
Abstract
-
CPPD is a clinically heterogeneous disorder characterized by the presence of intra-articular calcium pyrophosphate (CPP) crystals that form in normally unmineralized pericellular matrix of articular hyaline and fibrocartilage.
-
The most common sites of involvement are the knee menisci, the triangular fibrocartilage of the wrist, and the glenohumeral joint. Chondrocalcinosis is common in these sites as well as in others (e.g., the symphysis pubis).
-
CPP crystals deposit primarily in the middle zone of hyaline articular cartilage in joints. In gout, by contrast, the monosodium urate crystals tend to deposit on articular cartilage surface. The differing locations of crystal deposition in these conditions result in imaging appearances – e.g., on ultrasound – that are quite distinct.
-
Ultrasonography has greater sensitivity than plain radiography in detecting CPPD.
-
Pathologic cartilage calcification in CPPD is promoted by changes in inorganic pyrophosphate (PPi) metabolism and transport, and in chondrocyte differentiation.
-
CPPD has a close, complex relationship with osteoarthritis, another disease that is highly prevalent in aging and increases progressively with more advanced aging.
-
CPPD can occur in patients younger than age 55, who have a familial variant of the condition, a history of joint trauma, or who are afflicted with certain metabolic diseases that predispose to CPP crystal deposition.
-
No specific evidence-based therapies exist to limit or reverse CPP crystal deposition. The inflammation promoted by CPPD crystal deposition can be managed successfully in most patients through systemic therapies typically employed for the treatment of gout. However, the evidence base for the success of such systemic therapies in resolving acute inflammatory arthritis flares in CPPD is limited compared to gout, and intra-articular glucocorticoid injection remains a mainstay of management.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Calcium pyrophosphate deposition disease
- CPPD
- pseudogout
- pseudo-rheumatoid arthritis
- glucocorticoid
- colchicine
- hydroxychloroquine
- positive birefringence
- osteoprotegerin
- ANKH
-
CPPD is a clinically heterogeneous disorder characterized by the presence of intra-articular calcium pyrophosphate (CPP) crystals that form in normally unmineralized pericellular matrix of articular hyaline and fibrocartilage.
-
The most common sites of involvement are the knee menisci, the triangular fibrocartilage of the wrist, and the glenohumeral joint. Chondrocalcinosis is common in these sites as well as in others (e.g., the symphysis pubis).
-
CPP crystals deposit primarily in the middle zone of hyaline articular cartilage in joints. In gout, by contrast, the monosodium urate crystals tend to deposit on articular cartilage surface. The differing locations of crystal deposition in these conditions result in imaging appearances—e.g., on ultrasound—that are quite distinct.
-
Ultrasonography has greater sensitivity than plain radiography in detecting CPPD.
-
Pathologic cartilage calcification in CPPD is promoted by changes in inorganic pyrophosphate (PPi) metabolism and transport, and in chondrocyte differentiation.
-
CPPD has a close, complex relationship with osteoarthritis, another disease that is highly prevalent in aging and increases progressively with more advanced aging.
-
CPPD can occur in patients younger than age 55, who have a familial variant of the condition, a history of joint trauma, or who are afflicted with certain metabolic diseases that predispose to CPP crystal deposition.
-
No specific evidence-based therapies exist to limit or reverse CPP crystal deposition. The inflammation promoted by CPPD crystal deposition can be managed successfully in most patients through systemic therapies typically employed for the treatment of gout. However, the evidence base for the success of such systemic therapies in resolving acute inflammatory arthritis flares in CPPD is limited compared to gout, and intra-articular glucocorticoid injection remains a mainstay of management.
Symptoms and Signs
Pearl
CPPD can present not only as acute CPP crystal arthritis but also as a persistent polyarticular inflammatory arthritis.
Comment: In a small but significant fraction of subjects with CPPD, the manifestations of polyarticular CPP crystal arthropathy overlap substantially with those of rheumatoid arthritis (RA). CPPD can mimic RA in its inflammatory signs and symptoms as well as its ability to involve either small or large joints (or both) in a symmetrical manner (McCarty 1975; Zhang et al. 2011a, 2011b).
A positive rheumatoid factor (RF) occurs in 10% of patients with CPPD deposition disease (McCarty 1975). This reflects the high frequency of false-positive RF assays in aging. Elevated markers of systemic inflammation are also common in symptomatic CPPD patients, particularly those with polyarticular CPPD.
The other side of the coin is this: patients with long-standing RA sometimes develop articular CPP crystal deposition. This is attributable to the occurrence of secondary degenerative joint disease, as well as to the effects of aging. In fact, in a study of synovial fluid samples from 93 patients who fulfilled the American College of Rheumatology (ACR) classification criteria for RA, 25% contained CPP crystals (Gerster et al. 2006). The average interval between the onset of RA and the development of CPPD was 17 years (Sabchyshyn 2018). The possibility of CPPD, not simply joint infection, should therefore be kept in mind when an RA patient presents with a single joint inflamed out of proportion to all others. Arthrocentesis is essential to exclude infection in this setting, but one should also bear in mind that CPPD may be the culprit—particularly if it is a joint commonly affected by CPPD.
The response to therapy may not differentiate CPPD from RA in all cases. Small studies suggest that some patients with refractory, polyarticular CPPD deposition disease also respond to methotrexate, but this finding requires additional confirmation in adequately sized, blinded, controlled studies (Parperis 2020).
Pearl
CPPD can mimic a variety of rheumatic disorders.
Comment: CPPD deposition disease can present not simply as acute CPP crystal inflammatory arthritis (“pseudogout”), but also as pseudoseptic arthritis, as a component of neuropathic arthritis, as pseudo-polymyalgia rheumatica (PMR), as pseudotumorous masses involving soft tissue, bone, and joints, as recurrent hemarthrosis, and as pseudo-meningitis in the context of the crowned dens syndrome.
Pearl
CPP crystal deposition is often present but unrelated to the cause of the patient’s joint pain.
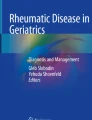
Comment: Prevalence of CPP crystal deposition is remarkably high in the elderly. However, CPP crystal deposition is subclinical in many cases. This disorder is detected often as an incidental finding on radiographs, with calcification of the knee menisci or triangular fibrocartilage of the wrist (Fig. 37.1a, b).

(a and b) Calcium pyrophosphate dehydrate (CPPD) deposition within the meniscal cartilage of the knee (a) and the triangular fibrocartilage of the wrist (b)
Inflammatory arthritis in elderly patients with pre-existing CPP crystal deposition should not be attributed automatically to CPPD. Other disorders must be excluded carefully. As examples, both RA and PMR can co-exist with and be mimicked by CPPD.
True infectious arthritis is a particular consideration in patients with established CPPD. CPP crystal deposits are detected in some infected joint fluids. CPP crystals and infection are often identified together in synovial fluids. CPP crystals within articular cartilage may be “strip-mined” by the inflammatory enzymes associated with joint infection.
Pearl
Clinical clues help differentiate gout and acute CPP crystal inflammatory arthritis (“pseudogout”).
Comment: It is impossible to differentiate among the major causes of monoarticular arthritis—infection, gout, and pseudogout—on physical examination criteria alone. Clinical context is important, however, in making educated guesses about the cause of monoarthritis in individual cases. Certain clinical clues, for example, raise the index of suspicion for pseudogout. As an example, pseudogout predominantly affects large- and intermediate-sized joints such as the knee and wrist. The elbow and ankle can also be affected by pseudogout, albeit less commonly. In contrast, pseudogout flares affect small joints of the feet and hands much less commonly.
The classic location for an initial flare of gout, of course, is the first metatarsophalangeal joint, with mid-foot and ankle involvement also being common. Nevertheless, gout is generally more protean in terms of the joints that it can affect, and a patient with long-standing gouty arthropathy can certainly have flares that affect the same large and intermediate-sized joints prone to pseudogout.
In the final analysis, one must have a low threshold for performing joint arthrocentesis when no strong presumption about the cause of a monoarthritis is possible. This is particularly important when there is any hint of possibility that the cause might be an infection.
Myth
CPPD -induced arthritis ceases after total joint arthroplasty.
Comment: One might assume that removal of joint cartilages puts a halt to clinical manifestations of CPPD. However, CPP crystals can deposit in the joint following arthroplasty, and pseudogout flares can develop early and late after this procedure (Crawford et al. 1999; Holt et al. 2005; Harato and Yoshida 2013; Hirose and Wright 2007; Sonsale and Philipson 2007).
Pearl
Chronic degenerative arthropathy in CPPD commonly affects several joints that are spared in classic cases of primary osteoarthritis.
Comment: The metacarpophalangeal joints, wrists, elbows, and glenohumeral joints are not typical sites of primary osteoarthritis. However, these joints are affected commonly in CPPD. If an elderly patient has arthritis of these joints and does not have RA or typical OA, CPPD is a good bet.
Pearl
Tumoral deposits of CPP crystal can behave as a locally aggressive but benign chondroid tumor.
Comment: Tumoral or pseudotophaceous CPP crystal deposition has been reported in periarticular structures such as tendons, ligaments, bursae, as well as in bones (close to a joint) such as the temporal bone, femur, and tibia. The clinical presentation may be of a slowly growing lump. Tumoral CPP crystal deposition sometimes necessitates surgical removal.
Radiology
Myth
If there is no chondrocalcinosis of the knee on radiographic assessment, the patient does not have CPPD.
Comment: CPPD deposition is commonly observed on plain radiography of the wrists and hips in the absence of knee chondrocalcinosis (Abhishek et al. 2012). Moreover, plain radiographs have a low sensitivity for detecting chondrocalcinosis. Ultrasonography should be used to detect CPPD if plain films are normal and CPPD is suspected clinically. Figure 37.2a, b illustrates well the greater sensitivity of ultrasound compared with plain radiography.

(a and b) Conventional radiograph of knee that is normal and a contemporaneous ultrasound study of the same joint confirming calcium pyrophosphate deposition pattern. An 89 year-old man presented with intermittent left knee pain. (a and b) show standing frontal and lateral radiographs of the left knee, without evidence for degenerative changes or chondrocalcinosis. (c and d). Transverse and longitudinal greyscale ultrasound images demonstrate curvilinear hyperechoic areas in the mid-substance of the central trochlear articular cartilage. No hypervascularity noted on Doppler interrogation. (Figure courtesy of Laureen Daft, BS, and Karen Chan, MD (San Diego VA Healthcare Service, University of California San Diego)
Myth
Conventional radiographic findings correlate reliably with pathological and clinical manifestations in CPPD.
Reality: Conventional radiography is most often the initial approach to the evaluation of patients with suspected CPPD. However, in one study that employed knee arthroscopy, the correlation between radiographic and pathological findings was only 39% (Fisseler-Eckhoff and Muller 1992). Studies of CPPD by ultrasonography, advanced imaging such as dual-energy CT, and quantitative physical-chemical analyses of joint fluid and tissue crystals are needed to understand better the relationships between the amounts and articular foci of crystal deposition, symptoms, and disease outcome.
Pearl
In an elderly patient presenting with fever, neck pain, and high inflammatory markers, remember that the “crowned dens” syndrome may be the explanation—and that it has a wonderfully simple solution.
Comment: CPP crystal deposits can develop in the ligamentum flavum or the transverse ligament at C1. Consequently, crystal-induced inflammation can occur at this site (Fig. 37.3). The collection of disease features resulting from this anatomical location of CPP crystals and the incitement of inflammation there is termed the “crowned dens” syndrome (Younis 2017; Moshrif et al. 2019; Haikal et al. 2020). Patients typically present with fever, acute-onset meningismus, high inflammatory markers, and stenosis of the cervical spinal canal. Confusional symptoms such as delirium are also common, making this presentation difficult to sort out if the patient is the only available historian. Myelopathy or the foramen magnum syndrome occurs occasionally. Fracture of the odontoid peg precipitated by calcification at C1–C2 has been reported.

The crowned dens syndrome. Computed tomography scan of the C1 region, showing calcium deposition around the odontoid process of the axis
Although it can occur in an isolated fashion with symptoms limited only to the head and neck, the crowned dens syndrome caused by CPP crystals is often part of a polyarthritis involving peripheral joints. Large joints such as shoulders, knees, or ankles are commonly affected, often mimicking polymyalgia rheumatica. When facing a patient with acute, inflammatory neck pain, the systematic joint assessment may reveal the presence of peripheral arthritis. Aspiration of one of these joints, confirmation of CPPD crystals, and putting two and two together can crack the overall case, leading to a wonderful “Aha!” moment. These patients respond quite beautifully to glucocorticoids.
Diagnosis
Pearl
CPP may be the causal crystal in elderly patients with acute crystal synovitis even if the crystal aspirate is negative and the plain radiograph does not show chondrocalcinosis.
Comment: Due to the low sensitivity of plain radiography and the high-false negative rate of laboratory observers in detecting CPP crystals, CPPD should be a potential explanation for the older adult patient with a syndrome consistent with an acute crystal-inducted synovitis affecting the knee or the wrist. This is particularly likely if the patient has no clinical history of gout—which would be unlikely to appear in another joint with antecedent podagra. The diagnosis may be aided by ultrasonography or dual-energy CT (which is more specific than CT).
Myth
CPP crystals can be hard to identify on the microscope.
Reality: CPP crystals vary in size and shape, from rods or rhomboids to tiny, thin needles resembling urate. Large, thick crystals can often be identified. Under polarized light, the birefringence of CPP crystals is weak and present in about 20% of crystals (Ivorra et al. 1999).
Crystal identification often relies on polarized light microscopy. Because urate crystals shine intensively under polarized light, they are easily detected. The identification of CPP crystals under polarized light, however, is generally more challenging. The assessment of a synovial fluid sample by microscopy should actually begin, therefore, under ordinary light (Pascual et al. 1989). Magnification at 600× and 1000× is helpful (1000× requires immersion oil). The rod-shaped CPP crystals can often be observed without the light polarizer.
The rod-shaped crystals typical of CPPD sometimes even have a needle-shaped appearance and therefore might be mistaken for urate crystals. In such cases, the birefringence characteristics of the crystals can be informative. Other types of crystals with more characteristic shapes should also be sought (Andrés et al. 2019). The synovial fluid sample should be examined for the presence of intraleukocytic vacuoles containing crystals. Due to different membranolytic properties, urate crystals are not seen inside such vacuoles, but CPP crystals can be visualized there (Fig. 37.4a–d).

(a) Calcium pyrophosphate crystals (arrow) found intracellularly and within vacuoles (see the empty space around the crystals). The shape of crystals differs, with a typical rhomboid on the right and a needle-like crystal on the left. (400× magnification, ordinary light microscopy). (b) Under polarized light, needle-shaped crystal shows no birefringence, while while the birefringence is in the rhomboid. (400× fields, simple polarized light microscopy). (c) A typical needle-shaped monosodium urate crystal (dashed arrow) inside a leukocyte. (400× magnification, ordinary light microscopy). (d) Note the absence of intracellular vacuoles containing the crystal and the intense brightness displayed under simple polarized light. (400× fields, simple polarized light microscopy)
Pearl
CPP crystals can be hard to find. Keep looking!
Comment: CPPD crystals, notoriously difficult to detect in some synovial fluids, are missed or misidentified routinely in clinical specimens (Zell et al. 2019). CPP crystals vary more widely in size and shape than urate crystals. CPP crystals are generally smaller than their monosodium urate counterparts and are typically rod- or rhomboid-shaped (Fig. 37.5). CPP crystals demonstrate weakly positive birefringence or sometimes no birefringence, in contrast to the consistently bright, negatively birefringent monosodium urate crystals. Rhomboid CPP crystals are more likely to demonstrate birefringence than the rod-shaped versions (Andrés et al. 2019).

Calcium pyrophosphate dehydrate (CPPD) crystals in synovial fluid. CPPD crystals are often weakly positively birefringent and have a characteristic rectangular shape with blunted ends
Several factors and techniques enhance the likelihood of finding such crystals, if present:
-
The microscopist’s experience.
-
The length of time spent searching for crystals. Second looks often yield the diagnosis (Yuan et al. 2003).
-
The use of phase contrast and high magnification.
-
Use of the oil objective (permits examination for crystals within synovial fluid leukocytes).
-
Finally, centrifugation (10 min at 700 RPM) to pellet the leukocytes with intracellular crystals may increase the sensitivity of synovial fluid analysis to detect CPP crystals (Boumans et al. 2017).
Pearl
Beware CPP crystal mimics in synovial fluid.
Comment: All positively birefringent particulate matter within synovial fluid is not CPP crystals. In particular, be wary of crystals that are described as “brightly” birefringent or fluids described as having large quantities of crystals. The most common mimics of CPP crystals are contaminants. Particular offenders are glucocorticoid crystals (Fig. 37.6), the result of previous intra-articular injections; and talc (Fig. 37.7), from gloves used during the procedure.

Glucocorticoid crystals in synovial fluid. These brightly birefringent crystals are from an intra-articular glucorticoid injection performed several weeks before this joint aspiration

Talc crystals in synovial fluid. These crystals are seen less frequently as less talc is used in the manufacture of gloves. They typically appear as round “beach-ball”-like structures
Myth
Synovial fluid examinations are worthless unless performed immediately. Stored synovial fluid generates artifactual calcium-containing crystals, including CPP crystals.
Reality: It is a widely held belief that the storage of synovial fluid (e.g., overnight) results in the de novo formation of crystals that are of no clinical significance. Several older studies suggested that stored synovial fluids produce brushite, a calcium-containing crystal (CaHPO4·2H2O), that is described often as having a star-shaped morphology (Dieppe et al. 1979).
More recent studies do not support the phenomenon of brushite formation. One study demonstrated that for synovial fluid samples deemed to be crystal-free upon immediate examination, no new crystals appeared following storage in either a refrigerator or freezer (Galvez et al. 2002). Moreover, clinically important crystals were retained in the fluids despite refrigeration for at least 72 h, with only minor losses observed with freezing.
These findings support the theory, based on the known levels of calcium and pyrophosphate in synovial fluids, that CPP crystals are unlikely to form in solution (Hearn et al. 1978; Zell et al. 2019).
Myth
Intracellular CPP crystals are more significant than extracellular ones.
Reality: A prevailing Myth from the past holds that unless CPP crystals are intracellular, they are clinically irrelevant (Fig. 37.8). On the contrary, in one study, neither the clinical presentation nor the presence or absence of joint inflammation correlated with the location of CPP crystals (intracellular versus extracellular) (Martinez-Sanchis and Pascual 2005). CPP crystals may be important wherever they are found—in intra-cellular or extra-cellular locations. Clinical correlation is required.

Intra- and extracellular calcium pyrophosphate dehydrate (CPPD) crystals. Typically, CPPD crystals are seen both intra- and extra-cellularly
Myth
All patients with CPPD should undergo a thorough metabolic evaluation to exclude underlying causes.
Reality: The three most common risk factors for articular CPPD deposition are: (1) age; (2) age; and, (3) age! Approximately 20% of individuals over the age of 80 have articular CPP crystals visible on plain radiography. Given how insensitive plain radiography is for detecting CPPD, this is almost certainly an underestimate of the true prevalence of intra-articular CPPD crystals in this age set (Mitrovic et al. 1988). It is rare for CPPD crystals to be detected in patients younger than 60 years of age unless the disease is familial, caused by trauma to a single joint, or associated with one of a handful of metabolic abnormalities. A 90-year-old patient with chondrocalcinosis on a knee film is unlikely to have an occult metabolic condition (except for primary hyperparathyroidism, which becomes more common with age).
Young patients should be screened for the metabolic associations of CPPD crystal deposition (Table 37.1). The most common include primary hyperparathyroidism, hemochromatosis, hypophosphatasia, and hypomagnesemia (Conti et al. 2017). (Note that this list does NOT include hypothyroidism. See below). Gout is another well-characterized risk factor for CPPD via the phenomenon of epitaxy (one crystal forming over the other). Some constituents of degenerated cartilage appear to promote the deposition of urate crystals, leading in turn to the formation of CPP crystal formation. The appropriate laboratory evaluation for these disorders is shown in Table 37.2.
Myth
Hypothyroidism is a common metabolic cause of secondary CPPD crystal deposition disease.
Reality: In case studies, CPP crystals have been detected in joint effusions of some patients with severe hypothyroidism, a condition that by itself can cause arthropathy. However, hypothyroidism and CPPD are both extremely common among older individuals. This fact alone probably explains the frequent co-existence of these two conditions. Indeed, several cross-sectional studies of patients with radiographically detected CPPD have failed to detect a significant association between hypothyroidism and chondrocalcinosis (Kleiber Balderrama et al. 2017).
Pearl
Metabolic and inherited CPPD typically present with recurrent flares of acute CPP crystal arthritis. The exception to this rule is hemochromatosis.
Comment: Hypophosphatasia, hypomagnesemia, and hyperparathyroidism present with recurrent flares of acute CPP crystal arthritis. CPPD disease in people with ANKH mutations also presents with recurrent flares of acute crystal synovitis. In contrast, among the secondary causes of CPPD, hemochromatosis alone causes structural arthritis. The secondary CPPD resulting from that condition probably results from increased crystal nucleation in the context of iron overload and cartilage damage. CPPD can also occur in the context of severe dysplastic (inherited) osteoarthritis.
Epidemiology and Genetics
Myth
CPPD is equally prevalent in all ethnic groups.
Reality: CPPD of the wrist and knee is markedly less common among Chinese persons living in Beijing than in Caucasians residing in Framingham, Massachusetts (Zhang et al. 2006). It is also less common among Japanese than among Caucasians (Chiba et al. 2017). This disparity is evident despite the higher prevalence of knee osteoarthritis in the Chinese population. Relatively high calcium in drinking water in Beijing, which leads to long-term suppression of parathyroid hormone production, has been suggested as a partial explanation of this observation.
Myth
The clinical presentation of familial CPPD is homogeneous.
Reality: Familial CPP crystal deposition disease usually presents in the third and fourth decades of life, but familial disease can also be detected before the age of 20 or into late middle age.
The ANKH gene, which encodes a transmembrane protein that channels PPi into and out of the chondrocyte, is important in the pathophysiology of chondrocalcinosis (Zaka and Williams 2006). Some kindreds with linkages to ANKH on chromosome 5p manifest early-onset polyarthritis. The knees and wrists are affected most commonly, but ankylosing intervertebral disease and involvement of the symphysis pubis and sacroiliac joints are also described. Most patients with inherited CPPD due to ANKH gene mutations present with intermittent flares of acute crystal synovitis without structural arthropathy (Abhishek and Doherty 2011).
Chondrocalcinosis of late onset has also been reported in some kindreds. Familial CPPD deposition disease can involve more than one joint and manifests a level of clinical intensity comparable to that seen in idiopathic CPPD deposition disease. In patients with ANKH mutations, CPP crystal deposition occurs before the onset of premature osteoarthritis.
A major cluster of CPPD mutations on chromosome 8q (CCAL1) has been identified as related to mutations in the gene that encodes osteoprotegerin. The CPPD mutation results in a loss of osteoprotegerin function and thus may promote osteoclast formation (Williams et al. 2018). The exact mechanism through which this mutation causes CPP crystal formation in cartilage is under investigation. Patients with the osteoprotegerin mutation present with simultaneous onset of osteoarthritis and CPP crystal deposition, suggesting a different initial mechanism than occurs with ANKH mutations.
Pearl
Expand genetic testing for familial CPPD to include the osteoprotegerin mutation.
Comment: CPPD might occur at early ages and cluster in families, as initially reported in the 1960s (Zitnan and Sitaj 1960). Subsequent investigations located the genetic basis for familiar CPPD at the ANKH gene (chromosome 5p, CCAL2 locus, OMIM #118600) (Hughes et al. 1995). ANKH is a transmembrane protein that transports the inorganic pyrophosphate outside the chondrocyte to the extracellular matrix, where interacting with calcium would crystallize as CPP (Rosenthal and Ryan 2016). Several commercial tests for ANKH mutations are available.
A particular familial phenotype of CPPD that is associated with the early development of osteoarthritis was linked in 1995 to mutations at chromosome 8q (CCAL1 locus, OMIM #600668) (Baldwin et al. 1995). The affected gene, which has remained unknown for more than twenty-five years, is considered an “osteoarthritic” gene. Finally, the CCAL1 locus has been identified as the Tumor Necrosis Factor Receptor Super Family member 11B (TNFRSF11B) gene, coding for osteoprotegerin (Williams et al. 2018). Osteoprotegerin is a regulatory protein of osteoclast activation. An in vitro report suggests that CCAL1 mutation (the “osteoprotegerin gene”) leads to loss of function (Mitton-Fitzgerald et al. 2021). The mechanism through which this mutation predisposes CPPD remains to be clarified.
Pearl
Many elderly patients with chondrocalcinosis have radiographic evidence of this disorder in joints other than the knee.
Comment: Many joints can be involved in patients with CPP crystal deposition. In one study of 428 people who had radiographs of the knees, pelvis, and hands (mean age 66 years), 13.7% had chondrocalcinosis at least one of those sites. Many had involvement of joints other than the knee. For example, 44% of the patients with wrist involvement lacked any evidence of knee chondrocalcinosis.
Pathophysiology
Myth
The pathophysiology of CPPD is poorly understood.
Comment: Altered local (not systemic) concentrations of calcium, PPi, and the solubility products of these ions clearly promote the formation of CPP crystals. The levels of magnesium in cartilage and the composition of the extracellular matrix also influence the dynamics of CPP crystal formation. These factors determine the ratio of monoclinic to triclinic CPP crystals. Monoclinic CPP crystals are more inflammatory, and therefore this ratio is important.
Both calcium and PPi also exert important effects on gene expression, cell differentiation, and viability in chondrocytes. Excess quantities of PPi lead to the induction of matrix metalloproteinase-13 and the promotion of apoptosis. Hence, “pyrophosphate arthropathy” appropriately describes some of the chronic degenerative changes in cartilage in CPPD crystal deposition disease. These changes are not simply due to the toxic effects on chondrocytes and pro-inflammatory effects of CPPD crystals.
Pearl
Acute CPP crystal inflammatory arthritis flares can be provoked reliably by certain medical procedures.
Comment: The vast majority of flares do not have a recognized trigger. They can, however, be provoked by minor trauma. In theory, this is the result of a “shaking loose” of CPP crystals from joint cartilage—but the precise pathophysiology remains unclear. A variety of medical and surgical procedures, however, can trigger acute CPP crystal arthritis flares (Table 37.3).
Pearl
Altered PP i transport by ANKH is central to the pathogenesis of both idiopathic and familial CPPD crystal deposition disease.
Comment: ANKH encodes a transmembrane protein that facilitates the transport of PPi into and out of the chondrocyte (Zaka and Williams 2006). “Gain of function” alterations in intrinsic ANKH PPi channeling activity could lead to chronic, low-grade “PPi leak” from chondrocytes.
ANKH is increased in osteoarthritic and chondrocalcinotic cartilage chondrocytes. In addition, homozygosity for a single nucleotide substitution (−4 G to A) in the ANKH 5′-untranslated region that promotes increased ANKH expression was present in approximately 4% of British subjects with the diagnosis of idiopathic CPPD disease (Zhang et al. 2005). This was validated in an independent dataset (Abhishek et al. 2014). Hence, some patients with late-onset CPP crystal deposition disease may have a familial component.
Two major chromosomal linkages, 8q and 5p, have been identified in studies of familial CPPD deposition disease. Chromosome 5p-linked chondrocalcinosis, which is more widely distributed than 8q-linked disease, is associated with ANKH mutations. The 8q linked locus was recently identified as being the Tumor Necrosis Factor Receptor Super Family member 11B (TNFRSF11B) gene coding for osteoprotegerin (Williams et al. 2018). The chondrocyte in idiopathic chondrocalcinosis responds abnormally to growth factors insulin-like growth factor-1 and transforming growth factor, with increased PPi production.
Treatment and Outcomes
Pearl
Systemic glucocorticoids are useful for treatment of acute CPP crystal inflammatory arthritis.
Comment: Several studies support use of short-term systemic glucocorticoids for acute CPP crystal inflammatory arthritis (Parperis 2021). Most studies to date have employed either one or two 60 mg intramuscular injections of triamcinolone or oral prednisone for up to ten days.
On the other hand, prolonged courses or the use of high doses of prednisone have not been studied in acute CPP crystal inflammatory arthritis. Such approaches may create more problems than they solve, particularly in the elderly population that is at greatest risk for CPPD disease. Thus, systemic glucocorticoid bursts are helpful in treating acute CPPD disease flares, but “maintenance” prednisone is a bad idea.
Pearl
Compared to gout flares, flares of acute CPP crystal inflammatory arthritis take longer to peak in intensity, respond more slowly to therapy in general, and often demonstrate less complete treatment responses.
Comment: Delayed and inconsistent responses to NSAIDS, oral glucocorticoids, and colchicine are a feature of CPP crystal-induced pseudogout flares. Results have been encouraging for use of off-label anakinra to treat pseudogout flares (Dumusc and So 2021; Moltó et al. 2012; Ottaviani et al. 2013), but anakinra does not have any clear efficacy for off-label use long-term to treat chronic, refractory synovitis in CPPD (Doaré et al. 2021). Glucocorticoid injection into affected intermediate and large joints is the most consistently effective treatment.
When gout and CPP crystals coexist, lowering uric acid levels may not completely ameliorate the arthritis (Fig. 37.9 (formerly 4)). A recent study suggests that gouty tophi may also contain CPP crystals and that this may occur in patients without previous evidence of CPPD (Ea et al. 2021).

Coexistence of monosodium urate and calcium pyrophosphate dehydrate (CPPD) crystals in a single joint fluid. In this fluid, both monosodium urate and CPPD crystals are seen
Pearl
CPP crystals cannot be dissolved. Treatment, therefore, should take aim at inflammation.
Comment: In contrast to the situation of urate crystals, CPP crystals cannot be removed from joints via a medical therapy. Several agents, such as probenecid, pyrophosphatases, phosphocitrate or magnesium supplements demonstrated promise in in vitro studies but failed at more advanced stages of testing (Announ and Guerne 2008). The management of CPPD, therefore, focuses on the reduction of joint inflammation in the setting of acute flares (Zhang et al. 2011b). Most patients have only intermittent flares, requiring only short-term therapy courses (Yates et al. 2020). When flares occur frequently or develop into a persistent arthritis, long-term treatment is needed. The evidence base for such long-term treatment, unfortunately, is slim.
Pearl
For acute episodes of CPP crystal arthritis, glucocorticoids are the first-line agent.
Comment: The management of acute CPP crystal arthritis resembles the management of gout flares. The presence of hypertension, atherosclerotic disease, chronic kidney disease or peptic ulcers limits NSAID use in the typical CPPD patient, however, and low-dose colchicine is less effective than in gout flares. Thus, glucocorticoids are the best approach for CPP flares. Intra-articular injections of a long-lasting glucocorticoid such as triamcinolone acetonide or methylprednisolone are rapid, safe choices for monoarticular and even oligoarticular flares. Short courses of oral prednisolone are also effective and more appropriate for acute polyarthritis. The lack of robust evidence behind the use of glucocorticoids for acute CPP flares reflects the scant critical attention CPPD has received since its discovery in the 1960s (Parperis 2021). For refractory cases or when the usual agents appear contraindicated, short courses of the interleukin-1 receptor antagonist anakinra can be tried (Thomas et al. 2019).
Pearl
Intraarticular glucocorticoids are the most effective and often the safest therapy for acute CPP crystal inflammatory arthritis.
Comment: Some treatments that are highly effective in gout—e.g., glucocorticoids, colchicine, and NSAIDs—are used for managing acute CPP crystal inflammatory arthritis. However, the risks of these medications are not trivial in elderly patients. Few controlled trials of any therapy exist, but intraarticular glucocorticoids appear to be more effective than the alternatives and are certainly safer than most systemic therapies (O'Duffy 1976). Intra-articular glucocorticoids should be used as the treatment of choice unless there is a concurrent infection or, in rare instances, when the involved joint is inaccessible to injection. Oral glucocorticoids are likely the best approach in that case.
Pearl
Consider DMARDs or biologics for persistent CPP arthritis.
Comment: Fortunately, most patients with CPPD develop their episodes of acute arthritis only on an infrequent basis. However, a minority of patients develop persistent inflammation. Chronic CPP arthritis is often unresponsive to colchicine, and long-term use of glucocorticoids or NSAIDs should be avoided in the elderly. In clinical practice, these patients often benefit from initiating a disease-modifying agent, mainly methotrexate or antimalarials. The effectiveness is supported by case series and small controlled studies (Rothschild and Yakubov 1997; Andres et al. 2012; Parperis et al. 2021). A placebo-controlled trial evaluating methotrexate, however, was unsuccessful (Finckh et al. 2014).
For cases in which DMARDs fail or are tolerated poorly, anakinra, an interleukin-1interleukin-1 receptor antagonist, should be considered. In practice, patients may work with schemes including daily colchicine and 100 mg anakinra every two or three days. There are also preliminary reports suggesting a role for tocilizumab, an interleukin-6 receptor blocker (Quilis et al. 2018; Latourte et al. 2020).
Pearl
Low-dose hydroxychloroquine or colchicine may be used to prevent recurrent flares of CPPD disease.
Comment: Hydroxychloroquine limits experimental crystal-induced inflammatory processes by stabilizing phagolysosomes containing ingested crystals. One clinical trial suggested that patients treated 200–400 mg of hydroxychloroquine daily had fewer flares than those treated with placebo (Rothschild and Yakubov 1997). Uncontrolled studies suggest that low-dose colchicine also has some efficacy in preventing recurrent flares of acute CPP crystal arthritis (Parperis 2021).
References
Abhishek A, Doherty M. Pathophysiology of articular chondrocalcinosis--role of ANKH. Nat Rev Rheumatol. 2011;7(2):96–104.
Abhishek A, Doherty S, Maciewicz R, Muir K, Zhang W, Doherty M. Chondrocalcinosis is common in the absence of knee involvement. Arthritis Res Ther. 2012;14(5):R205.
Abhishek A, Doherty S, Maciewicz R, et al. The association between ANKH promoter polymorphism and chondrocalcinosis is independent of age and osteoarthritis: results of a case–control study. Arthritis Res Ther. 2014;16:R25.
Andres M, Sivera F, Pascual E. Methotrexate is an option for patients with refractory calcium pyrophosphate crystal arthritis. J Clin Rheumatol. 2012;18(5):234–6.
Andrés M, Vela P, Jovaní V, Pascual E. Most needle-shaped calcium pyrophosphate crystals lack birefringence. Rheumatology (Oxford). 2019;58(6):1095–8.
Announ N, Guerne PA. Treating difficult crystal pyrophosphate dihydrate deposition disease. Curr Rheumatol Rep. 2008;10(3):228–34.
Baldwin CT, Farrer LA, Adair R, Dharmavaram R, Jimenez S, Anderson L. Linkage of early-onset osteoarthritis and chondrocalcinosis to human chromosome 8q. Am J Hum Genet. 1995;56(3):692–7.
Boumans D, et al. The added value of centrifugation for monosodium urate and calcium pyrophosphate crystal detection. Clin Rheumatol. 2017;36:1599–605.
Chiba D, Tsuda E, Sasaki E, et al. Low prevalence of knee chondrocalcinosis and its catabolic association with serum matrix metalloproteinase 3: a rural Japanese population study. Int J Rheum Dis. 2017;21:2011–8.
Conti F, et al. Hypophosphatasia: clinical manifestation and burden of disease in adults. Clin Cases Miner Bone Metab. 2017;14(2):230–4.
Crawford R, Puddle B, Hunt N, et al. Deposition of calcium pyrophosphate in tissue after revision arthroplasty of the hip. J Bone Joint Surg Br. 1999;81(3):552–4.
Dieppe P, Crocker P, Corke C, et al. Synovial fluid crystals. Quarter J Med. 1979;48:533–55.
Doaré E, Robin F, Racapé H, Le Mélédo G, Orione C, Guggenbuhl P, Goupille P, Gervais E, Dernis E, Bouvard B, Marhadour T, Coiffier G, Saraux A. Features and outcomes of microcrystalline arthritis treated by biologics: a retrospective study. Rheumatol Ther. 2021;8(3):1241–53. https://doi.org/10.1007/s40744-021-00335-7. Epub ahead of print. PMID: 34218418
Dumusc A, So A. Answer to Cipolletta et al. “Treatment of acute CPP crystal arthritis: what are we missing?”. Joint Bone Spine. 2021;88:105217.
Ea HK, et al. Calcium pyrophosphate dihydrate crystal deposition in gouty tophi. Arthritis Rheum. 2021;73(2):324–9.
Finckh A, Mc Carthy GM, Madigan A, et al. Methotrexate in chronic-recurrent calcium pyrophosphate deposition disease: no significant effect in a randomized crossover trial. Arthritis Res Ther. 2014;16(5):458.
Fisseler-Eckhoff A, Muller KM. Arthroscopy and chondrocalcinosis. Arthroscopy. 1992;8:98–104.
Galvez J, Saiz E, Linares L, et al. Delayed examination of synovial fluid by ordinary and polarized light microscopy to detect and identify crystals. Ann Rheum Dis. 2002;61:444–7.
Gerster J, Varisco P, Kern J, et al. CPPD crystal deposition disease in patients with rheumatoid arthritis. Clin Rheumatol. 2006;25:468–9.
Haikal A, Everist BM, Jetanalin P, Maz M. Cervical CT-dependent diagnosis of crowned dens syndrome in calcium pyrophosphate dihydrate crystal deposition disease. Am J Med. 2020;133(2):e32–7.
Harato K, Yoshida H. Pseudogout in the early postoperative period after total knee arthroplasty. J Arthroplast. 2013;28(2):374.e9–374.e11.
Hearn P, Russell R, Elliott J, et al. Formation products of calcium pyrophosphate crystals in vitro and the effect of iron salts. Clin Sci. 1978;54:29P.
Hirose CB, Wright RW. Calcium pyrophosphate dihydrate deposition disease (pseudogout) after total knee arthroplasty. J Arthroplast. 2007;22(2):273–6.
Holt G, Vass C, Kumar CS. Acute crystal arthritis mimicking infection after total knee arthroplasty. BMJ. 2005;331(7528):1322–3.
Hughes AE, McGibbon D, Woodward E, Dixey J, Doherty M. Localisation of a gene for chondrocalcinosis to chromosome 5p. Hum Mol Genet. 1995;4(7):1225–8.
Ivorra J, Rosas J, Pascual E. Most calcium pyrophosphate crystals appear as non-birefringent. Ann Rheum Dis. 1999;58(9):582–4.
Kleiber Balderrama C, Rosenthal AK, Lans D, Singh JA, Bartels CM. Calcium pyrophosphate deposition disease and associated medical comorbidities: a National Cross-Sectional Study of US veterans. Arthritis Care Res (Hoboken). 2017;69(9):1400–6.
Latourte A, Ea HK, Frazier A, et al. Tocilizumab in symptomatic calcium pyrophosphate deposition disease: a pilot study. Ann Rheum Dis. 2020;79(8):1126–8.
Martinez-Sanchis A, Pascual E. Intracellular and extracellular CPPD crystals are a regular feature in synovial fluid from uninflamed joints of patients with CPPD related arthropathy. Ann Rheum Dis. 2005;64:1769–72.
McCarty DJ. Diagnostic mimicry in arthritis: patterns of joint involvement associated with calcium pyrophosphate dihydrate crystal deposits. Ann Rheum Dis. 1975;25:804–9.
Mitrovic D, Stankovic A, Iriarte-Borda O, et al. The prevalence of chondrocalcinosis in the human knee joint. An autopsy survey. J Rheumatol. 1988;15:633–41.
Mitton-Fitzgerald E, Gohr CM, Williams CJ, Ortiz A, Mbalaviele G, Rosenthal AK. The TNFRSF11B mutation associated with calcium pyrophosphate deposition disease results in ineffective osteoclast suppression. Rheumatol. 2021;73(8):1543–9. https://doi.org/10.1002/art.41678.
Moltó A, Ea HK, Richette P, Bardin T, Lioté F. Efficacy of anakinra for refractory acute calcium pyrophosphate crystal arthritis. Joint Bone Spine. 2012;79(6):621–3.
Moshrif A, Laredo JD, Bassiouni H, Abdelkareem M, Richette P, Rigon MR, Bardin T. Spinal involvement with calcium pyrophosphate deposition disease in an academic rheumatology center: a series of 37 patients. Semin Arthritis Rheum. 2019;48(6):1113–26.
O'Duffy J. Clinical studies of acute pseudogout attacks. Comments on prevalence, predisposition and treatment. Arthritis Rheum. 1976;19(Suppl):349–52.
Ottaviani S, Brunier L, Sibilia J, Maurier F, Ardizzone M, Wendling D, Gill G, Palazzo E, Meyer O, Dieudé P. Efficacy of anakinra in calcium pyrophosphate crystal-induced arthritis: a report of 16 cases and review of the literature. Joint Bone Spine. 2013;80(2):178–82.
Parperis K, Papachristodoulou E, Kakoullis L, Rosenthal AK. Management of calcium pyrophosphate crystal deposition disease: a systematic review. Semin Arthritis Rheum. 2021;51(1):84–94.
Pascual E, Tovar J, Ruiz MT. The ordinary light microscope: an appropriate tool for provisional detection and identification of crystals in synovial fluid. Ann Rheum Dis. 1989;48(12):983–5.
Quilis N, Andrés M, Vela P, Pascual E. Interleukin-6 pathway blockade as an option for managing refractory cases of crystal arthritis: two cases report. Joint Bone Spine. 2018;85(3):377–8.
Rosenthal AK, Ryan LM. Calcium pyrophosphate deposition disease. N Engl J Med. 2016;374(26):2575–84.
Rothschild B, Yakubov LE. Prospective 6-month, double-blind trial of hydroxychloroquine treatment of CPPD. Compr Ther. 1997;23(5):327–31.
Sabchyshyn V, Konon I, Ryan LM, Rosenthal AK. Concurrence of rheumatoid arthritis and calcium pyrophosphate deposition disease: A case collection and review of the literature. Semin Arthritis Rheum. 2018;48(1):9–11. https://doi.org/10.1016/j.semarthrit.2017.11.009. Epub 2017 Dec 2. PMID: 29338885; PMCID: PMC6240440.
Sonsale PD, Philipson MR. Pseudogout after total knee arthroplasty. J Arthroplast. 2007;22(2):271–2.
Thomas M, Forien M, Palazzo E, Dieudé P, Ottaviani S. Efficacy and tolerance of anakinra in acute calcium pyrophosphate crystal arthritis: a retrospective study of 33 cases. Clin Rheumatol. 2019;38(2):425–30.
Williams CJ, Qazi U, Bernstein M, et al. Mutations in osteoprotegerin account for the CCAL1 locus in calcium pyrophosphate deposition disease. Osteoarthr Cartil. 2018;26(6):797–806.
Yates KA, Yoshida K, Xu C, et al. Acute calcium pyrophosphate crystal arthritis flare rate and risk factors for recurrence. J Rheumatol. 2020;47(8):1261–6.
Younis AA. Crowned dens syndrome as a cause of acute neck pain: a case report and review of the literature. Mediterr J Rheumatol. 2017;28(2):101–5.
Yuan S, Bien C, Wener M, et al. Repeat examination of synovial fluid for crystals: is it useful? Clin Chem. 2003;49:1562–3.
Zaka R, Williams CJ. Role of the progressive ankylosis gene in cartilage mineralization. Curr Opin Rheumatol. 2006;18:181–6.
Zell M, Zhang D, FitzGerald J. Diagnostic advances in synovial fluid analysis and radiographic identification for crystalline arthritis. Curr Opin Rheumatol. 2019;31(2):134–43.
Zhang W, Doherty M, Bardin T, et al. European league against rheumatism recommendations for calcium pyrophosphate deposition. Part I: terminology and diagnosis. Ann Rheum Dis. 2011a;70(4):563–70.
Zhang W, Doherty M, Pascual E, et al. EULAR recommendations for calcium pyrophosphate deposition. Part II: management. Ann Rheum Dis. 2011b;70(4):571–5.
Zhang Y, Johnson K, Russell RG, et al. Association of sporadic chondrocalcinosis with a −4-basepair G-to-a transition in the 5′-untranslated region of ANKH that promotes enhanced expression of ANKH protein and excess generation of extracellular inorganic pyrophosphate. Arthritis Rheum. 2005;52:1110–7.
Zhang Y, Terkeltaub R, Nevitt M, et al. Lower prevalence of chondrocalcinosis in Chinese subjects in Beijing than in white subjects in the United States: the Beijing osteoarthritis study. Arthritis Rheum. 2006;54:3508–12.
Zitnan D, Sitaj S. Chondrocalcinosis polyarticularis (familiaris): roentgenological and clinical analysis. Cesk Rentgenol. 1960;14:27–34.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Rosenthal, A.K., Andres, M., Abhishek, A., Terkeltaub, R. (2023). CPPD and Other Microcrystalline Disorders. In: Stone, J.H. (eds) A Clinician's Pearls & Myths in Rheumatology. Springer, Cham. https://doi.org/10.1007/978-3-031-23488-0_37
Download citation
DOI: https://doi.org/10.1007/978-3-031-23488-0_37
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-23487-3
Online ISBN: 978-3-031-23488-0
eBook Packages: MedicineMedicine (R0)