
Abstract
The aim of the study is to investigate the impact of SELP and IL-6 genetic single-nucleotide polymorphisms (SNPs) and its gene–gene interaction on cardiovascular disease (CVD) risk based on Chinese population. A total of 1082 subjects (519 males, 563 females), with a mean age of 53.9 ± 13.1 years, were selected, including 540 CVD patients and 542 normal control participants. Logistic regression model was used to examine the association between six SNPs and CVD risk. Odds ratio (OR) and 95% confident interval (95% CI) were calculated. Generalized multifactor dimensionality reduction (GMDR) was employed to analyze the gene–gene interaction. CVD risk was significantly higher in carriers with rs1800805-A allele than those with GG genotype (GA + AA vs. GG), adjusted OR (95% CI) = 1.69 (1.31–2.16), and CVD risk was also higher in carriers with rs6136-AC or CC genotype than those with AA genotype (AC + CC vs. AA), adjusted OR (95% CI) = 1.78 (1.28–2.26), and higher in carriers with rs1800796-GC or CC genotype than those with GG genotype (CC + GC vs. GG), adjusted OR (95% CI) = 1.67 (1.25–2.14). GMDR analysis suggested a significant two-locus model (p = 0.0010) involving rs1800805 and rs1800796. Overall, the cross-validation consistency of this model was 10/10, and the testing accuracy was 62.17%, and participants with rs1800805-GA or AA and rs1800796-GC or CC genotype have the highest CVD risk, compared to participants with rs1800805-GG and rs1800796-GG genotypes, and OR (95% CI) was 2.52 (1.81–2.66). Our results support an important association of rs1800805, rs6136 minor allele of SELP gene, rs1800796 within IL-6 gene, and additional interaction between rs1800805 and rs1800796 with increased risk of CVD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cardiovascular disease (CVD), including heart disease, vascular disease, and atherosclerosis, is the most critical global health threat, and in many countries the prevalence has been decreasing over the last decades (Nichols et al. 2012; Go et al. 2013). This widespread, addictive habit is now proven causal of many diseases, including CVD (U.S. Department of Health and Human Services 2004).
The human SELP gene maps on chromosome 1q22eq25 and is organized in 17 exons that span about 40 kb (Johnston et al. 1990). To date, polymorphic variants of SELP have been intensively studied in the pathogenesis of atherosclerotic and inflammatory diseases, including CVD and myocardial infarction (MI) (Ghazouani et al. 2009; Pasquali et al. 2010; Elmas et al. 2010). Large quantities of evidence have suggested that SELP genetic polymorphisms may contribute to an increased risk of CVD; however, the results of these studies were inconsistent (Carter et al. 2003; Kee et al. 2000). The IL-6 gene was mapped to chromosome 7 at p21 (Ray et al. 1990). Studies have identified that single-nucleotide polymorphisms (SNPs) in the promoter regions of the IL-6 gene were mediators for the circulation of mRNA and IL-6 levels and the status of inflammation (Yeh et al. 2010; Pereira et al. 2011). Several studies have reported the association between the IL-6 gene SNPs and CHD susceptibility in different populations (Basso et al. 2002; Humphries et al. 2001; Wei et al. 2006). However, these studies could not conclude a certain and definitive conclusion. In addition, the pathogenesis of CVD is diverse, including both genetic and environmental factors. However, till now, only a less number of studies have focused on the influence of gene–gene interaction among several SNPs on CVD susceptibility. Given the conflicting evidence on SELP and IL-6 gene–CVD association and missing on gene–gene interaction, we conducted this case–control study to investigate the impact of SELP and IL-6 genetic polymorphisms and its interactions on CVD risk based on Chinese population.
Materials and methods
Subjects
Participants were consecutively recruited between July 2012 and December 2014 from Tianjin Chest Hospital. All patients were confirmed by clinical diagnosis. CVD cases were diagnosed according to the following events: interventional therapy of coronary artery (cardiac catheterization, percutaneous coronary intervention, or coronary artery bypass grafting), stable angina pectoris, unstable angina pectoris, the first occurrence of acute MI, congestive heart failure caused by myocardial ischemia after baseline investigation, ischemic stroke, hemorrhagic stroke, and peripheral vascular disease, or cardiovascular death. Healthy controls were randomly selected from a population screening program for risk factors of CVD in the same regions and matched to cases on the basis of age (±4 years). Participants with diabetes, hypertension, hyperlipidemia, and missing data and those with BMI < 18.5 kg/m2 were not included in the controls. Informed consent was obtained from all participants.
Body measurements
Body weight, height, and waist circumference were measured, and BMI was calculated as weight in kilograms divided by the square of the height in meters. WC was measured two times at 1 cm above the umbilicus at minimal respiration by trained observers; the mean of the two WC measurements was utilized in the analysis. Information on demographic, lifestyle risk factors for all participants was obtained using a standard questionnaire administered by trained staffs, including smoking and drinking status. Cigarette smokers were those who self-reported smoking cigarettes at least once a day for 1 year or more. Alcohol consumption was expressed as the sum of milliliters of alcohol per week from wine, beer, and spirits. Blood samples were collected in the morning after at least 8 h of fasting. The concentrations of TC, FPG, HDL cholesterol, and triglycerides were assessed enzymatically using an automatic biochemistry analyzer (Hitachi Inc., Tokyo, Japan) and commercial reagents.
Genomic DNA extraction and genotyping
Blood samples were collected from each participant. We selected SNPs within the SELP and IL-6 gene according to the following criteria: (1) which have been reported associations with risk factors of CVD; (2) minor allele frequency (MAF) greater than 5%. At last, three SNPs within SELP gene and three SNPs within IL-6 gene were selected for genotyping in the current study, including rs1800805, rs1800808, and rs6136 within SELP gene, and rs1800796, rs1800795, and rs1800797 within IL-6 gene. Genomic DNA from participants was extracted from EDTA-treated whole blood, using the DNA Blood Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. SNPs within SELP gene were detected by Taqman fluorescence probe, and the detailed methods and procedure have been well described in our previous study (Kou et al. 2016). Genotyping for three SNPs within IL-6 was performed by polymerase chain reaction (PCR) restriction fragment length polymorphism (PCR-RELP) method. The nucleotide sequence of primers and description for the six SNPs are shown in Table 1. The PCR was carried out in a 25 μl reaction mixture containing 100 ng genomic DNA, 1.5 mM MgCl2, 0.2 mM dNTPs, 1 mM each primer, reaction buffer, and 0.625 U Taq polymerase. The following cycling conditions were used: initial denaturation at 94 °C for 3 min, followed by 35 cycles of 94 °C for 30 s, 56 °C for 30 s (52 °C for 30 s for rs1800795), 72 °C for 20 s, and a final extension at 72 °C for 5 min.
Statistical analysis
The means and SDs were calculated for normally distributed continuous variables, which were analyzed using Student’s t test. And percentages were calculated for categorical variables, which were analyzed using χ2 test. Hardy–Weinberg equilibrium (HWE) was performed using SNPStats (available online at http://bioinfo.iconcologia.net/SNPstats). Logistic regression was performed to investigate the association between six SNPs within SELP and IL-6 genes and CVD using gender, age, smoking and alcohol status, FPG, TC, TG, and HDL as covariates in the model. Generalized multifactor dimensionality reduction (GMDR) was used for gene–gene interaction, some parameters including cross-validation consistency, the testing-balanced accuracy, and the sign test, to assess each selected interaction were calculated. All reported p values were two-tailed, and to correct for multiple testing we defined a Bonferroni-corrected threshold in different tables.
Results
A total of 1082 subjects (519 males, 563 females), with a mean age of 53.9 ± 13.1 years, were selected, including 540 CVD patients and 542 normal control participants. Table 2 shows the characteristics of cases and controls. The distribution of smoking was significantly different between CVD cases and controls, and smoking rate was higher in cases than in controls. The mean values of WC, BMI, FPG, TG, and TC were also significantly higher in CVD cases than in controls. The concentration of HDL was lower in cases than in controls.
All genotypes were distributed according to HWE in controls (all p values were more than 0.05). The frequencies of rs1800805-A allele and AC genotype of rs6136 within SELP gene were significantly higher in CVD cases than in controls (29.6 vs. 22.1%; 40.2 vs. 31.2%), and rs1800796-G allele within IL-6 gene was also significantly higher in CVD cases than in controls. Logistic regression analysis showed that CVD risk was significantly higher in carriers with rs1800805-A allele than those with GG genotype (GA + AA vs. GG), adjusted OR (95% CI) = 1.69 (1.31–2.16), and CVD risk was also higher in carriers with AC or CC genotype of the rs6136 polymorphism than those with AA genotype (AC + CC vs. AA), adjusted OR (95% CI) = 1.78 (1.28–2.26), and higher in carriers with GC or CC genotype of the rs1800796 polymorphism than those with GG genotype (CC + GC vs. GG), adjusted OR (95% CI) = 1.67 (1.25–2.14). (Table 3).
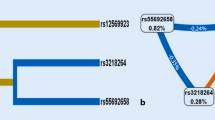
GMDR analysis was used to find the best gene–gene interaction combination among six SNPs within SELP and IL-6 genes in this study. It can be suggested from Table 4 a significant two-locus model (p = 0.0010) involving rs1800805 and rs1800796, indicating a potential gene–gene interaction between rs1800805 and rs1800796. Overall, the cross-validation consistency of this model was 10/10, the testing accuracy was 62.17%, and participants with rs1800805-GA or AA genotype and rs1800796-GC or CC have the highest CVD risk, compared to participants with rs1800805-GG and rs1800796-GG genotypes, and OR (95% CI) was 2.52 (1.81–2.66), after adjustment for gender, age, smoking and alcohol status, FPG, TC, TG, and HDL (Table 5).
Discussion
In the present study, we found that the CVD risks were higher in the rs1800805-A allele, C allele of rs6136 within SELP, and rs1800796-G allele within IL-6 carriers, suggesting that variants in three SNPs were associated with increased CVD risk. The human SELP gene maps on chromosome 1q22eq25 and is organized in 17 exons that span about 40 kb (Johnston et al. 1990), and many SNPs distributed in the promoter and coding sequences have been reported previously (Ay et al. 2007; Herrmann et al. 1998) with some other diseases, such as MI and IS (Tregouet et al. 2002; Nadar et al. 2004); however, the association of SNPs within SELP gene and susceptibility to CVD still remains controversial. A study (Barbaux et al. 2001) suggested a significant association between SELP gene polymorphisms and serum P-selectin levels, which was associated with coronary artery disease (CAD) risk as reported previously (Bielinski et al. 2015). Ghazouani et al. (2009) suggested that −2123C/G in SELP gene was associated with increased CHD risk in Tunisians. However, the inconsistent results were also obtained in some other studies. Volcik et al. (2006) indicated that Thr715Pro polymorphism is not associated with incident CHD or ischemic stroke (IS) in either whites or African-Americans, although genotypes carrying the P-selectin Pro715 variant allele are associated with decreased P-selectin levels compared to the homozygous wild-type genotype in whites. Zhou et al. (2014) also suggested no significant associations between SELP genetic polymorphisms and the risk of CHD and MI among Africans.
Several similar studies were also performed on the relationship between IL-6 SNP and CHD- or CVD-related diseases risk; however, these studies could not conclude consolidated results. Gigante et al. (2015) indicate no significant association of IL6R haplotypes with the risk of CHD in European populations. A meta-analysis (Song et al. 2015) suggested that the IL-6-572G > C polymorphism may play a protective role on the risk of CHD. Another Chinese study in Han Chinese population (Jia et al. 2010) indicated a significant association between the −572G/C polymorphism within IL-6 gene and pathogenesis of CHD. Tong et al. (2013) suggested that IL-6 SNPs were associated with increased CAD risk in the Chinese population and may be useful predictive markers for CAD susceptibility. Another Chinese case–control study (Fan et al. 2011) also suggested that IL-6 572C/G polymorphism was associated with susceptibility to CHD after adjustment for several other risk factors, and they concluded that IL-6-572C/G polymorphism might be a potential risk factor for CHD in Chinese population. A meta-analysis (Yin et al. 2012) also suggested a positive association between L-6 gene polymorphism and increased CHD risk among Asians.
The pathogenesis of CVD is diverse, including too many genetic factors, gene–gene and gene–environment interactions. However, till now, no studies focused on the impact of gene–gene interactions between SELP gene and IL-6 gene on CVD risk. In this study, GMDR analysis was used to investigate gene–gene interaction among these six SNPs in this study; we found a significant gene–gene interaction between rs1800805 and rs1800796, and participants with rs1800805-GA or AA genotype and rs1800796-GC or CC have the highest CVD risk, compared to participants with rs1800805-GG and rs1800796-GG genotype. To our knowledge, this is the first study focused on the impact of gene–gene interaction between SELP gene and IL-6 gene on CVD risk. The underlying mechanism of this interaction was not well known. The influence of this interaction on sP-selectin levels may be the possible explanation for this interaction on CVD risk.
Several limitations of this study should be considered. Firstly, more SNPs within SELP or IL-6 gene should be included in the gene–gene interaction analysis. Secondly, the sample size was relatively small, and the results obtained from this study should be checked in the future studies with a larger sample size.
In conclusion, we found an important association of rs1800805, rs6136 minor allele of SELP gene, rs1800796 within IL-6 gene, and additional interaction between rs1800805 and rs1800796 with increased risk of CVD.
References
Ay C, Jungbauer LV, Sailer T, Tengler T, Koder S, Kaider A, Panzer S, Quehenberger P, Pabinger I, Mannhalter C (2007) High concentrations of soluble P-selectin are associated with risk of venous thromboembolism and the P-selectin Thr715 variant. Clin Chem 53:1235–1243
Barbaux SC, Blankenberg S, Rupprecht HJ, Francomme C, Bickel C, Hafner G, Nicaud V, Meyer J, Cambien F, Tiret L (2001) Association between P-selectin gene polymorphisms and soluble P-selectin levels and their relation to Coronary artery disease. Arterioscler Thromb Vasc Biol 21(10):1668–1673
Basso F, Lowe GD, Rumley A, McMahon AD, Humphries SE (2002) Interleukin-6 -174G>C polymorphism and risk of coronary heart disease in West of Scotland coronary prevention study (WOSCOPS). Arterioscler Thromb Vasc Biol 22(4):599–604
Bielinski SJ, Berardi C, Decker PA, Kirsch PS, Larson NB, Pankow JS, Sale M, de Andrade M, Sicotte H, Tang W, Hanson NQ, Wassel CL, Polak JF, Tsai MY (2015) P-selectin and subclinical and clinical atherosclerosis: the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 240(1):3–9
Carter AM, Anagnostopoulou K, Mansfield MW, Grant PJ (2003) Soluble P-selectin levels, P-selectin polymorphisms and cardiovascular disease. J Thromb Haemost 1:1718–1723
Elmas E, Bugert P, Popp T, Lang S, Weiss C, Behnes M, Borggrefe M, Kalsch T (2010) The P-selectin gene polymorphism val168met: a novel risk marker for the occurrence of primary ventricular fibrillation during acute myocardial infarction. J Cardiovasc Electrophysiol 21:1260–1265
Fan WH, Liu DL, Xiao LM, Xie CJ, Sun SY, Zhang JC (2011) Coronary heart disease and chronic periodontitis: is polymorphism of interleukin-6 gene the common risk factor in a Chinese population? Oral Dis 17(3):270–276
Ghazouani L, Abboud N, Khlifa SB, Perret C, Nicaud V, Cambien F, AlmawiWY, Mahjoub T (2009) P-selectin gene polymorphisms and risk of coronary heart disease among tunisians. J Thromb Thrombolysis 28:314–319
Gigante B, Strawbridge RJ, Velasquez IM, Golabkesh Z, Silveira A, Goel A, Baldassarre D, Veglia F, Tremoli E, Clarke R, Watkins H, Hamsten A, Humphries SE, de Faire U (2015) Analysis of the role of interleukin 6 receptor haplotypes in the regulation of circulating levels of inflammatory biomarkers and risk of coronary heart disease. PLoS ONE 10(3):e0119980
Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB, American Heart Association Statistics Committee and Stroke Statistics Subcommittee (2013) Heart disease and stroke statistics-2013 update: a report from the American Heart Association. Circulation 127(23):e841
Herrmann SM, Ricard S, Nicaud V, Mallet C, Evans A, Ruidavets JB, Arveiler D, Luc G, Cambien F (1998) The P-selectin gene is highly polymorphic: reduced frequency of the Pro715 allele carriers in patients with myocardial infarction. Hum Mol Genet 7:1277–1284
Humphries SE, Luong LA, Ogg MS, Hawe E, Miller GJ (2001) The interleukin-6 -174 G/C promoter polymorphism is associated with risk of coronary heart disease and systolic blood pressure in healthy men. Eur Heart J 22(24):2243–2252
Jia X, Tian Y, Wang Y, Deng X, Dong Z, Scafa N, Zhang X (2010) Association between the interleukin-6 gene -572G/C and -597G/A polymorphisms and coronary heart disease in the Han Chinese. Med Sci Monit 16(3):CR103–C108
Johnston GI, Bliss GA, Newman PJ, McEver RP (1990) Structure of the human gene encoding granule membrane protein-140, a member of the selectin family of adhesion receptors for leukocytes. J Biol Chem 265:21381–21385
Kee F, Morrison C, Evans AE, McCrum E, McMaster D, Dallongeville J, Nicaud V, Poirier O, Cambien F (2000) Polymorphisms of the P-selectin gene and risk of myocardial infarction in men and women in the ectim extension study. Etude castemoin de l’infarctus myocarde. Heart 84:548–552
Kou L, Yang N, Chen G, Li Y, Yang J, Dong B, Qin Q (2016) Association of SELP genetic polymorphisms and additional gene-smoking interaction on cardiovascular disease in Chinese Han population. Int J Clin Exp Pathol 9(9):9612–9618
Nadar SK, Lip GY, Blann AD (2004) Platelet morphology, soluble P selectin and platelet P-selectin in acute ischaemic stroke. The West Birmingham stroke project. Thromb Haemost 92:1342–1348
Nichols M, Townsend N, Luengo-Fernandez R, Leal J, Gray A, Scarborough P, Rayner M (2012) European cardiovascular disease statistics 2012. European Heart Network/European Society of Cardiology, Brussels/Sophia Antipolis
Pasquali A, Trabetti E, Romanelli MG, Galavotti R, Martinelli N, Girelli D, Gambaro G, Olivieri O, Pignatti PF (2010) Detection of a large deletion in the P-selectin (selp) gene. Mol Cell Probes 24(3):161–165
Pereira DS, Garcia DM, Narciso FM, Santos ML, Dias JM, Queiroz BZ, Souza ER, Nóbrega OT, Pereira LS (2011) Effects of 174 G/C polymorphism in the promoter region of the interleukin-6 gene on plasma IL-6 levels and muscle strength in elderly women. Braz J Med Biol Res 44(2):123–129
Ray A, LaForge KS, Sehgal PB (1990) On the mechanism for efficient repression of the interleukin-6 promoter by glucocorticoids: enhancer, TATA box, and RNA start site (Inrmotif) occlusion. Mol Cell Biol 10(11):5736–5746
Song C, Liu B, Yang D, Diao H, Zhao L, Lu Y, Yu Y, Guo Z, Zhang J, Liu J, Zaho Z, Zhang X (2015) Association between interleukin-6 gene 2572G > C polymorphism and coronary heart disease. Cell Biochem Biophys 71(1):359–365
Tong Z, Li Q, Zhang J, Wei Y, Miao G, Yang X (2013) Association between interleukin 6 and interleukin 16 gene polymorphisms and coronary heart disease risk in a Chinese population. J Int Med Res 41(4):1049–1056
Tregouet DA, Barbaux S, Escolano S, Tahri N, Golmard JL, Tiret L, Cambien F (2002) Specific haplotypes of the P-selectin gene are associated with myocardial infarction. Hum Mol Genet 11:2015–2023
U.S. Department of Health and Human Services (2004) The Health Consequences of Smoking: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health
Volcik KA, Ballantyne CM, Coresh J, Folsom AR, Wu KK, Boerwinkle E (2006) P-selectin Thr715Pro polymorphism predicts P-selectin levels but not risk of incident coronary heart disease or ischemic stroke in a cohort of 14 595 participants: the Atherosclerosis Risk In Communities Study. Atherosclerosis 186(1):74–79
Wei YS, Lan Y, Liu YG, Tang RG, Lan JS (2006) Relationship between interleukin-6 gene polymorphism and coronary heart disease and its effect on plasma lipid levels. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 18(4):233–236
Yeh KY, Li YY, Hsieh LL, Chen JR, Tang RP (2010) The -174 G/C polymorphism in interleukin-6 (IL-6) promoter region is associated with serum IL-6 and carcinoembryonic antigen levels in patients with colorectal cancers in Taiwan. J Clin Immunol 30(1):53–59
Yin YW, Hu AM, Sun QQ, Liu HL, Wang Q, Zeng YH, Xu RJ, Hou ZZ, Zhang ZD, Zhang SJ, Zhou MQ (2012) Association between interleukin-6 gene -174 G/C polymorphism and the risk of coronary heart disease: A meta-analysis of 20 studies including 9619 cases and 10,919 controls. Gene 503(1):25–30
Zhou DH, Wang Y, Hu WN, Wang LJ, Wang Q, Chi M, Jin YZ (2014) SELP genetic polymorphisms may contribute to the pathogenesis of coronary heart disease and myocardial infarction: a meta-analysis. Mol Biol Rep 41(5):3369–3380
Acknowledgements
The writing of this paper was supported by Tianjin Chest Hospital. We thank all the partners and staffs who helped us in conducting this study. This study was funded by the key project of Science and Technology of Tianjin Health and Family Planning Commission.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kou, L., Yang, N., Dong, B. et al. Interaction between SELP genetic polymorphisms with inflammatory cytokine interleukin-6 (IL-6) gene variants on cardiovascular disease in Chinese Han population. Mamm Genome 28, 436–442 (2017). https://doi.org/10.1007/s00335-017-9712-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00335-017-9712-9