
Abstract
Purpose
An epidemiologic study that evaluated population’s iodine nutrition status and its relationship with thyroid hormones is lacking in iodine-sufficient area. This nationwide study aimed to evaluate the iodine nutrition status in Korea and relationship between urine iodine concentration (UIC) and thyroid hormones.
Methods
A total of 8318 subjects of the Korea National Health and Nutrition Examination Survey VI (2013–2015) with UIC and thyroid hormone evaluation were included. Median UIC level and estimated 24-h iodine intake were calculated. The prevalence of iodine deficiency or excess was obtained using estimated average requirement or above the tolerable upper intake level cut-point method by estimated iodine intake. We analyzed UIC with regard to age, sex, social economic status, and geographic characteristics.
Results
The median UIC in general population and estimated iodine intake in adult population were 293.9 μg/L (above requirement according to World Health Organization classification) and 249.3μg/day, respectively. The prevalence of iodine deficiency and excess was 14.0 and 13.4%. The median UIC was higher among SAC [511 (299.9–948.5)] and lower among seventies [251.2 (98.9–761.6)] compared to other age groups. The median UIC increased with household income level (p for trend < 0.001). The subjects living in rural and inland region had lowest UIC among the enrolled subjects. The subgroups with higher median UIC were associated with higher mean TSH levels.
Conclusions
This first nationwide study in Korea demonstrated that the median of UIC and estimated iodine intake lie at nearly 300 µg/L and 250 µg/day, respectively, which shows an overall excellent iodine nutrition.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Iodine is essential for the synthesis of thyroid hormones and maintenance of normal thyroid function. Iodine deficiency may decrease iodine availability, resulting in hypothyroidism and goiter formation [1]. Excessive iodine intake is related to a higher prevalence of hypothyroidism [2]. Urinary iodine concentration (UIC) is a well-accepted, cost-efficient, and easily obtainable indicator for iodine status of population. According to iodine nutrition epidemiologic criteria of World Health Organization (WHO), a population’s median UIC of < 100, 100–199, 200–299, and ≥ 300 µg/L are each representative for insufficient, adequate, above requirements, and excessive iodine intake [3]. The national iodine nutrition status is important for determining health policy so that WHO provides country-specific iodine status. Up to date, estimated iodine nutrition were calculated based on median UIC data available from nationwide studies of 130 countries [4, 5].
In contrast to many other countries, mandatory fortification program of iodized salt was not implemented in Korea which has been known as a high iodine intake area in previous small studies. In 1998, Kim et al. [6] reported that the average iodine intake of volunteer over 20 years without history of thyroid disease in Korea was 479 µg/day according to a food questionnaire, and the average UIC was 674 µg/g creatinine. However, Korea is not registered upon WHO map for iodine nutrition status [3] because nationwide epidemiological study evaluating UIC has not yet been conducted.
Herein, we evaluated iodine nutrition status of Korea, and the association between UIC and thyroid hormones using nationwide data from Korea National Health and Nutrition Examination Survey (KNHANES) 2013–2015.
Patients and methods
Study subjects
We used dataset from the KNHANES IV (2013–2015), a nationwide, cross-sectional survey of the Korean population for surveillance of health and nutritional status that used a stratified, multistage clustered probability sampling to select a representative sample of the civilian, non-institutionalized Korean population [7]. Research subjects were selected through two-stage stratified cluster sampling using population and housing census data. KNHANE VI included school-aged children (SAC) subgroup, and there were 481 SAC in this study. Additionally, laboratory tests for serum thyroid stimulating hormone (TSH), free thyroxine (FT4), and UIC were newly added for one-third of the KNHANES IV participants who were subsampled based on gender and age. The study protocol was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention.
Demographic variables of the subject
Social economic data including education, household income, alcohol intake, and smoking status were interviewed through questionnaire. Education level was classified into four categories: graduated from elementary school, middle school, high school, or university. Monthly income was reported in Korean currency and divided into four groups: the lowest, lower-middle, upper-middle, or the highest. Subjects who consumed alcoholic beverages at least once in a month were regarded as current drinkers. Additionally, subjects who smoked at time of enrollment into this study were considered current smokers. The administrative area where subjects lived at the time of survey was also investigated. According to geographic characteristics, the 16 administrative areas of Korea were categorized into four groups (urban and coastal, urban and inland, rural and coastal, and rural and inland). Urban area was defined as metropolitan cities (Gwangyeoksi or Teukbyeolsi), whereas province (Do) was classified into rural area. The administrative area that contains sea was defined as coastal area.
Biochemical variables and laboratory methods
UIC was measured in single spot urine specimen with an inductively coupled plasma mass spectrometry device (ICP-MS; Perkin Elmer ICPMS, Waltham, MA, USA) (reference range 42–350 µg/L for spot urine samples) using an Iodine standard (Inorganic Venture, Christiansburg, VA, USA). The laboratory that measured the UIC is enrolled in “Ensuring the Quality of Urinary Iodine Procedures (EQUIP)” program run by the Centers for Disease Control of the United States of America for quality assurance. Serum TSH and FT4 levels were measured with an electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany): TSH (reference range 0.35–5.50 mU/L) and FT4 (reference range 0.89–1.76 ng/dL) were measured using an E-TSH kit (Roche Diagnostics) and E-Free T4 kit (Roche Diagnostics), respectively. The reported results of TSH and FT4 met the specifications regarding accuracy, general chemistry, special immunology, and ligand of the quality control and quality assurance program of the College of American Immunoassay.
Evaluating iodine status
The representative iodine status of Korea was estimated by median UIC based on WHO recommendation [3]. However, UIC alone might be inappropriate for evaluating the prevalence of iodine deficiency or excess intake [8]. Therefore, we obtained ‘estimated iodine intake’ through the following process under the supervision of an experienced nephrologist (L.J.E): At first, 24-h creatinine excretion rates were calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) estimated creatinine excretion rate (eCER1) Eq. (1) [9], which was developed by CKD EPI in 2011 using data from three large studies and validated them in three separate studies [10]. This equation is unsuitable for children because they have markedly less muscularity which results in less creatinine excretion per bodyweight than adults. So, for subjects under 19 years of age, we used anthropometry-based reference values of 24-h urinary creatinine excretion [11] instead of Eq. (1). Second, we estimated iodine intake using the creatinine excretion rate, urine creatinine (Ucr), bioavailability of iodine, and UIC (2).
Then, the prevalence of iodine deficiency or iodine excess was defined as proportion of subjects below the estimated average requirement (EAR), and above the tolerable upper intake level (UL) based on Institute of Medicine (IOM) [8, 12, 13].
Statistics
SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for the statistical analysis of correlated data to account for the complex sample survey design using the weights assigned to the individuals sampled to represent the Korea population. All categorical variables were presented as number with weighted percentage (%) using Proc Surveyfreq. Among continuous variables, UIC, FT4, and TSH were presented as weighted median with interquartile range (IQR), weighted mean ± standard error (SE), and weighted geographic mean ± SE, respectively, using Proc Surveymeans. The difference and trend of median UIC according to social economic status or geographic pattern were analyzed by Proc Surveyreg adjusted for age and sex. p values < 0.05 were considered significant.
Results
Iodine nutrition status of the Korean population
UIC was measured in 8318 subjects of the KNHANES VI (2013–2015) who were non-pregnant population over 6 years old. Their median UIC (IQR) was 293.9 µg/L (156.5–683.6). On classification of subjects according to EAR or UL cut-point method, the prevalence of iodine deficiency and iodine excess was 14.0 and 13.4% (Table 1). For adult population (age > 19 years) only, median of UIC and estimated 24-h iodine intake was 274.2 µg/L (148.4–643.5) and 249.3 µg/day (131.1–590.5), respectively.
UIC according to age and sex
Among the age groups, population younger than 10 years showed highest median UIC [511.0 µg/L (299.9–948.5), Table 1]. From age 20 years onwards, median UIC was lesser than those of aged under 20 years, but all of the age groups were population of above requirements for iodine nutrition. In the elderly over 70 years, median UIC was 251.2 µg/L (98.9–761.6), which was lower than other age groups of adults and approximately one-fourths (106/505, 22.8%) of this elderly group was iodine deficiency based on EAR cut-point method. For almost age groups, the median UIC of female was slightly higher than that of male but each age stratum in male and female group was similar (Table 1). The median UIC of school-aged children (SAC 6–12 years) was 528 µg/L (283.8–996.8) and 32.6% of them had estimated iodine intake above the UL (Table S1).
UIC according to social economic status
Table 2 showed the median UIC according to income levels, education levels, alcohol intake status, and smoking status. The higher income a household reported, the higher median UIC was reported; the median UIC was 250.4 µg/L (121.3–585.9), 277.1 µg/L (151.3–627.1), 298.7 µg/L (158.4–689.2), and 313.1 µg/L (173.2–757.1) for the lowest, lower-middle, upper-middle, and the highest quartile of income level (p for trend < 0.001). High school education group had a lower median UIC (IQR) than those with elementary school education or less [330.6 µg/L (163.6–859.8) vs. 264.2 µg/L (145.8–580.3); p < 0.001]. Median UIC in subjects with alcohol experience was significantly lower than those in never drinker [279.5 µg/L (151.3–643.1) vs. 348.0 µg/L (164.6–892.9); p < 0.001]. Similarly, current smoker showed lower median UIC than never smoker [279.6 µg/L (147.6–652.5) vs. 248.3 µg/L (138.1–577.6); p < 0.001]. In subgroup analysis by gender, the relationship between social economic status and UIC was more obvious in males.
UIC according to geographic location
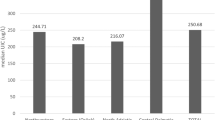
Figure 1 shows the difference of median UIC among the 16 administrative areas of Korea. Among the four categories according to geographic characteristics of residence (urban and coastal, urban and inland, rural and coastal, and rural and inland), UIC was highest in urban and coastal region [316.8 µg/L (163.7–784.2)] and lowest in rural and inland region [232.3 µg/L (116.8–495.5)] (Table 3).

Choropleth map of median UIC of administrative areas in Korea
UIC and thyroid function
UIC, TSH, and FT4 were simultaneously measured in 6564 subjects of the KNHANES VI (2013–2015). Table 4 shows changes of serum TSH or FT4 levels according to UIC categories. Geometric mean (mU/L) (SE) of serum TSH were 1.92 (0.04), 2.01 (0.02), 2.09 (0.03), 2.24 (0.03), 2.19 (0.03), and 2.39 (0.04) in subgroup with UIC < 100, 100–199, 200–299, 300–499, 500–999, and ≥ 1000 µg/L, respectively. The serum TSH level showed significant increasing trend as UIC was increasing (Table 4; p for trend < 0.001). The serum FT4 levels showed statistically significant but not clinically significant change according to UIC (Table 4; p for trend < 0.001).
Discussion
In this study, we firstly reported the nationwide iodine status of Korea, and found that the median UIC was 293.9 µg/L (156.5–683.6). The median UIC was varied according to age, gender, social economic status, and geographic characteristic of residence. The subgroups with higher median UIC were associated with higher mean TSH levels while the relationship was not evident between UIC and FT4 levels.
The Korean population has been suggested to be iodine-sufficient in several non-representative studies [14,15,16]. A recent study of 540 healthy, urban-dwelling adults in Korea reported a median UIC of 268 µg/L [15]. Another study by Lee et al. [16] reported excessive iodine status in Korean preschool children (2–7 years of age), reporting a median UIC of 438.8 µg/L. Despite these some studies, there were no national data so that Korea was not registered in iodine nutrition map of WHO. In the first presented nationwide report of this study, Korean population is above requirements for iodine nutrition. Unique diet pattern such as seaweed soup or basic ingredient made from sea tangle or kelp is considered as main cause of above requirements for iodine nutrition [17]. The major sources of dietary iodine in the Korean population are seaweed (66%), milk and dairy products (11%), and fish (9%) [18].
However, variations in UIC existed among the different age groups. In this study, median UIC of SAC was above 500 µg/L [528 µg/L (283.8–996.8)] and 32.6% of them was iodine excess which is associated with increasing thyroid volume reflecting the adverse effects of chronic iodine excess [19]. They are considered as the target and representative group for iodine nutrition status surveillance because of their combined high vulnerability, easy access, and applicability to a variety of surveillance activities [3]. However, in this study, SAC did not represent the general population of Korea. It is also observed in the US NHANES data that SAC had a higher median UIC than adult. In addition, excessive iodine intake of SAC has been reported in the Food and Drug Administration’s Total Diet Study on iodine intake [20]. Given that the UIC was not high in the age group of parents, school meal or snack outside seems to be the main cause of exceed iodine intake in SAC. Further assessment of iodine nutrition and relevant health policy is needed to help prevent iodine excess-induced thyroid dysfunction in later life [2].
In contrast, 22.8% of elderly over 70 years have estimated iodine intake below the EAR. Although we did not demonstrate the exact reason, it might be associated with malnutrition. Iodine deficiency could lead to the development of hypothyroidism with corresponding fatigue, goiter, mental slowing, depression, and weight gain [1]. Therefore, further consideration of the iodine nutrition status is needed in the elderly population, even in iodine-sufficient countries. The median iodine concentration of the pregnant and lactating population in Korea was 210.2 µg/L (137.4–449.9). However, the data of pregnancy and lactation population might be unreliable due to small number of people surveyed (only 46 subjects). Rather, a recent study of 344 healthy pregnant women in Korea reported that the median UIC was 427.3 µg/L [21].
Analysis of the association between social economic status and UIC revealed that current smoker or alcohol drinker showed lower UIC than never smoker or never drinker. Association between smoking or alcohol habits and iodine intake has been discussed in some previous studies [22], and smokers or alcohol drinkers may have a higher requirement for iodine [23, 24]. However, clinical impact of these findings may be small in Korea because UIC of smoker or alcohol drinkers are even not low. Our results also confirmed that incomes and education level were possible contributors to iodine nutrition. The previous study of 4865 women in China showed that having income ≥ 2000 yuan (compared with those having income < 1000 yuan) and less than high school education (compared with those having more than a high school education) had a higher UIC [25], which supports our data. The difference of UIC according to income and education levels could be explained by fact that income and education might simply represent more diverse food choices or a greater awareness of health.
In this study, the subjects living in seaside areas showed higher UIC than those living in inland areas. Better access to seaweed which is the main source of iodine intake in Korea might contribute the result. This trend is consistent with the previous studies [26, 27]. The subjects living in urban areas had higher UIC than those who were not. It is similar to the result of study in southern Italy [28] but contrast to that of study in Zhejiang province of China [26]. This difference could be explained by the fact that rural subjects in the study of china consumed much pickled food with iodized salt which is not implemented in Korea. More consumption of processed food or high income level of the subjects in urban areas is possible reason of higher UIC.
In current study, subgroups with higher median UIC were associated with higher mean TSH levels. However, it does not imply that sufficient iodine supply increased risk for hypothyroidism. First of all, this study is not longitudinal study. Moreover, considering physiologic adaptation of thyroid glands after iodine supplement, increased TSH level should not be interpreted as evidence for real hypothyroidism [29].
The strength of this study is that it is the first report of nationwide UIC and its relationship with thyroid hormones of Korea. However, we did not present the median UIC of the SAC as a representative value recommended by WHO guideline due to relatively small subjects in SAC. In addition, intra-individual variation (day to day variation) of UIC was not adjusted because repeated data of UIC are absent in KNHANES. For exact evaluation, further study with repeated data of UIC or large cohort of SAC in Korea will be required. Another limitation is that estimated iodine intake for children was calculated using reference value of Caucasian children because there are no data of Korean children. Additionally, because this was a cross-sectional study, we cannot guarantee the causal relationship between urine iodine and thyroid hormones.
In conclusion, this first nationwide study in Korea demonstrated that the median of UIC and estimated iodine intake in the adult population lies at nearly 300 µg/L and 250 µg/day, respectively, showing an overall excellent iodine nutrition in Koreans. And our study confirms that higher UIC is associated with higher TSH levels. However, considerable proportion of subjects (13.4% for excess iodine intake and 14.0% for iodine deficiency) was inadequate for iodine intake which could be related to an increase in the risk of thyroid disease. Therefore, more attention in health policy for iodine nutrition is needed, especially for vulnerable groups such as elderly, pre-existing thyroid disease, or young people [30]: further nutritional studies to identify accurate dietary sources of iodine in Korean education program about adverse effects of inadequate iodine intake or diet sources of iodine, and long-term monitoring about iodine status for adjusting iodine intake.
References
Zimmermann MB (2009) Iodine deficiency. Endocr Rev 30:376–408
Leung AM, Braverman LE (2014) Consequences of excess iodine. Nat Rev Endocrinol 10:136–142
World Health Organization, United Nations Children’s Fund, International Council for the Control of Iodine Deficiency Disorders (2007) Assessment of iodine deficiency disorders and monitoring their elimination: a guide for programme managers, 3rd edn. World Health Organization, Geneva [cited: 2 August 2017]. http://apps.who.int/iris/bitstream/10665/43781/1/9789241595827_eng.pdf
Zimmermann MB (2013) Iodine deficiency and excess in children: worldwide status in 2013. Endocr Pract 19:839–846
Zimmermann MB, Andersson M (2012) Update on iodine status worldwide. Curr Opin Endocrinol Diabetes Obes 19:382–387
Kim JY, Moon SJ, Kim KR, Sohn CY, Oh JJ (1998) Dietary iodine intake and urinary iodine excretion in normal Korean adults. Yonsei Med J 39:355–362
Tran BT, Jeong BY, Oh JK (2017) The prevalence trend of metabolic syndrome and its components and risk factors in Korean adults: results from the Korean National Health and Nutrition Examination Survey 2008–2013. BMC Public Health 17:71
Zimmermann MB, Andersson M (2012) Assessment of iodine nutrition in populations: past, present, and future. Nutr Rev 70:553–570
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J, CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
Matsushita K, Mahmoodi BK, Woodward M, Emberson JR, Jafar TH, Jee SH, Polkinghorne KR, Shankar A, Smith DH, Tonelli M, Warnock DG, Wen CP, Coresh J, Gansevoort RT, Hemmelgarn BR, Levey AS (2012) Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA 307:1941–1951
Remer T, Neubert A, Maser-Gluth C (2002) Anthropometry-based reference values for 24-h urinary creatinine excretion during growth and their use in endocrine and nutritional research. Am J Clin Nutr 75:561–569
Institute of Medicine (US) Pannel on Micronutrients (2001) Dietary reference intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium and zinc. The National Academies Press (US), Washington, DC
Zimmermann MB, Hussein I, Al Ghannami S, El Badawi S, Al Hamad NM, Abbas Hajj B, Al-Thani M, Al-Thani AA, Winichagoon P, Pongcharoen T, van der Haar F, Qing-Zhen J, Dold S, Andersson M, Carriquiry AL (2016) Estimation of the prevalence of inadequate and excessive iodine intakes in school-age children from the adjusted distribution of urinary iodine concentrations from population surveys. J Nutr 146:1204–1211
Chung JH (2013) Low iodine diet for preparation for radioactive iodine therapy in differentiated thyroid carcinoma in Korea. Endocrinol Metab (Seoul) 28:157–163
Choi J, Kim HS, Hong DJ, Lim H, Kim JH (2012) Urinary iodine and sodium status of urban Korean subjects: a pilot study. Clin Biochem 45:596–598
Lee J, Kim JH, Lee SY, Lee JH (2014) Iodine status in Korean preschool children as determined by urinary iodine excretion. Eur J Nutr 53:683–688
Rhee SS, Braverman LE, Pino S, He X, Pearce EN (2011) High iodine content of Korean seaweed soup: a health risk for lactating women and their infants? Thyroid 21:927–928
Kim JY, Kim KR (2000) Dietary iodine intake and urinary iodine excretion in patients with thyroid diseases. Yonsei Med J 41:22–28
Zimmermann MB, Ito Y, Hess SY, Fujieda K, Molinari L (2005) High thyroid volume in children with excess dietary iodine intakes. Am J Clin Nutr 81:840–844
Caldwell KL, Makhmudov A, Ely E, Jones RL, Wang RY (2011) Iodine status of the U.S. population, National Health and Nutrition Examination Survey, 2005–2006 and 2007–2008. Thyroid 21:419–427
Cho YY, Kim HJ, Oh SY, Choi SJ, Lee SY, Joung JY, Jeong DJ, Sohn SY, Chung JH, Roh CR, Kim SW (2016) Iodine status in healthy pregnant women in Korea: a first report. Eur J Nutr 55:469–475
Valeix P, Faure P, Peneau S, Estaquio C, Hercberg S, Bertrais S (2009) Lifestyle factors related to iodine intakes in French adults. Public Health Nutr 12:2428–2437
Valeix P, Faure P, Bertrais S, Vergnaud AC, Dauchet L, Hercberg S (2008) Effects of light to moderate alcohol consumption on thyroid volume and thyroid function. Clin Endocrinol (Oxf) 68:988–995
Vestergaard P (2002) Smoking and thyroid disorders–a meta-analysis. Eur J Endocrinol 146:153–161
Yang J, Zheng H, Li X, Zhu L, Hao Z, Chen G, Liu Y, Wang Y (2014) Assessment of iodine status and associated factors in vulnerable populations in Henan Province, China, in 2012. Asia Pac J Clin Nutr 23:626–633
Zou Y, Lou X, Ding G, Mo Z, Zhu W, Mao G (2014) A cross-sectional comparison study on the iodine nutritional status between rural and urban residents in Zhejiang Province, China. BMJ Open 4:e005484
Medani AM, Elnour AA, Saeed AM (2011) Endemic goitre in the Sudan despite long-standing programmes for the control of iodine deficiency disorders. Bull World Health Organ 89:121–126
Aghini-Lombardi F, Vitti P, Antonangeli L, Fiore E, Piaggi P, Pallara A, Consiglio E, Pinchera A (2013) The size of the community rather than its geographical location better defines the risk of iodine deficiency: results of an extensive survey in Southern Italy. J Endocrinol Invest 36:282–286
Johner SA, Thamm M, Stehle P, Nothlings U, Kriener E, Volzke H, Gartner R, Remer T (2014) Interrelations between thyrotropin levels and iodine status in thyroid-healthy children. Thyroid 24:1071–1079
Laurberg P, Cerqueira C, Ovesen L, Rasmussen LB, Perrild H, Andersen S, Pedersen IB, Carle A (2010) Iodine intake as a determinant of thyroid disorders in populations. Best Pract Res Clin Endocrinol Metab 24:13–27.
Acknowledgements
The authors thank the Korea National Health and Nutrition Examination Survey for providing public access to its data and Jung Eun Lee, MD, Ph.D. (Division of Nephrology, Samsung Medical Center) for advice about estimated iodine intake.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kim, H.I., Oh, HK., Park, S.Y. et al. Urinary iodine concentration and thyroid hormones: Korea National Health and Nutrition Examination Survey 2013–2015. Eur J Nutr 58, 233–240 (2019). https://doi.org/10.1007/s00394-017-1587-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-017-1587-8