
Abstract
Purpose
Neuropathic pain is a common diabetic complication. It is characterized by symptoms of spontaneous and stimulus-evoked pain including hyperalgesia and allodynia. l-Arginine is a common precursor of many metabolites of biological interest, in particular, nitric oxide (NO), ornithine, and hence polyamines. In central nervous system, NO, glutamate, and polyamines share an N-methyl-d-aspartate (NMDA) receptor-mediated effect. We hypothesized that a variation in arginine metabolism caused by diabetes may contribute to development and maintenance of neuropathic pain and to the worsening of clinical and biological signs of diabetes.
Methods
We examined whether oral l-arginine supplementation (2.58 ± 0.13 g/l in drinking water for 3 weeks) could improve the development of neuropathic pain and the clinical, biological, and metabolic complications of diabetes in streptozocin (STZ)-induced diabetic (D) rats.
Results
STZ administration induced classical symptoms of type 1 diabetes. Diabetic rats also displayed mechanical hypersensitivity, tactile, and thermal allodynia. Plasma citrulline and NO levels were increased in diabetic hyperalgesic/allodynic rats. l-Arginine supplementation failed to reduce hyperglycaemia, polyphagia, and weight loss. Moreover, it abolished hyperalgesia and allodynia by normalizing NO plasma concentration and increasing plasma agmatine concentration.
Conclusions
l-Arginine supplementation prevented the development of mechanical hyperalgesia, tactile, and thermal allodynia in painful diabetic neuropathy with concomitant reduction of NO and increased agmatine production, offering new therapeutic opportunities for the management of diabetic neuropathic pain.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetic neuropathy (DN) is a common complication of both type 1 (T1DM) and type 2 diabetes mellitus (T2DM) [1]. Indeed, over 246 million of diabetic patients, between 20 and 30 million are affected by symptomatic diabetic neuropathy [2]. The most frequent clinical form of diabetic neuropathy is by far the diabetic distal sensory or sensorimotor polyneuropathy sometimes asymptomatic but usually causing abnormal sensations (paresthesia and dysesthesia) and/or pain. Spontaneous or evoked pain and abnormal sensations are associated with neuropathy. The estimated prevalence of painful polyneuropathy varies between 8% [3] and 65% [4] with an overall prevalence around 15% [5]. The first-line drugs based on Grading of Recommendations Assessment, Development, and Evaluation (GRADE) recommended for neuropathic pain are noradrenaline serotonin reuptake inhibitor antidepressants (duloxetine and venlafaxine), tricyclic antidepressants, pregabalin, gabapentin, or gabapentin enacarbil [6, 7].
However, a substantial percentage of patients do not respond favourably to these treatments. The estimated Number Needed to Treat (corresponding to the number of patients who must be treated for one patient to demonstrate a >50% reduction of pain from baseline) ranges from 3.6 for amitriptyline, 7.7–7.2 for pregabalin and gabapentin [8] and 6.4 for SNRI [7]. Therefore, there is a need for efficient additional therapies [9], including non-pharmacological modalities.
Arginine deficiency has been reported in streptozocin (STZ)-induced experimental diabetes in rats [10]. Although l-arginine can be endogenously synthesized from citrulline or protein breakdown, it is considered as a semi-essential amino acid in some situations [11]. It is involved in multiple biological and metabolic effects [12] such as muscle and protein metabolism, vasorelaxation, immune responses, growth hormone, prolactin, and glucagon release [13, 14]. l-Arginine also stimulates in vitro and in vivo insulin release [12, 15]. l-Arginine is a common precursor for nitric oxide (NO), agmatine, ornithine and hence polyamines, glutamate, and glutamine, i.e., molecules involved in cellular signalization [16]. In central nervous system (CNS), NO, agmatine, glutamate, and polyamines share a common N-methyl-d-aspartate (NMDA) receptor-mediated effect [12, 17]. NMDA receptor plays a major role in chronic pain processing particularly in central sensitization resulting from peripheral nerve injury. In such pathological condition, sustained release of glutamate from primary afferent fibres activates post-synaptic α-amino-3-hydroxy-5-methylisoxazole-propionic acid (AMPA) receptors resulting in sodium entry and membrane depolarization. This relieves the magnesium voltage-dependant blockade [18] allowing NMDA receptor activation and calcium influx. High intracellular calcium concentration stimulates neuronal nitric oxide synthase (nNOS) and other signaling pathways [19] resulting an increase of neuronal excitability, hyperalgesia, and allodynia. In STZ-diabetic hyperalgesic rats, NMDA receptor phosphorylation as well as hyperalgesia and allodynia can be suppressed pharmacologically with an NMDA receptor antagonist [20] and by an oral magnesium supplementation [21]. The main disadvantages of such pharmacological and nutritional approaches are the lack of benefit effect on hyperglycemia and the onset of side effects (cognitive, sedative, and dissociative effects), respectively.
We previously reported that agmatine suppressed tactile and thermal allodynia and mechanical hyperalgesia in STZ-induced diabetic rats. This effect involved the inhibition of NOS activity [22]. Given that l-arginine metabolites (NO and polyamines) can modulate NMDA channel currents (and hence contribute to neuropathic pain) and that arginine may influence insulin release and sensitivity, we examined whether oral l-arginine supplementation can improve biological and metabolic (blood glucose, urine nitrogen, plasma insulin, arginine, ornithine, glutamate, glutamine, citrulline, agmatine, and NO), as well as clinical parameters (body weight, food, and water intakes) and hence pain-related behavior (mechanical hypersensitivity, tactile, and thermal allodynia) in STZ-induced diabetic (STZ-D) rats.
Materials and methods
Animals and diets
Male Sprague–Dawley rats weighting 226–250 g were purchased from Charles River (Cléon, France). Rats were fed a normal chow diet: Rat/Souris Entretien AO4 (Safe, Epinay-sur-Orge, France) containing protein 16 g/kg and arginine 9.8 g/kg. Animals were housed three per cage under the standard laboratory conditions and a 12–12 h light–dark cycle and liter was changed every day. Water and food were available ad libitum. The animals were maintained and handled according to the recommendations of the International Association for the Study of Pain (IASP) guidelines for animal experiments [23] and approved by the local Ethics Committee (C2EA, approval no. CE3-06). Great care was taken, particularly with regard to housing conditions, to avoid or minimize discomfort for animals.
Induction of diabetes and l-arginine supplementation
Animals were rendered diabetic by a single intraperitoneal (i.p.) injection of STZ (72 mg/kg) (Sigma-Aldrich, St Quentin Fallavier, France) dissolved in distilled water. Diabetes was confirmed 1 week after by measuring tail vein blood glucose level on an ACCU-CHEK glucose meter (Roche Diagnostics, Paris, France). Animals with blood glucose level ≥2 g/l were considered diabetic (D) and included in the study. For the control group, ten male Sprague–Dawley rats i.p. injected with 5 ml/kg of distilled water and were used as control for STZ-D rats.
One week after STZ (STZ-D rats) or distilled water (control non-diabetic rats) injection, and immediately after blood glucose level measurement, the animals were assigned to the following experimental groups:
-
l-Arginine (l-Arg)-supplemented STZ-D group: STZ-D rats receiving l-arginine (2.58 ± 0.13 g/l) in drinking water for 3 weeks (n = 10);
-
Non-supplemented STZ-D group: STZ-D rats given tap water for 3 weeks (n = 10);
-
Control non-diabetic group: rats given tap water for 3 weeks (n = 10).
Three separate experimental groups (n = 6 per group) were added to measure agmatine plasma concentrations.
Measurement of clinical, biological, and metabolic parameters
Body weight, expressed as an average of two repeated measures, was determined weekly using an automated balance S/SI-2002 (Fisher Scientific, New York, USA).
Glycaemia was determined once a week for 4 weeks by measuring tail vein blood glucose level using an ACCU-CHEK glucose-meter (Roche Diagnostics, Paris, France). For determination of metabolic parameters, rats were housed individually in metabolic cages for 24 h with free access to food and water. Food and water intakes as well as urine excretion were measured for each rat daily. Urine was collected in tubes containing 200 µl of antiseptics (Amukine, 0.06%, Gifrer Barbezat, Décines, France) and freezed at −20 °C until analysis.
Urine nitrogen excretion was measured after adequate dilution (1/800). The nitrogen content was determined by gas-phase chemiluminescence (Antek Instruments Inc. 7000, Houston, TX, USA) as previously described [24]. The instrument converts all chemically bound nitrogen to NO at 1100 °C in the pyroreactor. NO is read by a photomultiplier tube attached to the instrument, at a wavelength between 650 and 900 nm.
Blood was collected under halothane (3.5%) anesthesia by cardiac puncture and immediately centrifuged (3500×g for 10 min, 4 °C). Plasma was separated and stored at −20 °C until analysis. Plasma insulin concentration was measured using an enzyme-linked immunosorbent assay kit (Insulin ELISA, Ultrasensitive Rat Insulin Elit, Mercodia, Uppsala, Sweden).
Measurement of l-arginine and its metabolites
Nitric oxide concentration was determined by its degradation products in plasma [NO(x)]: nitrites (NO2) plus nitrates (NO3 −). Nitrites were determined using a colorimetric assay based on the Griess reaction [25]: 100 µl of plasma was combined to 100 µl of Griess reagent (1 vol of 0.5% sulphalinamide in 6-phosphoric acid plus 1 volume of 0.05% natphthylethylene-diamine dihydrochloride in distilled water) and incubated 10 min at room temperature. Nitrates were measured as nitrite after enzymatic conversion by nitrate reductase as described by Schmidt et al. [26]. The absorbance was measured at 540 nm in a microplate reader (Dynatech Laboratories, El Paso, TX, USA) and NO2 − concentrations were determined with reference to a sodium-nitrite standard. Values obtained represent the sum of nitrite plus nitrate concentrations.
Arginine, glutamate, glutamine, citrulline, and ornithine concentrations were determined by ion-exchange column chromatography (IEC) with post-column ninhydrin derivatization as described previously [27, 28] on a amino-acid analyzer (model 6300, Beckmann Instruments, Palo Alto, CA, USA). Before amino-acid analysis, plasma were treated for deproteinization with sulfosalicylic acid (50 mg/ml plasma). After 5 min, the samples were centrifuged (750×g, 10 min, 4 °C) and amino-acid content of the supernatants was quantified. Chromatographic peaks were recorded. The Laboratory participates in the European Control Quality Scheme (ERNDIM, Brussels, Bergium) and the results indicate the accuracy and reproducibility of the measurements with a between batch reproductibility ranging from 2 to 5% for various amino acids.
Thin-layer chromatography (TLC) method was used to separate and determine agmatine plasma concentration. Agmatine sulfate was prepared at a concentration of 2.0 mg/ml (free base) in 5% trichloroacetic acid (TCA). The serum was adjusted at 5% TCA on ice. The homogenate was centrifuged (12,000×g, 15 min, 4 °C). The precipitate was discarded and supernatant was used for dansylation of agmatine. Aliquots of 1 ml of the supernatant of the serum or of agmatine (100 µg/ml in 5% TCA), i.e., 100 µg were placed in test tubes and NaHCO3 was added until saturation. Then, 1 ml of dansyl chloride (5 mg/ml in acetone) was added, using a Vortex mixer while adding the reagent. The tubes were closed and incubated at 40 °C for 1 h. After dansylation, 0.5 ml of 0.1 g/ml glycine solution was added to react with residual dansyl chloride. The content of tubes was mixed and tubes were heated at 40 °C for 30 min. Water (3 ml) was added and dansyl amines were extracted with 3× 2 ml diethyl ether, leaving the dansyl-glycine behind. The combined diethyl ether extracts were evaporated to dryness and the residue was dissolved in 250 µl ethyl acetate. During this procedure, exposure to light was minimized. The dansyl amines were separated by TLC: high-performance thin-layer chromatography plates (HPTLC, 20 × 10 cm; Merck) were used. Samples were applied under a flow of nitrogen on the HPTLC plate using Linomat IV (CAMAG, Muttenz, Switzerland) and separated using the following sequential development system: development either to half final distance in methyl acetate followed by full development in cyclohexane–ethylacetate (50:50, v/v). The quantification was performed after photographing the plates under UV and measuring density with the Image.Lab 5.1 (Biorad) software.
Measurement of mechanical sensitivity
Rats underwent the paw pressure test as described by Randall and Selitto [29]. Nociceptive thresholds, expressed in grams (g), were measured using an analgesimeter (Ugo Basile, Bioseb, France) by applying increasing pressure to the left hind-paw until vocalization was elicited. The maximal pressure applied (cutoff) was 450 g. As this test involves animal handling, the experimenter got the rat used to being handled. The vocalization threshold (VT) was measured three or four times to obtain two consecutive values that differed no more than 10%, and respecting an interval of at least 10 min between two measures. The results are expressed as VT variations using the formula: VT pre-STZ or distilled water—VT post-STZ or distilled water (g).
Measurement of tactile sensitivity
Rats were placed individually on an elevated plastic mesh (1 cm2 perforations) in a clear plastic cage and allowed at least 15 min to adapt to the testing environment. Von Frey hairs (Semmes–Weinstein monofilaments, Stoelting, IL, USA) with calibrated bending forces (from 1.479 to 15.136 g) were used to deliver punctuated mechanical stimuli of varying intensity. Starting with the lowest filament force, von Frey hairs were applied from below the mesh floor to the plantar surface of the hind-paw with sufficient force to cause slight bending against the paw, and held for 1 s. Each stimulus was applied five times at inter stimulus intervals of 4–5 s. Care was taken to stimulate random locations on the plantar surface. A positive response was recorded if the paw was robustly and immediately withdrawn. Paw-withdrawal threshold was defined as the minimum pressure required eliciting a paw-withdrawal reflex at least once out of the five trials. If no response was recorded in any trial, the process was repeated with the next-highest force hair. Tactile allodynia was defined as a significant decrease in withdrawal thresholds to von Frey hair application. The 15.136 g hair was selected as the upper limit cutoff for testing.
Measurement of thermal sensitivity
The rat’s tail was immersed in a water bath maintained at 42 °C, i.e., a temperature normally innocuous in normal rats [30], until tail withdrawal or signs of struggle were observed (cut-off time 15 s). As this test involves handling of the animals, the experimenter got the rat used to being handled. The reaction latency (i.e., time before withdrawal of the tail from the bath) was measured two-to-three times to obtain two consecutive values that differed by no more than 10%, and respecting an interval of at least 15 min between two measures. The rat’s tail was immediately dried with soft cellulose paper to avoid tail cooling between two measures. A shortened duration of immersion indicated allodynia.
Statistical analysis
Values are expressed as mean ± standard error of the mean (SEM). Differences among experimental groups were determined by one-way analysis of variance (ANOVA) followed by a Tukey test. Qualitative analysis was determined by a Chi-square test. For correlation analysis, Pearson correlation test was used. Differences were considered significant at P < 0.05. The software used was GraphPad Prism, version 5.01 (GraphPad Software, Inc., La Jolla, CA, USA).
Results
Effect of diabetes and l-arginine supplementation on biological and clinical parameters
STZ-induced diabetes induced disturbances in biological and clinical parameters. By the first week after STZ treatment, 50% (20/40) of STZ-treated rats were hyperglycemic, and blood glucose concentration had increased more than fourfold in non-supplemented (5.12 ± 0.22 g/l) and future l-Arg-supplemented STZ-D rats (5.14 ± 0.14 g/l), compared with pre-STZ injection glycaemia values (Fig. 1). Despite a mild decrease in glucose levels on week 2 in l-Arg-supplemented STZ-D rats, high blood glucose levels were maintained throughout the experiment (week 4: 5.71 ± 0.14 and 5.67 ± 0.14 g/l in non-supplemented and l-Arg-supplemented STZ-D rats, respectively). Over 4 weeks of study, control rats maintained glucose levels in a normal range (mean 1.22 ± 0.02 and 1.18 ± 0.02 g/l, weeks 0 and 4, respectively) (Fig. 1).

Time course of glycaemia in non-diabetic (non-D), non-supplemented STZ-diabetic (non-suppl STZ-D), and l-Arg-supplemented diabetic (l-Arg-suppl STZ-D) rats. Values are expressed as mean ± SEM (n = 10 for each group). Statistical analysis was performed by one-way ANOVA followed by a Tukey test. ***P < 0.001 vs. non-D rats; † P < 0.05 vs. non-suppl STZ-D rats
A significant decrease in plasma insulin concentration was observed in non-supplemented STZ-D rats when compared to control rats (−0.32 ± 0.02 µg/l), whereas no significant variation was reported when l-arginine rats were compared to controls and non-supplemented STZ-D rats (Fig. 2).

Insulin plasma concentrations in non-diabetic (non-D), non-supplemented STZ-diabetic (non-suppl STZ-D), and l-Arg-supplemented diabetic (l-Arg-suppl STZ-D) rats. Values are expressed as mean ± SEM (n = 6–8/group). Statistical analysis was performed by one-way ANOVA followed by a Tukey test. *P < 0.05 vs. non-D rats
Water intake in non-supplemented and l-Arg-supplemented STZ-D rats was ten and sevenfold higher, respectively, when compared to control rats. Concerning l-Arg-supplemented STZ-D rats, water intake was significantly lower (−27 ± 5%) than in non-supplemented STZ-D rats (Table 1). This was related with a high urine excretion in non-supplemented (r = 0.89) and l-Arg-supplemented STZ-D rats (r = 0.97). A significant increase of food intake was observed in non-supplemented and l-Arg-supplemented STZ-D rats (+78 ± 12 and +52 ± 8%, respectively) compared with control rats (Table 1). Hence, non-supplemented STZ-D rats presented a significantly higher protein and arginine intakes compared with non-diabetic rats (+148 ± 22% in both variables). In addition, protein intake in l-Arg-supplemented STZ-D rats was significantly higher than in control rats (+154 ± 8%). l-Arg-supplemented STZ-D rats received an additional oral l-arginine supplementation of 3.6 ± 0.3 g/kg/24 h in drinking water and 2.0 ± 0.1 g/kg/24 h in food, for a total dose (food and water content) of 5.6 ± 0.1 g/kg/24 h. The total l-Arg intake corresponds to an increase of 547 ± 15 and 162 ± 6%, respectively, when compared with control rats and non-supplemented STZ-D rats (Table 1).
The kinetic curve of the body weight gain (Fig. 3) shows that the three groups progressed differently over the time of experiment. A sustained weight gain was observed in control rats corresponding to body weight increase of +37 ± 4% at week 4 vs. week 0. In contrast, non-supplemented STZ-D rats did not gain weight which remained the same until the end of treatment (Fig. 3). Supplementation with l-arginine did not prevent body weight arrest, but slightly increased body weight loss from week 2 to week 4, compared to non-supplemented STZ-D rats (−14 ± 3%, at week 4).

Time course of body weight gain in non-diabetic (non-D), non-supplemented STZ-diabetic (non-suppl STZ-D), and l-Arg-supplemented diabetic (l-Arg-suppl STZ-D) rats. Values are expressed as mean ± SEM (n = 10 for each group). Statistical analysis was performed by one-way ANOVA followed by a Tukey test. ***P < 0.001, **P < 0.01 vs. non-D rats; † P < 0.05 vs. non-suppl STZ-D rats
In non-supplemented STZ-D rats, the urine nitrogen excretion was significantly higher than in control rats (+60 ± 11%). l-Arginine supplementation lowered nitrogen excretion (−16 ± 4% compared to non-supplemented STZ-D rats) (Fig. 4).

Urine nitrogen concentrations in non-diabetic (non-D), non-supplemented STZ-diabetic (non-suppl STZ-D), and l-Arg-supplemented diabetic (l-Arg-suppl STZ-D) rats. Values are expressed as mean ± SEM (n = 9–10 for each group). Statistical analysis was performed by one-way ANOVA followed by a Tukey test. ***P < 0.001, *P < 0.05 vs. non-D rats; †† P < 0.01 vs. non-suppl. STZ-D rats
Comparison of nitrogen balance of control and non-supplemented STZ-D rats revealed that there was a greater nitrogen loss in STZ-D rats (2.0 ± 0.1 g/kg) than in non-D rats (0.9 ± 0.1 g/kg), but levels of total amino-acid nitrogen intake were significantly higher in non-supplemented STZ-D than in control rats (5.0 ± 0.5 vs. 2.0 ± 0.1 g/kg) (Table 1). Consequently, the nitrogen balance was found significantly more positive in STZ-D rats (5.0 ± 0.2 g/kg) than in control rats (1.1 ± 0.2 g/kg). Whereas total nitrogen intake of l-Arg-supplemented group increased up to 6.9 ± 0.2 g/kg, nitrogen loss (2.0 ± 0.1 g/kg) did not change and caused a statistical increase in the positive nitrogen balance of l-Arg supplemented STZ-D rats (5.0 ± 0.2 g/kg) compared with non-supplemented STZ-D and control rats (2.9 ± 0.4 and 1.1 ± 0.2 g/kg, respectively).
Effect of diabetes and l-arginine supplementation on plasma NO, arginine, agmatine, and its related amino-acid concentrations
Nitric oxide plasma concentration was significantly increased in non-supplemented STZ-D rats (+69 ± 20%) compared to control rats (Table 2). l-Arginine supplementation normalized plasma NO concentration (Table 2). Agmatine plasma concentration was not different in STZ-D rats (1.11 ± 0.24 µM) compared to non-D rat (0.94 ± 0.20 µM), but was significantly increased in l-arginine supplemented STZ rats (+389 ± 72%, 4.58 ± 0.68 µM) compared to non-D rats. Unexpectedly, plasma arginine concentration was unaffected by diabetes; moreover, lower plasma arginine concentration was observed in l-Arg-supplemented STZ-D rats (−59 ± 4%) when compared to controls. Glutamate plasma concentration was significantly reduced by 57 ± 14%, in non-supplemented STZ-D rats compared to non-diabetic rats (Table 2). Glutamine plasma concentration was significantly lowered in non-supplemented STZ-D rats (−46 ± 2%) and l-Arg-supplemented STZ-D rats (−72 ± 3%). Citrulline plasma concentration was significantly increased in both non-supplemented and l-Arg-supplemented STZ-D rats by 65 ± 19 and 70 ± 18%, respectively, compared to control rats. l-Arginine supplementation was associated with a lowered ornithine plasma concentration compared to control rats (−9 ± 9%), whereas no difference was observed when compared to non-supplemented STZ-D rats (Table 2).
Effect of diabetes and l-arginine supplementation on mechanical thresholds
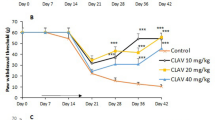
Mechanical nociceptive thresholds did not vary during the 4 week study in non-diabetic rats (Fig. 5). At the second week of study, mechanical hyperalgesia was evident in all the non-supplemented STZ-D rats (−125.1 ± 12.6 g reduction in paw pressure-induced vocalization thresholds) which worsened at week 4 (−209.3 ± 13.4 g). l-Arginine supplementation prevented mechanical hypersensitivity over 4 weeks of study in 80% of rats and only 20% of rats presented a reduction in paw pressure-induced vocalization thresholds (−143.1 ± 26.9 and −163.1 ± 6.9 g at weeks 2 and 4, respectively).

Time course of mechanical sensitivity measured by paw pressure-induced vocalization threshold (VT) variations in non-diabetic (non-D), non-supplemented STZ-diabetic (non-suppl STZ-D), and l-Arg-supplemented diabetic (l-Arg-suppl STZ-D) rats. Results are expressed as mean ± SEM (n = 8–10 for each group). Statistical analysis was performed by one-way ANOVA followed by a Tukey test. ***P < 0.001 vs. non-D rats; ††† P < 0.001, †† P < 0.01 vs. non-suppl. STZ-D rats
Effect of diabetes and l-arginine supplementation on tactile allodynia
Before the administration of STZ or its vehicle, no painful reaction to the application of a non-noxious stimulation of 15.136 g von Frey hair application was observed in any of the three groups studied (Table 3). Four weeks after STZ injection, 60% of the non-supplemented STZ-D rats showed painful reaction characterized by a paw-withdrawal threshold of 8.5 ± 2.3 g. Half of these rats already presented a painful reaction at 2 weeks after STZ injection (mean paw-withdrawal threshold 11.8 ± 1.9 g). When evaluating l-arginine supplementation in STZ-D rats, no withdrawal response to the strongest von Frey filament was observed in all STZ-D supplemented rats during 4 weeks of study. This later indicates that tactile allodynia was totally prevented.
Effect of diabetes and l-arginine supplementation on thermal allodynia
Before the injection of STZ or distilled water, no response occurred during the 15 s application of a non-noxious stimulation (tail immersion in a 42 °C water bath) in the three groups of rats (Table 3). At week 2, a reaction appeared in 60% of the non-supplemented STZ-D rats before the cut-off time (7.3 ± 1.1 s) indicating allodynia. This reaction latency remained the same until the end of the experiment (8.1 ± 0.4 s, at week 4). l-Arginine supplementation totally prevented thermal allodynia in all l-Arg-supplemented STZ-D rats, as demonstrated by the lack of any responses to the warm stimulus throughout the study (reaction latency >15 s at weeks 2 and 4).
Discussion
In the current study, we show that l-arginine supplementation prevents mechanical hyperalgesia, tactile, and thermal allodynia in STZ-induced diabetic neuropathic rats by normalizing NO(x) plasma concentration and increasing agmatine plasma concentration. Oral l-arginine supply also reduced polydipsia, polyuria, urine nitrogen excretion, and slightly limited hypoinsulinemia, but failed to reduce hyperglycemia.
As previously reported [21, 30, 31], the administration of STZ in rats induced an experimental T1DM, with severe hyperglycemia and hypoinsulinemia, polydipsia, polyuria and polyphagia, a blockade in body weight gain, and high urine nitrogen excretion.
No significant variation on plasma insulin concentration in l-Arg-supplemented STZ-D rats compared to STZ-D and controls was observed. This is in concordance with high blood glucose levels observed in l-Arg-supplemented STZ-D rats. Studies have observed that l-arginine supplementation improves insulin sensitivity but not blood glucose levels in patients with T2DM [32]. Other studies have shown a preventive effect of l-arginine supplementation on hyperglygemia in diabetes by improvement of plasma insulin levels and insulin sensitivity [15, 32]. Poor glycemic control, increased glomerular flow rate, and decreased fluid reabsorption may be responsible for polyuria, polydipsia, and polyphagia observed in diabetes [33, 34]. In our study, l-arginine supplementation in STZ-D rats reduced polydipsia and hence polyuria. Despite an anorectic activity reported by nitric oxide synthase inhibitors, such as NG-nitro-l-arginine (l-NO Arg) [35], polyphagia was not prevented but only reduced in l-arginine supplemented STZ-D rats. It resulted in high protein and l-arginine intakes without preventing body weight growth halt. This latter may be related to insulin deficiency, reduced glucose uptake, and altered protein turn over [36, 37]. The reduction of nitrogen excretion resulting from l-arginine supplementation could be related to a reduced body protein catabolism. Accordingly, l-arginine supplementation or infusion was shown to improve protein anabolism and to attenuate muscle protein catabolism [38]. Supporting this, nitrogen balance was more positive in supplemented STZ-D rats than in non-supplemented STZ-D or non-D rats. Performing pair fed studies in rats receiving an isonitrogenous and isocaloric mixture of non-essential amino acids could have allowed to compare more specifically the effect of l-Arg independently of calorie and nitrogen intakes.
Surprisingly, contrary to previous studies reporting a decrease of plasmatic level of l-arginine in diabetic rats [39, 40] and humans [41], we found that l-arginine plasma concentration in non-supplemented STZ-D rats was similar to that of control rats and that of l-Arg supplemented rats was reduced by half. In addition, the plasma level of citrulline, the immediate precursor of l-arginine, was increased by almost twofold in both non-supplemented and l-Arg supplemented diabetic rats. Consequently, the ratio l-arginine/citrulline was 2.3, 1.3, and 0.5 in control rats, non-supplemented and l-Arg supplemented STZ-D rats, respectively. This later suggest that, in such conditions of diabetes and arginine supplementation, either enzyme activities involved in l-arginine synthesis are altered or that l-arginine is over metabolized and enters in another metabolic pathways.
In the present study, plasma citrulline concentration was higher in non-supplemented STZ-D rats than in controls as recently reported [42], as well as plasma NO(x) levels, previously found to be either increased [43] or decreased [44, 45] in diabetic patients and diabetic animals. In addition, the plasma level of l-ornithine remained unchanged, suggesting that l-arginine metabolism in non-supplemented STZ-D rats is directed principally to activation of the NOS pathway resulting in an increased citrulline and NO production. Indeed, it is known that many cell types utilize arginine to generate NO.
In l-Arg-supplemented STZ-D rats, plasma levels of l-arginine as well as the ratio l-arginine/citrulline are lower than in control or non-supplemented STZ-D rats. This was accompanied by changes in arginine metabolites: low glutamine and ornithine and high citrulline plasma concentrations without variations in glutamate plasma level. Results from pharmacokinetic studies in healthy or hypercholesterolemic subjects indicate that arginine, administered either i.v. or orally, is cleared rapidly from the circulation [46, 47]. Low plasma arginine levels may indicate, among other, that arginine-dependent pathways and metabolism can be disturbed in both pathological (diabetes) and increased arginine intake condition [48]. We hypothesize that in diabetic rats under arginine supplementation, arginine metabolism is directed to agmatine synthesis via arginine decarboxylase activation, since other metabolites derived from arginine are increased (agmatine), reduced (ornithine), or normalized (NO). Indeed, we found that l-arginine supplementation not only normalized NO(x) plasma concentrations as previously reported [40], but also increased by almost fivefold plasma levels of agmatine in STZ-diabetic rats. Consequently, we assume that agmatine resulting from arginine decarboxylation is able to compete with NO synthesis, as previously reported [49, 50].
Diabetes-induced neuropathic pain is due to primary dysfunction of peripheral nociceptive, as well as non-nociceptive nerves, associated with neuroplastic changes responsible for sensitization of spinal processing (central pain), thereby causing persistent hyperalgesia and/or allodynia [51]. In the present study, diabetic rats developed mechanical hyperalgesia, tactile, and thermal allodynia with some variability in the kinetics of onset and the proportion of painful animals. First, the sensitization of small (C)- and medium (delta)-diameter fibres which are responsible for mechanical hyperalgesia and thermal allodynia occurs more rapidly [52,53,54] than mechanisms responsible for tactile allodynia. Second, STZ-induced diabetes resulted in variability in tactile allodynia onset between subjects. Only 30% of diabetic rats presented an aversive reaction to non-painful tactile stimulation at the second week of diabetes and 60% at the fourth week of diabetes suggesting different mechanisms than those underlying mechanical hyperalgesia and thermal allodynia. Indeed, more than the frequency firing of C-fibres to stimulus application, it is the reduction of conduction failure of high-fire-frequency polymodal C-fibres (an intrinsic self-inhibition mechanism known to modulate pain processing) that may underlie tactile allodynia [55]. Development and maintenance of thermal hyperalgesia [56] as well as mechanical hyperalgesia [57] have been previously related to NO synthesis. Here, non-supplemented STZ-D rats presented high citrulline and NO(x) plasma concentrations which may indicate high activity of NOS and consequently NO synthesis, coinciding with pronounced signs of mechanical hyperalgesia, thermal, and tactile allodynia.
Arginine is a common precursor, of NO and agmatine, displaying pronociceptive and antinociceptive effects, respectively. In this study, l-arginine supplementation normalized NO plasma concentration and rescued normal pain sensation in 100 and 80% of diabetic rats. This suggests that arginine supplementation in diabetes may be directed to the synthesis of agmatine, impairing NO production. Decarboxylated arginine has shown to reduce pain associated behaviors in rodent models of neuropathic and inflammatory pain [22, 58, 59]. Similarly, it was shown that intravenous administration of l-arginine induced a dose-dependent analgesic effect in patients with persistent pain [60].
In conclusion, our data indicate that l-arginine supplementation prevents mechanical hyperalgesia, tactile, and thermal allodynia in painful diabetic neuropathy. The lack of effect of oral l-arginine supplementation on glycemia and weight loss suggests that prevention of allodynia and hyperalgesia is more likely due to the normalization of plasma NO(x) concentration which may modulate spinal pain processing than to peripheral metabolic effects. Thus, in diabetes, l-arginine oral supplementation may be an original therapeutic alternative, free of major side effects to prevent the onset of neuropathic pain.
References
Tavakoli M, Mojaddidi M, Fadavi H, Malik RA (2008) Pathophysiology and treatment of painful diabetic neuropathy. Curr Pain Headache Rep 12:192–197
Said G (2007) Diabetic neuropathy—a review. Nat Clin Pract Neurol 3:331–340. doi:10.1038/ncpneuro0504
Wu EQ, Borton J, Said G, Le TK, Monz B, Rosilio M, Avoinet S (2007) Estimated prevalence of peripheral neuropathy and associated pain in adults with diabetes in France. Curr Med Res Opin 23:2035–2042. doi:10.1185/030079907X210516
Halawa MR, Karawagh A, Zeidan A, Mahmoud AE, Sakr M, Hegazy A (2010) Prevalence of painful diabetic peripheral neuropathy among patients suffering from diabetes mellitus in Saudi Arabia. Curr Med Res Opin 26:337–343. doi:10.1185/03007990903471940
Sadosky A, McDermott AM, Brandenburg NA, Strauss M (2008) A review of the epidemiology of painful diabetic peripheral neuropathy, postherpetic neuralgia, and less commonly studied neuropathic pain conditions. Pain Pract 8:45–56. doi:10.1111/j.1533-2500.2007.00164.x
Attal N, Bouhassira D (2015) Pharmacotherapy of neuropathic pain: which drugs, which treatment algorithms? Pain 156(Suppl 1):S104–S114. doi:10.1097/01.j.pain.0000460358.01998.15
Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R, Dworkin RH, Gilron I, Haanpaa M, Hansson P, Jensen TS, Kamerman PR, Lund K, Moore A, Raja SN, Rice AS, Rowbotham M, Sena E, Siddall P, Smith BH, Wallace M (2015) Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol 14:162–173. doi:10.1016/S1474-4422(14)70251-0
Finnerup NB, Sindrup SH, Jensen TS (2010) Recent advances in pharmacological treatment of neuropathic pain. F1000 Med Rep 2:52. doi:10.3410/M2-52
Sang CN, Bennett GJ (2009) Novel therapies for the control and prevention of neuropathic pain. Neurotherapeutics 6:607–608. doi:10.1016/j.nurt.2009.08.004
Pieper GM, Siebeneich W (1997) Diabetes-induced endothelial dysfunction is prevented by long-term treatment with the modified iron chelator, hydroxyethyl starch conjugated-deferoxamine. J Cardiovasc Pharmacol 30:734–738
Wu G, Morris SM (2004) Arginine metabolism in mammals. In: Cynober LA (ed) Metabolic and therapeutic aspects of amino acids in clinical nutrition. CRC Press, Boa Raton, pp 153–167
Raghavan SA, Dikshit M (2004) Vascular regulation by the l-arginine metabolites, nitric oxide and agmatine. Pharmacol Res 49:397–414. doi:10.1016/j.phrs.2003.10.008
Reyes AA, Karl IE, Klahr S (1994) Role of arginine in health and in renal disease. Am J Physiol 267:F331–F346
Wu G, Morris SM Jr (1998) Arginine metabolism: nitric oxide and beyond. Biochem J 336(Pt 1):1–17
Flynn NE, Meininger CJ, Haynes TE, Wu G (2002) The metabolic basis of arginine nutrition and pharmacotherapy. Biomed Pharmacother 56:427–438
Blantz RC, Satriano J, Gabbai F, Kelly C (2000) Biological effects of arginine metabolites. Acta Physiol Scand 168:21–25
Luiking YC, Engelen MP, Deutz NE (2010) Regulation of nitric oxide production in health and disease. Curr Opin Clin Nutr Metab Care 13:97–104. doi:10.1097/MCO.0b013e328332f99d
Bennett GJ (2000) Update on the neurophysiology of pain transmission and modulation: focus on the NMDA-receptor. J Pain Symptom Manag 19:S2–S6
Malcangio M, Tomlinson DR (1998) A pharmacologic analysis of mechanical hyperalgesia in streptozotocin/diabetic rats. Pain 76:151–157
Daulhac L, Maffre V, Mallet C, Etienne M, Privat AM, Kowalski-Chauvel A, Seva C, Fialip J, Eschalier A (2011) Phosphorylation of spinal N-methyl-d-aspartate receptor NR1 subunits by extracellular signal-regulated kinase in dorsal horn neurons and microglia contributes to diabetes-induced painful neuropathy. Eur J Pain 15:169 e112–169 e161. doi:10.1016/j.ejpain.2010.06.003
Rondon LJ, Privat AM, Daulhac L, Davin N, Mazur A, Fialip J, Eschalier A, Courteix C (2010) Magnesium attenuates chronic hypersensitivity and spinal cord NMDA receptor phosphorylation in a rat model of diabetic neuropathic pain. J Physiol 588:4205–4215. doi:10.1113/jphysiol.2010.197004
Courteix C, Privat AM, Pelissier T, Hernandez A, Eschalier A, Fialip J (2007) Agmatine induces antihyperalgesic effects in diabetic rats and a superadditive interaction with R(−)-3-(2-carboxypiperazine-4-yl)-propyl-1-phosphonic acid, a N-methyl-d-aspartate-receptor antagonist. J Pharmacol Exp Ther 322:1237–1245. doi:10.1124/jpet.107.123018
Zimmermann M (1983) Ethical guidelines for investigations of experimental pain in conscious animals. Pain 16:109–110
Skogerboe KJ, Labbe RF, Rettmer RL, Sundquist JP, Gargett AM (1990) Chemiluminescent measurement of total urinary nitrogen for accurate calculation of nitrogen balance. Clin Chem 36:752–755
Green LC, Wagner DA, Glogowski J, Skipper PL, Wishnok JS, Tannenbaum SR (1982) Analysis of nitrate, nitrite, and [15N]nitrate in biological fluids. Anal Biochem 126:131–138
Schmidt HH, Warner TD, Ishii K, Sheng H, Murad F (1992) Insulin secretion from pancreatic B cells caused by l-arginine-derived nitrogen oxides. Science (New York, NY) 255:721–723
Fekkes D (1996) State-of-the-art of high-performance liquid chromatographic analysis of amino acids in physiological samples. J Chromatogr B Biomed Appl 682:3–22
Farges MC, Berard MP, Raul F, Cezard JP, Joly B, Davot P, Vasson MP, Cynober L (1999) Oral administration of a glutamine-enriched diet before or after endotoxin challenge in aged rats has limited effects. J Nutr 129:1799–1806
Randall LO, Selitto JJ (1957) A method for measurement of analgesic activity on inflamed tissue. Arch Int Pharmacodyn Ther 111:409–419
Courteix C, Eschalier A, Lavarenne J (1993) Streptozocin-induced diabetic rats: behavioural evidence for a model of chronic pain. Pain 53:81–88
El-Lithy GM, El-Bakly WM, Matboli M, Abd-Alkhalek HA, Masoud SI, Hamza M (2016) Prophylactic l-arginine and ibuprofen delay the development of tactile allodynia and suppress spinal miR-155 in a rat model of diabetic neuropathy. Transl Res J Lab Clin Med 177(85–97):e81. doi:10.1016/j.trsl.2016.06.005
Piatti PM, Monti LD, Valsecchi G, Magni F, Setola E, Marchesi F, Galli-Kienle M, Pozza G, Alberti KG (2001) Long-term oral l-arginine administration improves peripheral and hepatic insulin sensitivity in type 2 diabetic patients. Diabetes Care 24:875–880
Hans CP, Chaudhary DP, Bansal DD (2003) Effect of magnesium supplementation on oxidative stress in alloxanic diabetic rats. Magnes Res 16:13–19
Ward DT, Yau SK, Mee AP, Mawer EB, Miller CA, Garland HO, Riccardi D (2001) Functional, molecular, and biochemical characterization of streptozotocin-induced diabetes. J Am Soc Nephrol 12:779–790
Squadrito F, Calapai G, Cucinotta D, Altavilla D, Zingarelli B, Ioculano M, Urna G, Sardella A, Campo GM, Caputi AP (1993) Anorectic activity of NG-nitro-l-arginine, an inhibitor of brain nitric oxide synthase, in obese Zucker rats. Eur J Pharmacol 230:125–128
Rodriguez T, Alvarez B, Busquets S, Carbo N, Lopez-Soriano FJ, Argiles JM (1997) The increased skeletal muscle protein turnover of the streptozotocin diabetic rat is associated with high concentrations of branched-chain amino acids. Biochem Mol Med 61:87–94
Lariviere F, Kupranycz DB, Chiasson JL, Hoffer LJ (1992) Plasma leucine kinetics and urinary nitrogen excretion in intensively treated diabetes mellitus. Am J Physiol 263:E173–E179
Bruins MJ, Soeters PB, Lamers WH, Deutz NE (2002) l-Arginine supplementation in pigs decreases liver protein turnover and increases hindquarter protein turnover both during and after endotoxemia. Am J Clin Nutr 75:1031–1044
Brosnan JT, Man KC, Hall DE, Colbourne SA, Brosnan ME (1983) Interorgan metabolism of amino acids in streptozotocin-diabetic ketoacidotic rat. Am J Physiol 244:E151–E158
Kohli R, Meininger CJ, Haynes TE, Yan W, Self JT, Wu G (2004) Dietary l-arginine supplementation enhances endothelial nitric oxide synthesis in streptozotocin-induced diabetic rats. J Nutr 134:600–608
Grill V, Bjorkman O, Gutniak M, Lindqvist M (1992) Brain uptake and release of amino acids in nondiabetic and insulin-dependent diabetic subjects: important role of glutamine release for nitrogen balance. Metabolism 41:28–32
Jabecka A, Ast J, Bogdaski P, Drozdowski M, Pawlak-Lemaska K, Cielewicz AR, Pupek-Musialik D (2012) Oral l-arginine supplementation in patients with mild arterial hypertension and its effect on plasma level of asymmetric dimethylarginine, l-citruline, l-arginine and antioxidant status. Eur Rev Med Pharmacol Sci 16:1665–1674
Chien WY, Yang KD, Eng HL, Hu YH, Lee PY, Wang ST, Wang PW (2005) Increased plasma concentration of nitric oxide in type 2 diabetes but not in nondiabetic individuals with insulin resistance. Diabetes Metab 31:63–68
Ghosh A, Sherpa ML, Bhutia Y, Pal R, Dahal S (2011) Serum nitric oxide status in patients with type 2 diabetes mellitus in Sikkim. Int J App Basic Med Res 1:31–35
Vural P, Cevik A, Curgunlu A, Canbaz M (2002) Effects of diabetes mellitus and acute hypertension on plasma nitric oxide and endothelin concentrations in rats. Clin Chim Acta 320:43–47
Boger RH, Bode-Boger SM (2001) The clinical pharmacology of l-arginine. Annu Rev Pharmacol Toxicol 41:79–99. doi:10.1146/annurev.pharmtox.41.1.79
Tangphao O, Chalon S, Moreno H Jr, Hoffman BB, Blaschke TF (1999) Pharmacokinetics of l-arginine during chronic administration to patients with hypercholesterolaemia. Clin Sci (Lond) 96:199–207
Wu G, Bazer FW, Davis TA, Kim SW, Li P, Marc Rhoads J, Carey Satterfield M, Smith SB, Spencer TE, Yin Y (2009) Arginine metabolism and nutrition in growth, health and disease. Amino Acids 37:153–168. doi:10.1007/s00726-008-0210-y
Piletz JE, Aricioglu F, Cheng JT, Fairbanks CA, Gilad VH, Haenisch B, Halaris A, Hong S, Lee JE, Li J, Liu P, Molderings GJ, Rodrigues AL, Satriano J, Seong GJ, Wilcox G, Wu N, Gilad GM (2013) Agmatine: clinical applications after 100 years in translation. Drug Discov Today. doi:10.1016/j.drudis.2013.05.017
Raasch W, Regunathan S, Li G, Reis DJ (1995) Agmatine, the bacterial amine, is widely distributed in mammalian tissues. Life Sci 56:2319–2330
Todorovic SM (2016) Painful diabetic neuropathy: prevention or suppression? Int Rev Neurobiol 127:211–225. doi:10.1016/bs.irn.2016.03.005
Behse F, Buchthal F, Carlsen F (1977) Nerve biopsy and conduction studies in diabetic neuropathy. J Neurol Neurosurg Psychiatry 40:1072–1082
Bischoff A (1980) Morphology of diabetic neuropathy. Horm Metab Res Suppl 9:18–28
Said G (1983) Etiology of peripheral neuropathies. Presse Med 12:669–671
Sun W, Miao B, Wang XC, Duan JH, Wang WT, Kuang F, Xie RG, Xing JL, Xu H, Song XJ, Luo C, Hu SJ (2012) Reduced conduction failure of the main axon of polymodal nociceptive C-fibres contributes to painful diabetic neuropathy in rats. Brain J Neurol 135:359–375. doi:10.1093/brain/awr345
Malmberg AB, Yaksh TL (1993) Spinal nitric oxide synthesis inhibition blocks NMDA-induced thermal hyperalgesia and produces antinociception in the formalin test in rats. Pain 54:291–300
Meller ST, Cummings CP, Traub RJ, Gebhart GF (1994) The role of nitric oxide in the development and maintenance of the hyperalgesia produced by intraplantar injection of carrageenan in the rat. Neuroscience 60:367–374
Fairbanks CA, Schreiber KL, Brewer KL, Yu CG, Stone LS, Kitto KF, Nguyen HO, Grocholski BM, Shoeman DW, Kehl LJ, Regunathan S, Reis DJ, Yezierski RP, Wilcox GL (2000) Agmatine reverses pain induced by inflammation, neuropathy, and spinal cord injury. Proc Natl Acad Sci USA 97:10584–10589
Horvath G, Kekesi G, Dobos I, Szikszay M, Klimscha W, Benedek G (1999) Effect of intrathecal agmatine on inflammation-induced thermal hyperalgesia in rats. Eur J Pharmacol 368:197–204
Harima A, Shimizu H, Takagi H (1991) Analgesic effect of l-arginine in patients with persistent pain. Eur Neuropsychopharmacol 1:529–533
Acknowledgements
The authors wish to thank Eric Chapuy for his technical assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Rondón, L.J., Farges, M.C., Davin, N. et al. l-Arginine supplementation prevents allodynia and hyperalgesia in painful diabetic neuropathic rats by normalizing plasma nitric oxide concentration and increasing plasma agmatine concentration. Eur J Nutr 57, 2353–2363 (2018). https://doi.org/10.1007/s00394-017-1508-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-017-1508-x