
Abstract
Background
Dipeptidyl Peptidase-4 (DPP-4) inhibitors do not suppress cardiovascular events in diabetic patients with a history of cardiovascular disease. However, the effect of DPP-4 inhibitors on cardiovascular events in Japanese diabetic patients is unclear. Therefore, we investigated whether DPP-4 inhibitors alter the incidence of cardiovascular events in Japanese diabetic patients without a history of cardiovascular events.
Methods
The Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) trial was a multicenter, prospective, randomized, open label, blinded, end-point study conducted from 2002 to 2008. After completion of the JPAD trial, we followed up the patients until 2019. Patients who had had a cardiovascular event by the 2013 follow-up were excluded from the study. JPAD patients were divided into a DPP-4 group and a non-DPP-4 group based on whether they were taking DPP-4 inhibitors at the 2013 follow-up because few patients took DPP-4 inhibitors before 2013. We investigated the incidence of cardiovascular events consisting of coronary events, cerebrovascular events, heart failure requiring hospitalization, and aortic and peripheral vascular disease in 1099 JPAD patients until 2019.
Results
During the observation period from 2013 to 2019, 37 (7%) first cardiovascular events occurred in the DPP-4 group (n = 518) and 66 (11%) in the non-DPP-4 group (n = 581). The incidence of cardiovascular events was significantly lower in the DPP-4 group than in the non-DPP-4 group (Log-Rank P = 0.0065). Cox proportional hazards model analysis revealed that the use of DPP-4 inhibitors (hazard ratio 0.65; 95% confidence interval 0.43–0.98; P = 0.038) was an independent factor after adjustment for age ≥ 65 years, hypertension, statin usage, and insulin usage.
Conclusions
Our findings have demonstrated that the use of DPP-4 inhibitors may be associated with a reduced incidence of first cardiovascular events in Japanese diabetic patients. The results require confirmation in randomized controlled trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dipeptidyl peptidase-4 (DPP-4) inhibitors have several advantages over other glucose-lowering agents [1]. DPP-4 inhibitors improve glycemic control in monotherapy or combined therapy with other medications without many adverse effects [2]. DPP-4 inhibitors improve blood glucose control, reduce blood pressure, show neutral to modest beneficial effects on body weight, improve postprandial lipemia, reduce inflammatory markers, diminish oxidative stress, and improve endothelial function in diabetic patients [3,4,5,6,7,8,9,10]. Thus, DPP-4 inhibitors could reduce cardiovascular events through the improvement in risk factors. However, most studies and meta-analyses have shown that DPP-4 inhibitors do not significantly reduce cardiovascular events in Westerners [11,12,13,14,15,16,17]. These study populations mainly consisted of diabetic patients with a history of cardiovascular events. Furthermore, it is known that there is a difference in insulin secretory function between Japanese or east Asian and Westerners [18, 19].
Therefore, we sought to evaluate whether DPP-4 inhibitors alter the incidence of cardiovascular events in Japanese diabetic patients without a history of cardiovascular events.
Materials and methods
JPAD2 study
We undertook the Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) trial to examine the efficacy of low-dose aspirin therapy for the primary prevention of cardiovascular events in type 2 diabetic patients [20]. The study protocol for the JPAD trial is registered at clinicaltrials.gov with the identifier NCT00110448. The study protocol is in agreement with the guidelines of the ethics committees at Kumamoto University (Rinri 956) and Nara Medical University (No. 263), and the study complied with the Declaration of Helsinki. Briefly, this multicenter, prospective, randomized, open, clinical trial was conducted at 163 institutions throughout Japan, and 2536 type 2 diabetic patients who had no history of cardiovascular disease were enrolled. The institutional review board at each participating hospital approved this trial, and written informed consent was obtained from each patient. The inclusion criteria of the JPAD trial were a diagnosis of type 2 diabetes mellitus, 30–85 years of age, and the ability to provide informed consent. The exclusion criteria were electrocardiographic ischemic changes, a history of coronary heart disease, cerebrovascular disease, arteriosclerotic disease, atrial fibrillation, use of antiplatelet or antithrombotic therapy, a history of severe gastric or duodenal ulcer, severe liver dysfunction, severe renal dysfunction, or allergy to aspirin [20].
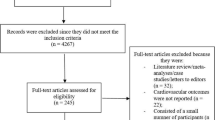
After completion of the JPAD trial in 2008, all patients were followed up biennially. The JPAD trial and its follow-up period together constitute the JPAD2 study (Fig. 1). We reported the results of the JPAD2 study using data obtained until 2015 [21]. In the present study, the JPAD patients were followed up until 2019.

JPAD trial, JPAD2 study and present study population. The Japanese primary prevention of atherosclerosis with aspirin for diabetes (JPAD) trial was a randomized controlled trial. All patients were biennially followed up after completion of the JPAD trial in 2008. The JPAD trial and its follow-up period together constitute the JPAD2 study. The present study consisting of the DPP-4 group and the non-DPP-4 group began in 2013
At the time of follow-up of JPAD patients in 2011, few patients were taking DPP-4 inhibitors. JPAD patients were divided into a DPP-4 group and a non-DPP-4 group based on whether they were taking DPP-4 inhibitors at the 2013 follow-up. None of the non-DPP-4 group had received DPP-4 by 2013. Patients who had had a cardiovascular event by the 2013 follow-up were excluded from the study. Finally, we investigated the incidence of cardiovascular events in 1099 JPAD patients who had had at least one follow-up by 2019. In the present study, cardiovascular events were defined as the following: sudden death; death resulting from coronary, cerebrovascular, and aortic causes; nonfatal acute myocardial infarction; unstable angina; newly developed exertional angina; heart failure requiring hospitalization; nonfatal ischemic and hemorrhagic stroke; transient ischemic attack; and nonfatal aortic and peripheral vascular disease.
Statistical analyses
Patient characteristics are presented as the mean ± standard deviation, median (interquartile range) or number (%). Comparisons of variables between the DPP-4 and non-DPP-4 groups were conducted using t-tests or Wilcoxon rank sum tests for continuous variables or Chi-square tests for categorical variables. We followed up the patients until the day of the first cardiovascular event or July 2019, if patients did not have a cardiovascular event. If the patients were not followed up until July 2019, they were censored on the day of their last visit. Comparisons of cardiovascular events were performed on the basis of time to the first event. The follow-up time was computed from baseline until death, or the date of last known contact. Cumulative incidences of primary end points were estimated using the Kaplan–Meier method and differences between groups were then assessed with the log-rank test. We constructed Cox proportional hazard models to estimate the hazards ratio of the DPP-4 group relative to the non-DPP-4 group, with a 95% confidence interval. We adjusted for several clinically relevant factors such as age ≥ 65 years, hypertension, use of statins, and use of insulin as confounders in the multivariable Cox proportional hazard models. Patients with missing values for any selected variable were excluded from the analyses that used this variable. All statistical analyses were conducted by a statistician (TM) from an independent data center (Institute for Clinical Effectiveness) using JMP version 15.2 (SAS Institute Inc, Cary, NS, USA). Two-tailed P-values of less than 0.05 were considered statistically significant.
Results
Baseline clinical characteristics
In the JPAD study in 2013 (Fig. 1), 1099 patients had no previous history of cardiovascular events, 518 patients were taking DPP-4 inhibitors (DPP-4 group), and 581 patients were not taking DPP-4 inhibitors (non-DPP-4 group).
The baseline clinical characteristics are shown in Table 1. There were significant differences in age, hemoglobin A1c and triglyceride levels, and in the frequency of dyslipidemia and diabetic retinopathy between the DPP-4 and non-DPP-4 groups. The use of insulin was significantly higher in the non-DPP-4 group than in the DPP-4 group. Furthermore, the use of statins was significantly higher in the DPP-4 group than in the non-DPP-4 group. Clinical characteristics such as sex, blood pressure, body mass index, estimated glomerular filtration rate, total cholesterol, high-density lipoprotein levels, duration of diabetes, the frequency of smoking and proteinuria, and the use of each antihypertensive drug were similar between the two groups.
Comparison of cardiovascular events between the DPP-4 and non-DPP-4 groups
During the observation period from 2013 to 2019, there were 37 (7%) cardiovascular events in the DPP-4 group and 66 (11%) in the non-DPP-4 group (Table 2). Fewer cardiovascular events occurred in the DPP-4 group than in the non-DPP-4 group. The frequency of coronary events, transient ischemic attack, vascular events, and sudden death were similar between the DPP-4 group and non-DPP-4 group. By contrast, the frequency of heart failure requiring hospitalization and cerebrovascular events were significantly lower in DPP-4 group than in the non-DPP-4 group: 8 (1.5%) and 10 (1.9%) events, respectively, in the DPP-4 group compared with 19 (3.3%) and 22 (3.8%) events, respectively, in the non-DPP-4 group.
Effects of administration of DPP-4 inhibitors on the incidence of cardiovascular events
The incidence of cardiovascular events was significantly lower in the DPP-4 group than in the non-DPP-4 group (Log-Rank P = 0.0065, Fig. 2). Cox proportional hazards model analysis revealed that the use of DPP-4 inhibitors (hazard ratio, 0.65; 95% confidence interval 0.43–0.98; P = 0.0377) independently reduced the incidence of cardiovascular events after adjustment for age ≥ 65 years, hypertension, statin usage, and, insulin usage (Table 3).

Comparison of cardiovascular events between the DPP-4 group and the non-DPP-4 group. The incidence of cardiovascular events was significantly reduced in the DPP-4 group compared to the non-DPP-4 group
Discussion
Our 6-year follow-up study has shown that administration of DPP-4 inhibitors may reduce the incidence of cardiovascular events in type 2 diabetic patients. This new evidence in Japanese diabetic patients reveals that the DPP-4 inhibitors might inhibit first cardiovascular events in diabetic patients without a history of cardiovascular events.
Numerous recent studies in Westerners, however, have reported that DPP-4 inhibitors do not significantly reduce cardiovascular events [11,12,13,14,15,16,17]. Differences in insulin secretory function exist between Japanese or east Asian and Westerners [18, 19]; therefore, there may be differences in the effects of DPP-4 inhibitors on the suppression of cardiovascular events. To the best of our knowledge, this is the first report to investigate the effect of DPP-4 inhibitors on suppression of cardiovascular events in Japanese diabetic patients.
Furthermore, the recent trials did not assess the cardiovascular benefits of DPP-4 inhibitors in the general population with type 2 diabetes mellitus, but assessed the cardiovascular safety of DPP-4 inhibitors in patients with very high-risk type 2 diabetes mellitus [22]. One possible cause of the negative result in the recent studies is the progress of preventive medicines such as the development and clinical prescription of intense-dose statins. The cardiovascular risk factors of patients with a history of cardiovascular events have become more tightly controlled, which may obscure the additional effect of DPP-4 inhibitors on reducing cardiovascular events. Therefore, recent studies in patients with a history of cardiovascular events may have low power to detect event-suppressing effects of DPP-4 inhibitors. Primary prevention studies, like our study, may facilitate the detection of cardiovascular event-suppressing effects of DPP-4 inhibitors.
Median follow-up in the recent studies on DPP-4 inhibitors was limited to 1.5 to 3 years [11,12,13,14,15,16,17], which may not represent sufficient time to assess the potential long-term benefits. The guidance document by the US Food and Drug Administration states that all new glucose-lowering agents must prove cardiovascular safety [23]. Therefore, many randomized controlled trials were primarily designed as noninferiority trials compared with placebo to exclude an unacceptable risk of cardiovascular events associated with DPP-4 inhibitors in the shortest possible time period [24]. The duration of these trials was rather short; therefore, the difference in hyperglycemia exposure between the two arms was probably too low to show any difference in cardiovascular events, especially in type 2 diabetic patients with advanced cardiovascular diseases [25].
Most of the recent studies used a composite, triple major adverse cardiac event as a primary outcome, which combined cardiovascular mortality, nonfatal myocardial infarction, and nonfatal stroke [11,12,13,14,15,16,17]. On the other hand, our study used a different composite, major adverse cardiac event, which included unstable angina, newly developed exertional angina, heart failure requiring hospitalization, and nonfatal aortic and peripheral vascular disease. The inhibition of cardiovascular events, especially heart failure requiring hospitalization and cerebrovascular events, was observed in our study. There are several possible mechanisms by which DPP-4 inhibitors may reduce cardiovascular events, including improved glycemic control and endothelial function and decreased lipids and blood pressure [3,4,5,6,7,8,9,10]. In the primary prevention setting, Mita et al. and Tanaka et al. showed significant inhibitory effects of aloglptin and sitagliptin on mean and maximum internal carotid artery intima-media thickness [26, 27]. An experimental study showed that linagliptin inhibited plaque growth in the brachiocephalic artery and stabilized plaque in Watanabe heritable hyperlipidemic rabbits [28]. This evidence may support the inhibition of stroke events by DPP-4 inhibitor in our data. Furthermore, in diabetic patients with acute coronary syndrome, DPP-4 inhibitors did not significantly reduce the percentage change in coronary plaque volume, but significantly reduced the percentage change in lipid plaque volume [29].
DPP-4 inhibitors decrease heart failure requiring hospitalization in diabetic patients with heart failure [30]. This finding supports our results. Moreover, DPP-4 inhibitors attenuate the severity of left ventricular fibrosis, and, thus, left ventricular diastolic dysfunction in rats [31]. Furthermore, DPP-4 inhibitors improve myocardial energy metabolism in a murine model of pressure-overloaded heart [32]. The association of DPP-4 inhibitors and better outcomes of heart failure might be partially because of these effects. Thus, DPP-4 inhibitors may still have the potential to suppress cardiovascular events in primary prevention studies even in Westerners.
Sodium glucose cotransporter 2 (SGLT2) inhibitors are associated with a significant reduction in cardiovascular events [33, 34]. In the present study, no patients had received SGLT2 inhibitors in 2013. In the DPP-4 group, SGLT2 inhibitors had been prescribed in 23 and 54 patients at the 2015 and 2017 follow-ups, respectively. In the non-DPP-4 group, SGLT2 inhibitors had been prescribed in 11 and 25 patients at the 2015 and 2017 follow-ups, respectively. Since the number of the study subject taking SGLT2 inhibitors was low and there was no significant difference in the prescription rate between the two groups, the effect of SGLT2 inhibitors on the study results is likely to be small.
Our study was a follow-up study of a randomized controlled trial. To confirm the effects of DPP-4 inhibitors on cardiovascular events, randomized controlled trials are needed. Given the current situation of type 2 diabetes, however, it may be hard to perform a new randomized clinical trial to assess the clinical benefits of DPP-4 inhibitors on cardiovascular events.
In our cohort study, we showed that DPP-4 inhibitors may have a primary preventive effect against cardiovascular events in Japanese diabetic patients. We believe that DPP-4 inhibitors are still necessary drugs for diabetes treatment even in terms of prevention of cardiovascular disease.
Our study had some limitations. First, this study was a follow-up study of the JPAD trial that was designed as a randomized controlled trial to evaluate the efficacy of low-dose aspirin, but not DPP-4 inhibitors, in preventing cardiovascular events. Second, there were some imbalances in clinical factors between the DPP-4 group and the non-DPP-4 group, and although we adjusted these, the they may have affected the results.
Conclusions
Our study suggests that the use of DPP-4 inhibitors is associated with a reduced incidence of first cardiovascular events in Japanese diabetic patients without a history of cardiovascular events. Randomized controlled trials are necessary to confirm the findings.
Data availability
The JPAD study is an ongoing cohort and data cannot be provided.
References
Scheen AJ, Paquot N (2012) Gliptin versus a sulphonylurea as add-on to metformin. Lancet 380:450–452
Deacon CF, Lebovitz HE (2016) Comparative review of dipeptidyl peptidase-4 inhibitors and sulphonylureas. Diabetes Obes Metab 18:333–347
Monami M, Iacomelli I, Marchionni N, Mannucci E (2010) Dipeptydil peptidase-4 inhibitors in type 2 diabetes: a meta-analysis of randomized clinical trials. Nutr Metab Cardiovasc Dis 20:224–235
Law MR, Morris JK, Wald NJ (2009) Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomized trials in the context of expectations from prospective epidemiological studies. BMJ 338:b1665
Horton ES, Silberman C, Davis KL, Berria R (2010) Weight loss, glycemic control, and changes in cardiovascular biomarkers in patients with type 2 diabetes receiving incretin therapies or insulin in a large cohort database. Diabetes Care 33:1759–1765
Scheen AJ (2013) Cardiovascular effects of gliptins. Nat Rev Cardiol 10:73–84
Ussher JR, Drucker DJ (2014) Cardiovascular actions of incretin-based therapies. Circ Res 114:1788–1803
Takasawa W, Ohnuma K, Hatano R, Endo Y, Dang NH, Morimoto C (2010) Inhibition of dipeptidyl peptidase 4 regulates microvascular endothelial growth induced by inflammatory cytokines. Biochem Biophys Res Commun 401:7–12
Fadini GP, Boscaro E, Albiero M, Menegazzo L, Frison V, de Kreutzenberg S, Agostini C, Tiengo A, Avogaro A (2010) The oral dipeptidyl peptidase-4 inhibitor sitagliptin increases circulating endothelial progenitor cells in patients with type 2 diabetes: possible role of stromal-derived factor-1alpha. Diabetes Care 33:1607–1609
Fadini GP, Avogaro A (2011) Cardiovascular effects of DPP-4 inhibition: beyond GLP-1. Vascul Pharmacol 55:10–16
White WB, Cannon CP, Heller SR, Nissen SE, Bergenstal RM, Bakris GL, Perez AT, Fleck PR, Mehta CR, Kupfer S, Wilson C, Cushman WC, Zannad F, EXAMINE Investigators (2013) Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 369:1327–1335
Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, Ohman P, Frederich R, Wiviott SD, Hoffman EB, Cavender MA, Udell JA, Desai NR, Mosenzon O, McGuire DK, Ray KK, Leiter LA, Raz I, SAVOR-TIMI 53 Steering Committee and Investigators (2013) Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 369:1317–1326
Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, Garg J, Josse R, Kaufman KD, Koglin J, Korn S, Lachin JM, McGuire DK, Pencina MJ, Standl E, Stein PP, Suryawanshi S, Van de Werf F, Peterson ED, Holman RR, TECOS Study Group (2015) Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med 373:232–242
Zannad F, Cannon CP, Cushman WC, Bakris GL, Menon V, Perez AT, Fleck PR, Mehta CR, Kupfer S, Wilson C, Lam H, White WB, EXAMINE Investigators (2015) Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: a multicentre, randomised, double-blind trial. Lancet 385:2067–2076
Abbas AS, Dehbi HM, Ray KK (2016) Cardiovascular and non-cardiovascular safety of dipeptidyl peptidase-4 inhibition: a meta-analysis of randomized controlled cardiovascular outcome trials. Diabetes Obes Metab 18:295–299
Xu S, Zhang X, Tang L, Zhang F, Tong N (2017) Cardiovascular effects of dipeptidyl peptidase-4 inhibitor in diabetic patients with and without established cardiovascular disease: a meta-analysis and systematic review. Postgrad Med 129:205–215
Mahmoud AN, Saad M, Mansoor H, Elgendy AY, Barakat AF, Abuzaid A, Mentias A, Elgendy IY (2017) Cardiovascular safety of incretin-based therapy for type 2 diabetes: a meta-analysis of randomized trials. Int J Cardiol 230:324–326
Fukushima M, Suzuki H, Seino Y (2004) Insulin secretion capacity in the development from normal glucose tolerance to type 2 diabetes. Diabetes Res Clin Pract 66(Suppl 1):S37–S43
Kodama K, Tojjar D, Yamada S, Toda K, Patel CJ, Butte AJ (2013) Ethnic differences in the relationship between insulin sensitivity and insulin response: a systematic review and meta-analysis. Diabetes Care 36:1789–1796
Ogawa H, Nakayama M, Morimoto T, Uemura S, Kanauchi M, Doi N, Jinnouchi H, Sugiyama S, Saito Y, Japanese primary prevention of atherosclerosis with aspirin for diabetes (JPAD) trial investigators (2008) Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA. 300:2134–2141
Saito Y, Okada S, Ogawa H, Soejima H, Sakuma M, Nakayama M, Doi N, Jinnouchi H, Waki M, Masuda I, Morimoto T, JPAD Trial Investigators (2017) Low-dose aspirin for primary prevention of cardiovascular events in patients with type 2 diabetes mellitus: 10-year follow-up of a randomized controlled trial. Circulation. 135:659–670
Chawla H, Tandon N (2017) Interpreting cardiovascular endpoints in trials of antihyperglycemic drugs. Am J Cardiovasc Drugs 17:203–215
Goldfine AB (2008) Assessing the cardiovascular safety of diabetes therapies. N Engl J Med 359:1092–1095
Zannad F, Stough WG, Lipicky RJ, Tamargo J, Bakris GL, Borer JS, Alonso García Mde L, Hadjadj S, Koenig W, Kupfer S, McCullough PA, Mosenzon O, Pocock S, Scheen AJ, Sourij H, Van der Schueren B, Stahre C, White WB, Calvo G (2016) Assessment of cardiovascular risk of new drugs for the treatment of diabetes mellitus: risk assessment vs. risk aversion. Eur Heart J Cardiovasc Pharmacother 2:200–205
Roussel R, Steg PG, Mohammedi K, Marre M, Potier L (2018) Prevention of cardiovascular disease through reduction of glycaemic exposure in type 2 diabetes: a perspective on glucose-lowering interventions. Diabetes Obes Metab 20:238–244
Tanaka A, Yoshida H, Nanasato M, Oyama JI, Ishizu T, Ajioka M, Ishiki R, Saito M, Shibata Y, Kaku K, Maemura K, Higashi Y, Inoue T, Murohara T, Node K (2018) Sitagliptin on carotid intima-media thickness in type 2 diabetes patients receiving primary or secondary prevention of cardiovascular disease: a subgroup analysis of the PROLOGUE study. Int J Cardiol 271:331–335
Mita T, Katakami N, Yoshii H, Onuma T, Kaneto H, Osonoi T, Shiraiwa T, Kosugi K, Umayahara Y, Yamamoto T, Yokoyama H, Kuribayashi N, Jinnouchi H, Gosho M, Shimomura I, Watada H, Collaborators on the Study of Preventive Effects of Alogliptin on Diabetic Atherosclerosis (SPEAD-A) Trial (2016) Alogliptin, a dipeptidyl peptidase 4 inhibitor, prevents the progression of carotid atherosclerosis in patients with type 2 diabetes: the study of preventive effects of alogliptin on diabetic atherosclerosis (SPEAD-A). Diabetes Care 39:139–148
Kurosawa T, Li Y, Sudo M, Haruta H, Hagikura K, Takayama T, Hiro T, Shiomi M, Hao H, Matsumoto T, Hirayama A, Okumura Y (2021) Effect of the dipeptidyl peptidase-4 inhibitor linagliptin on atherosclerotic lesions in Watanabe heritable hyperlipidemic rabbits: iMap-IVUS and pathological analysis. Heart Vessels 36:127–135
Kuramitsu S, Miyauchi K, Yokoi H, Suwa S, Nishizaki Y, Yokoyama T, Nojiri S, Iwabuchi M, Shirai S, Ando K, Okazaki S, Tamura H, Watada H, Daida H (2017) Effect of sitagliptin on plaque changes in coronary artery following acute coronary syndrome in diabetic patients: the ESPECIAL-ACS study. J Cardiol 69:369–376
Enzan N, Matsushima S, Kaku H, Tohyama T, Nagata T, Ide T, Tsutsui H (2023) Beneficial effects of dipeptidyl peptidase-4 inhibitors on heart failure with preserved ejection fraction and diabetes. JACC Asia 3:93–104
Nakajima Y, Ito S, Asakura M, Min KD, Fu HY, Imazu M, Hitsumoto T, Takahama H, Shindo K, Fukuda H, Yamazaki S, Asanuma H, Kitakaze M (2019) A dipeptidyl peptidase-IV inhibitor improves diastolic dysfunction in Dahl salt-sensitive rats. J Mol Cell Cardiol 129:257–265
Furukawa N, Koitabashi N, Matsui H, Sunaga H, Umbarawan Y, Syamsunarno MRAA, Yamaguchi A, Obokata M, Hanaoka H, Yokoyama T, Kurabayashi M (2021) DPP-4 inhibitor induces FGF21 expression via sirtuin 1 signaling and improves myocardial energy metabolism. Heart Vessels 36:136–146
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE, EMPA-REGOUTCOME Investigators (2015) Empagliflozin, cardio- vascular outcomes, and mortality in type 2 diabetes. N Engl J Med 373:2117–2128
Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, Law G, Desai M, Matthews DR, CANVAS Program Collaborative Group (2017) Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 377:644–657
Acknowledgements
The authors thank M. Ohtorii (Institute for Clinical Effectiveness, Kyoto, Japan) for her roles in data management and statistical analyses. The authors also thank M. Aoyama (Kumamoto University), Y. Wada, Y. Kamada, and M. Miyagawa (Nara Medical University) for their secretarial work. A part of data of the manuscript was presented in American Heart Association Scientific Sessions 2021. We thank all members of the JPAD investigators for data collection: Kimiaki Miwa (Aiiku Hospital); Kazunobu. Akahoshi (Akahoshi Clinic); Kenji Misumi (Akita Hospital); Haruo Araki (Araki Heart Clinic); Yutaka Mitsudo (Arao Central Hospital); Norifumi Kondo (Asahikawa Cardiovascular Clinic); Kenichi Ashihara (Ashihara Clinic); Shinya Yumoto (Aso Medical Center); Masashi Horimoto (Chitose City Hospital); Osamu Doi (Doi Cardiovascular Clinic); Kenichi Doijiri (Doijiri Clinic); Ryo Fukami (Fukami Clinic); Michio Shimabukuro (Fukushima Medical University); Genshi Egusa (Genshi Egusa Clinic); Kazuo Goto (Goto Clinic); Yoichi Hanaoka (Hanaoka Cardiovascular Clinic); Yoshihiro Kimura (Hanazono Medical Clinic); Yoshikuni Haraguchi, and Osamu Haraguchi (Haraguchi Gastroenterology Clinic); Atsushi Hasegawa (Hasegawa Medicine Clinic); Yoshiko Shioya, and Yosuke Shioya (Hinohikari Clinic); Eiitiro Tanaka, and Kazuhiko Yamada (Hitoyoshi internal Hospital); Toshiya Atsumi (Hokkaido University Hospital); Satoshi Tanazawa (Hokusei Hospital); Yutaka Horio (Horio Internal Medicine Clinic); Seishi Ichihara (Ichihara Clinic); Isao Yasuda (Iinan Hospital); Tsuneo Ikeda (Ikeda Internal Medical Clinic); Makoto Ikemura (Ikemura medical Clinic); Chieko Imamoto (Imamoto Clinic); Yoshihisa Iseri (Iseri Internal Medicine Clinic); Ken Iwai (Iwai Clinic); Shinya Okamoto (Iwasaki Hospital); Seigo Sugiyama (Jinnouchi Hospital); Masanori Kamura (Kamura Clinic); Hirofumi Kan (Kankaimeido Clinic); Mayumi Kiyota (Kasuga Clinic); Kyousuke Kawamura (Kawamura Internal Medicine Clinic); Takashi Ono (Kimio Ono Clinic); Takeshi Koga (Koga Clinic); Etsuo Kinuwaki, Hiromichi Naito, and Kazuo Kozuma (Konan Hospital); Kiyotaka Kudou (Kudou Internal Medicine ); Yasuhiro Morikami (Kumamoto City Hospital); Hirofumi Yasue, and Yuji Mizuno (Kumamoto Kinoh Hospital); Hisao Fujimoto (Kumamoto Onjyaku Hospital); Kozaburo Matsuyama (Kumamoto Rehabilitation Hospital); Hiromi Fujii (Kumamoto Shinto General Hospital); Syuichi Kamijikkoku (Kumamoto Takumadai Hospital); Tetsuo Kuwahara (Kuwahara Medical Clinic); Kyoji Takaoka (Kyushu Memorial Hospital); Kazuo Machii (Machii Cardiovascular Clinic); Kazutaka Maeda (Maeda Internal medical Clinic); Keiji Mahara (Mahara Internal Medicine Clinic); Akira Maki (Maki Cardiovascular Clinic); Naoki Manda (Manda Memorial Hospital); Kousuke Marutsuka, Naoki Sameshima, and Toshihiro Gi (Masuda Hospital); Terufumi Matsunaga (Matsunaga Cardiovascular Hospital); Syuichi Matsuo (Matsuo Clinic); Hiroto Okubo (Miike Hospital); Fuyuki Minagawa (Minagawa Internal Medicine Clinic); Kotaro Minoda (Minoda Cardiovascular Clinic); Junichi Miyata (Miyata Internal Medicine Clinic); Takeshi Matsuo (Miyazaki Social Insurance Hospital); Sueo Momosaki (Momosaki Internal Medicine Clinic); Tetsuo Munakata (Munakata Hospital); Tomoki Nakamura (Nakamura Clinic); Hisatoshi Nagano, Kazuto Goshi, and Keisuke Sugimoto (Namino Clinic); Shojiro Naomi (Naomi medicinal Clinic); Toshiaki Nasu (Nasu Internal Medicine Clinic); Hiroyuki Tanaka (Niko Clinic); Ryuji Sonoda (Nishimura Internal Medicine and Neurosurgery Hospital); Keizo Kajiwara (Obiyama Central Hospital); Takafumi Odo (Odo Clinic); Hirofumi Ogata (Ogata Internal Medicine Clinic); Masayuki Ogihara (Ogihara Naika Clinic); Tateo Ogura (Ogura Internal Medicine Clinic); Keishiro Oka (Oka Clinic); Eiji Kawashima (Onishi Hospital); Eiji Oshima (Oshima Medical Clinic); Ken Ozaki (Ozaki Clinic); Seiji Ozawa (Ozawa Clinic); Hiroyuki Shono (Saiseikai Misumi Hospital); Yasuhiro Sakamoto (Sakamoto Cardiovascular Clinic ); Nobuko Sakurai (Sakurai Cardiovascular Clinic); Chikashi Wakabayashi (Sapporo cardiovascular Hospital); Tomohiro Sawada (Sawada Internal Medicine Clinic); Junji Shibata (Shibata Gastroenterology Clinic); Hisashi Shimono (Shimono Cardiovascular Clinic); Akihiro Iemura (Shinmachi Iemura Clinic); Akira Matsutani (Shunan City Shinnanyo Hospital); Hisakazu Suefuji (Suefuji Cardiovascular Clinic); Hiromichi Sugiyama (Sugiyama Clinic); Jun Hokamaki, and Kenichi Komori (Tamana Central Hospital); Yoshimi Kinoshita (Tanimura Hospital); Hironori Murakami (Teinekeijinkai Hospital); Jun Hashiguchi, Yasuhiro Hashiguchi (Tempozan Naika Medical Clinic); Koryo Sawai (Terada Hospital); Atuko Hifumi (Terao Hospital); Koji Seo (Tochigi Public Health Service); Masamitsu Toihata (Toihata Internal Medicine Clinic); Koji Tokube (Tokube Internal Medicine Clinic); Hiroshi Ogawa (Tokyo Women's Medical University Hospital); Fumishi Tomita (Tomita Medical Clinic); Madoka Taguchi (Toshiba General Hospital); Toshio Tsubokura (Tsubokura Clinic); Tatsuaki Tsuchiya (Tsuchiya Clinic); Kaoru Tsuda (Tsuda Kaoru Clinic); Ryuichiro Tsurusaki (Tsurusaki Internal Medicine Clinic); Kenji Obata (Tsuruta Hospital); Katumi Watanabe, and Raisuke Hayasida (Ubuyamamura Clinic); Yutaka Ishibashi (West Shimane Medical and Welfare Center); Yoshiaki Osamura (Yamada Heart Clinic); Yoshito Yamanaka (Yamanaka Clinic); Kazuhiro Sonoda, and Taisuke Iwaoka (Yatsuda Hospital); Hiromitsu Yokota (Yokota Cardiovascular Clinic); Motoki Yoshinari (Yosinari Surgery and Internal Medicine Clinic); Nanami Abe (Abe Clinic); Noriaki Ando (Ando Medical Clinic); Hiroshi Bando (Bando Clinic); Takeshi Takami (Clinic Jingumae); Michiaki Doi (Doi Clinic); Yoshihiro Fujii (Fujii Naika Clinic); Masahiro Fukuda (Fukuda Clinic); Yoshiaki Fukuoka (Fukuoka Clinic); Masayoshi Hamano, and Minoru Takaoka (Hamano Clinic); Hiromi Hasegawa (Hasegawa Clinic); Ikuo Yabuta (Heart Land Shigisan Hospital); Kenshi Higami, and Satomi Higami (Higami Hospital); Akiko Yasuno, and Yuriko Fujinaga (Higashiyama Takeda Hospital); Yoko Onishi (Higuchi Clinic); Katsutoshi Yoshimura, Shigetoshi Minami, and Takao Nakashima (Hirao Hospital); Hiroaki Horie (Horie Clinic); Kazuko Horii (Horii Naika Clinic); Norihiko Matsumura (Horii Clinic); Tetsuo Ikuno (Ikuno Clinic); Yoshiyuki Katsuyama (Katsuyama Naika Clinic); Shiro Uemura (Kawasaki Medical School Hospital); Masao Kikukawa (Kikukawa Clinic); Masao Kanauchi (Kio University); Hideshi Kuzuya, and Arata Iwasaki (Kousekai Clinic); Takehiko Koutani (Koutani Clinic); Hisaharu Makino (Makino Clinic); Hiroshi Miki (Miki Clinic); Susumu Misugi (Misugi Clinic); Masaki Naito, and Masatoshi Naito (Naito Hospital); Yukitaka Nakano (Nakano Clinic); Akira Nakatani (Nakatani Clinic); Fumihiko Nakatani (Nakatani Naika Clinic); Manabu Horii, and Matahiro Yabuta (Nara City Hospital); Ayako Seno, Hiroyuki Kawata, Kenichi Samejima, Kenji Onoue, Rika Kawakami, Tomoya Nakano, Tomoya Ueda, Tsunenari Soeda, and Yoko Kita (Nara Medical University); Fumitaka Inoue (Nara Prefecture General Medical Center); Shigeru Yamano (Nara Prefecture General Rehabilitation Center); Hajime Iwama, Hirokazu Sakan, Megumi Suzuki, Tadashi Kagoshima, Takehito Nakai, Toshio Hashimoto, Yoshiharu Nishitani, and Yoshiyuki Kobayashi (Nara Prefecture Western Medical Center); Koichi Hoda (Nara Seibu Hospital); Junko Uejima, Yoshinobu Morikawa, and Takahiro Kawano (Nara South Medical Center); Hideki Yamada (Nijo Ekimae Clinic); Kazuo Nishimoto (Nishimoto Medical Clinic); Kyouyuki Ohsumi (Ohsumi Naika Clinic); Nobushige Ote (Ote Naika Clinic); Akiko Oya (Oya Clinic); Kimiaki Nishiura (Oyodo Hospital); Joji Masuda, Keiichiro Ban, and Yusuke Kyoda (Saiseikai Gose Hospital); Izumi Sawada, and Yoko Sawada (Sawada Hospital); Koichi Okada (Sawai Hospital); Akihiro Yazaki, Masakazu Hanatani (Shiraniwa Hospital); Toshio Sutani (Sutani Clinic); Yuko Hiramori (Takanohara Suzuran Clinic); Yuya Tanaka (Tanaka Naika Clinic); Toshiro Igaki, and Yukio Tomioka (Tomioka Naika Clinic); Hideo Shiiki, Kiyotaka Sugihara, Motomu Hayashi, Yasunobu Sasaki, and Yasuo Matsukura (Uda City Hospital); Michiaki Ueda (Ueda Clinic); Masakuni Ueyama (Ueyama Clinic); Hideto Uyama (Uyama Clinic); Hiroharu Yamada (Yamada Clinic); Kenichi Yamaga (Yamaga Clinic); Tamio Nakajima (Yamatokashihara Hospital); Kazumi Yoshimoto (Yoshimoto Clinic); Midori Yoshimura (Yoshimura Clinic).
Kimiaki Miwa, Kazunobu Akahoshi, Kenji Misumi, Haruo Araki, Yutaka Mitsudo, Norifumi Kondo, Kenichi Ashihara, Shinya Yumoto, Masashi Horimoto, Osamu Doi, Kenichi Doijiri, Ryo Fukami, Michio Shimabukuro, Genshi Egusa, Kazuo Goto, Yoichi Hanaoka, Yoshihiro Kimura, Yoshikuni Haraguchi, Osamu Haraguchi, Atsushi Hasegawa, Yoshiko Shioya, Yosuke Shioya, Eiitiro Tanaka, Kazuhiko Yamada, Toshiya Atsumi, Satoshi Tanazawa, Yutaka Horio, Seishi Ichihara, Isao Yasuda, Tsuneo Ikeda, Makoto Ikemura, Chieko Imamoto, Yoshihisa Iseri, Ken Iwai, Shinya Okamoto, Seigo Sugiyama, Masanori Kamura, Hirofumi Kan, Mayumi Kiyota, Kyousuke Kawamura, Takashi Ono, Takeshi Koga, Etsuo Kinuwaki, Hiromichi Naito, Kazuo Kozuma, Kiyotaka Kudou, Yasuhiro Morikami, Hirofumi Yasue, Yuji Mizuno, Hisao Fujimoto, Kozaburo Matsuyama, Hiromi Fujii, Syuichi Kamijikkoku, Tetsuo Kuwahara, Kyoji Takaoka, Kazuo Machii, Kazutaka Maeda, Keiji Mahara, Akira Maki, Naoki Manda, Kousuke Marutsuka, Naoki Sameshima, Toshihiro Gi, Terufumi Matsunaga, Syuichi Matsuo, Hiroto Okubo, Fuyuki Minagawa, Kotaro Minoda, Junichi Miyata, Takeshi Matsuo, Sueo Momosaki, Tetsuo Munakata, Tomoki Nakamura, Hisatoshi Nagano, Kazuto Goshi, Keisuke Sugimoto, Shojiro Naomi, Toshiaki Nasu, Hiroyuki Tanaka, Ryuji Sonoda, Keizo Kajiwara, Takafumi Odo, Hirofumi Ogata, Masayuki Ogihara, Tateo Ogura, Keishiro Oka, Eiji Kawashima, Eiji Oshima, Ken Ozaki, Seiji Ozawa, Hiroyuki Shono, Yasuhiro Sakamoto, Nobuko Sakurai, Chikashi Wakabayashi, Tomohiro Sawada, Junji Shibata, Hisashi Shimono, Akihiro Iemura, Akira Matsutani, Hisakazu Suefuji, Hiromichi Sugiyama, Jun Hokamaki, Kenichi Komori, Yoshimi Kinoshita, Hironori Murakami, Jun Hashiguchi, Yasuhiro Hashiguchi, Koryo Sawai, Atuko Hifumi, Koji Seo, Masamitsu Toihata, Koji Tokube, Hiroshi Ogawa, Fumishi Tomita, Madoka Taguchi, Toshio Tsubokura, Tatsuaki Tsuchiya, Kaoru Tsuda, Ryuichiro Tsurusaki, Kenji Obata, Katumi Watanabe, Raisuke Hayasida, Yutaka Ishibashi, Yoshiaki Osamura, Yoshito Yamanaka, Kazuhiro Sonoda, Taisuke Iwaoka, Hiromitsu Yokota, Motoki Yoshinari, Nanami Abe, Noriaki Ando, Hiroshi Bando, Takeshi Takami, Michiaki Doi, Yoshihiro Fujii, Masahiro Fukuda, Yoshiaki Fukuoka, Masayoshi Hamano, Minoru Takaoka, Hiromi Hasegawa, Ikuo Yabuta, Kenshi Higami, Satomi Higami, Akiko Yasuno, Yuriko Fujinaga, Yoko Onishi, Katsutoshi Yoshimura, Shigetoshi Minami, Takao Nakashima, Hiroaki Horie, Kazuko Horii, Norihiko Matsumura, Tetsuo Ikuno, Yoshiyuki Katsuyama, Shiro Uemura, Masao Kikukawa, Masao Kanauchi, Hideshi Kuzuya, Arata Iwasaki, Takehiko Koutani, Hisaharu Makino, Hiroshi Miki, Susumu Misugi, Masaki Naito, Masatoshi Naito, Yukitaka Nakano, Akira Nakatani, Fumihiko Nakatani, Manabu Horii, Matahiro Yabuta, Ayako Seno, Hiroyuki Kawata, Kenichi Samejima, Kenji Onoue, Rika Kawakami, Tomoya Nakano, Tomoya Ueda, Tsunenari Soeda, Yoko Kita, Fumitaka Inoue, Shigeru Yamano, Hajime Iwama, Hirokazu Sakan, Megumi Suzuki, Tadashi Kagoshima, Takehito Nakai, Toshio Hashimoto, Yoshiharu Nishitani, Yoshiyuki Kobayashi, Koichi Hoda, Junko Uejima, Yoshinobu Morikawa, Takahiro Kawano, Hideki Yamada, Kazuo Nishimoto, Kyouyuki Ohsumi, Nobushige Ote, Akiko Oya, Kimiaki Nishiura, Joji Masuda, Keiichiro Ban, Yusuke Kyoda, Izumi Sawada, Yoko Sawada, Koichi Okada, Akihiro Yazaki, Masakazu Hanatani, Toshio Sutani, Yuko Hiramori, Yuya Tanaka, Toshiro Igaki, Yukio Tomioka, Hideo Shiiki, Kiyotaka Sugihara, Motomu Hayashi, Yasunobu Sasaki, Yasuo Matsukura, Michiaki Ueda, Masakuni Ueyama, Hideto Uyama, Hiroharu Yamada, Kenichi Yamaga, Tamio Nakajima, Kazumi Yoshimoto, Midori Yoshimura
Funding
This study was supported by the Ministry of Health, Labour and Welfare of Japan (H16-Junkanki-004, and H27-Junkanki-Ippan-001). The study funder was not involved in the design of the study; the collection, analysis, and interpretation of data; writing the report; and did not impose any restrictions regarding the publication of the report.
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed to the study conception and design. Data collection was performed by HS and SO. Data analysis were performed by TM. The first draft of the manuscript was written by HS and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Dr Soejima reports lecturer's fees from Kowa. Dr Ogawa reports lecturer's fees from Bayer, Bristol-Myers Squibb, and Towa; manuscript fee from Novartis. Dr Morimoto reports lecturer's fees from Bristol-Myers Squibb, Daiichi Sankyo, Japan Lifeline, Kowa, Kyocera, Novartis, and Toray; manuscript fees from Bristol-Myers Squibb and Kowa; advisory board for Sanofi. Dr Okada reports lecturer's fees from AstraZeneca, Eli Lilly, Mitsubishi Tanabe, Novartis, Ono, Sumitomo Dainippon, and Takeda. Dr Nakayama reports research grants from Bayer; lecturer's fees from Astellas Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eisai, Kowa, Nippon Shinyaku, Ono, Otsuka, Pfizer, Sumitomo Dainippon, and Takeda. Dr Masuda reports lecturer's fees from Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Kowa, Mitsubishi Tanabe, MSD, Ono, Shionogi, and Takeda. Dr Jinnouchi reports research grants from Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Chugai, Daiichi Sankyo, Eli Lilly, GlaxoSmithKline, MSD, Novo Nordisk, Ono, Pfizer, Sanofi, Sanwa Kagaku Kenkyusho, Shionogi, Taisho Toyama, and Takeda; lecturer's fees from Abbott, Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Kyowa Hakko Kirin, Mitsubishi Tanabe, MSD, Novo Nordisk, Sanofi, Sanwa Kagaku Kenkyusho, Taisho Toyama, Takeda, Teijin, and Terumo; manuscript fees from Novo Nordisk and Taisho Toyama. Dr Waki reports research grants from AstraZeneca, Eli Lilly, and Sanofi; lecturer's fees from Abbott, Astellas, Astellas Amgen Bio Pharma, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Kowa, Kyowa Hakko Kirin, Mitsubishi Tanabe, MSD, Novartis, Novo Nordisk, Ono, Otsuka, Sanofi, Sanwa Kagaku Kenkyusho, Sumitomo Dainippon, Taisho Toyama, Takeda, and Teijin. Dr Saito reports research grants from Actelion, Astellas, Astellas Amgen Bio Pharma, Bayer, Cmic, Daiichi Sankyo, EP‐CRSU, Japan Lifeline, Kowa, Mebix, Meditrix, Novartis, Ono, Roche Diagnostics, and Terumo; non-purpose research grants from Astellas, Chugai, Daiichi Sankyo, Fuji Yakuhin, Kowa, Kyowa Hakko Kirin, Medtronic, Mitsubishi Tanabe, MSD, Nihon Medi-Physics, Ono, Otsuka, Sanofi, Shionogi, Sumitomo Dainippon, Takeda, and Teijin; lecturer’s fees from Alnylam, Asahi Kasei, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Janssen, Kowa, Mitsubishi Tanabe, MSD, Novartis, Ono, Otsuka, Pfizer, Taisho Toyama, Takeda, and Toa Eiyo; manuscript fees from Asahi Kasei and Novartis; advisory boards for Amgen, Bayer, Boehringer Ingelheim, Mitsubishi Tanabe, Novartis, Ono, Pfizer, and Roche Diagnostics. The other authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Soejima, H., Ogawa, H., Morimoto, T. et al. Dipeptidyl peptidase-4 inhibitors reduce the incidence of first cardiovascular events in Japanese diabetic patients. Heart Vessels 38, 1371–1379 (2023). https://doi.org/10.1007/s00380-023-02291-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-023-02291-4