
Abstract
Purpose
For renal stones < 2 cm, guidelines recommend the use of retrograde intrarenal surgery as a first line treatment option. Many available single use flexible ureteroscopy were found. We aim to compare the effectiveness of two single use flexible ureteroscopy; Pusen Uscope 3011 versus LithoVue in the management of renal stones less than 2 cm.
Methods
Our study prospectively included 60 patients equally divided in to two groups: Pusen group and LithoVue group during the period from June 2020 to June 2021. The included patients were above 18 years old. Perioperative details as operative time, fluoroscopy time, hospital stay, and complications were recorded. Stone free rate was assessed. Base purchase cost was also compared.
Results
There was no statistically significant difference between the two groups regarding age, gender, and body mass index (BMI), stones size, side, number and location. The perioperative evaluation and outcome had no statistically significant differences between the two groups regarding the operative time, hospital stay, access sheath use, and stone free rate or radiation exposure. Among all cases, we had 49 cases (81.6%) with no postoperative complications (21 cases for Pusen group and 28 cases for LithoVue group). The incidence of postoperative complications was significantly higher among Pusen group than LithoVue group (p = 0.02). Initial purchase cost for both FURS had no significant difference (P = 0.86).
Conclusion
RIRS can be performed effectively with Pusen 3011 and LithoVue single use flexible ureteroscopy in patients diagnosed with renal calculi < 2 cm with superior outcomes with LithoVue.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Urinary urolithiasis is one of the most common diseases in the urology field (approximately 12% of the world’s population). [1] For renal stones < 2 cm, guidelines from the European and American Urological Associations recommend the use of retrograde intrarenal surgery (RIRS) as a first line treatment option, alternative to extracorporeal shock wave lithotripsy (SWL) or percutaneous nephrolithotomy (PCNL) [2] [3].
In 1964, the endoscopic access to the renal collecting systems was firstly introduced [4] and with technical and optical improvements; RIRS has become a more widespread approach. Currently, there is a variety of flexible ureteroscopes (FURS) available, including reusable and disposable ureteroscopes and due to the high cost, limited durability and lack of need for sterilization; the disposable FURS have been developed to overcome some of the limitations of reusable FURS [5]. Also, only experienced hands can use reusable FURS perfectly without damage, on the other hand, single use FURS can be performed by juniors very easy so, advantages of single use FURS gaining more popularity [6].
Many single use FURS are found commercially. Pusen Uscope UE3011 (Zhuhai Pusen Medical Technology Co., Ltd. China) and LithoVue (Boston Scientific, Marlborough, MA) were the first digital single use FURS in the Egyptian market. The Pusen Uscope UE3011, has the same dimensions and deflection as the LithoVue, but is designed with a semiflexible shaft and a flexible tip only. Also, the design of the handle differs; the Pusen UE3011 provides a pistol-like handle [7]. In this study, we aimed to compare the effectiveness of Pusen Uscope 3011 versus LithoVue FURS in the management of renal stones less than 2 cm.
Methods
This prospective study was carried out at Urology department, Menoufia university hospitals, Egypt during the period from June 2020 to June 2021. Sixty patients were included and were randomly divided into two groups: Pusen group and LithoVue group. The study protocol was approved from the Ethics Committee of our faculty and university. The included patients were above 18 years old with renal stones up to 2 cm. An informed consent was obtained from all patients. Patients with renal or skeletal anomaly, ureteral stone, chronic kidney disease, solitary kidney, stones in calyceal diverticulum and patient with coagulopathy were excluded from the study.
All patients were preoperatively evaluated by medical history, examination, routine pre-operative investigations including urine culture, pelvi-abdominol ultrasound, plain X ray (KUB) and spiral C.T scan. Preoperative antibiotic prophylaxis had given according to the culture and sensitivity test. After general anesthesia, the patient was placed in the dorsal lithotomy position. With cystoscopy, identification of ureteric orifice and a hydrophilic guide wire was introduced. Diagnostic semi-rigid ureteroscopy was done to assess the ureter. Next, 12 F / 45 cm ureteric access sheath (UAS) (Coloplast, PORGES, France) was placed through the wire under fluoroscopy guidance. Retrograde access to the upper urinary tract was obtained with one of both types of FURS. Once the calculus is seen, 200 µm laser fiber was inserted for lithotripsy. The lithotripsy stopped when small stone fragments (< 3 mm) were seen. Small stones and fragments were retrieved with a 1.9 F zero tip nitinol basket. A 5-6Fr/ 26–28 cm double J stent was inserted routinely at the end of the procedure for both prevention and treatment of ureteral obstruction or infection complications following FURS.
Perioperative details as operative time, fluoroscopy time, hospital stay, and complications were recorded. Stone free rate (SFR) was assessed by plan abdominal X-ray (KUB) and ultrasound after 1 week and by spiral CT scan after 2 months. Base purchase cost was also compared because it is an important factor in every country health system.
The data were collected, tabulated, and analyzed by SPSS (statistical package for social science) version 17.0 on IBM compatible computer (SPSS Inc., Chicago, IL, USA). Qualitative data were described as number and percentage. Shapiro–Wilk test was used to verify the normality of distribution. Quantitative data were expressed as mean and standard deviation and qualitative data was compared using chi square and Fisher's Exact test. Significance level was considered at 0.05.
Results
The study included 30 patients in each group with mean age 45 years and average stone volume 13.5 ± 3.9 mm3 for Pusen group and mean age 43 years with average stone volume 13.3 ± 3.3 mm3 for LithoVue group. Most of the cases, 55 cases (91.7%), were with single stones. There was no statistically significant difference between the two groups regarding age, gender and body mass index (BMI), stones size, side, number and location. Detailed patient demographic parameters and stone characteristics were summarized in Table 1.
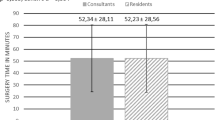
As regard operative time, it was 90 ± 45.5 min in Pusen group and 89.2 ± 41.4 min in LithoVue group. Hospital stay was 36 ± 34.22 h in Pusen group and 34 ± 33.67 h for LithoVue group.
We had 20 cases stone free (66.7%), 7 cases with residual fragments (5–7 mm) (23.3%) and 3 cases with failed procedure (10%) in Pusen group but, in LithoVue group, we had 24 cases stone free (80%), 4 cases with residual fragment (13.3%) and 2 cases with failed procedure (6.7%). Stone free defined by no residual stone or insignificant residual stones ≤ 4 mm [8]. Regarding preoperative stenting, we had total 32 cases with prior stenting and 28 cases not stented pre-operatively. In Pusen group, 17 cases (56.7%) had prior stenting versus 15 cases (50%) stented preoperatively in LithoVue group. SFR had no significant difference between the two groups (p = 0.3) and preoperative stenting had also no significant difference (p = 0.6).
Among all cases we had 49 cases (81.6%) with no postoperative complications (21 cases for Pusen group and 28 cases for LithoVue group). There were six cases (10%) where patients suffered from post-operative fever (Clavien classification grade II) due to urinary tract infection (UTI), five cases of them in Pusen group versus one case in LithoVue group (P = 0.03). Mild hematuria (Clavien classification grade I) were found in three cases in Pusen group and one case in LithoVue group (P = 0.01). There is only one case with intraoperative ureteric mucosal injury (Clavien classification grade I) caused by UAS (P = 0.1). The perioperative evaluation and outcome are illustrated in Table 2 with no statistically significant differences between the two groups regarding the operative time, hospital stay, preoperative stenting, access sheath use, and SFR or radiation exposure but, the incidence of postoperative complications was significantly higher among Pusen group than LithoVue group (p < 0.05). Initial purchase cost was 875 US dollar for Pusen FURS versus 1000 US dollar for LithoVue FURS with no significant difference between the two groups (P = 0.86).
Discussion
Since 2020, we managed our cases with renal stone < 2 cm with FURS instead of SWL or PCNL. In this study, there was no statistically significant difference between the two groups regarding age, gender and body mass index (BMI), stones size, side, number and location. The mean operation time was 90.7 ± 45.5 min for Pusen group and 89.2 ± 41.4 for LithoVue group, which little longer than the operation time in the study done by Guisti et al., 2016 (80 ± 35.5 min) [9]. It was due to our early experience in usage of single use FURS. Kuroda et al., 2018 also predict 6 causes of increase FURS operative time (preoperative stent, stone volume, maximum HFU, ureteral access sheath diameter, patient sex and lastly operator experience) [10].
Regarding stone free rate (SFR), we had 20 cases stone free (66.7%), 7 cases with residual fragments (5–7 mm) (23.3%) and 3 cases with failed procedure (10%) in Pusen group but, in LithoVue group, we had 24 cases stone free (80%), 4 cases with residual fragment (13.3%) and 2 cases with failed procedure (6.7%). In the study done by Ekici et al., 2019 the SFR was 67% after the first session of FURS and 90% after second session [11]. This was similar to our study as the stone free rate ranged from 67 to 80%. Other studies showed higher SFR than our study as Jessen et al., 2014 who reported about 88% stone free rate among 111 cases with calyceal stones [12]. We had 25 cases of lower calyx stones (41.7%); 68% were stone free and 32% with residual (< 4 mm), with no significant difference between the two groups. Our results were parallel to Xun et al., 2020 in which stone free rate in lower calyceal stones about 70% [13].
Portis et al., in 2014 concluded that any residual fragment may be associated with high risk of regrowth and retreatment [14] so, for residual stone (5–7 mm), retreatment with SWL was performed. For asymptomatic stones < 4 mm, we would not intervene. Intervention is indicated if there was evidence of persistent infection.
UAS was used successfully in 23 cases (76.7%) in Pusen group and in 20 cases (70%) in LithoVue group (P = 0.56). The use of ureteral access sheath (UAS) is useful to facilitate ureteric entry, decrease operative time, decrease intrarenal pressure which may decrease the postoperative UTI and less traumatism to the scopes [15]. Failed procedure was due to the complex renal anatomy or due to neglected DJ with severe peri-ureteritis, which make the ureter not malleable to introduce the FURS. Sanguedolce et al., 2017 concluded that the efficacy of RIRS depends on stone (composition, number, and size), anatomical site (e.g., lower pole) and surgeon (volume/experience) characteristics [16]. PCNL was done for non-accessible stones.
Among all cases, we had 49 cases (81.6%) with no postoperative complications (21 cases for Pusen group (A) and 28 cases for LithoVue group). There were six cases (10%) suffered from post-operative fever (grade II) due to urinary tract infection (UTI), five cases of them in Pusen group versus one case in LithoVue group (p = 0.03) (Table 2). All cases managed conservatively by fluids, antibiotics and antipyretics with no serious outcomes. Postoperative hematuria (grade I) were found in four cases (6.7%), three cases in Pusen group and one case in LithoVue group (P = 0.01). It was managed conservatively with fluids and hemostatic agents.
Fever and hematuria were with higher incidence among Pusen group due to inferior image quality of Pusen device (Fig. 1) and in whom the access sheath was not used. The Pusen Uscope UE3011 is designed with a semiflexible shaft and a flexible tip only. We think this made Pusen FURS was more difficult in negotiation in pelvicalyceal system with more traumas to renal mucosa. Relative poor vision needs more wash for good vision which leads to increase in hematuria and intrarenal pressure with increase in incidence of UTI and fever. Immediate postoperative of 5-points Likert score survey had been sent to the surgeons to assess image quality between the two devices. Grading was on a scale from 1 to 5 corresponding to very poor to very good. Pusen group was 2 ± 1 and LithoVue group was 4 ± 1 that was significantly clear image with LithoVue group. This was parallel to Marchini et al., 2018 in which LithoVue had a higher resolution power than Pusen 3011 FURS [17]. Recently, Pusen has introduced a modified version (Pusen UE3022) with improved image quality and mechanical performance to overcome drawbacks of Pusen UE3011.

Image quality of Pusen Uscope (UE3011) (A) versus LithoVue FURS (B) (colour figure online)
There is also one case with intraoperative ureteric mucosal injury caused by UAS which was managed by removal of access sheath and double J insertion (p = 0.1). Traxer and Thomas, 2013 demonstrated a large study of 359 cases of introduction of 12\14 Fr UAS, in which 167 cases had visible ureteric injury, 86% of them with low grade injury (injury of mucosal and not reach to smooth muscle), 10% with high grade injury (extending to smooth muscle) [18]. In The Clinical Research Office of the Endourological Society (CROES) URS Global Study, the complications among 11,885 worldwide patients who underwent URS are introduced. The most frequent complications were fever, bleeding and failed procedures. The overall complication rate was 7.4% which are comparable with our results [19].
Despite the effectiveness of FURS, the high costs hinder FURS being embraced worldwide, particularly in developing countries [20]. Variability in reusable FURS costs is determined by the initial purchase price, the cost of repair and the cost associated with sterile reprocessing whereas the cost of single use FURS is defined with the initial purchase price only [21]. Comparing baseline purchase price of both FURS provided by the manufacturer in our study was insignificant (P = 0.86) (Table 3).
We think that we are the first study in Egypt comparing these two types of FURS and we had several potential limitations that should be considered. First, sample size was relatively small. The studies with a small sample size were more likely to overestimate the treatment effect than those with larger sample sizes. Second, the mechanical and irrigation properties of both single use FURS were not investigated.
Conclusion
RIRS can be performed effectively with Pusen 3011 and LithoVue single use flexible ureteroscopy in patients diagnosed with renal calculi less than 2 cm with superior outcomes with LithoVue.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CT scan:
-
Computerized tomography
- FURS:
-
Flexible ureteroscopy
- PNL:
-
Percutaneous nephrolithotomy
- SWL:
-
Extracorporeal shockwave lithotripsy
- SFR:
-
Stone free rate
- US:
-
Ultrasound
- UAS:
-
Ureteral access sheath
- URS:
-
Ureteroscopy
- UTI:
-
Urinary tract infection
References
Li Y et al (2021) Comparison of single-use and reusable flexible ureteroscope for renal stone management: a pooled analysis of 772 patients. Transl Androl Urol 10(1):483–493
Turk C et al (2016) EAU guidelines on interventional treatment for urolithiasis. Eur Urol 69(3):475–482
Assimos D et al (2016) Surgical management of stones: american urological association/endourological society guideline. PART I J Urol 196(4):1153–1160
Marshall VF (1964) Fiber optics in urology. J Urol 91:110–114
Emiliani E, Traxer O (2017) Single use and disposable flexible ureteroscopes. Curr Opin Urol 27(2):176–181
Talso M et al (2019) Reusable flexible ureterorenoscopes are more cost-effective than single-use scopes: results of a systematic review from PETRA Uro-group. Trans Androl Urol 8(Suppl 4):S418
Schlager D et al (2020) Current disposable ureteroscopes: performance and limitations in a standardized kidney model. J Endourol 34(10):1015–1020
Deters LA et al (2011) Evaluating the definition of “stone free status” in contemporary urologic literature. Clin Nephrol 76(5):354–357
Giusti G et al (2016) Current standard technique for modern flexible ureteroscopy: tips and tricks. Eur Urol 70(1):188–194
Kuroda S et al (2018) A new prediction model for operative time of flexible ureteroscopy with lithotripsy for the treatment of renal stones. PLoS ONE 13(2):e0192597
Ekici M et al. All-seeing-access sheath: a novel fluoroscopy-free placement technique in retrograde intrarenal surgery. 2019.
Jessen JP et al (2014) Flexible ureterorenoscopy for lower pole stones: influence of the collecting system’s anatomy. J Endourol 28(2):146–151
Xun Y et al. A novel clinical-radiomics model pre-operatively predicted the stone-free rate of flexible ureteroscopy strategy in kidney stone patients. Front Med 2020. 7.
Portis AJ et al (2014) Retreatment after percutaneous nephrolithotomy in the computed tomographic era: long-term follow-up. Urology 84(2):279–284
Monga M et al (2004) Prospective randomized comparison of 2 ureteral access sheaths during flexible retrograde ureteroscopy. J Urol 172(2):572–573
Sanguedolce F et al (2017) The evolving role of retrograde intrarenal surgery in the treatment of urolithiasis. Eur Urol Focus 3(1):46–55
Marchini GS et al (2018) In vitro evaluation of single-use digital flexible ureteroscopes: a practical comparison for a patient-centered approach. J Endourol 32(3):184–191
Traxer O, Thomas A (2013) Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol 189(2):580–584
de la Rosette J et al (2014) The clinical research office of the endourological society ureteroscopy global study: indications, complications, and outcomes in 11,885 patients. J Endourol 28(2):131–139
Proietti S et al (2016) Comparison of new single-use digital flexible ureteroscope versus nondisposable fiber optic and digital ureteroscope in a cadaveric model. J Endourol 30(6):655–659
Scotland KB, Chan JYH, Chew BH (2017) Single-use flexible ureteroscopes: how do they compare with reusable ureteroscopes? J Endourol 33(2):71–78
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
FZ: surgical procedure and manuscript writing. ME: surgical procedure and final manuscript revision. HK: data collection and analysis. BS: protocol development.
Corresponding author
Ethics declarations
Conflict of interest
None.
Research involving human participants and/or animals
The study was approved by Menoufia university—Faculty of medicine ethics committee. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
The study protocol was approved by our local ethical committee. All participants signed written informed consent before inclusion in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zanaty, F., Elshazly, M., Kandeel, H. et al. A single center comparative study of two single use digital flexible ureteroscopy in the management of renal stones less than 2 cm. World J Urol 41, 777–782 (2023). https://doi.org/10.1007/s00345-023-04290-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-023-04290-6