
Abstract
Gout and calcium pyrophosphate deposition disease (CPPD, pseudogout) are still the most frequent inflammatory arthritides in multimorbid elderly patients. Gout and CPPD are different diseases and based on different pathophysiological principles. Gout is closely associated with the metabolic syndrome and is an independent risk factor for cardiovascular mortality. The prevalence of asymptomatic hyperuricemia is estimated to be 10–20% of adults in industrial nations and prevalence is strongly associated with age. More than 7% of persons aged over 65 years suffer from clinically manifest gout. The underlying pathophysiological principle is an imbalance between the formation and elimination of uric acid. The degradation of the purine bases adenine and guanosine to uric acid is catalysed by xanthine oxidase and genetic polymorphisms and mutations play an important role in absorption and excretion processes. Furthermore, carrier proteins, such as URAT-1 or OAT-4 also have an influence on these processes. An imbalance of the physiological processes results in the solubility product being exceeded, which in consequence leads to crystallization of urate. This induces a cascade of massive inflammatory reactions at the molecular and cellular level with the activation of cytokines. The inflammatory process can be stopped by neutrophil extracellular traps (NETs) that modulate aggregation and degradation of chemokines and cytokines and partitioning of crystallized urate against immune cells. Calcium pyrophosphate dehydrate (CPP) crystals are formed in the cartilage and CPP deposition can be found in 30% of people aged over 80 years. Inorganic pyrophosphate (PPi) is synthesized in chondrocytes and plays an important part in the formation of calcium pyrophosphate crystals. The degradation is catalyzed by inorganic pyrophosphatases. If there is dysregulation of this homeostasis more PPi is produced, which ultimately contributes to the formation of the CPP crystals.
Zusammenfassung
Die Gicht und die Kalziumpyrophosphat-Arthritis (CPPD, Pseudogicht) stellen die häufigsten entzündlichen Gelenkerkrankungen des älteren multimorbiden Patienten dar. Diese beiden Erkrankungen beruhen auf verschiedenen pathophysiologischen Prinzipien. Die Gicht ist eng mit dem metabolischen Syndrom verknüpft und stellt einen eigenständigen Risikofaktor für die kardiovaskuläre Mortalität dar. Die Prävalenz einer asymptomatischen Erhöhung der Harnsäure im Serum wird in den Industrieländern auf 10–20 % der Erwachsenen geschätzt, und die Prävalenz der klinisch manifesten Gicht stark abhängig vom Lebensalter. Bei den über 65-jährigen leiden über 7 % an einer Gicht. Pathophysiologisch liegt einer Gicht ein Ungleichgewicht aus Harnsäureentstehung und Elimination zugrunde. Der Abbau der Purinbasen Adenin und Guanosin zur Harnsäure wird über die Xanthinoxidase katalysiert. Hierbei spielen zahlreiche genetische Polymorphismen und Genmutationen sowie Transportproteine wie URAT-1 oder (OAT)-4 bei den Resorptions- und Exkretionsvorgängen eine wichtige Rolle. Kommt es durch ein Ungleichgewicht der physiologischen Abläufe zur Überschreitung des Löslichkeitsproduktes, folgt eine Kristallisation von Urat. Diese führt zu einer fulminanten, kaskadenförmig ablaufenden Entzündungsreaktion auf molekularer und zellulärer Ebene. Die massive Aktivierung des angeborenen und erworbenen Immunsystems kann durch extrazelluläre „neutrophil extracellular traps“ (NETs) mit Aggregation und Degradation von Chemo- und Zytokinen, sowie Abschirmung der Harnsäurekristalle gegenüber Immunzellen beendet werden. Kalziumpyrophosphatdihydrat-Kristalle werden im Knorpel gebildet. Ablagerungen finden sich bei 30 % der über 80-Jährigen. Für die Bildung der Kalziumpyrophosphat-Kristalle spielt besonders das anorganische Pyrophosphat (PPi) eine Rolle, das in den Chondrozyten gebildet wird. Der Abbau wird durch anorganische Pyrophosphatasen katalysiert. Kommt es zu einer Dysregulation der Homöostase, wird vermehrt PPi gebildet, was eine pathologische Ablagerung von CPPD-Kristallen zur Folge hat.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Gout is one of the oldest diseases documented in humans. It was described by the Egyptians in 2640 B.C. Hippocrates later called it the arthritis of the rich due to its increased association with excessive binges of alcohol and food [20]; however, gout is a disease that remains underestimated and undertreated up to the present day. The aim of this three-part review is to consider the pathogenesis, clinical features and diagnosis and treatment of gout and calcium pyrophosphate arthritis in detail, emphasizing its special features in elderly persons.
Epidemiology
In the General Practice Research Database (GPRD), a large epidemiological study, gout prevalence was shown to depend highly on age. The prevalence in men in the 35–44 years age group is about 1% but prevalence increases to over 7% in the over 65 years age group [25]. Furthermore, a similar rise in incidence was found with 11 cases (95% confidence interval CI 9.9–12.5) in the under 44 years age group and 53 (95% CI 49–57.9) in the over 65-year-olds per 10,000 patient years [25]. The prevalence of hyperuricemia, i. e., a serum urate level above the reference range of 2.3–6.1 mg/dl (137–363 µmol/l) in adult women and 3.6–8.2 mg/dl (214–488 µmol/l) in men, is approximately 10–20% of all adults [12]. Men predominate with a ratio of 3–4:1 [35] and other authors report even higher predominance in men with a ratio of 7:1–9:1 compared with women [1, 42]. The risk of developing significant hyperuricemia in a 5-year period (cumulative gout incidence per 1000 patient years) depends on sex and increases with the urate level. If the risk corresponding to a serum urate level ≥8 mg/dl is considered over 5 years, this is only 4.8 (95% CI 2.4–9.5) in men and 2.3 (95% CI 0.9–5.6) in women [2]; however, if the urate range of 9–9.9 mg/dl is considered, the cumulative incidence is over 20% and over 30% at a level of over 10 mg/dl [35]. This association will be discussed in conjunction with consideration of the indications for treatment of hyperuricemia (see the continuation of this series). Gout has now been identified as an independent risk factor for increased cardiovascular mortality, as summarized in a table in the review by Roddy and Doherty [35]. It was shown in a meta-analysis by Kim et al. that the association of hyperuricemia and cardiovascular events due to coronary heart disease (CHD) is independent of traditional risk factors for CHD [17]; however, the association, although significant, can be regarded as moderate. It was apparent in subgroup analyses that women have a significantly raised risk for a cardiovascular event, whereas men do not exhibit increased mortality. The urate level above which there is actually an increased cardiovascular risk is still unclear. Evidence is increasing that initiation of uric acid-lowering treatment, e. g., by allopurinol, can reduce both the mortality risk and blood pressure [14, 19]. The level that the uric acid should be lowered to in order to reduce the cardiovascular risk is currently unclear. Possibly, the association of gout with cardiovascular mortality is stronger than hyperuricaemia alone [18].
Predisposing factors reported for gout include alimentary factors [35] and osteoarthritis of different joints [22]. Previously damaged joints appear to predispose to urate crystal precipitation with a consequent gout attack. This is possibly based on the observation that deposits of calcium pyrophosphate dihydrate (CPP deposition) occur in aging hyaline and fibrous cartilage. If CPPD crystals get into the free joint cavity, inflammation of varying intensity may occur, with clinical features like those of gout with urate crystals. A possible explanation would be that milder undulating inflammation associated with CPPD lowers the pH in the synovial fluid, further reducing the solubility of urate. Therefore, CPPD-associated acute joint inflammation is also called pseudogout or activated osteoarthritis. The prevalence of deposits of CPPD crystals in cartilage is reported to increase with age from 15% in over 60-year-olds to up to 30% in over 80-year-olds [22]. Gout and pseudogout or CPPD are thus the most common inflammatory joint diseases in elderly (multimorbid) patients and present the treating physician with a complex differential treatment challenge, especially with regard to the frequently impaired renal function, hypertension, diabetic metabolic status, vascular morbidity and heart failure.
Pathophysiology of gout
Uric acid crystals were first described as a gout-associated pathogenetic substrate by Max Freudweiler in 1899. In 1961 Jarvis Edwin Seegmiller demonstrated that the uric acid crystals trigger inflammation in gout [20]. With the introduction of the xanthine oxidase inhibitor allopurinol in 1965, it was mistakenly believed initially that the pathophysiology of gout had been fully elucidated and that gout had finally been conquered. In recent years, new knowledge in genetics and immunology has led to better understanding of the underlying pathophysiological mechanisms of gout.
Uric acid production and elimination
Uric acid is the degradation product of the purine bases adenine and guanine; it is increased either endogenously with cell destruction (fragile tumor cells, trauma and fasting diets) or exogenously due to unbalanced consumption of, e. g. sausage, offal, rinds, crustaceans, certain types of fish (e.g. sardines, anchovies and herrings),and also brassica vegetables and legumes. Moreover, increased alcohol and fructose consumption can contribute to hyperuricemia because of an interaction with adenine metabolism [7]. The key enzyme xanthine oxidase catalyzes the final steps in the biochemical degradation of adenine and guanine to uric acid. Humans lost the uricase gene, which converts uric acid into the much more water soluble allantoin, some 45 million years ago. One of the evolutionary advantages for humans could be a water-saving effect when excreting toxic nitrogen from DNA. Nowadays, with unlimited liquid available, injection of uricase is used to treat severe tophaceous gout; however, the effect of uric acid as an in vivo adjuvant in cells dying non-apoptotically appears much more important. The uric acid concentration in the cytosol is approximately 4 mg/ml. During cell destruction, DNA and RNA are degraded locally so local supersaturation can occur with crystallization of uric acid. This leads to activation of the inflammasome, a cytosol protein complex in neutrophils and macrophages. Following activation, it induces a series of reactions that culminates in activation of caspase-1, which in turn leads to activation of interleukin-1 beta, which is secreted by macrophages and triggers an inflammatory reaction. This stimulation of the innate and adaptive immune system leads to effective clearing away of the detritus [4]; however, autoimmunity can also develop in this context on account of the activation of the adaptive immune system [39].
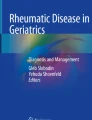
Under physiological conditions, roughly 350 mg of uric acid are produced daily by endogenous catabolism or as a result of food metabolism. About two thirds of the uric acid are excreted through the kidneys and one third via the bowels (Fig. 1). The serum uric acid level is determined by the balance between absorption and secretion of uric acid in the proximal renal tubules [7, 34, 40]. This principle utilizes newer treatment strategies, which will be discussed in the second part of this series. Numerous single nucleotide polymorphisms (SNPs) have been described for both absorption and secretion transporters [43]. In a recent review article, current knowledge of the genetics of hyperuricemia and gout was succinctly summarized [33]; however, the genetic variations can explain less than 6% of cases of hyperuricemia and gout. The serum uric acid continues to be the best predictor for the risk of developing gout. To understand the principle of uric acid regulation, some clinically relevant transport proteins will be emphasized. At the molecular level, urate anion transporter (URAT)-1 and organic anion transporter (OAT)-4 located luminally in the kidneys play a crucially important role in the reabsorption process [33]. Moreover, OAT-4 is induced by thiazide diuretics so it can contribute to the hyperuricemia that occurs with diuretic therapy through increased tubular reabsorption [41]. URAT-1 is inhibited by the uricosuric agents probenecid and benzbromarone, which leads to increased renal excretion of uric acid; however, URAT-1 can also be partially inhibited by medications such as low-dose acetylsalicylic acid and cyclosporine [27]. Genetic polymorphisms of the highly efficient ATP-binding cassette transporter G2 (ABCG2) [35] are found in approximately10% of Caucasians, leading to a 75% reduction in uric acid excretion by both the renal and gastrointestinal routes [24]. If less uric acid is excreted through the bowels, the serum uric acid level rises, which can lead to renal overloading and hence to hyperuricemia [23].

Purine metabolic pathway – humans, monkey species and birds have no uricase. Renal expression of ATP-binding cassette subfamily G 2 (ABCG2), urate anion transporter 1 (URAT-1) and organic anion transporter 4 (OAT4) is increased by diuretics + (green) promotes uric acid excretion, − (red) inhibits uric acid excretion through reabsorption (copyright: Peter Härle)
On the other hand, gene mutations that lead to loss of function of tubular reabsorption transporters result in increased excretion and therefore a reduction of serum uric acid. Mutations in the SLC2A9 and SCL22A12 genes should be mentioned, which code for GLUT-2 and URAT-1 transport proteins, respectively, leading to hypouricemia in different populations [37]; however, as a consequence, renal failure and renal urate calculi occur more in these patients due to elevated uric acid concentrations in the urine [37]. The GLUT-2 transporter is also regarded as a fructose–uric acid transporter and thus might reabsorb less uric acid because of competition when tubular fructose concentrations are high [33]. Elevated fructose concentrations in the urine would then have a uricosuric effect. These uricosuric effects of tubular fructose contrast with the epidemiologic association with the hyperuricemia-promoting influence of foods high in fructose, as shown in a prospective cohort study [6]. The fructose-gout causal link has to date been explained by classical biochemistry: in brief, the increased consumption and intracellular metabolism of fructose leads to depletion of inorganic phosphate and therefore to a relative surplus of adenosine monophosphate, which is then metabolized to uric acid through inosine monophosphate, causing an increased amount of this [8].
Increased alcohol consumption, even 10–14.9 g per day (0.3 l beer or 125 ml wine or 2 measures of spirits) is a risk factor for gout. On the one hand, less uric acid is excreted due to the degradation of ethanol to acetate competitively on the URAT-1/OAT4 transport protein in the proximal tubules of the kidneys. On the other hand, more acetyl-CoA is produced through the breakdown of ethanol, which leads to increased consumption and breakdown of adenosine triphosphate and thus can explain a rising uric acid level [5]. Interestingly, various alcoholic drinks differ with respect to the hyperuricemic effect. Because of the high DNA content of yeast (especially guanosine), beer drinking is associated with a higher risk compared with spirits. Consumption of wine, however, appears to have little or no effect on the rise in uric acid [5].
In summary, it is apparent that the equilibrium between uric acid production and excretion, genetic mutations of the different absorption and excretion transport proteins and also diet decide whether hyperuricemia will occur and possibly overt gout when the serum uric acid level is persistently elevated above the solubility limit. It is not possible to explain the pathophysiology of gout by considering any of these factors in isolation.
Uric acid precipitation and gout attack
In physicochemical terms, the solubility of uric acid in blood and tissue is decisive for the development of gout. The pathogenic monosodium urate crystals only form when the solubility product is exceeded. At normal body temperature and physiological pH, this can occur above a uric acid concentration of approximately 7 mg/dl (0.4 mmol/l) [34]. At lower body temperatures or pH in the acid range, the solubility product for monosodium urate is much lower. This also explains the particular danger for the extremities (lower body temperature, poorer perfusion) and arthritic joints (lower pH, CPPD deposits) as the site of predilection for gout [38]. In addition to the aforementioned factors, other unknown factors that inhibit or promote crystal formation are probably also important for urate crystallization. Finally, it has been known since the nineteenth century that deposits of urate in tissues and joints can be clinically asymptomatic. In recent years, this has again become important in the discussion of gout stages.
In general, crystals are identified as foreign bodies by the innate immune system through membrane receptors so they cause an inflammatory reaction that varies in strength. This principle is not restricted only to urate crystals, even if uric acid crystals have the greatest inflammatory potency of all crystals. Urate crystals, CPP crystals, basic calcium phosphate (BCP), octa calcium phosphate (OCP) in joints and tissues, and also cholesterol crystals as part of the arteriosclerosis process in vessel walls (Fig. 2) can lead to inflammation [9, 32]. Both toll-like receptors [28] and direct interaction of urate crystals with cholesterol components of the cell membrane appear to trigger cascade-like intracellular signals, which finally activate the NALP3 inflammasome. This results in activation of interleukin-1 (IL-1) converting enzyme (a caspase), which converts the inactive form of IL-1 beta and IL-18 to the active form. These cytokines are released from the immune cell and, via specific membrane cytokine receptors, they activate proinflammatory signal transduction pathways through NF-kB and MAP kinase. The result is massive activation of the innate and acquired immune system.

The figure shows in the first line the purely medical evidence in green, hyperuricemia, calcinosis of hyaline or fibrous cartilage (chondrocalcinosis), osteoarthritis with loss of cartilage with the possibility of bone erosion (BCP), and hypercholesterinemia. Under certain biological circumstances the medical evidence converts into a state, such that danger receptors are stimulated (second line in yellow). Danger receptors are receptors which recognize danger-associated molecular pattern molecules (DAMPs) from the host which are able to initiate and perpetuate a noninfectious inflammatory response. Toll-like receptors (TLRs) can function as danger receptors. This happens under conditions of urate crystal formation, CPP (calcium pyrophosphate), BCP (basic calcium phosphate) and derivatives, cholesterol crystals getting in contact with immune cells and then causing disease, e. g. gout, CPPD, activated osteoarthritis caused by BCP crystals, and atherosclerosis, which are depicted in red. All these processes lead to the same final common pathway, that is inflammation as shown in the last line of the figure in black. (Copyright: Peter Härle)
Since the urate crystals cannot dissolve spontaneously and can also be detected in the intercritical stage of gout, the question arises as to the mechanisms that terminate the gout attack. Recent data have shown that urate crystals provoke the production of neutrophil extracellular traps (NETs) by neutrophilic granulocytes [26]. NETs consist of chromatin elements and various proteins [3, 31] and can terminate the massive immunostimulation in the gout attack through aggregation and degradation of chemokines and cytokines and shielding of the uric acid crystals from immune cells [28, 37].
Pathophysiology of calcium pyrophosphate arthritis (CPPD)
Unlike uric acid crystals, which occur only when the solubility product in synovial fluid is exceeded, calcium pyrophosphate dihydrate (CPP) crystals are formed in the cartilage close to the surface of the chondrocytes. These cells are embedded in the collagen and proteoglycan-containing matrix. Inorganic pyrophosphate (PPi) in particular plays an important part in the formation of calcium pyrophosphate crystals. Chondrocytes are able to produce PPi enzymatically from ATP and other nucleoside triphosphatases. This is mediated by a number of enzymes with nucleoside triphosphatase pyrophosphohydrolase activity (NTPPPH), such as nucleotide pyrophosphatase/phosphodiesterase (NPP1). The degradation or hydrolysis of PPi to orthophosphate is catalyzed by inorganic pyrophosphatases, such as tissue non-specific alkaline phosphatase (TNAP). The production of inorganic pyrophosphate by NPP1 and its hydrolysis by TNAP are in equilibrium. If there is dysregulation of this homeostasis, which is modulated by additional factors such as age, growth factors (e. g., TGF-beta), chemokines (e. g., IL-1 beta), transport proteins, enzymes and enzyme substrates, NPP1 activity predominates in aging osteoarthritic cartilage, which results in accumulation of PPi. This in turn leads to pathological deposition of CPP crystals [29].
Polymorphisms in the progressive ankylosis protein homolog (ANKH gene) also appear to play a part in the transport of pyrophosphate and in the release of ATP by chondrocytes, which ultimately contributes to the formation of the CPP crystals [16, 36].The pathophysiological processes in CPP crystal-induced arthritis have great similarity with gout. The pro-inflammatory cytokine IL-1 beta is produced in several stages by activation of the NALP3 inflammasome; however, the inflammatory reaction caused by the CPP crystals tends to have a subclinical course, which can be explained by the interaction of the crystals with phagocytic cells and their mitogenic activation and release of the proinflammatory cytokines [11, 21].
Parkinson’s disease and gout
A growing number of studies show that elevated uric acid levels appear to have a neuroprotective effect. Why uric acid precisely should have this effect is the object of research. It seems that dopaminergic neurons in the substantia nigra possess increased vulnerability to reactive oxygen radicals. Antioxidant properties are attributed to uric acid. The elevated uric acid level could therefore represent an endogenous protective mechanism against developing Parkinson’s disease [10]. The precise pathomechanism has not yet been fully elucidated. A possible explanation is that dopaminergic neurons contribute to neurotoxicity by generating radicals in the presence of oxygen molecules and produce neuromelanin by auto-oxidation. Dopaminergic neurons are therefore exposed to increased oxidative stress, which makes them vulnerable to genetic mutations and toxins [13]. Whether an “unhealthy” diet with increased consumption of purines and alcohol ultimately leads to a lower risk of developing Parkinson’s disease has not been confirmed consistently even though there are a few studies in this respect [15, 30]. Future research will have to show whether routine clinical measurement of the uric acid level can help to establish the diagnosis and prognosis of Parkinson’s disease. At the present time, routine measurement in this context is rejected. Consideration of the uric acid level alone without involving other parameters does not appear expedient in future either. Nevertheless, the correlation is an interesting approach for further research in this area.
Conclusion for practice
-
Both the prevalence and the incidence of gout and CPPD increase with age.
-
Gout and CPPD are among the most frequent inflammatory joint diseases in elderly patients. The differential diagnosis can be clearly made by microscopic analysis of synovial fluid.
-
Hyperuricemia is closely linked with the metabolic syndrome so optimization is associated with a reduction of the uric acid levels.
-
Renal insufficiency is closely linked with the risk of hyperuricemia so optimal therapy of the renal insufficiency should be ensured.
A gout attack is due to a severe inflammatory reaction that activates the NALP3 inflammasome in a cascade-like sequence. The further process is then mediated by cytokine activation, ultimately leading to activation of the innate and acquired immune system.
-
Monosodium urate crystals form when the solubility product exceeds about 7 mg/dl.
-
Arthritic joints in which deposits of CPP crystals cause a mild inflammatory reaction, which shifts the pH in the synovial fluid to lower levels, are a predisposing factor.
-
Increased consumption of alcohol is a risk factor for gout. Because of the high DNA content in the yeast, drinking beer (over 0.3 l) has a greater effect than consumption of drinks such as spirits with a high percentage of alcohol. Wine appears to have little or no effect on the elevation of uric acid.
-
Increased consumption of fructose-containing foods such as soft drinks, fruit yoghurts and prepreparedmeals promotes hyperuricemia and is therefore unfavorable.
References
Bhansing KJ, Van Bon L, Janssen M et al (2010) Gout: A clinical syndrome illustrated and discussed. Neth J Med 68:352–359
Bhole V, De Vera M, Rahman MM et al (2010) Epidemiology of gout in women: Fifty-two-year followup of a prospective cohort. Arthritis Rheum 62:1069–1076
Branzk N, Papayannopoulos V (2013) Molecular mechanisms regulating NETosis in infection and disease. Semin Immunopathol 35:513–530
Busso N, So A (2010) Mechanisms of inflammation in gout. Arthritis Res Ther 12:206
Choi HK, Atkinson K, Karlson EW et al (2004) Alcohol intake and risk of incident gout in men: a prospective study. Lancet 363:1277–1281
Choi HK, Curhan G (2008) Soft drinks, fructose consumption, and the risk of gout in men: Prospective cohort study. BMJ 336:309–312
Choi HK, Mount DB, Reginato AM et al (2005) Pathogenesis of gout. Ann Intern Med 143:499–516
Choi HK, Willett W, Curhan G (2010) Fructose-rich beverages and risk of gout in women. JAMA 304:2270–2278
Chong CR, Chan WP, Nguyen TH et al (2014) Thioredoxin-interacting protein: Pathophysiology and emerging pharmacotherapeutics in cardiovascular disease and diabetes. Cardiovasc Drugs Ther 28:347–360
Cipriani S, Chen X, Schwarzschild MA (2010) Urate: a novel biomarker of Parkinson’s disease risk, diagnosis and prognosis. Biomark Med 4:701–712
Dalbeth NHD (2006) Pathophysiology of crystal-induced arthritis. In: Wortmann RLSHJ, Becker MA, Ryan LM (eds) Crystal-Induced Arthropathies: Gout, Pseudogout, and Apatite-Associated Syndromes. Taylor & Francis Group, New York, p 239
Edwards NL (2008) The role of hyperuricemia and gout in kidney and cardiovascular disease. Cleve Clin J Med 75(Suppl 5):13–16
Fahn S, Cohen G (1992) The oxidant stress hypothesis in Parkinson’s disease: Evidence supporting it. Ann Neurol 32:804–812
Feig DI, Soletsky B, Johnson RJ (2008) Effect of allopurinol on blood pressure of adolescents with newly diagnosed essential hypertension: A randomized trial. JAMA 300:924–932
Hernan MA, Chen H, Schwarzschild MA et al (2003) Alcohol consumption and the incidence of Parkinson’s disease. Ann Neurol 54:170–175
Ho AM, Johnson MD, Kingsley DM (2000) Role of the mouse ank gene in control of tissue calcification and arthritis. Science 289:265–270
Kim SY, Guevara JP, Kim KM et al (2010) Hyperuricemia and coronary heart disease: A systematic review and meta-analysis. Arthritis Care Res (Hoboken) 62:170–180
Lin JC, Lin CL, Chen MC et al (2015) Gout, not hyperuricemia alone, impairs left ventricular diastolic function. Arthritis Res Ther 17:323
Luk AJ, Levin GP, Moore EE et al (2009) Allopurinol and mortality in hyperuricaemic patients. Rheumatology (Oxford) 48:804–806
Marson PPG (2011) Some historical remarks on microcrystalline arthritis (gout and chondrocalcinosis). Reumatismo 63:199–206
Martinon F, Petrilli V, Mayor A et al (2006) Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature 440:237–241
Matsuo H, Chiba T, Nagamori S et al (2008) Mutations in glucose transporter 9 gene SLC2A9 cause renal hypouricemia. Am J Hum Genet 83:744–751
Matsuo H, Nakayama A, Sakiyama M et al (2014) ABCG2 dysfunction causes hyperuricemia due to both renal urate underexcretion and renal urate overload. Sci Rep 4:3755
Matsuo H, Takada T, Ichida K et al (2009) Common defects of ABCG2, a high-capacity urate exporter, cause gout: A function-based genetic analysis in a Japanese population. Sci Transl Med 1:5ra11
Mikuls TR, Farrar JT, Bilker WB et al (2005) Gout epidemiology: Results from the UK General Practice Research Database, 1990–1999. Ann Rheum Dis 64:267–272
Mitroulis I, Kambas K, Chrysanthopoulou A et al (2011) Neutrophil extracellular trap formation is associated with IL-1beta and autophagy-related signaling in gout. PLOS ONE 6:e29318
Neogi T (2011) Clinical practice. Gout. N Engl J Med 364:443–452
Netea MG, Brown GD, Kullberg BJ et al (2008) An integrated model of the recognition of Candida albicans by the innate immune system. Nat Rev Microbiol 6:67–78
Oliviero F, Scanu A, Punzi L (2011) Metabolism of crystals within the joint. Reumatismo 63:221–229
Palacios N, Gao X, O’reilly E et al (2012) Alcohol and risk of Parkinson’s disease in a large, prospective cohort of men and women. Mov Disord 27:980–987
Papayannopoulos V, Zychlinsky A (2009) NETs: a new strategy for using old weapons. Trends Immunol 30:513–521
Polekhina G, Ascher DB, Kok SF et al (2011) Crystallization and preliminary X‑ray analysis of the N‑terminal domain of human thioredoxin-interacting protein. Acta Crystallogr Sect F Struct Biol Cryst Commun 67:613–617
Reginato AM, Mount DB, Yang I et al (2012) The genetics of hyperuricaemia and gout. Nat Rev Rheumatol 8:610–621
Reinders MK, Jansen TL (2010) Management of hyperuricemia in gout: Focus on febuxostat. Clin Interv Aging 5:7–18
Roddy E, Doherty M (2010) Epidemiology of gout. Arthritis Res Ther 12:223
Rosenthal AK, Gohr CM, Mitton-Fitzgerald E et al (2013) The progressive ankylosis gene product ANK regulates extracellular ATP levels in primary articular chondrocytes. Arthritis Res Ther 15:R154
Schauer C, Janko C, Munoz LE et al (2014) Aggregated neutrophil extracellular traps limit inflammation by degrading cytokines and chemokines. Nat Med 20:511–517
Schlesinger N, Thiele RG (2010) The pathogenesis of bone erosions in gouty arthritis. Ann Rheum Dis 69:1907–1912
Shi Y, Evans JE, Rock KL (2003) Molecular identification of a danger signal that alerts the immune system to dying cells. Nature 425:516–521
So A (2007) Recent advances in the pathophysiology of hyperuricemia and gout. Rev Med Suisse 3(720):722–724
Tan P, Hyndman D, Liu S (2011) Lesinurad (RDEA594), a novel investigational uricosuric agent for hyperuricemia and gout, blocks transport of uric acid induced by hydrochlorothiazide. Ann Rheum Dis 70:187
Terkeltaub RA (2003) Clinical practice. Gout. N Engl J Med 349:1647–1655
Torres RJ, De Miguel E, Bailen R et al (2014) Tubular urate transporter gene polymorphisms differentiate patients with gout who have normal and decreased urinary uric acid excretion. J Rheumatol 41:1863–1870
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S. Schlee, L.C. Bollheimer, T. Bertsch, C.C. Sieber and P. Härle declare that they have no competing interests.
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Schlee, S., Bollheimer, L.C., Bertsch, T. et al. Crystal arthritides – gout and calcium pyrophosphate arthritis. Z Gerontol Geriat 51, 453–460 (2018). https://doi.org/10.1007/s00391-017-1197-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00391-017-1197-3