
Abstract
Background
Gangliogliomas are a relatively rare neoplasm with a major incidence in the pediatric population. As the temporal lobes are the most common site, patients usually present with seizures.
Case report
We report the case of a 9-year-old child with an extensive suprasellar ganglioglioma presenting with a cerebral infarction due to direct compression of the medium cerebral artery.
Conclusions
Suprasellar lesions can compress adjacent vascular structures, so an accurate diagnosis is necessary for an early treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Primary tumors in the sella turcica and suprasellar region comprise approximately 10% of primary brain tumors in children. Craniopharyngioma is the most common lesion in these locations, accounting for almost 50% of pediatric suprasellar tumors [4, 17]. Differential diagnosis in children includes gliomas of the optic pathway and the hypothalamus, and less frequently germinoma or eosinophilic granuloma [9]. Rarely, ganglioglioma and primitive neuroectodermal tumors present in this location. The lesion has a wide range of clinical presentations depending on its site of origin and size. Pituitary dysfunction and visual difficulties are the most common [4]. Another concern is that suprasellar gangliogliomas can extend along the chiasmatic-optic pathways, so radiological differentiation from optic glioma is not always possible [5].
We report a 9-year-old child harboring a suprasellar ganglioglioma who presented with a middle cerebral artery infarction.
Case report
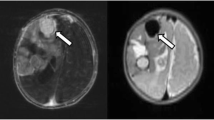
A 9-year-old Moroccan boy was referred to our institution in January 2019 because of a suprasellar lesion. Two months previously, he had been admitted to a hospital in Morocco with a strong headache and epistaxis followed by sudden left hemiparesis and gait impairment. Computed tomography (CT) performed at admission revealed an extra-axial mass in the suprasellar cistern with slight extension to the right Sylvian fissure, with central calcification, in contact with the optic chiasm, clinoid processes, and interpeduncular cistern. A hypodense right frontal area evidenced an ischemic lesion in part of the middle cerebral artery territory. Intraventricular hemorrhage was also visible, with no signs of hydrocephalus at that time. A magnetic resonance (MR) study was also performed before transfer (Fig. 1).

a, b In the MR images on admission, a low apparent diffusion coefficient in the medium cerebral artery area indicated an acute territorial infarct. c Evidence of intraventricular hemorrhage was also found in MR images, with no signs of hydrocephalus at that time.
Clinical examination at our center revealed an established right-sided spastic paresis and a limitation of lateral gaze in the left eye. An ophthalmologist noted incomplete palsy of the left 6th cranial nerve. Visual acuity and fields were normal.
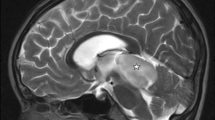
Figure 2 shows the MR findings. The tumor involved the prechiasmatic portion of both optic nerves and the chiasm and was in contact with the anterior and middle cerebral arteries. An extensive chronic stroke of the middle cerebral artery was identified, with areas of leukoaraiosis and microcystic leukomalacia. The infundibulum was centered, and the pituitary gland was not affected (Figs. 2 and 3).

Magnetic resonance imaging of suprasellar ganglioglioma. a, b The axial T2-FLAIR MR image showed the suprasellar lesion, with predominantly solid components near isointense to gray matter, and a punctate image compatible with calcium. c Sagittal T2-weighted image showed the mass with internal cysts. d Sagittal T1-weighted contrast-enhanced image showed heterogeneous enhancement of the mass approximately 22 mm in the anteroposterior plane and 25 mm transversely

3D TOF intracranial MR angiography detected narrowing in the internal carotid artery on its supra-cavernous segment, as well as in the M1 segment of the middle cerebral artery
The primary diagnostic consideration was germ-cell neoplasm versus hypothalamic glioma. Craniopharyngioma was considered less likely. No rise was detected in the serum of tumor marker levels, alpha-fetoprotein (AFP), or beta-human chorionic gonadotropin (b-HCG). His hormone profile was normal.
The patient underwent elective surgery with a right pterional craniotomy and tumor biopsy. Intraoperatively, the calibers of the anterior and middle right cerebral arteries were seen to be compromised by the mass effect of the lesion, with local perivascular arachnoiditis. The postoperative course was uneventful. As a complication of long-term corticosteroid therapy, the patient suffered a disseminated cutaneous herpes virus infection, treated for 2 weeks with daily oral acyclovir.
Pathologic analysis revealed a tumor composed of ganglion cells and neoplastic glial cells, compatible with the diagnosis of ganglioglioma. Immunohistochemistry showed positive staining of synaptophysin and chromogranin in ganglion cells, glial-fibrillary acidic protein (GFAP) in glial cells, and staining of CD34 and S100. The Ki-67 index was 2%. The biomolecular analysis detected no mutations of the IDH1 or IDH2 genes. A BRAF gene mutation in codon 600 was detected (Fig. 4).

a Tumor composed of ganglion cells and neoplastic glial cells (H & E, × 400). b Strong positive staining of GFAP in glial cells (× 200). c Immunohistochemical staining for chromogranin in ganglion cells (× 200). d Some neurons are also positive for CD34 (× 200). e Reticulin-rich matrix (× 200). f Positive Masson trichrome (× 200)
After discussion at a multidisciplinary oncological committee, the patient started treatment with dabrafenib.
Discussion
Ganglioglioma is a rare low-grade neoplasm accounting for 0.4–1.3% of all brain tumors, appearing more commonly in children and young adults. Its incidence is 7.6% [5]. The average age is approximately 12 years, with a male predominance [17].
Although these tumors may arise anywhere in the neuraxis, most are supratentorial and in the temporal lobes [16, 17]. Seizures are the most common presenting symptom, and long-standing epilepsy is frequent [15].
Gangliogliomas are characterized by CT scan as hypodense lesions with calcification and a variable contrast enhancement pattern [15]. MR imaging features are nonspecific, with isointense to hypointense T1-signal intensity and hyperintense T2-signal intensity. One-half of cases have cysts and approximately one-third calcifications. Contrast enhancement varies from none to marked and may be solid or rim-enhancing [3, 12].
Histologically, gangliogliomas are characterized by a dysplastic neuronal population accompanied by neoplastic glial cells. Up to 60% of gangliogliomas harbor a BRAF V600E mutation. BRAF is a member of the RAS/RAF/MEK/extracellular-regulated kinase pathway, and the BRAFV600E mutation is believed to mimic the activating amino acids T599 and S602, resulting in a constitutively activated protein promoting cell proliferation and differentiation. The mutant protein is predominantly expressed by the neuronal cells and has been associated with shorter recurrence-free survival [3, 6, 11].
IDH1 mutations occur in a few gangliogliomas and are associated with older age and a worse outcome, including high-grade transformation and shorter recurrence-free survival [4].
Initial management is surgical resection. Only a few supratentorial gangliogliomas have a risk of recurrence and malignant transformation within 3 years of surgery [7]. When complete resection is impossible, BRAF inhibitors, alone or with mitogen-activated protein kinase inhibitors, have had clinically meaningful responses in patients with tumors harboring a BRAF V600E mutation [11]. Radiotherapy may lead to malignant transformation and is reserved for unresectable tumors that progress [8, 10, 13].
Reversible and irreversible cerebral ischemia are uncommon complications of pituitary apoplexy, due to vasospasm following apoplexy, or mechanical compression of the nearby vascular structures [1, 14].
The suprasellar ganglioglioma described here caused stretching and compression of the middle cerebral artery, presenting with cerebral infarction in this territory. To our knowledge, no other cases of cerebral ischemia secondary to vascular compression due to a suprasellar tumor that is not pituitary apoplexy have been reported. We are only aware of two cases of intracranial gangliogliomas presenting with an intraventricular hemorrhage [2, 16]. The most likely cause of the hemorrhage in our case was a reperfusion phenomenon secondary to ischemia.
Conclusions
Suprasellar lesions can present with cerebral infarction due to direct compression over adjacent structures. Early detection of vascular compromise caused by a suprasellar mass can prevent treatment delay. The histological study is important for accurate diagnosis and treatment.
References
Abbas MS, AlBerawi MN, Al Bozom I, Shaikh NF, Salem KY (2016) Unusual complication of pituitary macroadenoma: a case report and review. Am J Case Rep 17:707–711
Bhat DI, Mahadevan A, Manish R, Sampath S, Chandramouli BA, Shankar SK (2010) Intraventricular ganglioglioma with bleed: a rare case report. Neurol India 58:477–480
Dahiya S, Haydon DH, Alvarado D, Gurnett CA, Gutmann DH, Leonard JR (2013) BRAF (V600E) mutation is a negative prognosticator in pediatric ganglioglioma. Acta Neuropathol 125(6):901–910
Horbinsky C, Kofler J, Yeaney G, Camelo-Piragua S, Venneti S, Louis DN, Perry A, Murdoch G, Nikiforova M (2011) Isocitrate dehydrogenase 1 analysis differentiates gangliogliomas from infiltrative gliomas. Brain Pathol 21:564
Karaaslan B, Uçar M, Kulduk G, Börcek AÖ, Baykaner MK (2016) Bilateral optic pathway ganglioglioma: the fifth case in the literature. Pediatr Neurosurg 51:48–54
Koelsche C, Wöhrer A, Jeibmann A, Schittenhelm J, Schindler G, Preusser M, Lasitschka F, von Deimling A, Capper D (2013) Mutant BRAF V600E protein in ganglioglioma is predominantly expressed by neuronal tumor cells. Acta Neuropathol 125:891–900
Luyken C, Blümcke I, Fimmers R, Urback H, Wiestler OD, Schramm J (2004) Supratentorial gangliogliomas: histophatologic grading and tumor recurrence in 184 patients with a median follow-up of 8 years. Cancer 101(1):146–155
Puget S, Alshehri A, Beccaria K, Blauwblomme T, Paternoster G, James S, Dirocco F, Dufour C, Zerah M, Varlet P, Sainte-Rose C (2015) Pediatric infratentorial ganglioglioma. Childs Nerv Syst 31(10):1707–1716
Resta IT, Singh A, Gilbert BC, Rojiani MV, Alleyne C, Roijani AM (2018) Suprasellar ganglioglioma: expanding the differential diagnosis. Case Rep Pathol 2018:9486064
Rumana CS, Valadka AB (1998) Radiation therapy and malignant degeneration of benign supratentorial gangliogliomas. Neurosrugery 42(5):1038–1043
Schroeder JW, Vezina LG (2011) Pediatric sellar and suprasellar lesions. Pediatr Radiol 41(3):287–298
Seeburg DP, Dremmen MH, Huisman TA (2017) Imaging of the sella and parasellar region in the pediatric population. Neuroimaging Clin N Am 27(1):99–121
Shih KC, Shastry M, Williams JT, Jelsma PF, Abram SR, Ayyanar K, Burris HA 3rd, Infante JR (2014) Successful treatment with dabrafenib (GSK2118436) in a patient with ganglioglioma. J Clin Oncol 32(29):e98–e100
Shono T, Tosaka M, Matsumoto K, Onaka S, Yamaguchi S, Mizoguchi M, Iwaki T, Nakazato Y, Sasaki T (2007) Ganglioglioma in the third ventricle: report on two cases. Neurosurg Rev 30:253–258 discussion 258
Shuangshoti S, Kirsch E, Bannan P, Fabian VA (2000) Ganglioglioma of the optic chiasm: case report and review of the literature. AJNR Am J Neuroradiol 21(8):1486–1489
Warnica W, Provias JP (2017) Intraventricular ganglioglioma with extensive hemorrhage. Clin Neuropathol 36(4):178–182
Zaky W, Patil SS, Park M, Liu D, Wang WL, Wani KM, Calle S, Ketonen L, Khatua S (2018) Ganglioglioma in children and young adults: single institution experience and review of the literature. J Neuro-Oncol 139:739–747
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Pastor, L., Iglesias, S., Ros, B. et al. Suprasellar ganglioglioma presenting as a middle cerebral artery infarction. Childs Nerv Syst 35, 1625–1628 (2019). https://doi.org/10.1007/s00381-019-04292-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-019-04292-z