (2016) Modeling electrophysiological coupling and fusion between human mesenchymal stem cells and cardiomyocytes. Plos Comput Biol 12:e1005014
McDougal AD, Dewey CF (2017) Modeling oxygen requirements in ischemic cardiomyocytes. J Biol Chem 292:11760–11776
Potyagaylo D, Seemann G, Schulze WH, Dossel O (2015) Magnetocardiography did not uncover electrically silent ischemia in an in-silico study case. 2015 Comput. Cardiol. Conf. IEEE, pp 1145–1148
Quinn TA, Kohl P (2013) Combining wet and dry research: experience with model development for cardiac mechano-electric structure-function studies. Cardiovasc Res 97:601–611
Schwab BC, Seemann G, Lasher RA et al (2013) Quantitative analysis of cardiac tissue including fibroblasts using three-dimensional confocal microscopy and image reconstruction: towards a basis for electrophysiological modeling. IEEE Trans Med Imaging 32:862–872
Siogkas PK, Rigas G, Exarchos TP et al (2017) Computational estimation of the hemodynamic significance of coronary stenoses in arterial branches deriving from CCTA: A proof-of-concept study. Eng. Med. Biol. Soc. IEEE, pp 1348–1351
Stinstra JG, Shome S, Hopenfeld B, MacLeod RS (2005) Modelling passive cardiac conductivity during ischaemia. Med Biol Eng Comput 43:776–782
ten Tusscher KHWJ, Panfilov AV (2006) Alternans and spiral breakup in a human ventricular tissue model. Am J Physiol Heart Circ Physiol 291:H1088–H1100
Weiss DL, Ifland M, Sachse FB et al (2009) Modeling of cardiac ischemia in human myocytes and tissue including spatiotemporal electrophysiological variations. Biomed Tech (Berl) 54:107–125
Wilhelms M, Dössel O, Seemann G (2010) Simulating the impact of the transmural extent of acute ischemia on the electrocardiogram. Comput Cardiol (2010) 37:13–16
Wilhelms M, Dössel O, Seemann G (2011) Comparing simulated electrocardiograms of different stages of acute cardiac ischemia. Lect Notes Comput Sci, vol. 6666., pp 11–19
Wilhelms M, Dössel O, Seemann G (2011) In silico investigation of electrically silent acute cardiac ischemia in the human ventricles. IEEE Trans Biomed Eng 58:2961–2964
Xie Y, Garfinkel A, Camelliti P et al (2009) Effects of fibroblast-myocyte coupling on cardiac conduction and vulnerability to reentry: a computational study. Heart Rhythm 6:1641–1649
Xie Y, Garfinkel A, Weiss JN, Qu Z (2009) Cardiac alternans induced by fibroblast-myocyte coupling: mechanistic insights from computational models. Am J Physiol Heart Circ Physiol 297:H775–H784
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Loewe, E.M. Wülfers and G. Seemann declare that they have no competing interests.
This article does not contain any studies with human participants or animals performed by any of the authors. The ethical guidelines of the studies cited are provided within those studies.
Rights and permissions
About this article

Cite this article
Loewe, A., Wülfers, E.M. & Seemann, G. Cardiac ischemia—insights from computational models. Herzschr Elektrophys 29, 48–56 (2018). https://doi.org/10.1007/s00399-017-0539-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00399-017-0539-6