
Abstract
Cardiac fibrosis caused by adverse cardiac remodeling following myocardial infarction can eventually lead to heart failure. Although the role of soluble factors such as TGF-β is well studied in cardiac fibrosis following myocardial injury, the physiological role of mechanotransduction is not fully understood. Here, we investigated the molecular mechanism and functional role of TRPV4 mechanotransduction in cardiac fibrosis. TRPV4KO mice, 8 weeks following myocardial infarction (MI), exhibited preserved cardiac function compared to WT mice. Histological analysis demonstrated reduced cardiac fibrosis in TRPV4KO mice. We found that WT CF exhibited hypotonicity-induced calcium influx and extracellular matrix (ECM)-stiffness-dependent differentiation in response to TGF-β1. In contrast, TRPV4KO CF did not display hypotonicity-induced calcium influx and failed to differentiate on high-stiffness ECM gels even in the presence of saturating amounts of TGF-β1. Mechanistically, TRPV4 mediated cardiac fibrotic gene promoter activity and fibroblast differentiation through the activation of the Rho/Rho kinase pathway and the mechanosensitive transcription factor MRTF-A. Our findings suggest that genetic deletion of TRPV4 channels protects heart from adverse cardiac remodeling following MI by modulating Rho/MRTF-A pathway-mediated cardiac fibroblast differentiation and cardiac fibrosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coronary heart disease (CHD) is the leading cause of death in the USA [7]. Multiple stimuli including hypertension, smoking, aortic stenosis, myocardial infarction and stress alter the biochemical and mechanical properties of the myocardium, leading to pathological remodeling which results in heart failure [4, 9, 11, 24, 30, 41, 42, 44]. Adaptation of the heart after injury is critical for maintaining long-term cardiac function in the surviving patients. Therefore, the clinical management of cardiac fibrosis after injury such as MI presents a major challenge [4, 6, 18, 33, 36, 44]. After cardiac injury, myocardium undergoes remodeling process which frequently exhibits adverse effects like excessive extracellular matrix (ECM) deposition, resulting in compromised heart function [12, 28, 41, 48].
Cardiac fibroblasts (CF) are critical for maintaining the structural integrity of the myocardium by balancing ECM turn over. Cardiac injury or insult triggers cardiac fibroblast differentiation into hypersecretory and hyper-contractile myofibroblasts (MF). However, persistent activation of MF increases ECM synthesis that can eventually lead to pathological fibrosis [26, 31, 61]. CF differentiation requires integration of both biochemical and mechanical signaling pathways [17, 39, 49]. Although signaling produced by soluble factors has been studied extensively, the sensing and biochemical transduction mechanisms that integrate soluble and mechanical signaling during CF differentiation are not well understood.
We have recently, for the first time, shown that mechanosensitive ion channel transient receptor potential vanilloid 4 (TRPV4) mediates rat cardiac fibroblast (rCF) differentiation via integration of soluble and mechanical signaling in vitro [3]. In fact, TRPV4 was identified as a mechanosensor of osmotic cell swelling [38, 53], matrix viscoelasticity in mesenchymal stem cells [37], flow-induced shear stress in endothelial [23, 32, 46] and renal collecting duct cells [8]. We have previously demonstrated that TRPV4 is a mechanosensor of cyclic stretch and ECM stiffness in endothelial cells and negatively regulates tumor angiogenesis in vivo [2, 10, 29, 54,55,56]. However, the pathophysiological role of TRPV4 and TRPV4-dependent mechanotransduction mechanism(s) in myocardial adaptation (cardiac remodeling) in response to injury/insult is not known. In the present study, we investigated the physiological role of TRPV4 in cardiac remodeling following MI and dissected the molecular mechanisms responsible for its role in CF differentiation.
Material and methods
Materials
GSK1016790A (GSK), EDA fibronectin (EDA-FN) and alpha-smooth muscle actin (α-SMA; A2547) antibodies were purchased from Sigma-Aldrich (St. Louis, MO, USA); lipofectamine 2000, Fluo-4 AM, Fura-2 AM and Alexa-conjugated secondary antibodies were purchased from Invitrogen (Carlsbad, CA, USA). AB159908 (AB1) was obtained from ABCR GmbH (Germany). TGF-β1 was purchased from PeproTech (Rocky Hill, NJ, USA). CCG1423 and Y27623 (Y27) were purchased from Cayman Chemicals (Ann Arbor, MI, USA). siLentFect and clarity ECL chemiluminescent reagent were obtained from Bio-Rad (Hercules, CA, USA), MRTF-A siRNA (M-054350-01) from Dharmacon (Lafayette, CO, USA), and MRTF-A (SC-32909) antibody from Santa Cruz Biotechnology (Dallas, TX, USA). Rho kinase activity assay and luciferase assays kits were acquired from Cyclex (Japan) and Promega (Madison, WI, USA), respectively. Stiffness gels (0.2, 8, 50 kPa) were obtained from Matrigen Life Technologies (Berea, CA, USA). pGL3-α-SMA and pGL3-col1a2 plasmids were kindly gifted by Dr. Eric Small (Mayo Clinic, Rochester, NY, USA).
Animals
All animal procedures were approved by the Institutional Animal Care and Use Committee (IACUC) at Northeast Ohio Medical University (NEOMED). WT and TRPV4KO mice in C57BL/6J background [1, 62] were fed a standard diet and water ad libitum and kept under a 12-h light/dark cycle.
Myocardial Infarction (MI)
Myocardial infarction was induced in WT and TRPV4KO male mice (12–16 weeks of age) by ligating left anterior descending (LAD) artery as previously described [40]. Briefly, mice were first given atropine sulfate (0.04 mg/kg body wt, i.m.; Phoenix Scientific, St. Joseph, MO, USA) as a pre-anesthetic and intubated with 20-gauge angio-catheter which was connected to rodent ventilator. The mouse was lied on supine position and continuously anesthetized with 2–3% isoflurane through the ventilator. The heart was exteriorized by making an incision in between 4 and 5th ribs, and LAD was permanently ligated with 8-0 suture. The induction of infarction was confirmed with ST elevation in EKG apparatus (Mouse Monitor, Indus Instruments). After the MI surgery, mice were administered with analgesics Buprenex (0.03 mg/kg) and anesthesia was stopped. The mouse was monitored until it recovered from anesthesia and have normal behavior and then transferred to animal facility.
Thoracic echocardiography
Cardiac function was assessed using a Vevo770 system (VisualSonics Inc., Toronto Canada) with a 710B-075 transducer (20–30 MHz) with a frame rate of 40–60 Hz. Animals were anesthetized with 2–3% isoflurane through a nose cone, and parasternal short- and long-axis 2D-M-mode images were acquired at mid-papillary level. All measurements were calculated offline by a blinded reviewer using Vevo770/3.0 software.
Immunohistochemistry
Cardiac fibrosis was analyzed from the heart paraffin sections. Briefly, heart sections (10 µm) were deparaffinized and rehydrated with serial washes with xylene, ethanol (100, 90 and 70%) and water. Then, the sections were stained with picrosirius red staining followed by acquiring bright-field images and 2 × images were used to measure percent collagen deposition using ImageJ software. Additionally, individual collagen types were observed using polarized light microscopy on PSR-stained sections. The presence of red to orange birefringence indicates collagen I, whereas green to yellowish suggests collagen III under polarized light [58].
Cardiac fibroblast isolation and culture
Cardiac fibroblasts (CF) were isolated from adult male, WT and TRPV4KO mice as stated in the previously described protocol with minor modifications [3]. Briefly, hearts from 4 to 6 mice were minced into small pieces which were incubated with 0.75 mg/mL of collagenase 2 and trypsin for 1 h and then cell suspension was centrifuged and plated on 60-mm dishes. Cells were cultured in low-glucose DMEM supplemented with 10% FBS, Nu serum IV, pen/strep, insulin-transferrin-selenium (ITS), FGF, VEGF and heparin. Cells from passage 1 to 2 were used for calcium and TGF-β1-induced differentiation experiments. Rat cardiac fibroblasts (rCFs) were isolated from adult male Sprague Dawley rats, and cells were cultured in low-glucose DMEM media with 10% FBS and 1% pen/strep [3]. Cells from passages 1 to 3 were used for promoter activity assays. mCFs at p1 were plated on the collagen-I-coated varying stiffness gels (0.2, 8 and 50 kpa) for 4 h. Bright-field images were acquired using 4 × with IX51 Olympus microscope, and cell spreading was measured using ImageJ analysis.
Calcium imaging
WT and TRPV4KO CF cultured on MatTek dishes coated with collagen I were loaded with Fluo-4/AM (3 µM) for 20 min and then visualized on Olympus IX80/FV-1000 confocal microscope. Cells were stimulated with GSK (100 nM), and images were acquired every 3 s up to 5 min and analyzed using MetaMorph basic software and Microsoft Excel as previously described [1,2,3]. In the indicated experiments, cells were pre-treated with TRPV4 antagonists: AB1 (10 µM) for 20 min. In some experiments, calcium influx was measured using Fura-2/AM as described previously [5] and data are presented as the ratio of fluorescence 340/380 nm. To investigate TRPV4 mechanosensitivity in CF, we measured hypotonicity-evoked membrane stretch-induced calcium influx. Briefly, Fluo-4-loaded WT and TRPV4KO CF were exposed to either isotonic solution (~ 300 mOSM) (139 mM NaCl, 5 mM KCl, 0.5 mM MgCl2, 1.3 mM CaCl2, 5 mM glucose, 10 mM HEPES, pH 7.4) or hypotonic solution (~ 140 mOSM) 50 mM NaCl, 5 mM KCl, 0.5 mM MgCl2, 1.3 mM CaCl2, 5 mM glucose, 10 mM HEPES, pH 7.4).
CF differentiation and immunofluorescence
CF were serum-starved for 24 h and stimulated with TGF-β1 (10 ng/mL) or GSK (100 nM) for 24 h. For inhibitor studies, cells were pre-treated with Y27 (10 µM) or AB1 (10 µM) for 20 min prior stimulation. Cells were then rinsed with phosphate-buffered saline and fixed with PBS containing 4% paraformaldehyde for 20 min, permeabilized with 0.25% Triton-X100 for 15 min, and blocked with 10% serum-containing media for 30 min. Cells were then incubated with the primary antibodies (α-SMA 1: 250; MRTF-A 1:100; ED-A-FN 1:100) followed by Alexa Fluor-conjugated secondary antibodies (1:500). Images were obtained using an Olympus IX80 fluorescence or IX81 confocal microscope and processed using ImageJ (NIH) software. In some studies, CF were cultured on ECM gels of varying stiffnesses (0.2, 8 and 50 kPa, serum-starved for 24 h and then treated with TGF-β1 for 24 h. α-SMA expression and its incorporation into stress fibers were used as an indicative of differentiation into myofibroblasts (MF), which was independently confirmed by measuring the expression of EDA-FN as previously described [3].
siRNA transfection
CF were transfected with 10 nM mouse MRTF-A-specific SMART pool siRNAs (Dharmacon) using siLentFect reagent (Bio-Rad). After 48 h, MRTF-A knockdown was assessed using quantitative real-time PCR and WB.
Rho kinase assay
mCFs were stimulated with TGF-β1 with or without AB1(10 µM) or CCG1423 (10 µM) for 1 h, and the cells were lysed with 0.1% Triton X-100 lysis buffer containing phosphatase and protease inhibitors. Lysates were centrifuged, and equal protein concentration was used to analyze Rho kinase activity by employing Rho kinase activity assay kit (Cyclex, Japan) according to manufacturer’s instructions.
Promoter activity assay
We have used rCF for the promoter activity assays as they were easier to transfect and show higher expression of reporter genes compared to mCF. We have previously shown that TRPV4 is required for rCF differentiation by TGF-β1 [3]. Briefly, rCFs were transiently transfected with pGL3-α-SMA or pGL3-Col1a2 [52, 57] using lipofectamine 2000 (Invitrogen) transfection reagent. After 24 h of transfection, cells were serum-starved for overnight and treated for 1 h with TGF-β1 or TRPV4 agonist (GSK) in the presence or absence of TRPV4 antagonist (AB1) or MRTF-A antagonist (CCG1423; 10 µM). Then, cells were lysed, and luciferase activity was measured according to manufacturer’s protocol. pSV-β-gal was used as internal control for transfection, and the luciferase activity was normalized with β-galactosidase activity.
Quantitative PCR
RNA was isolated from the cells using an RNeasy Mini Kit (Qiagen), and cDNA was synthesized using qScript cDNA SuperMix (Quanta Biosciences). Real-time PCR (RT-PCR) was performed using the GoTaq Master Mix (Promega) and Fast SYBR Green Master Mix (Applied Biosystems) on the Bio-Rad thermocycler and Fast Real-Time PCR System (Applied Biosystems), respectively, for mouse TRPV4 (F-CCTGCACATTGCCATCGAAC, R-ATCCTT GGGCTGGAAGC), mouse MRTF-A (F-CCCTGGTTAAGAGACTGTG, R-GCTGAAATCTCTCCACTCTGAA) and mouse GAPDH (F-GGGTCCCAGCTTGGTTCATC, R-ATCCGTTCACACCGACCTTC). Gene expression was normalized to GAPDH expression and represented as a relative expression.
Western blotting
Cells were lysed with 1% Triton X-100 containing protease and phosphatase inhibitors; protein concentration was measured using BCA protein assay (Thermo Scientific). Lysates were subjected to 4–20% SDS-PAGE gel electrophoresis and then transferred onto PVDF membrane; PVDF membrane was blocked with 5% milk and then incubated overnight with primary antibodies (MRTF-A, 1:500; Tubulin, 1:2000). Membranes were then washed with TBST (X 3) and incubated with HRP-conjugated secondary antibodies (1:10,000) for 1 h at room temperature. After incubation, membranes were washed with TBST (× 3), incubated with chemiluminescence reagent and developed using ProteinSimple. The intensity of protein bands was quantified using the ImageJ.
Statistical analysis
Statistical analysis was performed using one-way and two-way ANOVA followed by Tukey post hoc analysis or Student’s t test, and the significance was set at p ≤ 0.05.
Results
TRPV4KO mice exhibit preserved myocardial integrity and cardiac function following MI
To investigate whether TRPV4 plays a critical physiological role in cardiac fibrosis/remodeling following injury, WT and TRPV4KO mice were subjected to MI by permanently ligating the LAD and monitored cardiac function for 8 weeks. We found that TRPV4KO mice exhibited improved survival rates compared to the WT mice in response to MI (Fig. 1a). Additionally, we found that WT-MI exhibited anterior wall akinesis, increased LV diameter, LV volume and reduced LV wall thickness compared to TRPV4KO-MI mice (Fig. 1b–d; echocardiographic measurements in Table 1). Immunohistology and serial 2D echocardiography revealed no comparable differences in cardiac function (ejection fraction, EF; fractional shortening, FS) between WT and TRPV4KO at basal level; however, post-MI showed significant differences between WT and TRPV4KO. Importantly, both EF and FS were significantly declined in WT-MI mice compared to WT-sham animals 8 weeks post-MI (WT-sham vs WT-MI; %EF: 62 ± 2.56 vs 25.86 ± 2.51; %FS: 33.80 ± 1.06 vs 11.70 ± 1.85; Fig. 1e, f). In contrast, EF and FS were significantly higher in TRPV4KO-MI mice compared to WT-MI (WT-MI vs TRPV4-MI; %EF: 25.86 ± 2.51 vs 40.11 ± 3.73; %FS: 11.70 ± 1.85 vs 19.69 ± 3.22; Fig. 1e, f). Notably, though there was a similar decline in ejection fraction between WT and TRPV4KO mice 1 week after MI, cardiac function was further declined over the time (8 weeks) in WT-MI mice but preserved in TRPV4KO-MI mice (1E).

Genetic deletion of TRPV4 preserves cardiac function post-MI. a Kaplan–Meier survival graph showing that survival rate was improved in TRPV4KO mice compared to WT mice following 8 weeks after MI. WT-sham (n = 8); WT-MI (n = 14); TRPV4KO-sham (n = 9); TRPV4KO-MI (n = 11). b Representative 2D-echocardiographic M-mode images showing increased wall integrity in TRPV4KO mice compared to WT mice, post-MI. Quantitative analysis of cardiac function LV internal diamerer (c), LV volume (d); % ejection fraction (e) and % fractional shortening (f) from sham and MI, WT and TRPV4KO mice, 1 and 8 weeks after the surgey (n = 8–10; two-way ANOVA followed by Tukey post hoc analysis; significance was set at p ≤ 0.05). *Sham vs MI; $WT vs TRPV4KO, 8 weeks, post-MI
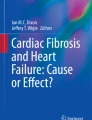
Next, we asked if the preserved myocardial function is due to reduced reactive fibrosis and scar formation in response to MI in TRPV4KO mice. To determine this, heart sections from WT and TRPV4KO of 8 weeks post-MI were stained with picrosirius red (PSR). PSR staining revealed that WT-MI hearts have increased fibrosis both at infarct (scar) and at remote regions (reactive fibrosis) of the myocardium (Fig. 2a). In contrast, TRPV4KO-MI heart sections showed reduced fibrosis at infarct area (scar) and very little or no fibrosis at remote zone area. Notably, TRPV4KO-MI hearts exhibited viable tissue at the infarcted areas which indicate that the absence of TRPV4 attenuated excessive deposition and organization of ECM at the infarct zone and preserved myocardium (Fig. 2a). Quantitative analysis revealed that fibrosis (collagen percent) was significantly lower in TRPV4KO hearts compared to WT mice following MI (Fig. 2b). Further, polarized microscopy images from PSR-stained heart sections from WT-MI mice revealed densely red (birefringence) scars made up of matured collagen throughout entire scar volume, suggesting near total loss of viable tissue in the infarcted region and increased collagen fibers at remote zone areas during remodeling process following MI. However, images from TRPV4KO mice demonstrated a sparse pattern of red birefringence, indicating reduced deposition of matured collagen at the infarcted zone with viable tissue (Fig. 2a). These findings suggest that deletion of TRPV4 preserved cardiac function and myocardial integrity, by reducing cardiac fibrosis 8 weeks post-MI.

Absence of TRPV4 ameliorates cardiac fibrosis following MI. a Representative images of picrosirius red-stained heart sections from WT and TRPV4KO mice, 8 weeks post-sham or MI surgeries. Polarized microscopy of picrosirius red-stained hearts revealed deposition of matured collagen in WT which was absent in TRPV4KO post-MI hearts. Scale bar 500 µm. b Quantification of percent of collagen deposition (fibrosis) in WT and TRPV4KO hearts, 8 weeks after sham or MI surgeries (n = 3–5; one-way ANOVA followed by Tukey post hoc analysis and significance was set at *p ≤ 0.05)
TRPV4 deletion attenuates TGF-β1-induced differentiation in mouse cardiac fibroblasts
Previously, we have shown that TRPV4 integrates soluble (TGF-β1) and mechanical (ECM stiffness) signals in the differentiation of rat cardiac fibroblasts (rCFs) [3]. To confirm if the genetic deletion of TRPV4 influences mouse cardiac fibroblast (mCF) differentiation, we isolated mCFs from WT and TRPV4KO mice and measured CF differentiation on ECM of varying stiffnesses that mimic normal and failing hearts. First, we confirmed the functional deletion of TRPV4 in TRPV4KO mCF using RT-PCR and calcium imaging. RT-PCR analysis showed that TRPV4 was expressed in WT mCF, but absent from TRPV4KO mCF (Fig. 3a). Notably, we found that stimulation with a TRPV4 activator, GSK, failed to induce calcium influx in TRPV4KO mCF (Suppl. Fig. 1). In contrast, GSK induced robust calcium influx in WT mCF, which was inhibited by pre-treatment with TRPV4 antagonist, AB1 (Suppl. Fig. 1). We independently confirmed the functional downregulation of TRPV4 in TRPV4KO mCF by measuring GSK-induced calcium influx using the ratiometric calcium indicator and Fura-2 in the presence and absence of AB1 (Suppl. Fig. 2). Importantly, we found that ATP stimulation evoked calcium influx in both WT and TRPV4KO mCF (Suppl. Fig. 2). To investigate if TRPV4 modulates CF mechanosensitivity, first, we exposed WT and TRPV4KO mCF to hypoosmoloric solution to induce membrane stretch-dependent TRPV4-mediated calcium influx. We found that hypotonicity-induced membrane stretch triggered robust calcium influx in WT CF which is significantly attenuated in TRPV4KO mCF (Fig. 3b). Next, we cultured WT and TRPV4KO mCF on ECM gels of varying stiffnesses that mimic stiffness of normal (8.0 kPa) and fibrotic (50 kPa) hearts for 4 h and compared their degree of spreading as an indicative of TRPV4-mediated mechanosensing [3]. We also included low-stiffness 0.2 kPa gels as controls. We found that both WT mCF spreading and TRPV4KO mCF spreading were similar on low-stiffness (0.2 kPa) gels (Fig. 3c, d). However, WT mCF increased their spreading with an increase in ECM stiffness (8 kPa) that was plateaued at maximum stiffness (50 kPa). In contrast, TRPV4KO mCF exhibited a continued increase in the spreading which was significantly higher compared to WT mCF at both 8 and 50 kPa stiffness (Fig. 3c, d), indicating aberrant mechanosensing. We then measured differentiation by treating the serum-starved mCF cultured on these ECM gels with TGF-β1. α-SMA expression and its incorporation into stress fibers were used as an indicative of differentiation into MF. We found that TGF-β1-treatment induced significant differentiation of WT mCF with increased α-SMA expression and incorporation into stress fibers compared to untreated controls on ECM gels of high stiffness 8 and 50 kPa (Fig. 3e, f). CF differentiation was independently confirmed by measuring the expression of EDA-FN (Suppl. Fig. 3). Importantly, even saturating amounts of TGF-β1 failed to induce CF differentiation on 0.2 kPa gels. Further, this TGF-β1-induced differentiation was completely abolished in TRPV4KO mCF cultured on 8 and 50 kPa gels, indicating that TRPV4 is required for mCF differentiation to MF. Quantitative analysis revealed that CF differentiation was significantly attenuated in TRPV4KO mCF than WT mCF cultured on high-stiffness ECM gels after stimulating with TGF-β1 (Fig. 3e, f).

Absence of TRPV4 attenuates TGF-β1-induced mouse CF differentiation. a Representative RT-PCR agarose gel shows TRPV4 expression in WT mCF but not in the TRPV4KO mCF. b Average calcium traces depicting calcium influx in response to the replacement of isotonic solution (~ 300 mOsm) (line) with hypotonic solution (~ 140 mOsm) (dashed line) in Fluo-4-loaded WT and TRPV4KO mCF. Note that hypotonic stimulation failed to induce calcium influx in TRPV4KO-mCF. The data presented are mean ± SEM of three separate experiments (n = 60 cells). c Bright-field images showing spreading of WT and TRPV4KO mCF on the ECM gels of varying stiffnesses coated with collagen I (0.2, 8, and 50 kPa). Scale bar 50 μm. d Quantification of cell area shows ECM stiffness-dependent spreading of WT mCF which reached platue at 50 kPa, while TRPV4KO mCF exhibited continuously increased spreading with an increase in stiffness. e Immunofluorescence images (× 40) showing α-SMA expression and incorporation into stress fibers in isolated WT and TRPV4KO mCF on different stiffness gels (0.2, 8 and 50 kPa) in response to TGF-β1 (10 ng/mL) (α-SMA: red and DAPI/nuclei: blue). Scale bar 50 μm. f Quantitative analysis of fibroblast differentiation (α-SMA-positive cells). The data presented are mean ± SEM of three independent experiments. Student’s t test; significance was set at *p ≤ 0.05
Rho/Rho kinase/MRTF-A mechanotranscriptional pathway acts downstream of TGF-β1/TRPV4-mediated CF differentiation
To uncover the molecular mechanism downstream of TRPV4 that mediates CF differentiation, we focused on the Rho/Rho kinase pathway. Rho has been implicated in the regulation of cell tension and focal adhesion maturation in response to mechanical forces [34]. We have previously shown that TRPV4 regulates cytoskeletal reorientation through integrin-dependent Rho activation [54]. Therefore, we asked if Rho kinase is activated in response to TGF-β1 stimulation and mediates CF differentiation. We found that pre-treatment with a Rho kinase inhibitor, Y27632, significantly inhibited TGF-β1-induced mCF differentiation (Fig. 4a, b). Importantly, TGF-β1 treatment significantly increased Rho kinase activity in WT mCF which was inhibited by pre-treatment of the cells with TRPV4 antagonist, AB1 (Fig. 4c), suggesting that Rho/Rho kinase pathway acts downstream of TRPV4 in CF differentiation to MF.

TRPV4 mediates CF differentiation via Rho/Rho kinase pathway. a Representative immunofluorescence images (× 20) displaying TGF-β1 (10 ng/mL)-induced differentiation of WT mCF in the presence or absence of Rho kinase inhibitor Y27632 (Y27-10 μM) (α-SMA: green and DAPI/nuclei: blue). Scale bar 10 µm. b Quantitative analysis of fibroblast differentiation (α-SMA-positive cells). c Rho kinase activity was measured in response to TGF-β1 in WT mCF either untreated or treated with TRPV4 antagonist AB1 (10 μM). The data presented are mean ± SEM of three separate experiments. Student’s t test; significance was set at *p ≤ 0.05
Next, we focused on mechanosensitive transcription factor myocardin-related transcription factor-A (MRTF-A) which was shown to be activated in response to stress fiber formation that is mediated by Rho/Rho kinase pathway [16]. First, we asked if MRTF-A is activated downstream of TGF-β1/TRPV4 and found that both TGF-β1 and GSK increased MRTF-A expression as well as its nuclear translocation (quantified as the number of cells with an increase in both cytoplasm and nucleus) in WT mCF, which is abolished by the TRPV4 inhibitor AB1 (Fig. 5a, b), suggesting that TRPV4 activates a Rho-dependent mechanotranscription pathway through MRTF-A. In contrast, we found that TGF-β1 failed to induce MRTF-A activation in TRPV4KO mCF (Suppl. Fig. 4). To confirm the role of MRTF-A in TGF-β1/TRPV4-mediated CF differentiation, we knocked down MRTF-A in mCF with siRNAs and measured their differentiation by staining with α-SMA. Treatment with MRTF-A-specific siRNAs (10 nM) significantly downregulated MRTF-A mRNA and protein expression in mCF (Suppl Fig. 5). Notably, siRNA knockdown of MRTF-A significantly attenuated both TGF-β1- and GSK-induced mCF differentiation (Fig. 5c, d).

TRPV4 mediates TGF-β1-induced CF differentiation via activation of MRTF-A. a Representative immunofluorescence images (× 20) showing activation of MRTF-A (green) in WT mCF in response to TGF-β1 (10 ng/mL) or GSK (100 nM), in the presence or absence of TRPV4 antagonist, AB1. Scale bar 10 µm. b Quantitative analysis of MRTF-A activation (cytosolic and nuclear translocation). c Immunofluorescence images (× 20) showing TGF-β1/GSK-induced differentiation of CF to MF (α-SMA: red, and nuclei were stained with DAPI, blue) in control siRNA and MRTF-A siRNA-treated mCF. d Quantitative analysis of fibroblast differentiation (α-SMA-positive cells). The data presented are mean ± SEM of three separate experiments. Student’s t test; significance was set at p ≤ 0.05. *Significance between TGF-β1 vs control or TGF-β1 + AB1 or AB1; $significance between GSK vs control, GSK + AB1 and AB1
We finally asked whether TRPV4 activation or inhibition effects fibrosis-associated genes. rCFs were transfected with pGL3-col1a2 and pGL3-α-SMA plasmids and stimulated with TGF-β1 in the presence or absence of TRPV4 antagonist AB1. After stimulating with TGF-β1, we found that TRPV4 inhibition significantly decreased α-SMA or col1a2 promoter activity when compared to cells treated alone with TGF-β1 (Fig. 6a, b). Moreover, TRPV4 activation by GSK significantly increased luciferase activity driven by the α-SMA and col1a2 promoters, compared to controls, or cells in the presence of AB1 (Fig. 6c, d). Finally, pharmacological inhibition of MRTF-A with CCG1423 completely abolished both TGF-β1- and GSK-induced activation of α-SMA promoter (Fig. 6e, f) but failed to inhibit TGF-β1-induced Rho kinase activation (Suppl. Fig. 6).

TRPV4 activation regulates cardiac fibrotic gene expression. rCFs (rat cardiac fibroblasts) transfected with either pGL3-α-SMA or pGL3-Col1a2 along with β-galactosidase plasmid were stimulated with TGF-β1 (a, b, e) or GSK (c, d, f) in the presence or absence of TRPV4 antagonist AB1 (10 µM) (a–d) or MRTF-A antagonist CCG 1423 (10 µM) (e, f); luciferase activity was measured 24 h after the stimulation. The data presented are mean ± SEM of three independent experiments. Student’s t test; significance was set at *p ≤ 0.05
Discussion
The present study demonstrates that mechanosensitive ion channel TRPV4 plays a crucial role during cardiac remodeling/fibrosis following MI via modulation of cardiac fibroblast differentiation. We conclude this based on our findings that: (1) absence of TRPV4 attenuated cardiac fibrosis and preserved cardiac function, following MI, (2) direct pharmacological activation of TRPV4 increased promoter activity of pro-fibrotic genes α-SMA and Col1a2 and (3) TRPV4 mediates CF differentiation into MF by modulating the novel mechanosensitive transcriptional Rho/Rho kinase/MRTF-A pathway.
Although both soluble (TGF-β1) and mechanical factors (mechanical stretch, matrix stiffness) are critical for myocardial adaptation to injury/insult, most of the studies on cardiac remodeling are focused on the effects of soluble factors [25, 36, 43]. In fact, the activation of soluble factors is dependent on the alterations in mechanical forces and matrix stiffness [25, 26, 60], but the mechanosensor and its effects in heart failure remain elusive. TRPV4 is a mechanosensitive ion channel, activated by mechanical stimuli such as shear stress, ECM stiffness and cyclic strain, which involved in both physiological and pathological conditions [1,2,3, 10, 29, 45, 50, 54, 56]. We have, for the first time, demonstrated that TRPV4 pharmacological inhibition or siRNA downregulation significantly reduces TGF-β1-induced differentiation of CF cultured on varying stiffness matrices [3], suggesting that TRPV4 mediates CF differentiation by integrating soluble (TGF-β1) and mechanical signaling. We and others have previously shown that CF express TRP channels other than TRPV4. In fact, we have shown that TRPM7 expression is very high in ventricular rCF, but inhibition of TRPM7 did not change TGF-β1-induced differentiation of rCF [3], suggesting that in ventricles TRPV4 is one of the major mechanosensory TRP channels that mediates CF differentiation. Here, by measuring hypotonicity-evoked membrane stretch-induced calcium influx and ECM stiffness-dependent cell spreading and TGF-β1 differentiation in WT and TRPV4KO mCF, we confirmed that TRPV4 is a mechanosensor in cardiac fibroblasts. However, the functional role of TRPV4 in cardiac fibrosis/remodeling following injury or insult is not known.
In our current study, we provide evidence for the functional role of TRPV4 in cardiac remodeling following MI. We found that the absence of TRPV4 reduced cardiac fibrosis following MI which may result in significantly intact live tissue in infarct/border region and maintenance of myocyte integrity in remote zones. Indeed, we found preserved systolic and diastolic function in TRPV4KO mice following MI compared to WT-MI mice. TRPV4 was recently shown to modulate myocyte contractility through the regulation of calcium transients and that pharmacological inhibition of TRPV4 prevented hypoosmotic-stress-induced myocyte death as well as ischemia–reperfusion-induced cardiac damage [27]. However, these studies did not investigate or provide any evidence for the role of TRPV4 in cardiac fibrosis. We hypothesized that the absence of TRPV4 may reduce cardiac fibrosis by inhibiting CF differentiation to MF which could limit myocyte dysfunction. In fact, histological analysis demonstrated that TRPV4KO hearts exhibited significantly less fibrosis (collagen deposition) after MI when compared with WT counterparts. Importantly, we found that genetic deletion or siRNA downregulation of TRPV4 completely attenuated TGF-β1-induced differentiation of cardiac fibroblasts in vitro. Further, we found that pharmacological activation of TRPV4 triggered MRTF-A-dependent activation of pro-fibrotic genes (α-SMA and Col1a2 promoter activity) in CF, suggesting that TRPV4 may regulate CF differentiation at the transcriptional level maybe through a mechanotranscriptional pathway. Indeed, we found that TGF-β1/TRPV4 activates Rho/Rho kinase/MRTF-A pathway upstream of CF differentiation.
Rho kinase is a crucial regulator of actin reorganization and controls many cellular functions, such as motility, adhesion, differentiation and proliferation [20, 21]. Genetic deletion of Rho kinase attenuated fibrosis following angiotensin II infusion-induced heart failure [51]. We have previously demonstrated that TRPV4 regulates mechanical stretch-induced endothelial cell reorientation via activation of Rho/Rho kinase pathway [2, 19, 54]. In the present study, we found that TGF-β1 increased Rho kinase activity which was significantly reduced upon TRPV4 inhibition. Further, inhibition of Rho kinase with Y27 significantly attenuated TGF-β1/TRPV4-induced CF differentiation. These findings confirmed that TRPV4 channels regulate CF differentiation by modulating Rho/Rho kinase pathway. One of the downstream effects of Rho kinase is the polymerization of monomeric G-actin into F-actin, which was shown to activate a mechanosensitive transcription factor, MRTF-A. When released from monomeric actin, MRTF-A translocates into nucleus and induces fibrotic gene expression [35, 52, 57]. We found that activation of TRPV4 by GSK or TGF-β1 treatment increased both MRTF-A expression and nuclear translocation in mCF which is sensitive to TRPV4 inhibition or genetic deletion, suggesting that MRTF-A is downstream of TRPV4 in CF differentiation. Although MRTF-A nuclear translocation is considered as MRTF-A activation, previous studies have shown that pharmacological activation of MRTF-A in fibroblast enriches MRTF-A in cytoplasm and nucleus, supporting our observations that MRTF-A is increased in both cytoplasm and nucleus [57]. Further, we found that pharmacological inhibition of MRTF-A significantly inhibited TGF-β1/GSK-induced fibrotic gene promoter activity (α-SMA and Col1a2). However, TGF-β1 treatment had no effect on Rho kinase activity, suggesting that MRTF-A acts downstream of Rho kinase. Similarly, siRNA knockdown of MRTF-A attenuated TGF-β1-induced CF differentiation, confirming that MRTF-A mediates CF differentiation downstream of TGF-β1/TRPV4 via regulation of pro-fibrotic gene expression. By using MRTF-A null mice, Small et al. have previously demonstrated MRTF-A controls fibroblast differentiation and fibrosis following myocardial infarction [52]. Further, a small molecule activator of MRTF-A has been shown to increase CF differentiation during wound healing [57]. However, the upstream mechanosensor or mechanotransduction mechanisms that regulate Rho kinase/MRTF-A during CF differentiation is not known. Our findings demonstrate that MRTF-A is activated by TRPV4 and identifies that TRPV4 is a mechanosensor in CF that regulates Rho/Rho kinase/MRTF-A mechanotranscriptional pathway.
Importantly, most of the previous studies on the role of soluble factors such as TGF-β1 and other TRP channels in CF differentiation are focused on CF proliferation and α-SMA expression and identified the molecular mechanism to be either classical SMAD/SRF pathway or p38/calcineurin/NFAT pathway [13, 14, 22]. Both pathways were shown to activate fibrotic gene expression including collagen and α-SMA. However, the mechanism that regulates α-SMA incorporation into stress fiber is not known which requires mechanotransduction. Our findings suggest that TRPV4-dependent activation of Rho kinase not only induces α-SMA expression via MRTF-A, but also promotes α-SMA incorporation into stress fibers. We speculate that TRPV4 activation by mechanical forces may induce activation of additional integrins which will increase mechanical stiffness of ECM on the one hand and TGF-β1 activation on the other hand. Once activated, TGF-β1 can cause TRPV4-dependent CF differentiation triggering a positive feedback loop. Recently, it has been shown that pulling of a single integrin can modulate the conformational changes in latent TGF-β1 to release active TGF-β1 from the ECM [59] supporting such a possibility. Our results thus demonstrate that TRPV4 acts as an upstream mechanosensor that not only activates α-SMA synthesis but also incorporates stress fibers during CF differentiation.
Since increased cardiac fibrosis and reduced cardiac function following MI can eventually lead to heart failure, it is feasible that increased TRPV4 expression can contribute to heart failure by increasing CF differentiation and cardiac fibrosis. Indeed, TRPV4 expression was demonstrated to be increased in aortic stenosis [27] and following pressure overload in LV of endoglin+/+ and endoglin+/− mice [47]. Our findings that genetic deletion of TRPV4 in mice protected heart from MI-induced cardiac injury compared to WT mice further support the role of TRPV4 in heart failure. Although our study provides evidence that the absence of TRPV4 protects heart following MI via inhibition of CF differentiation and pathological cardiac remodeling, we cannot rule out the role of TRPV4 from other cell types such as cardiomyocytes and endothelial cells as these studies were performed in global TRPV4KO mice. In fact, TRPV4 has been shown to regulate vascular tone via smooth muscle and endothelial-dependent vasodilation. In smooth muscle cells, TRPV4-mediated calcium influx is activated by Ang II or EET which further induce hyperpolarization via BK channels leading to relaxation [15]. In EC, TRPV4 mediates agonist/flow-induced NO production and vasodilation [23, 62]. Although TRPV4 critically regulates vascular tone, no or minimal change in basal mean arterial blood pressure was observed between WT and TRPV4KO mice [62], indicating that blood pressure regulation in vivo is complicated and does not solely dependent on TRPV4 function and has minimal bearing on the cardiac remodeling in the present study. Further, we have previously shown that TRPV4 deletion in EC induces abnormal angiogenesis in vitro and in vivo in tumor [2, 55, 56]. Therefore, it is plausible that the observed cardioprotection could be due to increased angiogenesis in the heart of global TRPV4KO. Interestingly, TRPV4 expression in cardiomyocyte was shown to be enhanced in aged mice and regulate contractility via modulation of calcium transients and cardiac damage in response to hypoosmotic stress induced by ischemia/reperfusion. However, it is not clear if there is a change in myocyte phenotype or fibrosis in cardiomyocyte-specific TRPV4 transgenic mice [27]. Hence, further studies are needed to dissect the cell-specific (fibroblast/EC/cardiomyocyte) role of TRPV4 in the myocardium. In conclusion, our results demonstrate that TRPV4 mediates TGF-β1-induced CF differentiation to MF via activation of a mechanotranscriptional Rho/Rho kinase/MRTF-A pathway, and genetic deletion of TRPV4 in mice-attenuated pathological remodeling reduced cardiac fibrosis and preserves cardiac function. These findings have clinical significance as they identify TRPV4 as a soluble factor-independent therapeutic target for cardiac fibrosis and heart failure.
References
Adapala RK, Talasila PK, Bratz IN, Zhang DX, Suzuki M, Meszaros JG, Thodeti CK (2011) PKCalpha mediates acetylcholine-induced activation of TRPV4-dependent calcium influx in endothelial cells. Am J Physiol Heart Circ Physiol 301:H757–H765. https://doi.org/10.1152/ajpheart.00142.2011
Adapala RK, Thoppil RJ, Ghosh K, Cappelli HC, Dudley AC, Paruchuri S, Keshamouni V, Klagsbrun M, Meszaros JG, Chilian WM, Ingber DE, Thodeti CK (2016) Activation of mechanosensitive ion channel TRPV4 normalizes tumor vasculature and improves cancer therapy. Oncogene 35:314–322. https://doi.org/10.1038/onc.2015.83
Adapala RK, Thoppil RJ, Luther DJ, Paruchuri S, Meszaros JG, Chilian WM, Thodeti CK (2013) TRPV4 channels mediate cardiac fibroblast differentiation by integrating mechanical and soluble signals. J Mol Cell Cardiol 54:45–52. https://doi.org/10.1016/j.yjmcc.2012.10.016
Al Hattab D, Czubryt MP (2017) A primer on current progress in cardiac fibrosis. Can J Physiol Pharmacol 95:1091–1099. https://doi.org/10.1139/cjpp-2016-0687
Andrei SR, Ghosh M, Sinharoy P, Dey S, Bratz IN, Damron DS (2017) TRPA1 ion channel stimulation enhances cardiomyocyte contractile function via a CaMKII-dependent pathway. Channels (Austin) 11:587–603. https://doi.org/10.1080/19336950.2017.1365206
Bell RM, Botker HE, Carr RD, Davidson SM, Downey JM, Dutka DP, Heusch G, Ibanez B, Macallister R, Stoppe C, Ovize M, Redington A, Walker JM, Yellon DM (2016) 9th Hatter Biannual Meeting: position document on ischaemia/reperfusion injury, conditioning and the ten commandments of cardioprotection. Basic Res Cardiol 111:41. https://doi.org/10.1007/s00395-016-0558-1
Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics C, Stroke Statistics S (2017) Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation 135:e146–e603. https://doi.org/10.1161/CIR.0000000000000485
Berrout J, Jin M, Mamenko M, Zaika O, Pochynyuk O, O'Neil RG (2012) Function of transient receptor potential cation channel subfamily V member 4 (TRPV4) as a mechanical transducer in flow-sensitive segments of renal collecting duct system. J Biol Chem 287:8782–8791. https://doi.org/10.1074/jbc.M111.308411
Burlew BS, Weber KT (2002) Cardiac fibrosis as a cause of diastolic dysfunction. Herz 27:92–98
Cappelli HC, Kanugula AK, Adapala RK, Amin V, Sharma P, Midha P, Paruchuri S, Thodeti CK (2019) Mechanosensitive TRPV4 channels stabilize VE-cadherin junctions to regulate tumor vascular integrity and metastasis. Cancer Lett 442:15–20. https://doi.org/10.1016/j.canlet.2018.07.042
Crowley SD, Gurley SB, Herrera MJ, Ruiz P, Griffiths R, Kumar AP, Kim HS, Smithies O, Le TH, Coffman TM (2006) Angiotensin II causes hypertension and cardiac hypertrophy through its receptors in the kidney. Proc Natl Acad Sci USA 103:17985–17990. https://doi.org/10.1073/pnas.0605545103
Curley D, Lavin Plaza B, Shah AM, Botnar RM (2018) Molecular imaging of cardiac remodelling after myocardial infarction. Basic Res Cardiol 113:10. https://doi.org/10.1007/s00395-018-0668-z
Davis J, Burr AR, Davis GF, Birnbaumer L, Molkentin JD (2012) A TRPC6-dependent pathway for myofibroblast transdifferentiation and wound healing in vivo. Dev Cell 23:705–715. https://doi.org/10.1016/j.devcel.2012.08.017
Du J, Xie J, Zhang Z, Tsujikawa H, Fusco D, Silverman D, Liang B, Yue L (2010) TRPM7-mediated Ca2+ signals confer fibrogenesis in human atrial fibrillation. Circ Res 106:992–1003. https://doi.org/10.1161/CIRCRESAHA.109.206771
Earley S, Heppner TJ, Nelson MT, Brayden JE (2005) TRPV4 forms a novel Ca2+ signaling complex with ryanodine receptors and BKCa channels. Circ Res 97:1270–1279. https://doi.org/10.1161/01.RES.0000194321.60300.d6
Esnault C, Stewart A, Gualdrini F, East P, Horswell S, Matthews N, Treisman R (2014) Rho-actin signaling to the MRTF coactivators dominates the immediate transcriptional response to serum in fibroblasts. Genes Dev 28:943–958. https://doi.org/10.1101/gad.239327.114
Fan D, Takawale A, Lee J, Kassiri Z (2012) Cardiac fibroblasts, fibrosis and extracellular matrix remodeling in heart disease. Fibrogenesis Tissue Repair 5:15. https://doi.org/10.1186/1755-1536-5-15
Fan Z, Guan J (2016) Antifibrotic therapies to control cardiac fibrosis. Biomater Res 20:13. https://doi.org/10.1186/s40824-016-0060-8
Ghosh K, Thodeti CK, Dudley AC, Mammoto A, Klagsbrun M, Ingber DE (2008) Tumor-derived endothelial cells exhibit aberrant Rho-mediated mechanosensing and abnormal angiogenesis in vitro. Proc Natl Acad Sci USA 105:11305–11310. https://doi.org/10.1073/pnas.0800835105
Hall A (2012) Rho family GTPases. Biochem Soc Trans 40:1378–1382. https://doi.org/10.1042/BST20120103
Hall A, Nobes CD (2000) Rho GTPases: molecular switches that control the organization and dynamics of the actin cytoskeleton. Philos Trans R Soc Lond Ser B Biol Sci 355:965–970. https://doi.org/10.1098/rstb.2000.0632
Harada M, Luo X, Qi XY, Tadevosyan A, Maguy A, Ordog B, Ledoux J, Kato T, Naud P, Voigt N, Shi Y, Kamiya K, Murohara T, Kodama I, Tardif JC, Schotten U, Van Wagoner DR, Dobrev D, Nattel S (2012) Transient receptor potential canonical-3 channel-dependent fibroblast regulation in atrial fibrillation. Circulation 126:2051–2064. https://doi.org/10.1161/CIRCULATIONAHA.112.121830
Hartmannsgruber V, Heyken WT, Kacik M, Kaistha A, Grgic I, Harteneck C, Liedtke W, Hoyer J, Kohler R (2007) Arterial response to shear stress critically depends on endothelial TRPV4 expression. PLoS ONE 2:e827. https://doi.org/10.1371/journal.pone.0000827
Harvey PA, Leinwand LA (2011) The cell biology of disease: cellular mechanisms of cardiomyopathy. J Cell Biol 194:355–365. https://doi.org/10.1083/jcb.201101100
Hinz B (2009) Tissue stiffness, latent TGF-beta1 activation, and mechanical signal transduction: implications for the pathogenesis and treatment of fibrosis. Curr Rheumatol Rep 11:120–126
Hinz B, Phan SH, Thannickal VJ, Galli A, Bochaton-Piallat ML, Gabbiani G (2007) The myofibroblast: one function, multiple origins. Am J Pathol 170:1807–1816. https://doi.org/10.2353/ajpath.2007.070112
Jones JL, Peana D, Veteto AB, Lambert MD, Nourian Z, Karasseva NG, Hill MA, Lindman BR, Baines CP, Krenz M, Domeier TL (2019) TRPV4 increases cardiomyocyte calcium cycling and contractility yet contributes to damage in the aged heart following hypoosmotic stress. Cardiovasc Res 115:46–56. https://doi.org/10.1093/cvr/cvy156
Jourdan-Lesaux C, Zhang J, Lindsey ML (2010) Extracellular matrix roles during cardiac repair. Life Sci 87:391–400. https://doi.org/10.1016/j.lfs.2010.07.010
Kanugula AK, Adapala RK, Midha P, Cappelli HC, Meszaros JG, Paruchuri S, Chilian WM, Thodeti CK (2019) Novel noncanonical regulation of soluble VEGF/VEGFR2 signaling by mechanosensitive ion channel TRPV4. FASEB J 33:195–203. https://doi.org/10.1096/fj.201800509R
Kass DA, Bronzwaer JG, Paulus WJ (2004) What mechanisms underlie diastolic dysfunction in heart failure? Circ Res 94:1533–1542. https://doi.org/10.1161/01.RES.0000129254.25507.d6
Kazakov A, Hall RA, Werner C, Meier T, Trouvain A, Rodionycheva S, Nickel A, Lammert F, Maack C, Bohm M, Laufs U (2018) Raf kinase inhibitor protein mediates myocardial fibrosis under conditions of enhanced myocardial oxidative stress. Basic Res Cardiol 113:42. https://doi.org/10.1007/s00395-018-0700-3
Kohler R, Heyken WT, Heinau P, Schubert R, Si H, Kacik M, Busch C, Grgic I, Maier T, Hoyer J (2006) Evidence for a functional role of endothelial transient receptor potential V4 in shear stress-induced vasodilatation. Arterioscler Thromb Vasc Biol 26:1495–1502. https://doi.org/10.1161/01.ATV.0000225698.36212.6a
Kong P, Christia P, Frangogiannis NG (2014) The pathogenesis of cardiac fibrosis. Cell Mol Life Sci 71:549–574. https://doi.org/10.1007/s00018-013-1349-6
Kuo JC (2013) Mechanotransduction at focal adhesions: integrating cytoskeletal mechanics in migrating cells. J Cell Mol Med 17:704–712. https://doi.org/10.1111/jcmm.12054
Kuwahara K, Barrientos T, Pipes GC, Li S, Olson EN (2005) Muscle-specific signaling mechanism that links actin dynamics to serum response factor. Mol Cell Biol 25:3173–3181. https://doi.org/10.1128/MCB.25.8.3173-3181.2005
Leask A (2010) Potential therapeutic targets for cardiac fibrosis: TGFbeta, angiotensin, endothelin, CCN2, and PDGF, partners in fibroblast activation. Circ Res 106:1675–1680. https://doi.org/10.1161/CIRCRESAHA.110.217737
Lee HP, Stowers R, Chaudhuri O (2019) Volume expansion and TRPV4 activation regulate stem cell fate in three-dimensional microenvironments. Nat Commun 10:529. https://doi.org/10.1038/s41467-019-08465-x
Liedtke W, Choe Y, Marti-Renom MA, Bell AM, Denis CS, Sali A, Hudspeth AJ, Friedman JM, Heller S (2000) Vanilloid receptor-related osmotically activated channel (VR-OAC), a candidate vertebrate osmoreceptor. Cell 103:525–535. https://doi.org/10.1016/s0092-8674(00)00143-4
Lighthouse JK, Small EM (2016) Transcriptional control of cardiac fibroblast plasticity. J Mol Cell Cardiol 91:52–60. https://doi.org/10.1016/j.yjmcc.2015.12.016
Luther DJ, Thodeti CK, Shamhart PE, Adapala RK, Hodnichak C, Weihrauch D, Bonaldo P, Chilian WM, Meszaros JG (2012) Absence of type VI collagen paradoxically improves cardiac function, structure, and remodeling after myocardial infarction. Circ Res 110:851–856. https://doi.org/10.1161/CIRCRESAHA.111.252734
Ma Y, Iyer RP, Jung M, Czubryt MP, Lindsey ML (2017) Cardiac fibroblast activation post-myocardial infarction: current knowledge gaps. Trends Pharmacol Sci 38:448–458. https://doi.org/10.1016/j.tips.2017.03.001
Mann DL, Bristow MR (2005) Mechanisms and models in heart failure: the biomechanical model and beyond. Circulation 111:2837–2849. https://doi.org/10.1161/CIRCULATIONAHA.104.500546
Manso AM, Okada H, Sakamoto FM, Moreno E, Monkley SJ, Li R, Critchley DR, Ross RS (2017) Loss of mouse cardiomyocyte talin-1 and talin-2 leads to beta-1 integrin reduction, costameric instability, and dilated cardiomyopathy. Proc Natl Acad Sci USA 114:E6250–E6259. https://doi.org/10.1073/pnas.1701416114
Marian AJ, Braunwald E (2017) Hypertrophic cardiomyopathy: genetics, pathogenesis, clinical manifestations, diagnosis, and therapy. Circ Res 121:749–770. https://doi.org/10.1161/CIRCRESAHA.117.311059
Matthews BD, Thodeti CK, Tytell JD, Mammoto A, Overby DR, Ingber DE (2010) Ultra-rapid activation of TRPV4 ion channels by mechanical forces applied to cell surface beta1 integrins. Integr Biol (Camb) 2:435–442. https://doi.org/10.1039/c0ib00034e
Mendoza SA, Fang J, Gutterman DD, Wilcox DA, Bubolz AH, Li R, Suzuki M, Zhang DX (2010) TRPV4-mediated endothelial Ca2+ influx and vasodilation in response to shear stress. Am J Physiol Heart Circ Physiol 298:H466–H476. https://doi.org/10.1152/ajpheart.00854.2009
Morine KJ, Paruchuri V, Qiao X, Aronovitz M, Huggins GS, DeNofrio D, Kiernan MS, Karas RH, Kapur NK (2016) Endoglin selectively modulates transient receptor potential channel expression in left and right heart failure. Cardiovasc Pathol 25:478–482. https://doi.org/10.1016/j.carpath.2016.08.004
Nielsen SH, Mouton AJ, DeLeon-Pennell KY, Genovese F, Karsdal M, Lindsey ML (2017) Understanding cardiac extracellular matrix remodeling to develop biomarkers of myocardial infarction outcomes. Matrix Biol. https://doi.org/10.1016/j.matbio.2017.12.001
Porter KE, Turner NA (2009) Cardiac fibroblasts: at the heart of myocardial remodeling. Pharmacol Ther 123:255–278. https://doi.org/10.1016/j.pharmthera.2009.05.002
Randhawa PK, Jaggi AS (2015) TRPV4 channels: physiological and pathological role in cardiovascular system. Basic Res Cardiol 110:54. https://doi.org/10.1007/s00395-015-0512-7
Shimizu T, Narang N, Chen P, Yu B, Knapp M, Janardanan J, Blair J, Liao JK (2017) Fibroblast deletion of ROCK2 attenuates cardiac hypertrophy, fibrosis, and diastolic dysfunction. JCI Insight. https://doi.org/10.1172/jci.insight.93187
Small EM, Thatcher JE, Sutherland LB, Kinoshita H, Gerard RD, Richardson JA, Dimaio JM, Sadek H, Kuwahara K, Olson EN (2010) Myocardin-related transcription factor-a controls myofibroblast activation and fibrosis in response to myocardial infarction. Circ Res 107:294–304. https://doi.org/10.1161/CIRCRESAHA.110.223172
Strotmann R, Harteneck C, Nunnenmacher K, Schultz G, Plant TD (2000) OTRPC4, a nonselective cation channel that confers sensitivity to extracellular osmolarity. Nat Cell Biol 2:695–702. https://doi.org/10.1038/35036318
Thodeti CK, Matthews B, Ravi A, Mammoto A, Ghosh K, Bracha AL, Ingber DE (2009) TRPV4 channels mediate cyclic strain-induced endothelial cell reorientation through integrin-to-integrin signaling. Circ Res 104:1123–1130. https://doi.org/10.1161/CIRCRESAHA.108.192930
Thoppil RJ, Adapala RK, Cappelli HC, Kondeti V, Dudley AC, Gary Meszaros J, Paruchuri S, Thodeti CK (2015) TRPV4 channel activation selectively inhibits tumor endothelial cell proliferation. Sci Rep 5:14257. https://doi.org/10.1038/srep14257
Thoppil RJ, Cappelli HC, Adapala RK, Kanugula AK, Paruchuri S, Thodeti CK (2016) TRPV4 channels regulate tumor angiogenesis via modulation of Rho/Rho kinase pathway. Oncotarget 7:25849–25861. https://doi.org/10.18632/oncotarget.8405
Velasquez LS, Sutherland LB, Liu Z, Grinnell F, Kamm KE, Schneider JW, Olson EN, Small EM (2013) Activation of MRTF-A-dependent gene expression with a small molecule promotes myofibroblast differentiation and wound healing. Proc Natl Acad Sci USA 110:16850–16855. https://doi.org/10.1073/pnas.1316764110
Whittaker P, Boughner DR, Kloner RA (1989) Analysis of healing after myocardial infarction using polarized light microscopy. Am J Pathol 134:879–893
Wipff PJ, Rifkin DB, Meister JJ, Hinz B (2007) Myofibroblast contraction activates latent TGF-beta1 from the extracellular matrix. J Cell Biol 179:1311–1323. https://doi.org/10.1083/jcb.200704042
Yamazaki T, Komuro I, Kudoh S, Zou Y, Shiojima I, Mizuno T, Takano H, Hiroi Y, Ueki K, Tobe K et al (1995) Angiotensin II partly mediates mechanical stress-induced cardiac hypertrophy. Circ Res 77:258–265. https://doi.org/10.1161/01.res.77.2.258
Yong KW, Li Y, Huang G, Lu TJ, Safwani WK, Pingguan-Murphy B, Xu F (2015) Mechanoregulation of cardiac myofibroblast differentiation: implications for cardiac fibrosis and therapy. Am J Physiol Heart Circ Physiol 309:H532–H542. https://doi.org/10.1152/ajpheart.00299.2015
Zhang DX, Mendoza SA, Bubolz AH, Mizuno A, Ge ZD, Li R, Warltier DC, Suzuki M, Gutterman DD (2009) Transient receptor potential vanilloid type 4-deficient mice exhibit impaired endothelium-dependent relaxation induced by acetylcholine in vitro and in vivo. Hypertension 53:532–538. https://doi.org/10.1161/HYPERTENSIONAHA.108.127100
Acknowledgements
This work was supported by National Institutes of Health (NIH) (R01HL119705, R01HL148585 and R15CA202847; CKT and R01AI144115; SP). We thank Ashot Minsayan for the technical assistance with MI and echocardiography.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
CKT filed a patent application based on some of the findings in the MS. Rest of the authors declare no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Adapala, R.K., Kanugula, A.K., Paruchuri, S. et al. TRPV4 deletion protects heart from myocardial infarction-induced adverse remodeling via modulation of cardiac fibroblast differentiation. Basic Res Cardiol 115, 14 (2020). https://doi.org/10.1007/s00395-020-0775-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00395-020-0775-5